
Abstract
Objective:
In this study we aimed to compare photoselective vaporization (PVP) with the GreenLight 120-W Laser and monopolar transurethral resection as surgical treatments of prostates less than 80 cc in men with obstructive benign prostatic hyperplasia.
Methods:
From February 2009 to March 2012 we allocated 101 patients with a prostate glands of less than 80 cc; patients were randomly assigned for surgical treatment with monopolar transurethral resection of the prostate (TURP) (n = 62) or PVP (n = 39). Serum prostate specific antigen (PSA), International Prostate Symptom Score (IPSS), Sexual Health Inventory for Men (SHIM), maximum flow rate (Qmax) postmicturition residual (PMR), transrectal ultrasound volumes (TRUS), postvoid urine residual (PVR), complications, re-operations and hospitalization time were collected. The patients were seen in the follow up at 6, 12 and 24 months.
Results:
Median age was 69 (56–87) years old in the TURP group and 67 (51–87) years old in the PVP group. Mean preoperative prostate volume was 55 cc (40–72) and 60 cc (41–75) cc in the TURP group versus the PVP group. There was no statistically difference in subjectively (IPSS, SHIM) and objectively (Qmax-PMR) parameters and postoperatively complication rates between the two groups (p
Conclusion:
Prostate PVP and TURP are effective surgical treatments for benign prostatic hyperplasia. Postoperative functional improvements were durable and equivalent in the two groups. The two techniques have a similar complication rate.
Keywords
Introduction
Benign prostatic hyperplasia (BPH) is a common condition and one of the important aetiologies of lower urinary tract symptoms (LUTS); it occurs in up to 30% of men older than 65 years and reduces quality of life [Chapple, 1999]. Although transurethral resection of the prostate (TURP) remains the reference standard for men with BPH, a number of minimally invasive treatments have become available [Shingleton et al. 2002]. Photoselective vaporization (PVP) of the prostate by GreenLight laser was one of the first new minimally invasive treatments available. The role of lasers in the surgical treatment of BPH is still being researched, particularly in specific patient groups such as patients on anticoagulant therapy [Tan and Gilling, 2003]. Preliminary short-term results suggest that this therapeutic modality is safe and effective [van Cleynenbreugel et al. 2009]. However, PVP cannot be yet recommended as a first-line therapy because comparative studies against TURP, especially with the GreenLight HPS™ 120-W power device, are still lacking [Jones et al. 2010]. The purpose of our prospective, randomized study was to compare the efficacy of PVP with GreenLight versus TURP less than 80 cc.
Patients and methods
Patients in whom medical therapy for their voiding symptoms had failed were offered into the study. After obtaining Institutional Review Board approval, 124 consecutive patients (mean age 64.3 years, range 54–82) with the symptoms of bladder outlet obstruction (BOO) due to BPH who referred to our urology clinic between February 2009 and March 2012 were prospectively enrolled to the study. A computer generated randomization schedule was used to assign patients to the treatment arms. One surgeon performed all the laser procedures and senior residents carried out the TURP procedures. Prostate size was measured with transrectal ultrasound (TRUS) and only those patients with a prostate volume <80 cc were accepted. Inclusion criteria for surgery were as follows: maximum flow rate (Qmax) <15 ml/s or postvoid urine residual (PVR) >150 cc in conjunction with an International Prostate Symptom Score (IPSS) >7. Criteria for patient exclusion from the study were neurogenic bladder disorder, urethral strictures, history of prostate adenocarcinoma or any previous prostatic, bladder neck or urethral surgery. Informed consent was obtained from all patients before any intervention. Patients were randomly assigned to following groups: group 1 (n = 64) underwent monopolar TURP and group 2 (n = 60) underwent PVP. All patients had undergone preoperatively by physical examination, including digital rectal examination (DRE). Information on urine analysis, urine culture, serum prostate specific antigen (PSA) measurement, IPSS, Sexual Health Inventory for Men (SHIM), Qmax, TRUS measurement of the prostate, PVR, complications, re-operations and hospitalization time were collected. The patients were seen at the follow up at 6, 12 and 24 months. At each visit, IPSS and uroflowmetry findings were obtained. SHIM scores and PVR were assessed preoperatively and postoperatively. Standard TURP was performed under spinal or general anaesthesia using a Storz 26F continuous flow resectoscope. PVP was performed with a PVP GreenLight HPS 120-W laser. A total of 23 cases were excluded from this study due to incomplete medical records and lack of follow-up information after randomization, resulting in 101 cases (TURP = 61, PVP = 39) with follow-up information included in this study. Primary outcome variables included: IPSS and Qmax changes at 6, 12, 24 months; and SHIM scores and PVR postoperatively. Secondary outcomes were complications, re-operations and hospitalization time.
Statistical analysis
All statistical analyses were performed using SPSS ver.16.5 (Statistical Package for Social Sciences for Windows 16.5 Inc., Chicago, IL, USA). The variables were investigated using visual (histograms probability plots) and analytical methods (Kolmogorov–Simirnov test) to determine whether or not they are normally distributed. Unpaired t-tests were performed for data with normal distribution. For parameters that did not show normal distribution, the nonparametric Mann–Whitney U-test was used to compare them. Between groups analysis were performed using the chi squared test. Changes in percentage of IPSS, Qmax and PVR values was calculated using the formula [(final value – baseline value) / baseline value × 100)] and the Mann–Whitney U-test. Improvement in voiding parameters in dependent groups was determined with nonparametric tests (Wilcoxon signed-rank test). A p value less than 0.05 was set for statistical significance.
Results
We noted no statistical difference in baseline characteristics such as patients’ age, prostate volume, PVR, PSA, Qmax, IPSS and SHIM scores between the two groups (Table 1). Median age was 69 (56–87) years old in the TURP group and 67 (51–87) years old in the PVP group. Median preoperative prostate volume was 55 cc (40–72) and 60 cc (41–75) in the TURP group versus the PVP group. A significant improvement was observed with voiding parameters in terms of IPSS and Qmax values that significantly improved after surgery and continued to do so during follow up in both groups at 6, 12 and 24 months according to baseline parameters (p < 0.001). However, there was no significant statistical difference in subjective (IPSS) and objective [Qmax, postmicturition residual (PMR)] parameters between TURP and PVP groups within each visit at 6, 12 and 24 months (Table 2). Erectile function was measured with the SHIM score and no significant change found during the follow-up period from baseline in both groups.
Preoperative baseline patient characteristics.

IPSS, International Prostate Symptom Score; PSA, prostate specific antigen; PVP, photoselective vaporization; PVR, postvoid urine residual; Qmax, maximum flow rate; SHIM, Sexual Health Inventory for Men; TURP, transurethral resection of the prostate.
Outcomes of the TURP and PVP groups.
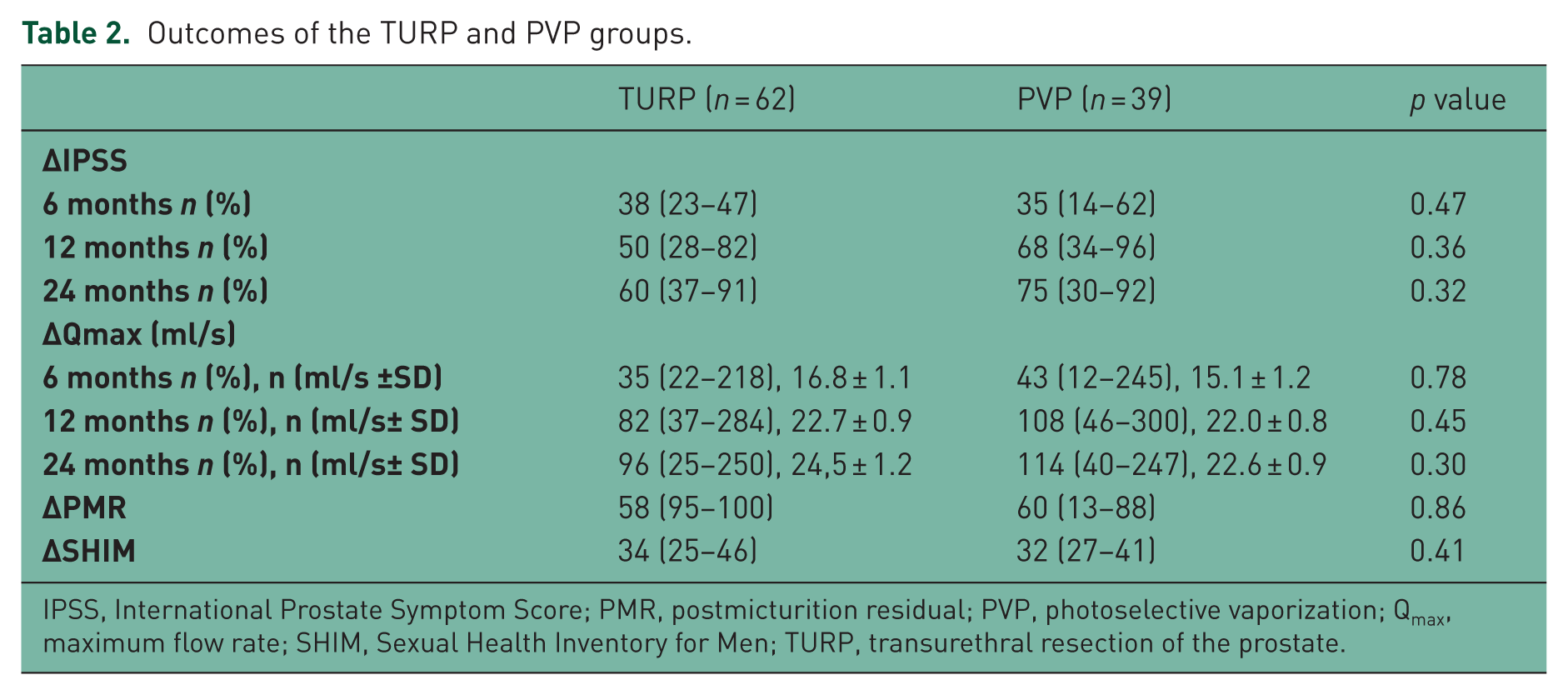
IPSS, International Prostate Symptom Score; PMR, postmicturition residual; PVP, photoselective vaporization; Qmax, maximum flow rate; SHIM, Sexual Health Inventory for Men; TURP, transurethral resection of the prostate.
There was no significant difference in early and late complications between groups (Table 3). A total of two patients (3.2%) in the TURP group and two patients (5.1%) in the PVP group required blood transfusions. Acute urinary retention early after the removal of catheter occurred in four patients (6.4%) in the TURP group and three patients (7.6%) in the PVP group. Urinary tract infection was documented with a urine culture test in six patients (9.6%) in the TURP group and four (10.2%) patients in the PVP group. Late complication rates were comparable in both groups. Urethral stricture was seen in 12 patients (19.4%) in the TURP group and five patients (12.8%) in the PVP group and internal urethrotomy performed. After 12 months, four patients (6.4%) required re-intervention in the TURP group and two patients (5.1%) in the PVP group. No urinary incontinence and the TUR syndrome occurred in both groups. Hospital stay was significantly shorter in the PVP group at 2 days (1–4) than the TURP group at 5 days (3–9) (p < 0.001).
Postoperative complication rates and hospital stay.

PVP, photoselective vaporization; TURP, transurethral resection of the prostate.
Discussion
TURP, which has been accepted as the standard surgical treatment for several years, constitutes almost 25% of all urologic operations. However, new endoscopic methods have developed as the result of medical needs and industrial progress. Our work is a randomized and prospective study comparing 120 W GreenLight PVP and TURP [Al-Ansari et al. 2010; Capitán et al. 2011; Lukacs et al. 2012]. The patients in this study were randomly assigned and the mean prostate volume was less than 80 cc.
In our study at 2-year follow up, IPSS had improved by 60 and 75%, and Qmax had increased by 96 and 114% in the TURP and PVP groups, respectively. Ruszat and colleagues reported long-term results of PVP after 500 procedures [Ruszat et al. 2008] which showed that PVP leads to immediate, sustained improvement in subjective and objective voiding parameters that lasts up to 5 years. In different prostate size subgroups (<40 and 40–80 ml), IPSS improved by 64 and 57%, and Qmax improved by 104 and 101%, respectively.
In our study the overall re-intervention rate for bladder neck obstruction and refractory symptom most likely caused by residual adenomas was four (6.4%) for TURP and two (5.1%) for PVP. Recent reports show a 15–23% overall retreatment rate after PVP with a 6.8–17.9% re-operation rate for residual adenoma [Horasanli et al. 2008; Ruszat et al. 2008]. In the current study blood transfusion was necessary in 3.2% of TURP patients and 5.1% of PVP patients. Similarly, Mebust and colleagues in their report on 3885 patients undergoing TURP noted a 2.5% transfusion rate [Mebust et al. 1989]. Although the minimal risk of bleeding either during or early after the surgery is the main advantage of PVP and the procedure could be applied in a safe manner even in high-risk patients in which some of the patients were under ongoing oral anticoagulant therapy during the procedure, two of our patients in the PVP arm needed a blood transfusion [Reich et al. 2004, 2005].
The recent 180-W XPS laser system represents a significant improvement over previous systems in terms of efficacy while maintaining the known safety characteristics of previous greenlight systems [Barry et al. 1995; Hoffman et al. 2004]. Similar to our study, in the GOLIATH study which compared TURP with laser prostatectomy using a 180-W GreenLight XPS™ system, the 180 W GreenLight XPS system was comparable with TURP in terms of IPSS, Qmax, overall complication-free rate and PVR reduction for the first 6 months. The GreenLight XPS system was superior to TURP in terms of shorter catheterization times, shorter hospital stay and more rapid return to stable health status. However, in our study the re-intervention rate was 6.4% in the TURP group versus 5.1% in the PVP group; although overall postoperative re-intervention rates were not significantly different between treatment arms, the early postoperative re-intervention rate was three times higher after TURP compared with GreenLight XPS [Bachmann et al. 2014].
A low rate of urinary retention in the TURP group (four patients, 6.4%) and in the PVP group (three patients,7.6%) was seen in our study, although the urinary retention after PVP (15.3%) was higher than in previously published studies [Sandhu et al. 2004; Bachmann et al. 2005a]. Our study showed that the risk of acute urinary retention was similar in the PVP group compared with the TURP group. We also found urethral stricture rates of 12 patients (19.4%) in the TURP group and five patients (12.8%) in the PVP group, but this was not statistically significant. Despite the 26F outer sheath used in the resectoscope and prolonged catheterization period, the risk of urethral and meatal strictures might be higher in the TURP group, However, in our study, the incidence of urethral strictures in the PVP group was comparable with the TURP group. Bachmann and colleagues reported a 7.8% incidence of urethral stricture after PVP [Bachmann et al. (2005b].
Sexual function after PVP has not been evaluated [Gacci et al. 2011] and some have questioned whether this procedure has an impact on erectile function [Bruyère et al. 2010]. Paick and colleagues reported improvement in the all International Index of Erectile Function (IIEF) domains at 6-month follow up [Paick et al. 2007]. Our results show that no significant improvement in the
Conclusion
Like the other randomized clinical trials, the result of our study show that during the 2-year follow-up period, patients undergoing PVP continued to experience the same improvement in symptom score and flow rate as patients undergoing TURP. PVP and TURP are effective surgical treatments for BPH, affecting LUTS improvement. PVP is associated with a reduced hospital stay. Postoperative functional improvements were durable and equivalent in the two groups. The two techniques have similar complication rates. Further studies with a large number of patients and longer follow up are warranted to assess the clinical benefits of this technique for the surgical management of LUTS.
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.