
Abstract
Background:
In multiple sclerosis (MS), the educational gradient in diagnostic and disease-modifying treatment (DMT) delays is sparsely examined, and the results are mixed.
Objectives:
Among patients with relapsing-remitting MS (RRMS), we aimed to examine the educational gradient in diagnostic delay and delay in the initiation of the first DMT.
Design:
A nationwide cohort study.
Methods:
We linked the Danish Multiple Sclerosis Registry with other nationwide registries. Diagnostic delay was evaluated in 4344 patients ⩾20 years at clinical onset with clinical onset from January 1, 2012, onwards, diagnosed by March 1, 2023. DMT delay was evaluated in 5402 patients ⩾20 years at MS diagnosis who were diagnosed from January 1, 2012, to March 1, 2022, with DMT initiation follow-up until March 1, 2023. The highest completed education before onset and diagnosis, respectively, was categorized using the International Standard Classification of Education (ISCED) into low (ISCED 0–2), medium (ISCED 3–4) and high (ISCED ⩾5) education. Endpoints were categorized according to their duration into four groups based on a population-specific quartile split. The highest quartile comprised long duration (⩾500 days (diagnostic delay) and ⩾76 days (DMT delay)). We calculated crude and adjusted odds ratios (OR) with 95% confidence intervals (CI).
Results:
The mean age was 36.7 years (SD = 10.3, diagnostic delay population) and 39.2 years (SD = 10.9, DMT delay population). Most were female (67.4% and 68.3%) and of Danish origin (90.3% and 90.5%). Patients with low educational attainment did not have higher odds of diagnostic delay (OR = 1.05; 95% CI: 0.81–1.35) but had higher odds of DMT delay (OR = 1.48; 95% CI: 1.17–1.87) compared to patients with high educational attainment.
Conclusion:
In adult patients with RRMS, low educational attainment was associated with higher odds of DMT delay but not diagnostic delay. Targeted interventions are needed to address educational disparities in healthcare access and treatment initiation.
Plain language summary
Social determinants may influence health outcomes in multiple sclerosis. Education is an important social determinant established in early adulthood. Timely diagnosis and early treatment with disease-modifying treatment (DMT) is crucial in relapsing-remitting MS (RRMS). Among patients with RRMS, we hypothesized that low educational attainment would be associated with higher odds of diagnostic delay and delay in initiating the first DMT after diagnosis. We linked individual-level data on patients with RRMS from the Danish Multiple Sclerosis Registry with other nationwide registries from 2012 to 2023. Based on the International Standard Classification of Education, we assessed educational attainment as the highest completed education. Endpoints were categorized according to their duration into four groups based on a population-specific quartile split. We calculated multivariable-adjusted odds ratios with 95% confidence intervals. In adult patients with RRMS, low educational attainment was associated with higher odds of DMT delay but not diagnostic delay. Targeted interventions are needed to address educational disparities in healthcare access and treatment initiation.
Introduction
Social determinants of health are non-medical but may influence health outcomes both overall1,2 and in multiple sclerosis (MS) 3 in terms of moderating negative impact of pathological brain changes on cognition 4 access to treatment, 5 risk of disability progression6–8 and mortality.9,10 Education is an important social determinant established in adolescence or early adulthood. Other social determinants include, for example, income, access to food, housing and health care.1,2
Pathways through which education impacts general and brain health are not fully understood 3 but may include employment, income, health behaviours and health literacy, which enables individuals to make informed decisions about their health and navigate the healthcare system effectively. Timely diagnosis and early treatment with disease-modifying treatment (DMT) after diagnosis are crucial in improving the prognosis and delaying disability progression in patients with MS.11,12
In privately funded healthcare systems, patients with MS with higher education have been shown to have better access to DMT. 13 However, recent studies based on data from publicly funded healthcare systems have shown mixed results about access to DMT.14,15 A population-based cohort study from the south-eastern part of Norway reported that access to DMT did not depend on the educational level of patients with MS. 14 In contrast, a community-based study using the UK MS Register found that university education was associated with a higher DMT uptake. 15 Neither of the two studies were nationwide, and the UK MS registry-based study was further limited by relying on self-reported education data.
Denmark’s healthcare system is publicly funded, and the Danish Medicines Council sets out guidelines for the uniform treatment of MS. 16 Data recording on patients with MS treated with DMT has been mandatory since DMT became available in 1996, and health authorities use these data as clinical quality indicators for the national monitoring of MS treatment in Denmark. 17
In this study, we aimed to examine the educational gradient in diagnostic and DMT delays in MS based on Danish clinical near-complete MS data linked with other nationwide registries. Among patients with relapsing-remitting MS (RRMS), we hypothesized that low educational attainment compared to high would be associated with higher odds of diagnostic delay and delay in initiation of the first DMT.
Methods
Study design and population
We conducted a contemporary nationwide cohort study in Denmark linking the Danish Multiple Sclerosis Registry (DMSR), 18 a nationwide clinical registry, with other nationwide administrative registries, to obtain information on educational attainment and migration background.19–21
The DMSR includes information on all patients diagnosed with MS by a neurologist in 1 of the 13 MS clinics in Denmark. The MS clinics are run by public hospitals and are the only ones allowed to prescribe and dispense DMTs. Since 1996, data collection during regular clinical visits has been mandatory for patients receiving DMTs. When a new patient is recorded in the DMSR, the time and type of clinical onset are recorded retrospectively. The definition of the time of MS diagnosis is the date of communicating the MS diagnosis to the patient. The diagnostic criteria used was the 2010 and the 2017 revisions of the McDonald criteria,22,23 and we enrolled patients in the two study populations with clinical onset and with MS diagnosis, respectively, after 2011. The data cut-off in this study was March 1, 2023, for both populations.
For the diagnostic delay analyses (population #1, n = 4344), we included all patients with RRMS who had a clinical onset date after December 31, 2011, and who were ⩾20 years old at clinical onset with complete information on education (95 patients did not have information on education and were excluded).
For the DMT delay analyses (population #2, n = 5402), we included all patients with RRMS diagnosed after December 31, 2011, until March 1, 2022, who were ⩾20 years old at diagnosis. This approach ensured a follow-up of at least 1 year for initiation of the first DMT after MS diagnosis. In total, 85 patients were excluded due to a lack of information on education.
The reporting of this study conforms to STROBE guidelines. 24
Assessment of educational attainment
Using the Danish education register20,25 including yearly updated educational information on all people residing in Denmark, we assessed educational attainment as the highest completed education. We assessed educational attainment as the highest completed education before clinical onset for the diagnostic delay analyses. For the DMT delay analyses, we assessed educational attainment as the highest completed education before diagnosis. Based on the International Standard Classification of Education (ISCED), 26 we categorized patients into groups of low (primary and lower secondary, ISCED level 0–2), medium (upper secondary and postsecondary, ISCED level 3–4) and high educational attainment (first- and second-stage tertiary, ISCED 5 or higher). ISCED, first developed in the 1970s and revised in 1997 and 2011, comprises uniform and internationally agreed definitions to make educational systems comparable across countries. ISCED was adopted by the UNESCO General Conference in 2011. 26
Assessment of diagnostic and treatment delay
The assessment of diagnostic and DMT delays were preselected. We used the DMSR 18 to calculate the number of days from the clinical onset date to the diagnosis date and the number of days from the diagnosis date to the date of initiation of the first DMT. DMTs in this study included ofatumumab, teriflunomide, interferon beta-1a, glatiramer acetate, interferon beta-1b, fingolimod, stem cells transplantation, alemtuzumab, rituximab, cladribine, mitoxantrone, ocrelizumab, peginterferon, human immunoglobulin, dimethyl fumarate, treosulfan, natalizumab, daclizumab, mycophenolate mofetil, siponimod and ozanimod. The DMT definition in this study also included when the treatment strategy was actively chosen to be that of no DMT (n = 103 patients) or symptomatic treatment with fampridine (n = 23) as a proxy for treatment decision.
We categorized each of the two measures into four groups based on a quartile split of the distribution within the study population #1 and #2, respectively, to examine the effect of educational attainment on different durations of time from clinical onset to diagnosis and from diagnosis to the first DMT.
The difference in days from the clinical onset date to the diagnosis date in categories was ‘very short duration’ (0–60 days), ‘short duration’ (61–183 days), ‘medium duration’ (184 to (496–499) days) and ‘long duration’ ((500–504) to (>3651) days). The ranges are reported instead of exact numbers due to data protection regulations, where at least five individuals are required within a category to report the data.
The difference in days from the diagnosis date to the DMT initiation date in categories was ‘concurrent’ (0–7 days), ‘short duration’ (8–28 days), ‘medium duration’ (29–75 days) and ‘long duration’ (76 to (>2934) days). In addition to the four categories of different durations from the diagnosis date to the DMT initiation date, we added one category of patients comprising those not initiating a DMT until the end of follow-up (n = 314).
Covariates
Covariates were assessed at baseline and included age and calendar year of clinical onset or diagnosis, respectively (continuous variables), sex (female, male) and migration background (Danish origin (the whole population in Denmark except immigrants and descendants of immigrants); immigrants (born abroad and none of the parents were either Danish citizens or born in Denmark); descendants of immigrants (born in Denmark and none of the parents were either Danish citizens or born in Denmark)).
Statistical analyses
Baseline characteristics of the two study populations were reported as frequencies and proportions (categorical variables) and as mean and standard deviations (SD) or median and interquartile range (IQR) (continuous variables).
We analysed the association between educational attainment and diagnostic and DMT delay, respectively, using multinomial logistic regression models contrasting each response level against the reference level specified as the category with the shortest duration of days. We used the logistic procedure in SAS 9.4 to estimate odds ratios (OR) and 95% confidence intervals (CI) for the association between educational attainment at baseline and subsequent duration of time in categories to diagnosis or DMT initiation, respectively. We estimated crude ORs and 95% CIs, and ORs and 95% CIs adjusted for age, sex, migration background and calendar year of clinical onset or diagnosis, respectively.
In supplementary analyses, we explored whether the results from the main analyses differed when stratified by age groups and sex and while including patients only with clinical onset date and diagnosis date, respectively, after 2013, at which time oral DMTs became more widely available.
Finally, we divided study population #2 into two groups according to whether the patients had initiated a DMT before the data cutoff date. Differences between study population #2 subgroups were tested using the χ2 and two-sample t-test.
Power calculations were not performed before conducting the study, as we aimed to include all patients in DMSR according to eligibility criteria in the study population.
Results
Clinical and demographic characteristics at baseline
Study population #1 (Table 1) comprised 4344 patients, of whom 67.4% were female (n = 2929) and 90.3% were of Danish origin (n = 3921). The mean age at clinical onset was 36.7 years (SD = 10.3), and the median clinical onset year was 2017 (IQR: 2014–2019). The proportions of patients in educational attainment groups were 17.2% (n = 745, low), 44.4% (n = 1929, medium) and 38.4% (n = 1670, high).
Characteristics of the study population #1 at the time of clinical onset and study population #2 at the time of diagnosis.
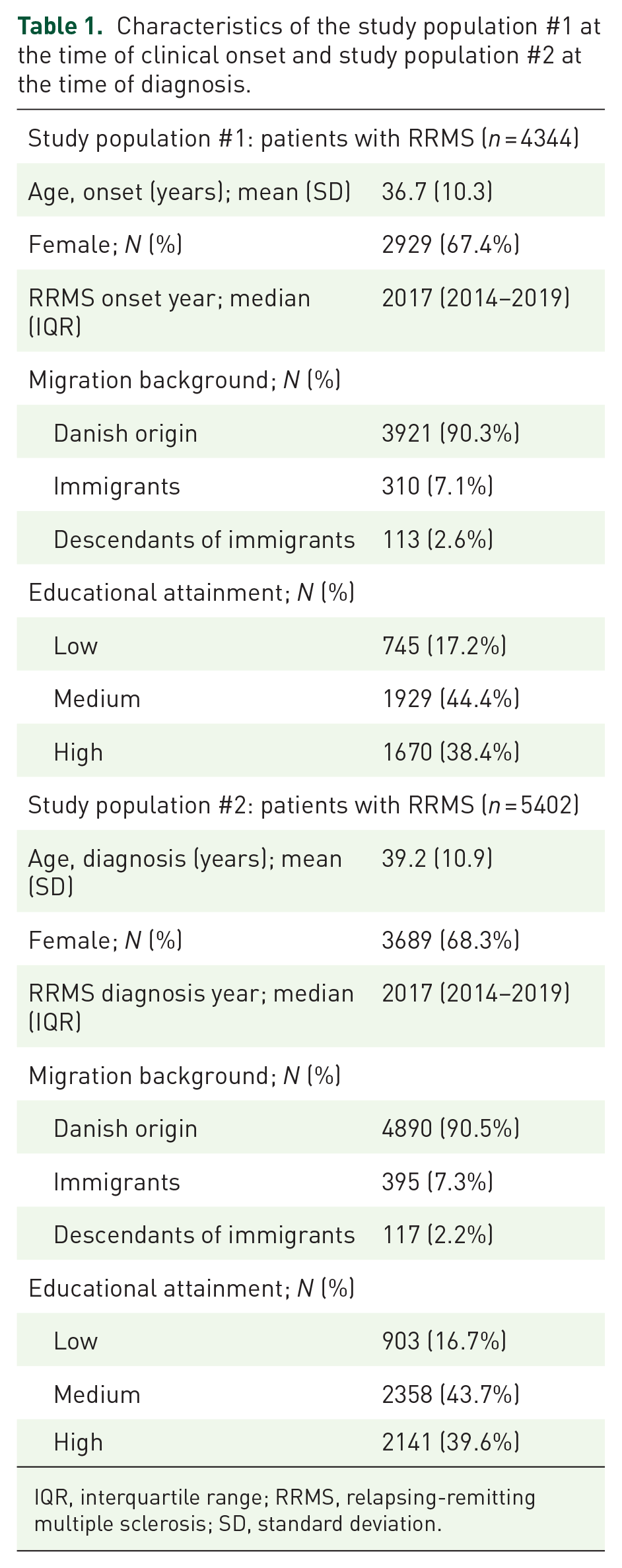
IQR, interquartile range; RRMS, relapsing-remitting multiple sclerosis; SD, standard deviation.
Study population #2 (Table 1) comprised 5402 patients, of whom 68.3% were female (n = 2929) and 90.5% were of Danish origin (n = 4890). The mean age at diagnosis was 39.2 (SD = 10.9), and the median year of diagnosis was 2017 (IQR: 2014–2019). The distribution in educational attainment groups was 16.7% (n = 903, low), 43.7% (n = 2358, medium) and 39.6% (n = 2141, high).
Educational attainment and duration from clinical onset to diagnosis
Results are shown in Table 2 and were modelled contrasting each response level against ‘very short duration’ which was specified as the reference category. Compared to high educational attainment, neither low nor medium educational attainment was associated with higher odds of short, medium or long duration from clinical onset to diagnosis with adjusted OR of OR = 1.05 (95% CI: 0.81–1.35, low education, long duration) and OR = 1.00 (95% CI: 0.82–1.21, medium education, long duration).
Crude and adjusted OR of different durations from clinical onset to diagnosis according to educational attainment.

Multinomial logistic regression model, ‘Very short duration’ was specified as the reference category. Adjusted OR is adjusted for sex, age, year of MS onset and migration background.
CI, confidence interval; OR, odds ratio.
Educational attainment and duration from diagnosis to DMT initiation
Results are shown in Table 3 and were modelled contrasting each response level against ‘concurrent’ which was specified as the reference category. Compared to high educational attainment, low educational attainment was associated with higher odds of long duration from diagnosis to DMT initiation both in the unadjusted (OR = 1.55; 95% CI: 1.23–1.95) and in the adjusted model (OR = 1.48; 95% CI: 1.17–1.87). Low educational attainment was not associated with higher odds of short or medium duration from diagnosis to DMT initiation. There were probable associations between low education and not initiating a DMT, but the results were not statistically significant. Estimates for medium educational attainment all included unity.
Crude and adjusted OR of different durations from diagnosis to DMT initiation according to educational attainment.

Multinomial logistic regression model, ‘Concurrent’ was specified as the reference category. Adjusted OR is adjusted for sex, age, year of MS diagnosis and migration background. Statistically significant results are printed in bold.
CI, confidence interval; DMT, disease-modifying treatment; OR, odds ratio.
Supplemental analyses
Clinical onset to diagnosis
All estimates for associations between educational attainment at clinical onset and subsequent duration of time to diagnosis included unity and were similar to results from the main analyses (data shown in Tables S_1a–S_3).
Diagnosis to DMT initiation
Results were similar when including patients only with diagnosis date after 2013; however, estimates were slightly stronger, and the estimate for low education and not initiating DMT reached statistical significance. Stratified by sex, point estimates were similar, but male patients’ results lost statistical significance. Point estimates for low education and long duration were similar by age groups, but the tendency towards higher odds of not initiating a DMT in the low educational group was seen only in the younger age group. In that group, the result for low education and long duration lost statistical significance (data shown in Tables S_4a–S_6).
Patients who had initiated versus not initiated a DMT at the data cutoff
Compared to patients who had initiated a DMT (n = 5088), patients who had not initiated a DMT (n = 314) were older, and a higher proportion of them had low educational attainment as their highest completed education (Table 4).
Patients with RRMS who had initiated versus not initiated a DMT at data cutoff date.

Statistically significant results are printed in bold.
DMT, disease-modifying treatment; IQR, interquartile range; RRMS, relapsing-remitting multiple sclerosis; SD, standard deviation.
Discussion
In this contemporary Danish nationwide cohort study, which included adult patients with RRMS, we found that low educational attainment was associated with a delay (⩾76 days) in treatment with the first DMT after MS diagnosis. Educational attainment was not associated with a diagnostic delay in terms of long duration from clinical onset to diagnosis. Supplementary analyses showed similar results as in the main analyses supporting the educational gradient in a delay in treatment with the first DMT after MS diagnosis in both sexes and age groups, and in patients diagnosed with MS after 2013 at which time oral DMTs became more widely available.
Our study is unique as we conducted a nationwide population-based study to examine the educational gradient in diagnostic and treatment delays in MS.
Our analyses included three educational levels, four durations from clinical onset to diagnosis, four durations from diagnosis to first DMT, plus an additional group of patients not initiating DMT during the study period. Despite detailed analyses, we found increased odds only for low education and the longest duration from diagnosis to DMT initiation. We found no increased odds for low education and other durations or medium education, indicating that a part of the 17% of the population with low educational attainment had an increased risk of delayed DMT initiation.
That educational attainment was not associated with a diagnostic delay aligns with previous research. 15 The initiation of the first DMT after MS diagnosis has previously been shown not to depend on educational attainment 14 and has been shown to depend on educational attainment 15 in publicly funded healthcare systems. Our results from a Danish context with a publicly funded healthcare system and near-complete nationwide registry data support an educational gradient in access to DMT in patients with RRMS. Targeted interventions are, therefore, needed to address educational disparities in healthcare access and treatment initiation.
Educational attainment is established in adolescence or early adulthood and may not be easily increased later in life. Therefore, pathways and mechanisms linking low educational attainment with a delay in the initiation of the first DMT after MS diagnosis may help inform the development of targeted interventions and once successfully implemented these interventions may help buffer the association between educational attainment and access to DMT. Educational attainment comes before other social determinants, such as income and working conditions, that is, factors that may also not be easily changeable. Therefore, identifying high-risk groups among patients with RRMS with a low educational attainment and supporting their health literacy during clinical visits in the MS clinic may be more feasible.
Strengths and limitations
Strengths include the contemporary nationwide cohort of patients with RRMS in Denmark and the date-based recording of clinical onset, diagnosis and DMT initiation for all patients with RRMS. Another strength was the availability of annually updated information on educational attainment for all patients ensuring that educational attainment was assessed before clinical onset and diagnosis, respectively. We did not include patients with primary progressive MS (PPMS) in the diagnostic delay analyses. The absence of relapses makes it difficult to assess the time of symptom onset. For example, motor symptoms such as walking difficulties are generally more clearly defined, whereas slight sensory disturbances, cognitive symptoms and fatigue are associated with greater uncertainty regarding their precise onset. Due to these differences and uncertainties, we decided that including people with PPMS in analyses of diagnostic delay was out of scope in this study. Other limitations may be related to the observational design, as unmeasured confounding cannot be ruled out. Information on health behaviour, such as smoking and diet, was not available in this study. These factors have most likely not confounded the education diagnosis and the education DMT associations, as it seems unlikely that they should have impacted educational attainment. A potential confounding effect of health status cannot be ruled out. The educational level, however, is established early in life, and comorbidities likely occur afterwards. Income too is preceded by educational attainment and associated with MS outcomes. Therefore, comorbidities and income are more likely mediators than confounders of the education diagnosis and the education DMT associations. Including information on comorbidities and income in future studies on educational attainment and MS outcomes will allow analysing their role in the pathways linking educational attainment with MS outcomes.
Concluding remark
In adult patients with RRMS, low educational attainment was associated with higher odds of DMT delay but not diagnostic delay. Targeted interventions are needed to address educational disparities in healthcare access and treatment initiation.
Supplemental Material
sj-docx-1-tan-10.1177_17562864251313918 – Supplemental material for The impact of educational attainment on diagnostic and treatment delays in multiple sclerosis: a nationwide cohort study in Denmark
Supplemental material, sj-docx-1-tan-10.1177_17562864251313918 for The impact of educational attainment on diagnostic and treatment delays in multiple sclerosis: a nationwide cohort study in Denmark by Elisabeth Framke and Melinda Magyari in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-2-tan-10.1177_17562864251313918 – Supplemental material for The impact of educational attainment on diagnostic and treatment delays in multiple sclerosis: a nationwide cohort study in Denmark
Supplemental material, sj-docx-2-tan-10.1177_17562864251313918 for The impact of educational attainment on diagnostic and treatment delays in multiple sclerosis: a nationwide cohort study in Denmark by Elisabeth Framke and Melinda Magyari in Therapeutic Advances in Neurological Disorders
Footnotes
Appendix
Acknowledgements
The authors would like to acknowledge all MS clinics in Denmark for their data collection efforts and the Danish Multiple Sclerosis Society for supporting the management of the Danish Multiple Sclerosis Registry.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.