
Abstract
Objectives:
To review outcomes for patients with irritable bowel syndrome (IBS) or inflammatory bowel disease (IBD) who undergo holmium laser enucleation of prostate (HoLEP) for bothersome urinary symptoms related to benign prostatic hyperplasia (BPH).
Methods:
We performed a retrospective review of patients who had undergone HoLEP by a single surgeon between January 2021 and August 2023. Preoperative, intraoperative, and postoperative characteristics were compared between patients with an ICD-10 diagnosis of IBS or IBD and those without, using Chi-square and paired T-tests as appropriate.
Results:
Out of 918 men, 24 (2.6%) had a diagnosis of IBS, and 36 (3.9%) had a diagnosis of IBD. There were no differences in age, BMI, preoperative American Urological Association symptoms score (AUASS), preoperative Michigan Incontinence Symptom Index (MISI) score, and history of urinary retention or incontinence. The IBS + IBD cohort had smaller prostates (100.9 vs 124.2 mL, p = 0.01) and shorter procedure times (57.0 vs 66.5 min, p = 0.02) than controls. IBS patients were more likely to require anticholinergic therapy at a 3-month follow-up (31% vs 13%, p = 0.03) and had more postoperative encounters within 90 days of HoLEP (3.7 vs 2.6, p = 0.01). There were no differences regarding changes in AUASS and MISI scores, same-day trial of void and same-day discharge rates, or complication rates.
Conclusion:
IBS patients who underwent HoLEP had more symptomatic postoperative courses requiring higher rates of anticholinergic medication use and more provider interactions compared to men without IBS, despite similar AUASS and MISI scores. These trends were not observed in patients with IBD.
Keywords
Introduction
Bladder and bowel dysfunction (BBD) is a term used to describe the spectrum of lower urinary tract symptoms (LUTS) accompanied by fecal elimination issues. While BBD is most commonly described in the pediatric population and represents up to 40% of pediatric urology consultations, 1 the association between bowel and bladder function is also well established in adults. Due to the neuronal crosstalk and proximity between the two systems, dysfunction in one system may lead to higher rates of dysfunction in the other, especially as we age. 2
Irritable bowel syndrome (IBS) is a common functional gastrointestinal disorder characterized by abdominal discomfort and abnormalities in bowel habits and affects up to 10%–15% of adults in the United States. Studies have shown that patients with IBS are disproportionally more likely to undergo abdominal and pelvic surgery with variable outcomes. 3 Patients with IBS are also more likely to have overactive bladder (OAB) urinary symptoms. 4 Animal studies and clinical data show that on a functional level, in animals and humans, bowel distension affects bladder activity and vice versa. Functional gastrointestinal disorders, such as constipation, can contribute to the development of LUTS including OAB symptoms. The exact etiology of this relationship is unknown; however, one theory is that of cross-organ sensitization, where sensory innervation of bowel and bladder interact. 5 While inflammatory bowel disease (IBD) is a separate disease entity and has a separate disease process compared to IBS, many patients experience similar bowel and lower urinary tract symptomatology.6,7
To our knowledge, there are very few studies evaluating the outcomes of patients with known bowel disorders who undergo surgery for urinary symptoms related to bladder outlet obstruction due to benign prostatic hyperplasia (BPH). Holmium laser enucleation of the prostate (HoLEP) is one of the surgical options for the treatment of BPH and is an increasingly prevalent safe, size-independent, durable treatment modality. 8 Because of the connection between bowel and bladder function, we sought to determine whether bowel disorders change characteristics of the HoLEP postoperative course by comparing patients with IBS and IBD to those without bowel disorder diagnoses.
Materials and methods
Under institutional review board (IRB) approval, using our institution’s enterprise data warehouse, we conducted a retrospective review of all men who had undergone HoLEP between January 2021 and August 2023 at our institution. All patients were over the age of 18 and did not have a concurrent procedure at the time of their HoLEP. All HoLEP procedures were performed by a single surgeon using MOSES 2.0 laser technology in a technique previously described by Assmus et al. 9 We identified men in this cohort with a known diagnosis of IBS or IBD prior to their HoLEP using the corresponding ICD-10 diagnosis codes. The IBD cohort included patients with either a diagnosis of Crohn’s disease (CD) or ulcerative colitis (UC). Patients without a documented diagnosis of IBS or IBD served as the control group to which our study cohort was compared. There were no other specific exclusion criteria outside of our data warehouse search criteria which included patients aged over 18 and patients undergoing HoLEP surgery by a specific single surgeon during the above designated time period.
Baseline clinical characteristics collected included age, BMI, preoperative prostate size, anticoagulation status, preoperative catheter status, history of prior UTIs, history of neurologic conditions, prior BPH surgery, history of urinary retention, history of urinary incontinence, AUA symptom scores, and Michigan Incontinence Symptom Index (MISI) scores. Neurologic conditions included documented diagnoses that may affect lower urinary tract function, including diabetes-related neuropathy/neurogenic bladder, Parkinson’s disease, dementia, cerebrovascular accident, multiple sclerosis, traumatic brain injury, brain/spinal tumors, myasthenia gravis, and spinal cord injury. The American Urologic Association (AUA) symptom score (AUASS) is a validated patient-reported questionnaire for measuring the severity of urinary symptoms from BPH. The questionnaire includes seven questions graded on a Likert scale from 1 to 5, for a total of 35 points, with higher scores denoting more severe symptoms. The AUASS was described by Barry et al. in 1992 and includes questions covering frequency, nocturia, weak urinary stream, hesitancy, intermittence, incomplete emptying, and urgency. 10 The MISI is another validated patient-reported questionnaire developed in 2014 that helps to measure the severity of urinary symptoms related to urinary incontinence. The MISI consists of 10 questions graded on a Likert scale from 1 to 5, with higher scores denoting more severe symptoms. 11
Intraoperative characteristics collected included procedure time, enucleation time, morcellation time, and intraoperative complication rates. Postoperative characteristics and outcomes included rates of the successful same-day trial of void (SDTOV), same-day discharge (SDD), length of Foley catheterization, length of hospital stay, 90-day complication rates including emergency room presentations and re-admissions, continence and catheterization rates, use of alpha-blocker or anticholinergic medication, AUASS and MISI scores postoperatively, and number of postoperative encounters within 90 days of surgery. Postoperative encounters included any urology-specific calls to the office, virtual office visits, face-to-face office visits, and hospital visits. At our institution, postoperative BPH medication and anticholinergics are not routinely prescribed after HoLEP. If patients have persistent bothersome irritative voiding symptoms after HoLEP, anticholinergic medication such as oxybutynin may be prescribed for symptomatic relief during the postoperative recovery period. Depending on patient age, preference, and comorbidities, beta-3 agonists such as mirabegron may be used instead.
All data analyses were performed using SPSS (IBM SPSS Statistics for Windows v.29., Chicago, IL). Descriptive statistics and comparisons between groups were performed with two-tailed Student T-tests and Chi-square tests for continuous and categorical variables, respectively, with p < 0.05 considered statistically significant. Changes in preoperative and postoperative AUASS and MISI scores were analyzed with paired T-tests. Multivariate regression was performed to control for prostate size.
Results
We identified a total of 918 men, of which 24 (2.6%) had a diagnosis of IBS and 36 (3.9%) had a diagnosis of IBD. The combined IBS + IBD patient cohort was not statistically different than the control group cohort in a variety of important baseline clinical characteristics shown in Table 1. There was no difference in patient age (70.9 vs 70.8 years, p = 0.95) or BMI (27.8 vs 28.1, p = 0.74). Both groups had similar rates of anticoagulation usage (20 vs 15%, p = 0.31) and neurological disease diagnoses (22 vs 20%, p = 0.78). More specifically, in the control cohort, 125 patients had diabetes, 3 patients had Parkinson’s disease, 17 patients had stroke, 9 patients had dementia, and 1 patient with spinal cord injury. There were 13 patients with both diabetes and a history of stroke, 2 patients with diabetes and dementia, 2 patients with diabetes, Parkinson’s, and stroke, and 1 patient with Parkinson’s and dementia. In the IBS + IBD patient cohort, 10 patients had diabetes, 1 patient had Parkinson’s, 1 patient had dementia, and 1 patient had a history of stroke. With regards to urologic history, there were similar rates of history of UTI within the prior 6 months (18 vs 19%, p = 0.52), history of urinary retention (47 vs 55%, p = 0.18), prior BPH medication usage (81 vs 84%, p = 0.525), prior ACh medication usage (8 vs 7%, p = 0.69), and history of urinary incontinence (21 vs 19%, p = 0.80). In addition, there were no differences in mean preoperative AUASS (19.7 vs 19.1, p = 0.64) or MISI (5.7 vs 5.7, p = 0.71) scores.
Baseline characteristics.

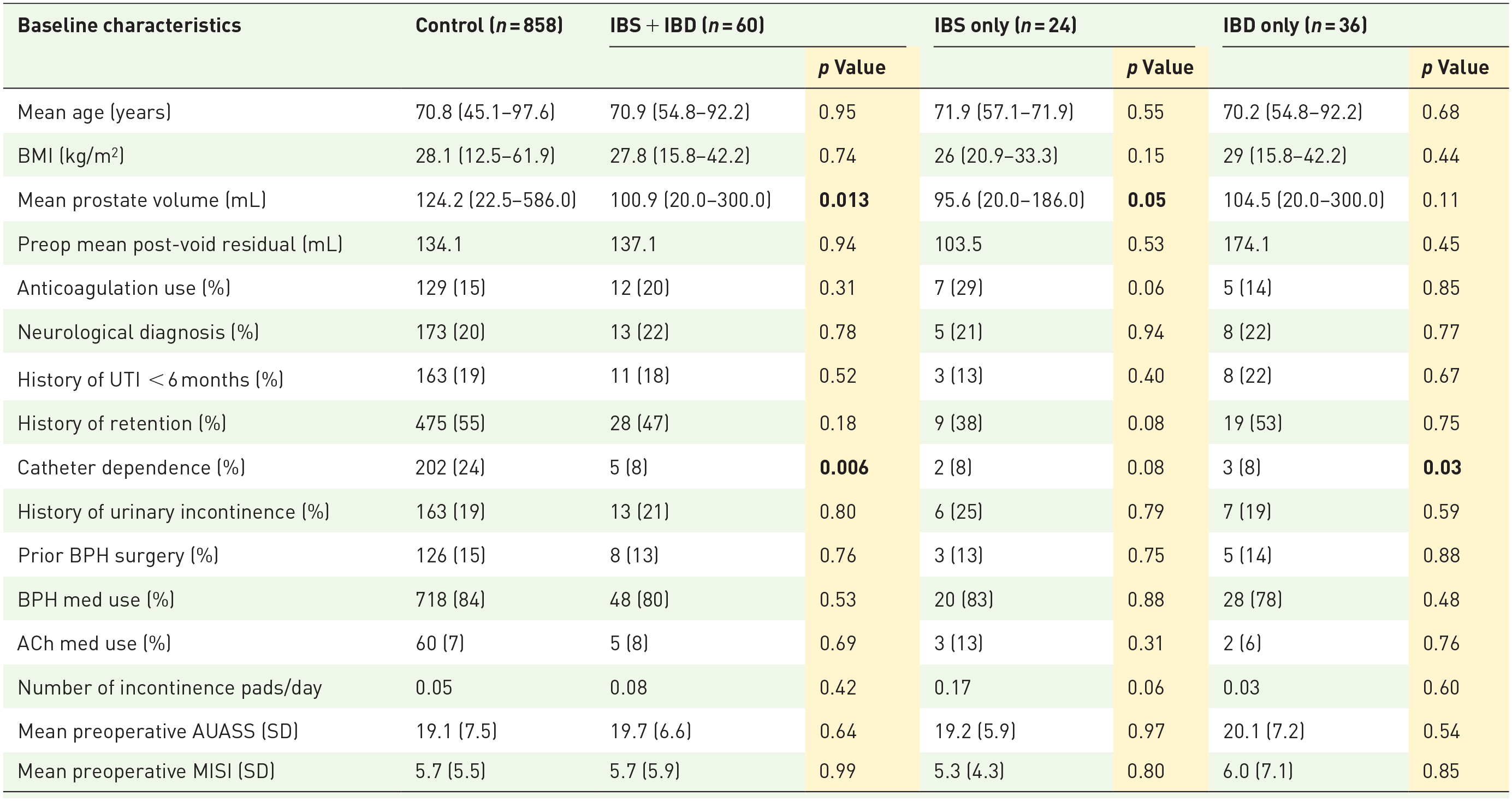
Bolding represents statistically significant p values <0.05.
Notably, we found that IBS + IBD patients had statistically smaller prostates than the controls, with IBS + IBD patients having an average prostate volume of 100.9 versus 124.2 mL for controls (p = 0.01). We also found that IBS + IBD patients were less likely to be catheter dependent at the time of HoLEP (8% vs 24%, p = 0.01).
Table 2 shows intraoperative characteristics and outcomes for each group. IBS + IBD patients had shorter mean total procedure times compared to controls (57.1 vs 66.5 min, p = 0.02). Enucleation time (29.3 vs 34.6 min, p = 0.02) and morcellation time (7.3 vs 10.5 min, p = 0.03) were both found to be significantly shorter in the study population. After controlling for prostate size with multivariate regression, there was no statistically significant difference in procedure time, enucleation time, and morcellation time (p > 0.05). There were no differences in intraoperative complication rates between the two groups (1.7 vs 3.6%, p = 0.42). There was a total of 32 (3.5%) intraoperative complications: 19 (2.1%) capsular perforations, 8 (0.9%) urethral injuries, 3 (0.3%) superficial bladder injuries, and 2 (0.2%) ureteral orifice injuries. None of these complications changed the patients’ postoperative course and were managed with catheterization overnight.
Intraoperative outcomes.


Table 3 shows selected postoperative outcomes. Postoperatively, there were no significant differences between the IBS + IBD patients and control group with regards to successful SDTOV (80 vs 75%, p = 0.41) and SDD (73 vs 71%, p = 0.76). The mean length of stay and mean length of Foley were similar. Ninety-day complication rates, including emergency room visits and readmissions, did not differ between the two groups (17 vs 22%, p = 0.42). There were similar rates of postoperative BPH medication use, ACh medication use, and continence rates at 90 days. Moreover, postoperative AUASS (9.3 vs 8.1, p = 0.32) and MISI scores (5.6 vs 6.2, p = 0.71) were similar between groups. AUASS scores postoperatively compared to preoperatively were significantly different among all cohorts, whereas MISI scores were not (Supplemental Table 1). There were no statistically significant differences in the degree of AUASS or MISI score changes between each cohort. Total postoperative encounters in the first 90 days after surgery were also similar (3.1 vs 2.6, p = 0.06). Ninety-day postoperative follow-up data including continence data, postoperative medication BPH and ACh use, and AUASS and MISI scores were available for 684 (80%) control patients and 45 (75%) IBS + IBD patients as shown in Table 3.
Postoperative outcomes.
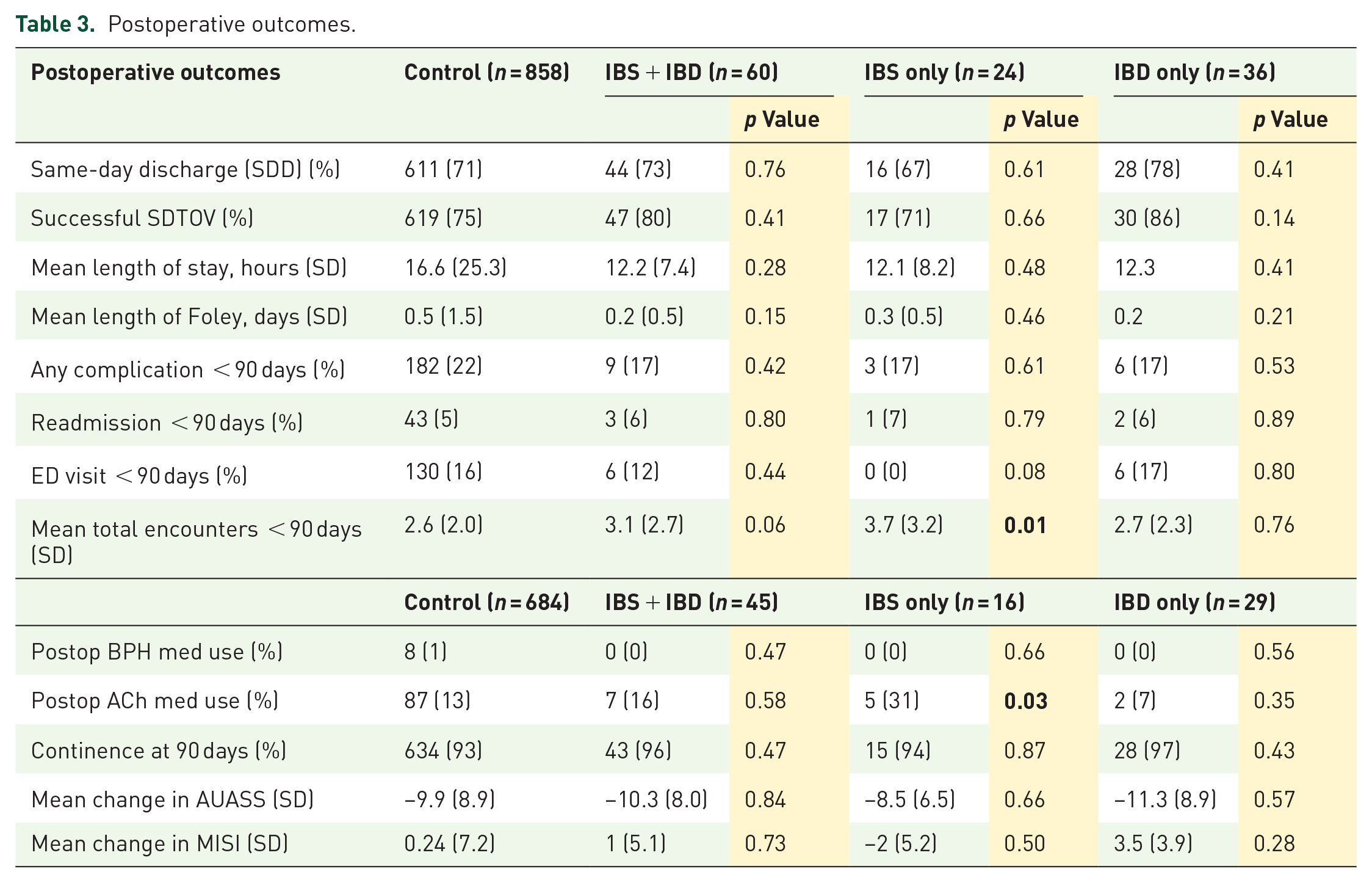

On subgroup analysis, IBS patients alone had significantly smaller prostates than controls (95.6 vs 124.2 mL, p = 0.05). Patients with IBD also had smaller prostates than controls but this was not statistically significant (104.5 vs 124.2 mL, p = 0.11). Patients with IBS were found independently to have shorter mean procedure times compared to controls (54.3 vs 66.5 min, p = 0.05). Patients with IBD had shorter procedure times compared to controls but did not reach statistical significance (59.0 vs 66.5 min, p = 0.16). After controlling for prostate size on multivariate regression, there were no differences in procedure time, enucleation time, or morcellation time (Supplemental Table 2). Subgroup analysis also revealed that patients with IBS were significantly more likely to require anticholinergic medication at 3 months of follow-up compared to controls (31 vs 13%, p = 0.03). We observed that patients with IBS had significantly more postoperative encounters within 90 days of surgery (3.7 vs 2.6, p = 0.01). These trends were not observed in patients with IBD.
Of the 36 patients with IBD, 14 (39%) had a diagnosis of CD, and 22 (61%) had a diagnosis of UC. Subgroup analysis was performed within these groups and did not show any significant preoperative, intraoperative, or postoperative differences between these groups and the control cohort.
Discussion
OAB and IBS symptoms greatly impact patient quality of life and a link between the two has been described in both animal models and human studies.12–14 Both disorders are characterized by increased frequency of emptying and hypersensitivity/hyperactivity. A large-scale survey study by Matsumoto et al. in Japan found high concordance between patients with OAB and patients with IBS. Among subjects with OAB, 33.3% had concurrent IBS. Similarly, roughly one-third of patients with IBS had concurrent OAB. 15 The relationship between bowel and bladder function is complex and its etiology is not well elucidated yet. The leading theory for this connection is that the bladder and intestines share common afferent nerve projections, suggesting the presence of neural crosstalk between the two organs. Sensitization of one organ through inflammation or damage may subsequently affect sensitization of other organs in its same nerve distribution.5,15
A previous study by Adibi et al. investigated the relationship between IBS and pelvic surgery in a small cohort and found no statistically significant differences in bowel symptoms following transurethral resection of the prostate (TURP). 16 This prior study evaluated patients 3 months after open simple prostatectomy or TURP for management of their BPH to determine if there were any functional bowel changes that persisted after the immediate recovery period. In their limited sample, they found increases in abdominal discomfort and relative frequency of diarrhea after open prostatectomy but not after transurethral surgery. Despite the well-established relationship and overlap between IBS and bothersome urinary issues, there remains limited knowledge as to whether patients with IBS or IBD present differently or have different outcomes after HoLEP than those without known diagnoses of bowel dysfunction. We sought to expand on the literature by providing our experience with regard to the characteristics and outcomes of patients with IBS and IBD who undergo HoLEP.
Our results show that patients with IBS and IBD who present with bothersome urinary symptoms and undergo HoLEP have significantly smaller prostate sizes than the general population at the time of presentation, with a size difference of about 20% (100.9 vs 124.2 mL). When performing subgroup analysis, patients with IBS continued to have statistically significantly smaller prostates. Patients with IBD also trended toward smaller prostates, though this did not reach statistical significance, likely due to sample size limitations. While larger prostate size does not always mean more severe LUTS or more obstructed voiding, there is a known correlation between prostate gland size, higher AUA symptom scores, and worse metrics on uroflowmetry.17–19 The significant difference in prostate size at presentation between the two cohorts could suggest that patients with IBS or IBD may be more likely to present to a urologist for irritative rather than obstructive voiding symptoms or issues with urinary retention, although there is insufficient data here to draw any definitive conclusions. Indeed, in our cohort, preoperative AUASS and MISI scores were not significantly different between the groups though we did see statistically significant improvements in AUASS across all groups. One limitation of our study and explanation for this finding is that our data is not granular enough to determine differences within each AUA symptom score domain. There may be higher scores (more severe symptoms) for irritative symptoms compared to obstructive symptoms for patients with bowel dysfunction. Future studies will be needed to investigate these subdomains more closely preoperatively compared to postoperatively.
Given that patients with IBS and IBD tend to have smaller prostates on presentation in our cohort, it is not surprising that these patients also had significantly shorter mean procedure durations, enucleation times, and morcellation times. There were no differences in procedure duration between the groups after controlling for prostate size on multivariate regression analysis. While HoLEP has been established as an effective and safe size-independent method of treating BPH, larger prostates are correlated with longer operative times and ostensibly, with higher risk to the patient.20,21 In our study, IBS or IBD disease status did not impact the safety of HoLEP.
The overall SDD rate was 71.6% and the successful SDTOV rate was 75.2% which is comparable with prior studies. 22 We did not observe any differences between patients with IBS or IBD and controls with regard to 90-day complication rates, ER visits, or readmissions. Overall, the 90-day continence rate in our study was 92.9% which is comparable to studies suggesting a continence rate of 80%–90%.23,24 On subgroup analysis, we found that patients with IBS had higher rates of anticholinergic medication use at 3 months and had more encounters with the urology department at 3 months. This reflects our hypothesis that patients with bowel disorders may have more issues with irritative voiding symptoms both preoperatively and postoperatively in the recovery period, though more work will need to be done in this space. One limitation of this study is that only 80% of our control patients (684/858) and 75% of our IBS + IBD patients (45/60) had 90-day clinic follow-up available for analysis. Regardless, managing both bowel and bladder symptoms postoperatively, appropriate anticipatory guidance, and setting expectations are important in reducing patient anxiety and enhancing recovery.
This study does have several limitations, namely its retrospective nature and limited sample size of patients with IBS or IBD. IBS and IBD patients were analyzed both together and separately due to similarities in bowel symptoms but also knowing that IBS and IBD are different disease entities and disease processes. There were not enough patients to do a meaningful analysis of patients with CD and UC. Due to the retrospective nature of data collection, we were not able to analyze with granularity changes within each sub-domain of the AUASS and MISI scores. Another limitation of this study is that we are not able to assess bowel symptom severity, quality, or disease control, which could influence characteristics at presentation as well as recovery outcomes. Future studies should evaluate functional bowel habits to evaluate the effects of bowel dysfunction on HoLEP outcomes more directly.
Conclusion
Functional bowel disorders and bowel diseases such as IBS and IBD are common and there are overlaps between bowel and bladder dysfunction. In our experience, men with IBS who undergo HoLEP for bothersome urinary symptoms are less likely to be catheter dependent at baseline and present with statistically significantly smaller prostate volumes than men without IBS or IBD. While there were no significant differences in rates of SDD, SDTOV, complications, or changes in AUASS and MISI scores, it appears that men with IBS tend to have more difficulty with recovery after HoLEP evidenced by higher rates of anticholinergic medication use and more postoperative encounters.
Supplemental Material
sj-docx-1-tau-10.1177_17562872251317918 – Supplemental material for Do Bowel Disorders Affect Holmium Laser Enucleation of Prostate Outcomes? A Retrospective Cohort Study
Supplemental material, sj-docx-1-tau-10.1177_17562872251317918 for Do Bowel Disorders Affect Holmium Laser Enucleation of Prostate Outcomes? A Retrospective Cohort Study by Kyle Tsai, Perry Xu, Jenny Guo, Nicholas Dean, Nabila Khondakar, Clayton Neill and Amy Krambeck in Therapeutic Advances in Urology
Supplemental Material
sj-docx-2-tau-10.1177_17562872251317918 – Supplemental material for Do Bowel Disorders Affect Holmium Laser Enucleation of Prostate Outcomes? A Retrospective Cohort Study
Supplemental material, sj-docx-2-tau-10.1177_17562872251317918 for Do Bowel Disorders Affect Holmium Laser Enucleation of Prostate Outcomes? A Retrospective Cohort Study by Kyle Tsai, Perry Xu, Jenny Guo, Nicholas Dean, Nabila Khondakar, Clayton Neill and Amy Krambeck in Therapeutic Advances in Urology
Supplemental Material
sj-docx-3-tau-10.1177_17562872251317918 – Supplemental material for Do Bowel Disorders Affect Holmium Laser Enucleation of Prostate Outcomes? A Retrospective Cohort Study
Supplemental material, sj-docx-3-tau-10.1177_17562872251317918 for Do Bowel Disorders Affect Holmium Laser Enucleation of Prostate Outcomes? A Retrospective Cohort Study by Kyle Tsai, Perry Xu, Jenny Guo, Nicholas Dean, Nabila Khondakar, Clayton Neill and Amy Krambeck in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.