
Abstract
Background:
Acute symptomatic seizures (ASYS) is a common presentation in cerebral sinus venous thrombosis (CSVT) patients.
Objectives:
We aimed to characterize CSVT patients experiencing ASYS within 7 days from presentation. Additionaly, we aimed to find predictors for ASYS within CSVT patients.
Methods:
Prospective CSVT databases from six academic centers (January 2010–December 2023) were retrospectively analyzed. Clinical outcomes at the 90-day follow-up included seizure occurrence and the modified-Rankin-Scale (mRS).
Results:
From 529 included patients (mean age 42.4 ± 18.6 years, 64.3% females), 106 (20%) had ASYS. ASYS patients were more often males (47.2% vs 20.1%, <0.001), and presented more often with focal neurological deficits (50% vs 22%, p < 0.001) but less often with papilledema (13.2% vs 29.3%, p < 0.001). On multivariate analysis cortical-vein thrombosis (odds ratio (OR) 4.17, p < 0.001), intracerebral hemorrhage (ICH; OR 3.06, p = 0.002), any superior-sagittal-sinus (SSS) thrombosis (OR 2.49, p = 0.006), predicted ASYS. Conversely, presentation with papilledema (OR 0.39, p = 0.03) negatively predicted ASYS. ASYS patients had lower rates of 90-day-mRS-0-1 (51.9% vs 83.9%, p < 0.001). Patients who experienced seizures between the second and seventh day (n = 58) had similar baseline characteristics to those with seizures only on the day of presentation (n = 48) but were less likely to achieve a good functional outcome by day 90 (42.6% vs 58.9%, p < 0.05) and had a lower rate of complete recanalization on follow-up venous imaging (25.5% vs 57.5%, p = 0.02). Status-epilepticus in comparison to non-ASYS patients achieved lower rates of 90-day-mRS-0-1 (11% vs 84%, p < 0.001) and higher 90-day-mortality (44% vs 5.6%, p < 0.001). In a multivariate analysis ASYS was a negative predictor for 90-day-mRS-0-1 (OR 3.3, 95% confidence interval 1.43–7.5, p = 0.005).
Conclusion:
CSVT patients experiencing ASYS, and to a greater degree patients with either status epilepticus or ASYS between second and seventh day achieved less often 90-day-mRS-0-1. Possibly, they epitomize a different course of disease that may require a more suitable treatment strategy.
Plain language summary
Some people with cerebral sinus venous thrombosis (CSVT) experience seizures within the first week of their symptoms. These are called acute symptomatic seizures (ASYS).
Objective:
We wanted to understand which CSVT patients are more likely to have ASYS and identify factors that could predict these seizures.
Methods:
We analyzed data from six hospitals, covering CSVT cases from 2010 to 2023. We looked at patient outcomes after 90 days, including whether they had seizures and how well they recovered (measured by a scale called the modified Rankin Scale, or mRS).
Results:
Out of 529 patients (average age 42, mostly women), 106 (20%) had ASYS. Patients with ASYS were more likely to be men and to have specific neurological issues, but they were less likely to have swelling of the optic nerve (papilledema). Certain factors increased the risk of ASYS, including blood clots in specific veins of the brain and brain bleeds. On the other hand, having papilledema made ASYS less likely. Patients with ASYS were less likely to have a good recovery after 90 days (52% vs. 84% of those without ASYS). Those who had seizures between days 2 and 7 after symptoms started had worse recovery outcomes and were less likely to have their blood clots fully dissolve. Patients who had a severe type of seizure called status epilepticus had even worse outcomes, including higher death rates (44% vs. 5.6%).
Conclusion:
Patients with ASYS—especially those with status epilepticus or seizures after the first day—tended to have worse recovery. This suggests they may have a more severe form of the disease and might need different treatment approaches.
Introduction
Although CSVT accounts for only 0.5%–1% of all strokes, it usually affects younger patients than those with arterial types of stroke with a median age of 37 years. 1 Unlike arterial stroke, seizures are one of the important presenting features of cerebral sinus venous thrombosis (CSVT) patients affecting around 20%–40% of patients, which may experience seizures in the early stage of the disease.2 –4 It may present as focal or generalized acute symptomatic seizures (ASYS), depending on the location and extent of the underlying pathology.
While early studies found ASYS to be associated with early death among CVST patients 5 (ferro 2003), recent multicenter cohorts did find that ASYS predicted poor prognostic outcomes.3,6 Moreover, an MRI-based study of CSVT patients found no specific brain parenchymal lesion in those with an ASYS that was independently associated with poor functional outcomes. 4 The pathophysiology of ASYS in CSVT is multifactorial, involving cortical irritation from ischemia, brain edema associated with increased ICP, and hemorrhagic infarction. Patients with cortical vein thrombosis and hemorrhagic infarctions are particularly prone to developing seizures. 3 Seizures in CSVT patients may worsen prognosis by increasing metabolic demand, causing further neuronal injury, and contributing to a higher risk of long-term complications such as epilepsy. 7 Possibly, early identification and management of ASYS may prevent further neurological deterioration and improve patient outcomes. Therefore, we aim to investigate the clinical predictors and outcomes of CSVT patients with ASYS. We assume that CVST patients presenting with ASYS will have more often parenchymal involvement sequentially resulting in worse prognostic outcomes. Furthermore, we assume that ASYS CSVT patients who develop status epilepticus or continue to have seizures despite first-line antiepileptic treatment, experience a more severe disease course, leading to poorer prognostic outcomes.
Methods
The dataset
A retrospective analysis was performed on a dataset including patients diagnosed with CSVT from six comprehensive stroke centers between 1/2010 and 12/2023. The dataset was collected in an ongoing prospective manner. We included in this analysis patients diagnosed with CVST aged 18 and above, excluding cases in which CSVT was secondary to head trauma, otolaryngeal, or neurosurgical procedures. Data regarding patient demographics, possible etiologies, comorbidities, and vascular risk factors were recorded. We have used the STROBE 8 guidelines for multicenter cohort observational studies while preparing the manuscript.
CSVT diagnosis
The diagnosis of CSVT in all included cases was based on cerebrovascular imaging (CT venography, MR venography, or digital subtraction angiography). These were interpreted by both an experienced neuroradiologist and an experienced stroke neurologist. The side and location of the occluded venous channels were reported and scored as following: 1 (superior sagittal sinus (SSS)), 2 (cortical vein), 3 (transverse and sigmoid sinus either with or without jugular), 4 (cavernous sinus), and 5 (deep venous system). The deep venous system was defined to include the internal cerebral veins (veins of Galen and Rosenthal). Multiple vein/sinus involvement was defined as involvement of more than one site according to the above vein scores. The presence of intracerebral hemorrhage (ICH) was determined from admission noncontrast CT. Patients underwent a thorough investigation according to similar institutional protocols.
ASYS definition
Like a recent multicenter study 3 ASYS was defined as any seizure that occurred between symptom onset and 7 days after diagnosis of CSVT. 9
Status epilepticus definition
We defined status epilepticus as continuous tonic-clonic seizure activity for 5 min or more, focal status epilepticus with impaired consciousness was defined if it lasts 10 min or more. Furthermore, we defined status epilepticus if multiple seizures occurred within 30 min without normalization of consciousness in-between. 10
Additional medical data
In all patients, a complete blood count, routine blood biochemistry, and coagulation profiles were performed. The following investigations were conducted.
Hematological workup and hypercoagulability evaluation
Routine laboratory screening for hypercoagulable states included tests for protein C, protein S, antithrombin III, factor V Leiden, homocysteine, and antibodies to anticardiolipin, beta-2 glycoprotein 1, and Lupus anticoagulant (LAC) were taken upon CSVT diagnosis. Laboratory criteria for antiphospholipid syndrome were defined by at least two positive tests performed at least 12 weeks apart. Tests included lupus anticoagulant (LAC) Russel viper venom time (RVVT) ratio >1.2, LAC Silica clotting time (SCT) >1.23, IgG/IgM anticardiolipin antibodies, and/or IgG/IgM anti-β2-glycoprotein I antibodies ELISA value above 40 units. In patients with thrombocytosis of unknown cause (platelet count >450,000/µL) or unexplained polycythemia (hemoglobin >18 g/dL for males and >16 g/dL for females), genetic analysis for JAK2-V617F mutation was performed.
Rheumatological assessment
A rheumatologic questionnaire was completed for all patients, documenting any history of arthritis, arthralgia, rash, oral or genital ulcers, and uveitis. Further rheumatologic investigations, including a full rheumatological laboratory workup, were performed when clinically indicated. Pathergy testing and genetic screening for HLA-B27 and HLA-B51 were conducted when Behçet’s disease was suspected.
Neoplastic investigation
In patients with CVST of unknown etiology, a panel of neoplastic markers was measured, including prostate-specific antigen, cancer antigen 125 (CA 125), carcinoembryonic antigen, carbohydrate antigen 19-9 (CA19-9), alpha-fetoprotein, and human chorionic gonadotropin. For patients aged ⩾50 years, chest, abdomen, and pelvis CT scans were also performed.
Follow-up data
Follow-up neuroimaging of either computed tomography venography (CTV) or magnetic resonance venography (MRV) of head was performed 3 months postadmission. Similar to previous definitions, 11 degree of recanalization, when specified, was classified as none, partial, or complete. Any recanalization was regarded as the combination of both partial and complete recanalization. Patient follow-up included a 3- and 12-months postadmission visit at the stroke prevention clinics of the participating centers. Functional independence on follow-up was graded using the modified Rankin Score (mRS). 12 The mRS ranges from 0 to 6, with lower scores indicating better functional status. mRS of 0 signifies that the patient has no residual deficits or symptoms from the stroke and is fully independent. mRS of 1 signifies that the patient has no significant disability despite symptoms and is able to carry out all usual duties and activities. Favorable outcome was defined as mRS 0–1 on 90-day follow-up. Late seizures were defined as any seizure beyond the first week from admission.
Statistical analysis
In the current analysis, we compared data for CVST patients with and without seizures in the early phase of the disease. Statistical analysis was performed with SPSS version 25 (IBM, Chicago, IL, USA). The two-sample Student’s t test was applied to test differences between the study groups for quantitative parameters. Nonparametric tests were used for the comparison of medians with interquartile ratios. Pearson’s Chi-square or Fisher’s exact tests were applied for testing the differences between the groups for the categorical parameters. A p value ⩽0.05 was considered statistically significant. Multivariate logistic regression models controlling for age, sex, venous infarction, and all variables that yielded a p < 0.05 were used to control possible confounders.
Using univariate analysis, we aimed to characterize the ASYS CSVT cohort. Additionally, multivariate logistic regression models were employed to identify predictors of ASYS and to determine whether ASYS serves as a negative predictor of favorable outcomes (mRS 0–1 at 90-day follow-up).
Ethical approval
Local institutional review boards approved the study with an exception from obtaining individual informed consent forms due to the anonymized nature of data collection and the retrospective analysis of data.
Results
Clinical characteristics of ASYS patients
A total of 529 CVST patients were included in the study (mean age: 42.8 ± 18.9 years; 74% female). Among them, 106 patients (20%) experienced ASYS within the first week of admission. Of these, 88 patients (83%) had ASYS on the first day of admission, while the remaining 18 patients experienced their first ASYS between the second and seventh day of admission. Although antiepileptic treatment was administered to all patients presenting with ASYS on the first day, nearly half (40/88, 45.4%) experienced additional seizures during the first week.
Of the 106 patients, 96 (90.6%) were discharged from the index admission on antiepileptic treatment, as per the discretion of the treating neurologist.
CSVT patients with ASYS had higher rates of male sex (47.2% vs 20.1%, p < 0.001), hypertension (19.8% vs 12.3%, p = 0.045), and diabetes (14.1% vs 7.3%, p = 0.026; Table 1). Notably, all CSVT predisposing conditions had no interaction with ASYS apart from Bechet’s disease patients who did not experience ASYS (n = 21, 5% vs 0%, p = 0.019). Similarly, hematological workup did not reveal significant differences between groups except for prothrombin 20210A mutation being more prevalent in the ASYS group (11.3% vs 3.1%, p < 0.001). The clinical presentation of CSVT patients with ASYS revealed significantly lower rates of papilledema (13.2% vs 29.3%, p < 0.001) and headache (63.2% vs 80.1%, p < 0.001). However, CSVT patients with ASYS had higher rates of focal neurological deficit (50% vs 22.5%, p < 0.001), higher admission National Institutes of Health Stroke Scale scores (3.9 vs 1.8, p < 0.001), and more frequent vomiting (26.4% vs 17.5%, p = 0.039).
Comparison between CVST with and without ASYS.

Values represent the number of patients unless otherwise stated. Statistically significant p values are in bold.
ASYS, acute symptomatic seizures; IQR, interquartile range; JAK2, Janus kinase 2; MTHFR, methylenetetrahydrofolate reductase; NIHSS, National Institutes of Health Stroke Scale.
Radiological characteristics of ASYS patients
ASYS CSVT patients exhibited higher rates of cortical vein involvement (28.3% vs 8.7%, p < 0.001), venous infarction (36.8% vs 9.4%, p < 0.001), ICH (42.5% vs 11.1%, p < 0.001), and isolated SSS involvement (59.4% vs 32.4%, p < 0.001) as compared to patients without ASYS. Conversely, ASYS CSVT patients had less often sigmoid sinus involvement (48.1% vs 70.7%, p < 0.001) or transverse sinus involvement (52.8% vs 73.8%, p < 0.001).
Prognostic outcomes
Clinical outcome on 90-day follow-up was worse among ASYS CSVT patients achieving a lower rate of favorable outcome (51.9% vs 83.9%, p < 0.001) and a higher chance for remote seizures despite receiving antiepileptic medication (7.5% vs 5%, p < 0.001). Mortality rates remained low and were comparable between groups.
A comparison was made between the 88 ASYS patients (83%) who experienced seizures on the first day of admission and 18 ASYS patients whose first seizure occurred between the second and seventh day of admission. Patients with seizures on the first day demonstrated a trend toward a better 90-day functional outcome (80% vs 58%, p = 0.06) and significantly lower 90-day mortality (3.4% vs 17.6%, p = 0.022).
Overall, 58 ASYS patients experienced seizures between the second and seventh days of admission. This group included 18 patients with their first seizure during this period and 40 patients who had an initial seizure on the first day but experienced additional seizures despite antiepileptic treatment. These 58 patients were compared to 48 ASYS patients who experienced seizures only on the first day of admission without subsequent episodes. Patients with seizures occurring between the second and seventh day had similar baseline characteristics but were less likely to achieve by day-90 a good functional outcome (42.6% vs 58.9%, p < 0.05) and complete recanalization on repeated venous imaging (25.5% vs 57.5%, p = 0.02).
Status epilepticus
Nine patients experienced status epilepticus within the first week of admission (Table 2). In comparison to CVST patients who did not experience ASYS, status epilepticus patients suffered more often from hypertension (66.7% vs 12.1%, p < 0.001), diabetes (55.6% vs 7.3%, p < 0.001), and hyperlipidemia (44.4% vs 14.4%, p = 0.013). Also, their initial radiological workup had higher rates of ICH (55.6% vs 11.1%), venous infarction (44.4% vs 9.4%), and cortical vein thrombosis (44.4% vs 8.7%; p < 0.001 for all). Unfortunately, prognostic outcomes were poor for status epilepticus patients. In comparison to patients without ASYS, they had lower rates of favorable functional outcome (11% vs 84%), mRS-90 (3 (IQR) vs 0 (IQR)), and higher mortality rates (44% vs 5.6%; p < 0.001 for all).
Comparison between CVST patients with status epilepticus and patients without ASYS.
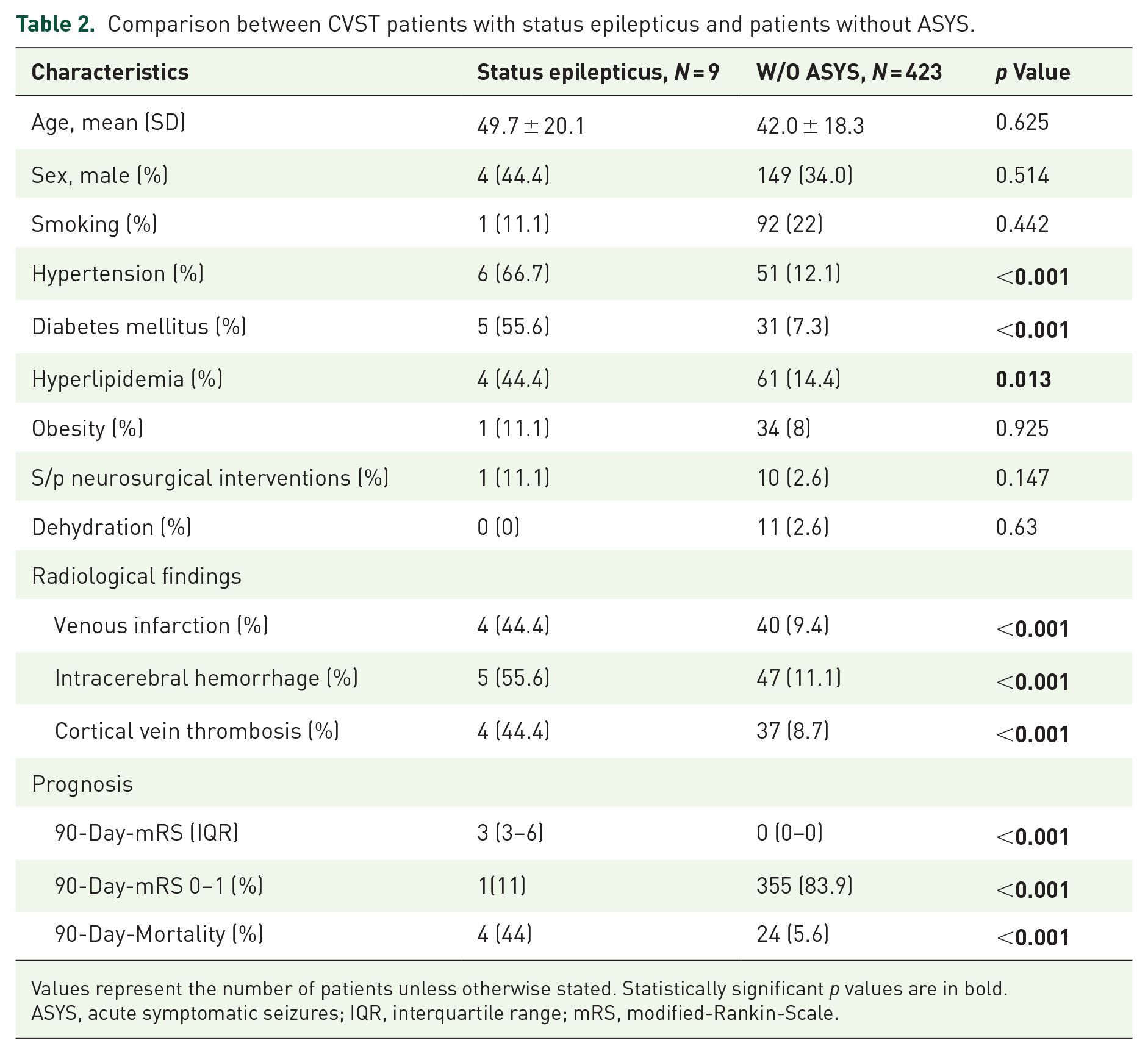
Values represent the number of patients unless otherwise stated. Statistically significant p values are in bold.
ASYS, acute symptomatic seizures; IQR, interquartile range; mRS, modified-Rankin-Scale.
Multivariate analysis models
A multivariate logistic regression model was used to assess possible predictors for ASYS (Table 3). We found that cortical vein involvement (odds ratio (OR) 4.17, p < 0.001), ICH (OR 3.06, p = 0.002), and any SSS thrombosis (OR 2.49, p = 0.006), predicted ASYS. Conversely, papilledema upon presentation negatively predicted ASYS (OR 0.39, p = 0.03).
Multivariate analysis for predictors of acute symptomatic seizure.

Statistically significant p values are in bold.
ICH, intracerebral hemorrhage; OR, odds ratio; PT, prothrombin; SSS, superior sagittal sinus.
An additional multivariate logistic regression model was used to assess possible predictors for worse functional outcome 90-day-mRS-2-6 (Table 4). Neurological deficit upon presentation (OR 4.4, 95% confidence interval (CI) 2.1–9.3, p < 0.001), ASYS (OR 3.3, 95% CI 1.43–7.53, p = 0.005), diabetes mellitus (OR 3.17, 95% CI 1.13–8.94, p = 0.029), and increasing age (OR 1.05, 95% CI 1.03–1.07, p < 0.001) were all independent predictors of worse functional outcomes. Conversely, headache upon presentation showed a negative tendency to predict worse functional outcomes (OR 0.47, 95% CI 0.21–1.05, p = 0.066).
Predictors of worse functional outcome 90-day-mRS-2-6.

Statistically significant p values are in bold.
mRS, modified-Rankin-Scale; OR, odds ratio; SSS, superior sagittal sinus.
Discussion
The occurrence of ASYS in our cohort was 20% and somewhat lower than the rates reported in other large cohorts (25%–30%).3,5,7 Notably, in contrast to the other large cohorts, our registry included only patients from more recent years (after 2010). Possibly, through higher awareness and more advanced imaging techniques our cohort-included patients with a more subtle clinical and radiological presentation of CVT were diagnosed thereby explaining the lower rate of ASYS in our cohort. Alternatively, earlier diagnosis and treatment may lead to lower rates of ASYS. Status epilepticus occurred in 1.7% of all CSVT patients and in 8.5% of patients with ASYS. Our findings are comparable to several previous studies that reported consistent findings of status epilepticus in CSVT ranging from 0.5% to 11% among all CSVT patients and 1% to 22% among patients with ASYS.2,5,6,9 Similar to the other large cohorts,3,13 as well as two extensive systematic reviews,14,15 age and sex were not independent predictors of ASYS.
In our study, independent predictors of ASYS were cortical vein involvement (OR 4.2), ICH (OR 3), and SSS involvement (OR 2.5). Our findings corroborate those observed in previous studies3,7 and systematic review 14 pointing out at those three variables as the main predictors of ASYS. This could be explained by proximity of the cortical veins to the cortical surface areas that are highly sensitive to electrical excitability and ischemic changes, both of which can trigger seizure activity. Finally, SSS involvement could lead to severe venous outflow obstruction and increased intracranial pressure, with localized edema with either secondary ischemic or hemorrhagic damage on the cortical areas, 11 which are known to increase the risk of ASYS.2,3
ICH has been consistently found as an independent predictor of ASYS in stroke patients in general 16 and in CVST patients in particular.2,3,17 It can increase the risk of ASYS through several mechanisms. The expansion of ICH and perihematomal edema compress adjacent brain structures, causing both displacement and inflammation. 18 Moreover, the release of irritants from blood products such as hemoglobin degradation (iron, methemoglobin, and hemosiderin) or thrombin may irritate cortical neurons and glial cells and disruption of ionic balance and excitotoxicity due to elevated glutamate.19,20
In contrast, papilledema was independently found as a negative predictor of ASYS (OR 0.39, p = 0.3). To the best of our knowledge, this predictor was not reported in the past. Previous study on the development of papilledema in CVST patients suggested a longer period from symptom onset to diagnosis thereby representing a more gradual increase in intracranial pressure. 21 Different courses of disease presentation and progression have been previously described. For example, a previous study looking at CVST without headache found higher rates of parenchymal lesions and seizures while CVST patients with headache had higher rates of papilledema. 22 Therefore, we presume that a pattern of dural sinus thrombosis without parenchymal lesions but with papilledema and possibly are less likely to experience seizures in contrast to a pattern with supratentorial cortical lesions.17,23
Our findings show that CVST patients with ASYS and to a greater degree with epilepticus status achieved less often excellent functional outcomes. Moreover, ASYS has been found as an independent predictor of worse functional outcome. However, the association of worse prognosis was not found in all studies, 3 and it was described in certain subpopulation such as pediatric 24 and Chinese. 25 Presumably, different underlying seizure pathophysiology, such as extent of parenchymal damage or additional infectious process may both reduce epileptic threshold and independently play a major role on prognostic outcomes. Alternatively, the poorer functional outcomes observed in ASYS patients may be partly attributed to their higher prevalence of baseline diabetes mellitus and hypertension. Admission hyperglycemia has been identified as an independent predictor of worse outcomes, 26 while chronic hypertension has been independently associated with an increased risk of hemorrhagic parenchymal involvement in CSVT patients, 17 ultimately contributing to poorer functional recovery. Although we adjusted in a multivariate model for the presence of diabetes mellitus and hypertension, we did not adjust for the severity of the diabetes as measured by HBA1C levels.
Notably, ASYS patients who experienced seizures between the second and seventh day were less likely to achieve a good functional outcome or complete recanalization by day 90, as observed on repeated venous imaging. This group included patients who developed seizures despite antiepileptic therapy, potentially indicating an aggravation of the cortical lesion and resulting epileptic activity. Similarly, in the largest study of ASYS CSVT patients, patients with postdiagnosis ASYS were more likely to have cortical lesions on imaging. 3 Possibly, patients who experienced their first ASYS during this period, despite anticoagulation therapy, may reflect challenges in early thrombus degradation and worsening focal edema. 27 The relatively low rates of complete recanalization in this unique group further suggest the presence of clots that are less responsive to anticoagulation treatment.
ASYS occurrence in CVST patients raises several concerns. Primarily, as CVST patients are anticoagulated, the risk of a seizure accompanied by trauma is alarming. Moreover, the risk of developing status epilepticus with its possible complications should be carefully assessed. More informed risk stratification may prompt higher levels of suspicion for possible ASYS that have a more subtle neurological presentation. Proper patient selection to either continuous video EEG monitoring or admission to a unit with a higher level of neurocritical care may aid in identification of subtle ASYS. As possibly, one may consider AED in high-risk patients with evidence of epileptiform activity.
Currently, prophylactic AED treatment in the acute presentation has not been recommended by both the European Stroke Organisation and the American Stroke Association guidelines.13,28 Thus, the decision-making regarding time, type, dosage, and duration of antiepileptic treatment in patients with CVST is often individualized. 29 The recently published validated scale predicting post CSVT epilepsy may aid decision-making. 30
Our study has several limitations. As a retrospective analysis, data collection was not uniform, with variations in recording the time from symptom onset and antiepileptic treatment details. Additionally, data were gathered from multiple centers, leading to potential differences in diagnostic and treatment approaches. For instance, because MRI was not routinely performed upon initial admission, our assessment of brain parenchymal lesions may be limited. Furthermore, decisions regarding antiepileptic treatment were based on the clinical judgment of individual stroke neurologists at each center, introducing variability. Finally, our study included a limited number of patients with status epilepticus, preventing the identification of predictors for its development. As a result, we did not assess whether any of these patients met the criteria for refractory or super-refractory status epilepticus. 31 Given these limitations, further prospective studies involving larger, well-characterized cohorts of ASYS CVST patients with status epilepticus are needed to improve our understanding of this condition.