
Abstract
Introduction
Renal failure and symptomatic benign prostatic hyperplasia (BPH) are two common health problems which co-exist in 5.9–13.6% of the male population over 50 years of age [McConnell et al. 1994; Gerber et al. 1997; Rule et al. 2005; Hong et al. 2010]. It is usually not clear in this group of patients whether the reason for renal insufficiency is or is not BPH. However, it has been reported in some studies that the incidence of diabetes mellitus and hypertension is higher in patients with renal failure (RF) and lower urinary tract symptoms (LUTS) due to BPH [Gerber et al. 1997; Rule et al. 2005]. On the other hand, it is known that due to chronic urinary obstruction, BPH can lead to RF and even death occasionally [Ekman, 1989; Napalkov et al. 1995].
Current treatment policy in BPH mostly targets the symptoms usually assessed by International Prostate Symptom Score (IPSS).
Over time the mainly constant indication for BPH surgery has been medical treatment-refractory moderate or severe LUTS; definite surgical indications also include upper urinary tract deterioration [Cam et al. 2010]. As it is known that RF increases the risk in prostatic surgery [Holtgrewe and Valk, 1962; Melchior et al. 1974], a tendency towards avoiding the surgery until the detection of an absolute indication may occur. However, most of these studies are based on data from two or three decades ago and do not represent contemporary urology and nephrology practice. Moreover, even if there is no external factor, it is known that, in some patients, renal insufficiency does not exhibit a progressive pattern [el Nahas and Coles, 1986].
The aim of this study was to evaluate the mortality and early and late morbidity of transurethral resection of prostate (TUR-P) in patients with mild RF, who were operated on for medical treatment-refractory moderate or severe LUTS, as well as the comorbid factors.
Methods
A total of 357 patients who underwent TUR-P in our institution during January 2007 to August 2010 were included in the study. Patients over 50 years of age who had symptomatic BPH with IPSS equal to or greater than 20, who were irresponsive to medical treatment with alpha adrenergic blockers or 5-alpha reductase inhibitors (ARIs) as the first-line therapy were included. Patients with initial prostate-specific antigen (PSA) values over 4 ng/ml (2 ng/ml after at least 6 months use of ARIs) were included after the pathological confirmation of cancer-free status.
Patients with indwelling urethral catheters, residual urine volumes greater than 300 ml, upper urinary tract dilatation on ultrasound, end-stage renal disease requiring hemodialysis and creatinine serum levels higher than 3 mg/dl were excluded from analysis. Exclusion of the patients with high residual urine volumes or complete urinary obstruction was made in an effort to provide the homogeneity of the RF group. Moreover, the loss of renal function in these patients may be reversible after the obstruction is removed. Patients with acute urinary infections were included after demonstration of sterile urine on culture. Patients who underwent open prostatectomy were not included in the study.
Patients with normal renal function and RF were grouped as groups 1 and 2, respectively.
Patient age, comorbid diseases, PSA level, IPSS, residual urine volume, prostate volume, urea, creatinine, Na, K levels and upper urinary tract dilatation on USG and plain abdominal pain were recorded. Patients with creatinine serum levels >1.5 mg/dl were accepted to have RF and included in group 2. These patients were consulted by a nephrologist before being included in the study.
TUR-P was performed using a 26f Storz continuous irrigation resectoscope and 1.5% glycine solution. Resection was carried on until the prostatic capsule was seen. Either general or regional anesthesia was applied. Early postoperative values of hemoglobin, Na, K, urea and creatinine levels which were measured 3 hours after the operation were recorded. The need for blood transfusion and presence of a TUR syndrome were also evaluated. The catheters of the patients were removed in 48–72 hours after the urine became clear.
Mean age, total and free PSA (fPSA) levels, IPSS, preoperative urea creatinine, Na and K levels, prostate volumes of the two groups and incidence of comorbid diseases were compared. Compared early postoperative (first 3 hours) parameters were hemoglobin, Na, K, creatinine levels and need for blood transfusion, as well as the incidence of TUR syndrome and volumes of resected tissue and operation times.
Patients were re-evaluated at the third month after surgery with evaluation of the renal function, presence of urethral stricture or residual prostatic tissue, comorbidities and other TUR-P complications.
Statistical calculations were made using the software SPSS16 for Windows (SPSS Inc. Chicago, IL, USA). Normality of data distribution was tested with the Shapiro–Wilk test. Continuous variables were compared using Student’s t-test and Mann–Whitney U-tests. Categorical data were analyzed with chi-squared test. p-values lower than 0.05 were accepted to be significant.
Results
Among 357 patients who were evaluated for the study, 8 from the RF group and 50 from the normal renal function group with indwelling urethral catheters and 2 patients with the diagnosis of Pca were excluded from the study. The incidence of elevated creatinine level in the group of patients who were candidates for BPH surgery was 9.9%.
The postoperative pathologic evaluation revealed BPH in 183 (67.2%), BPH + inflammation in 58 (21.3%), low-grade prostatic intraepithelial neoplasia (PIN) in 23 (8.4%) and prostate cancer in 8 (2.9%) patients in group 1. In group 2, 21 patients (84%) had BPH, 3 (12%) had BPH + inflammation and 1 patient (4%) had low-grade PIN in TUR-P specimens. No cancer was found in group 2.
Table 1 demonstrates the patient characteristics, resection time and amount of resected tissue.
Patient characteristics, resection time and amount of resected tissue of patients in groups 1 and 2.

Statistically significant
PV, prostate volume; RV, residual urine; TPSA, total PSA; fPSA, free PSA; IPSS, International Prostate Symptom Score; Cr, creatine; Hb, hemoglobin.
The two groups were similar regarding age, Na level, IPSS, prostate volume (PV), residual volume (RV), operation time and resected tissue. Total and fPSA, creatinine, urea and K levels of group 2 were significantly higher than group 1, while the mean hemoglobin level was significantly lower.
Na, K, urea, creatinine and hemoglobin levels of the two groups in the early postoperative period and the percentage changes between preoperative and postoperative values are given in Tables 2 and 3, respectively.
The Na, K, urea, creatinine and hemoglobin levels of the two groups in the early postoperative period (3 hours after operation).
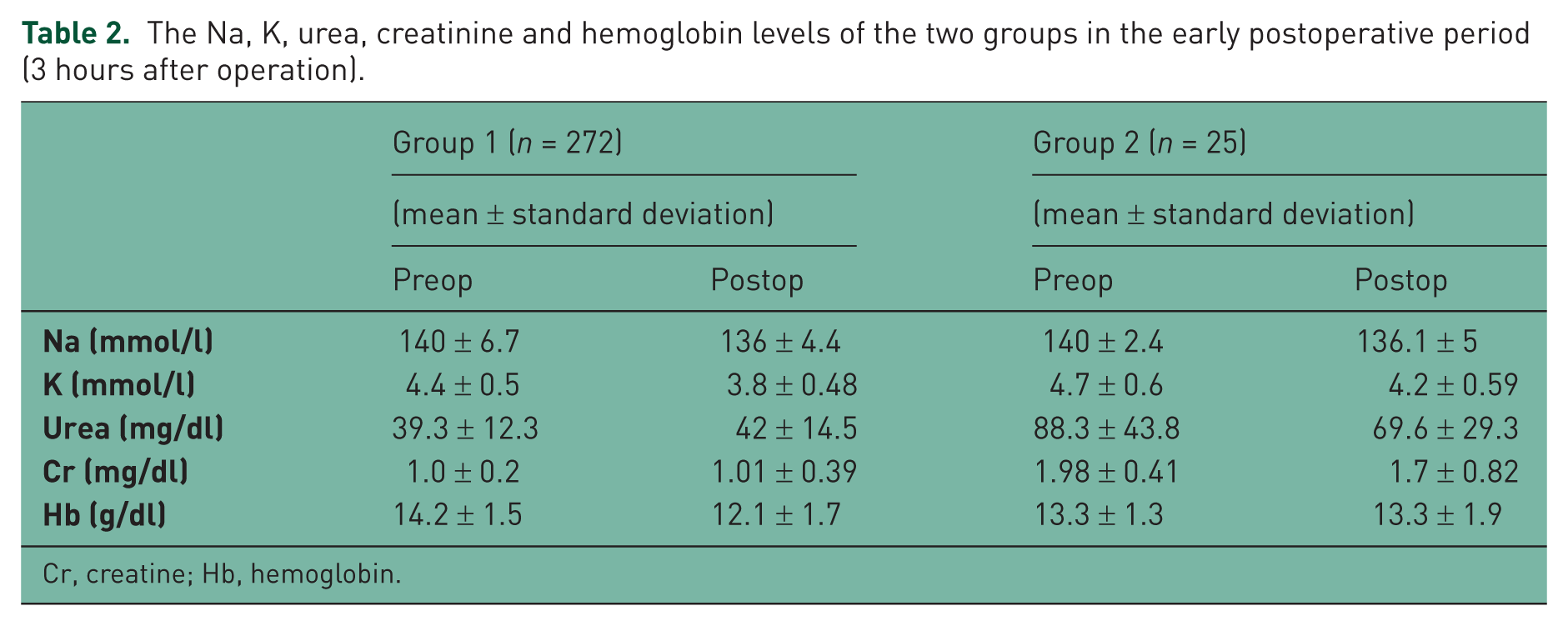
Cr, creatine; Hb, hemoglobin.
The percentage changes of variables before and after surgery.

Δ, percentage change; Cr, creatine
The percentage changes observed after TUR-P in Na, K, urea and creatinine levels were similar in both groups. One patient from each group experienced TUR syndrome with Na levels lower than 120 meq/l. Both patients responded well to supportive treatment with 3%NaCl solution and diuretics. None of the patients needed dialysis after the operation. Moreover, urethral stricture, re-operation, urinary tract infection and blood transfusion rates of the two groups were similar (p = 0.58).
Anesthesia technique was chosen by the anesthesiologist, no difference was observed among the groups regarding the method used (p > 0.05).
Comparison of the two groups regarding the preoperative comorbid factors is shown in Table 4.
Preoperative comorbid factors.

p = 0.027
CAD, coronary artery disease; CVE, cerebrovascular events; COLD, chronic obstructive lung disease.
While 112 of 272 patients in group 1 (41.1%) had one or more comorbid diseases, this ratio was 64% in group 2 (16 of 25 patients). Comorbid diseases were significantly more frequent in group 2.
Discussion
In patients over 50 years of age, BPH and RF are two health problems those can co-exist in a particular number of patients. This co-existence was observed in 9.9% of our series including 357 patients. A quarter of men aged 50–79 suffer from LUTS due to BPH [Jacobsen et al. 1995]. The most common indication for BPH surgery is medical treatment-refractory LUTS, and the main motive of BPH surgery is to improve quality of life [Mebust, 1998]. Various factors can contribute to the development of RF, including prerenal, intrinsic and postrenal causes. Among postrenal causes, bladder outlet obstruction due to BPH is the one that is most commonly observed, and these patients frequently experience dilatation and deterioration of the upper urinary tract [Sacks et al. 1989; Koch et al. 1996]. Catheterization of such patients for an appropriate time may reverse the changes in the upper urinary tract. On the other hand, some patients with BPH do not develop upper urinary tract dilatation although they have high urea and creatinine levels. The question ‘do these patients with high creatinine levels, but no urinary tract dilatation carry a higher operative risk for TUR-P than patients with normal renal function?’ remains to be answered. The aim of this study was to compare the morbidity and mortality of TUR-P in patients with and without creatinine level elevations (<1.5 versus 1.6–3 mg/dl) regarding age, complications, IPSS, free and total PSA serum levels, Na, K, urea, creatinine levels, PV, RV and other comorbid factors.
It was reported that RF increases BPH morbidity and mortality [Holtgrewe and Valk, 1962; Melchior et al. 1974; Mebust et al. 1989]. However, most of these studies were based on data of from two or three decades ago, since when significant advances in anesthesiology and intensive care medicine as well as urotechnology has been achieved. The use of continuous-flow resectoscopes, nonhemolytic irrigation fluids and decrease in operative time due to improving and refining of TUR-P technique in time with the increased number of operations performed probably has had significant positive effects on TUR-P outcomes. Similarly, there were no differences between the two groups regarding TUR-P complications in our study. Particularly, the low incidence of TUR syndrome (one patient in each group) and no need for postoperative hemodialysis confirm this idea. However, we think that the moderate mean prostate size of around 45 ml and moderate operation time of 35–40 minutes probably have a great influence on this relatively low complication rates. Mortality rates of the two groups were similar. Moreover, the two groups were similar regarding the need for blood transfusion and urethral stricture, 3 months after the operation. It was reported that diseases such as diabetes mellitus and hypertension are more common in patients with RF among BPH cohort [Gerber et al. 1997; Rule et al. 2005; Hong et al. 2010]. Similarly, in our study, the incidence of these diseases were found to be higher in the RF group. The mean age of RF group was numerically higher than group 1, although the difference lacked any significance. We think that advanced age may also be a factor in the development of RF. The mean PSA and free PSA levels of group 2 were significantly higher than those of group 1. Previous studies reported that RF did not affect PSA serum levels in BPH patients [Rule et al. 2005; Hong et al. 2010]. We think that these slight elevations in total and free PSA levels in RF group may be due to intraprostatic factors such as prostatic infarcts and infections. Expectedly, preoperative levels of hemoglobin, urea, creatinine and K were different between the two groups. No significant differences were observed between PV, RV and IPSS of the two groups. The exclusion of patients with excessive residual urine from the study explains the similarity of RV of the two groups.
The percentage changes between the preoperative and postoperative Na, K, urea and creatinine values of the two groups were similar. The resected volumes and resection times of the two groups were similar as expected, because of the similar prostate volumes.
Conclusions
Mild elevations in serum creatinine levels do not increase the operative risk of TUR-P in BPH patients without excessive residual urine or upper urinary tract dilatation. We think that TUR-P can be performed in patients with BPH and nonendstage RF, high IPSS, moderate prostate volume, residual urine less than 300 ml and without excessive dilatation of the upper urinary tract carrying similar morbidity risk with patients without RF, using continuous-flow resectoscopes.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors declare no conflicts of interest in preparing this article.