
Abstract
Background:
Complete vaccination coverage is recommended by multiple sclerosis (MS) societies for patients with multiple sclerosis (pwMS) to mitigate infection risks associated with disease-modifying therapies (DMTs).
Objectives:
To analyze vaccination coverage and its determinants in pwMS compared to healthy controls, considering vaccination hesitancy, MS-specific vaccination beliefs, trust in information sources, and the role of general practitioners (GPs).
Methods:
This cross-sectional multicenter observational study was conducted in six German MS centers. The primary endpoint was a vaccination index (VI) comprising eight standard vaccinations (range 0–1, with higher VI indicating better vaccination coverage). Secondary endpoints included validated measures of general vaccination hesitancy, MS-specific vaccination beliefs, and trust in information sources. Data were collected through questionnaires, vaccination card analysis, and a survey of GPs who vaccinate pwMS.
Results:
VI tended to be lower in pwMS (n = 397) compared to healthy controls (n = 300; 0.58 ± 0.30 vs 0.62 ± 0.31, p = 0.057). In pwMS receiving highly effective DMTs, VI did not differ significantly from those on no/platform DMTs. Vaccination hesitancy was comparably low, with no differences between pwMS and controls. Vaccination hesitancy, beliefs, and trust in information sources explained only 10%–16% of the variance in VI. Among 109 GPs, 82% cited reluctance to vaccinate pwMS due to concerns about MS-related side effects or interactions with DMTs.
Conclusion:
Despite clear recommendations from MS societies for full vaccination of all pwMS, vaccination coverage remains worryingly low. Approximately half of the patients lack standard vaccination coverage, even those on highly effective DMTs. In fact, vaccination coverage in pwMS tended to be even lower than in healthy controls. Vaccination hesitancy and other intrinsic factors do not sufficiently explain the low vaccination rates. Inconsistent vaccination recommendations from GPs due to uncertainties about vaccine safety and DMT interactions likely contribute.
Plain language summary
Vaccinations are crucial for people with multiple sclerosis (MS) to protect them from infections that may worsen their condition, especially during certain treatments. However, many MS patients are not fully vaccinated. This study examines vaccination rates and factors that affect whether MS patients receive vaccines. We found that general practitioners often hesitate to recommend vaccines due to concerns about safety and treatment interactions. Our results suggest that vaccinations should be administered by specialized vaccination centers to ensure patients receive the appropriate care.
Keywords
Introduction
Multiple sclerosis (MS) is one of the most common neurological diseases. 1 Over the last decade, numerous highly effective disease-modifying therapies (DMTs) have been approved. However, advances in disease control through immunosuppression have increased infection risks. 2
As a crucial component of managing infection risks in patients with MS (pwMS), vaccinations have become an integral part of routine clinical MS care, leading to the publication of extensive guidelines on MS vaccine management.3–8 These guidelines generally recommend complete basic vaccination coverage for all pwMS with additional indication-specific vaccinations depending on the degree of immunosuppression. However, it is unclear whether these recommendations are effectively implemented in routine care, as comprehensive data on actual vaccination coverage among pwMS and its influencing factors are lacking.
Vaccination coverage is influenced by a complex interplay of factors, with vaccination hesitancy thought to play the most prominent role. 9 Vaccine hesitancy has steadily grown in the general population and is a top global health threat according to the World Health Organization. 10 However, it is unknown if vaccine hesitancy is also an issue among pwMS affecting their vaccination status. Another factor thought to influence vaccination coverage in pwMS is the prevalence of “vaccination myths,” such as the belief that vaccination may trigger MS exacerbations.7,11,12 Additionally, initial indications suggest that MS-specific beliefs are also prevalent among general practitioners (GPs) who vaccinate pwMS, potentially influencing their vaccination recommendations. 13
This study aimed to analyze vaccination coverage and its determinants in pwMS. We hypothesized that due to regular medical care and the present of extensive guideline recommendations, vaccination coverage in pwMS would be higher than in healthy controls. To determine potential factors associated with vaccination coverage, we further investigated vaccine hesitancy, MS-related vaccination beliefs, trust in information sources, and the MS-specific vaccination recommendations and beliefs of GPs who vaccinate pwMS.
Methods
Study design
This cross-sectional multicenter observational study aimed to analyze vaccination coverage and its influencing factors in pwMS compared with healthy controls. The study was performed in six German MS-centers and affiliated nonneurological outpatient clinics and neurological practices (see Appendix). The reporting of this study conforms to STROBE guidelines. 14
Recruitment strategy
Study participants were recruited between June 2022 and May 2023 through outpatient consultations at the participating study centers, following an initial phone contact. MS group participants were specifically recruited from MS consultations, while control group participants were selected from general neurology or trauma surgery consultations. The proportion of controls was generally matched to the size of the MS group at each center and balanced with the MS group by age (±5 years) and sex to ensure comparability between the groups. Written informed consent was obtained, and vaccination documents were copied. Participants completed a questionnaire that collected demographic variables, socioeconomic data, information about their vaccinating GP, details of their last vaccination checkup, and responses to a validated vaccine hesitancy assessment. 15 MS-related information was collected from medical records. Participants’ MS-specific vaccination beliefs and their trust in various vaccination information sources were assessed using a custom-developed questionnaire (see Appendix).
Inclusion/Exclusion criteria
Study participants were required to be older than 18 years and possess a German vaccination card. Additional inclusion criteria for the MS group included a diagnosis of MS according to the McDonald criteria valid at the time of diagnosis. 16 Exclusion criteria for the MS group included a diagnosis made <3 months before participation. The exclusion criteria for the control group were designed to capture a cross-section of an otherwise healthy population by excluding chronic neurological, internal, dermatological, rheumatological, or oncological conditions that could impact an intact health span 17 (see Appendix). Consequently, control group participants presented to the study centers with uncomplicated nonchronic issues, such as mild cephalgia, acute back pain, nerve compression syndromes, or minor posttrauma concerns.
Outcome measures
Vaccination coverage and calculation of vaccination index (primary endpoint)
Vaccination documents were reviewed, and full vaccination coverage was assumed if the documented vaccinations fulfilled the recommendations of the German Standing Committee on Vaccination (STIKO) 18 (see Appendix). Vaccinations were categorized into standard vaccinations (tetanus, diphtheria, polio, pertussis, measles, mumps, rubella, COVID-19), which are recommended for all adults in the control and MS group, and indication-specific vaccinations (pneumococcal, meningococcal, hepatitis A, hepatitis B, seasonal influenza, herpes zoster) which are recommended for adults with certain predisposing conditions or those under immunosuppression. 18 Vaccination coverage for standard vaccinations was compared between the two study groups by means of a vaccination index (VI), which served as the primary endpoint. To calculate this index, the sum of each completed standard vaccination (yes = 1/no = 0) was divided by eight. Therefore, a higher VI indicates better vaccination coverage.
Vaccination hesitancy
Vaccination hesitancy was measured using the 7C scale, a validated questionnaire that assesses seven psychological antecedents influencing one’s general decision to receive vaccinations: confidence, complacency, constraints, calculation, collective responsibility, compliance, and conspiracy. 15 The questionnaire includes 21 items, with three questions for each psychological antecedent. Mean scores of items for each psychological antecedent and a total score were computed, with lower scores indicating higher vaccination hesitancy.
MS-specific vaccination beliefs and trust of pwMS in information sources
We developed two questionnaires to evaluate individual information knowledge regarding MS-specific vaccinations and vaccination beliefs (11-items) and pwMS’ confidence in different information sources (10-items), adapted from previous studies.11,13,19 After pilot testing, responses were collected using a 7-point Likert scale (see Appendix).
MS-specific vaccination recommendations among pwMS’ GPs
GPs were contacted via postal mail and invited to participate in the study by completing an anonymized questionnaire. This questionnaire addressed the GP’s MS-specific vaccination recommendations and their beliefs regarding vaccinations for their pwMS (see Appendix).
Statistical analysis
The sample size was calculated a priori based on anticipated tetanus vaccination coverage rates, assuming a 10% difference in coverage rates between groups. Using a two-sided Chi-square test at a 0.05 significance level, we determined that 323 participants per group would provide 80% power to detect this difference. All collected data were analyzed descriptively. Categorical variables were presented as both absolute and relative frequencies. Metric variables were described using the median, arithmetic mean, minimum and maximum values, and standard deviation. For the primary endpoint VI, the Wilcoxon two-sample test was employed to compare the MS and control groups after QQ plot inspection revealed deviations from normality, warranting a nonparametric approach. For vaccination hesitancy, a two-sided t-test assessed group differences, while three separate linear regression models evaluated the associations between VI and (a) vaccination hesitancy, (b) knowledge and vaccine-related beliefs, and (c) trust in information sources. Each model was adjusted for age, sex, education, and the size and geographical region of residence. Multicollinearity was assessed using Variance Inflation Factor scores, with all values below 4, indicating no significant multicollinearity. Secondary analyses, including t-tests and linear regression models, did not undergo normality checks due to the large sample size, which supports robustness in parametric tests even with minor assumption violations. 20 No formal statistical testing was performed for group differences in vaccination coverage for specific standard and indication-specific vaccinations. The level of significance (p < 0.05) was not adjusted for multiple outcomes. 21 All analyses were performed using SAS 9.4.
Results
Study cohorts
PwMS and control group
Of the initially 420 contacted subjects, 397 (94.5%) in the MS group and 300 (90.3%) in the control group met the inclusion criteria and agreed to participate. Both groups were well-balanced in age, sex, socioeconomic status, and geographical region though pwMS tended to live in smaller towns (Table 1).
Cohort characteristics.

DMT, disease-modifying therapy; EDSS, expanded disability status scale; platform DMT: Dimethyl-/Diroximel fumarate, Teriflunomide, Interferons, Glatirameracetate; highly effective DMT: Cladribine, S1P-receptor modulators, Ocrelizumab, Ofatumumab, Alemtuzumab, Natalizumab; GP, general practitioner.
“Unemployed” also includes subjects with disability pension, regular pensioners, and students.
General practitioners
Out of 397 pwMS, 230 provided their GPs’ contact details. Among 230 GPs contacted, 109 (47.4%) participated, with an average age of 52 years (SD 8.7), and 52 (47.7%) were female. The median number of pwMS treated by each GP was 7 (IQR 4–10).
VI for standard vaccinations (primary endpoint)
PwMS had their vaccination status checked slightly more recently compared to the control group (Table 1). The VI tended to be lower in pwMS than in controls (0.58 ± 0.30 vs 0.62 ± 0.31 (mean ± standard deviation), p = 0.057; Table 2). Among pwMS receiving highly effective DMTs, the VI did not differ significantly from controls or from pwMS on no/platform DMTs (Table 2).
Vaccination index for standard vaccinations.
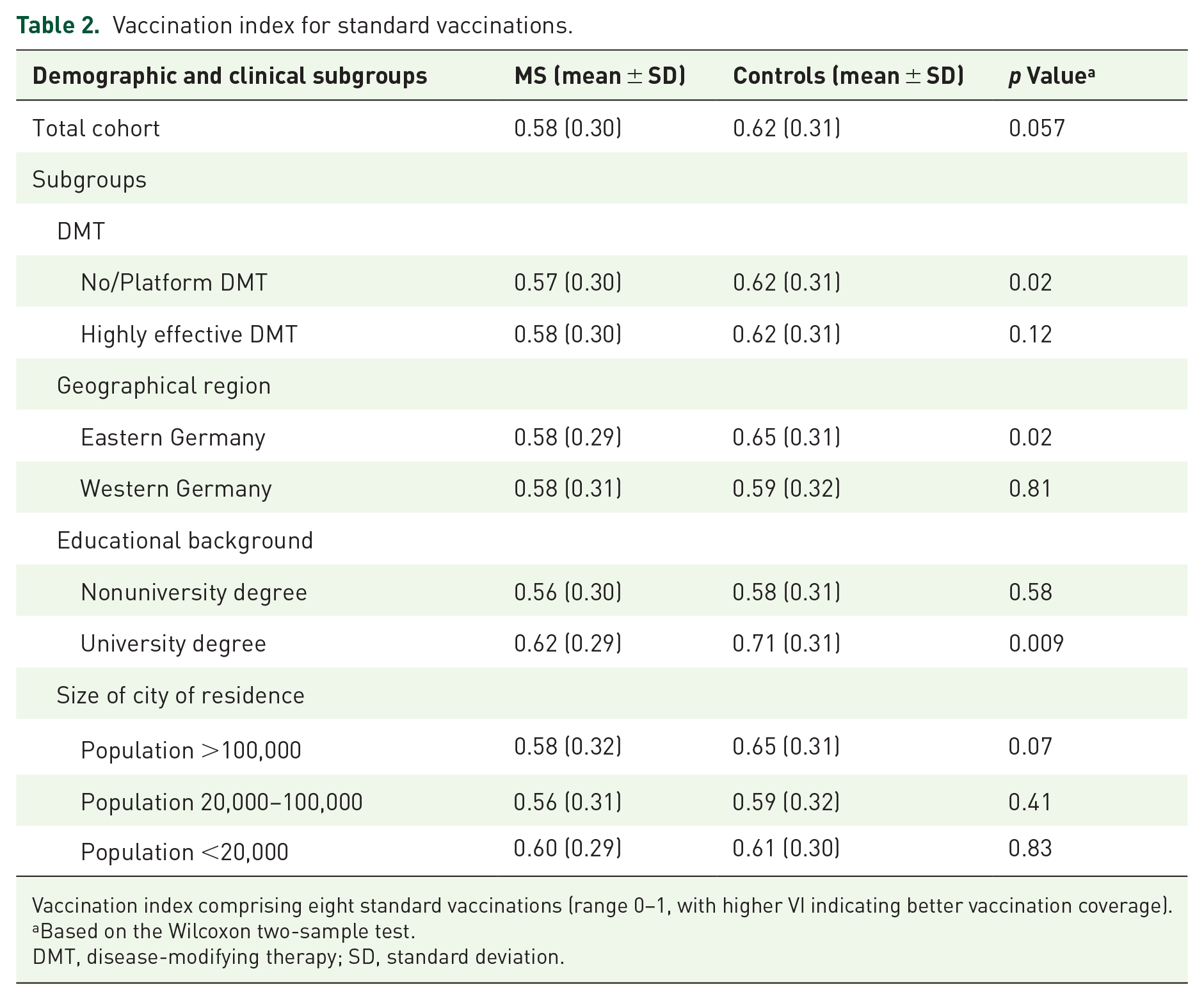
Vaccination index comprising eight standard vaccinations (range 0–1, with higher VI indicating better vaccination coverage).
Based on the Wilcoxon two-sample test.
DMT, disease-modifying therapy; SD, standard deviation.
Vaccination coverage for specific standard and indication-specific vaccinations
For all standard vaccinations except COVID-19, vaccination coverage was numerically lower in pwMS compared to controls (Table 3). A similar pattern was observed for pwMS receiving highly effective DMTs compared to controls (Table 3). There was no relevant difference in vaccination coverage for all standard vaccinations between pwMS receiving highly effective DMTs and those on no/platform DMTs (Table 3).
Descriptive data on full vaccination coverage for standard and indication-specific vaccinations.
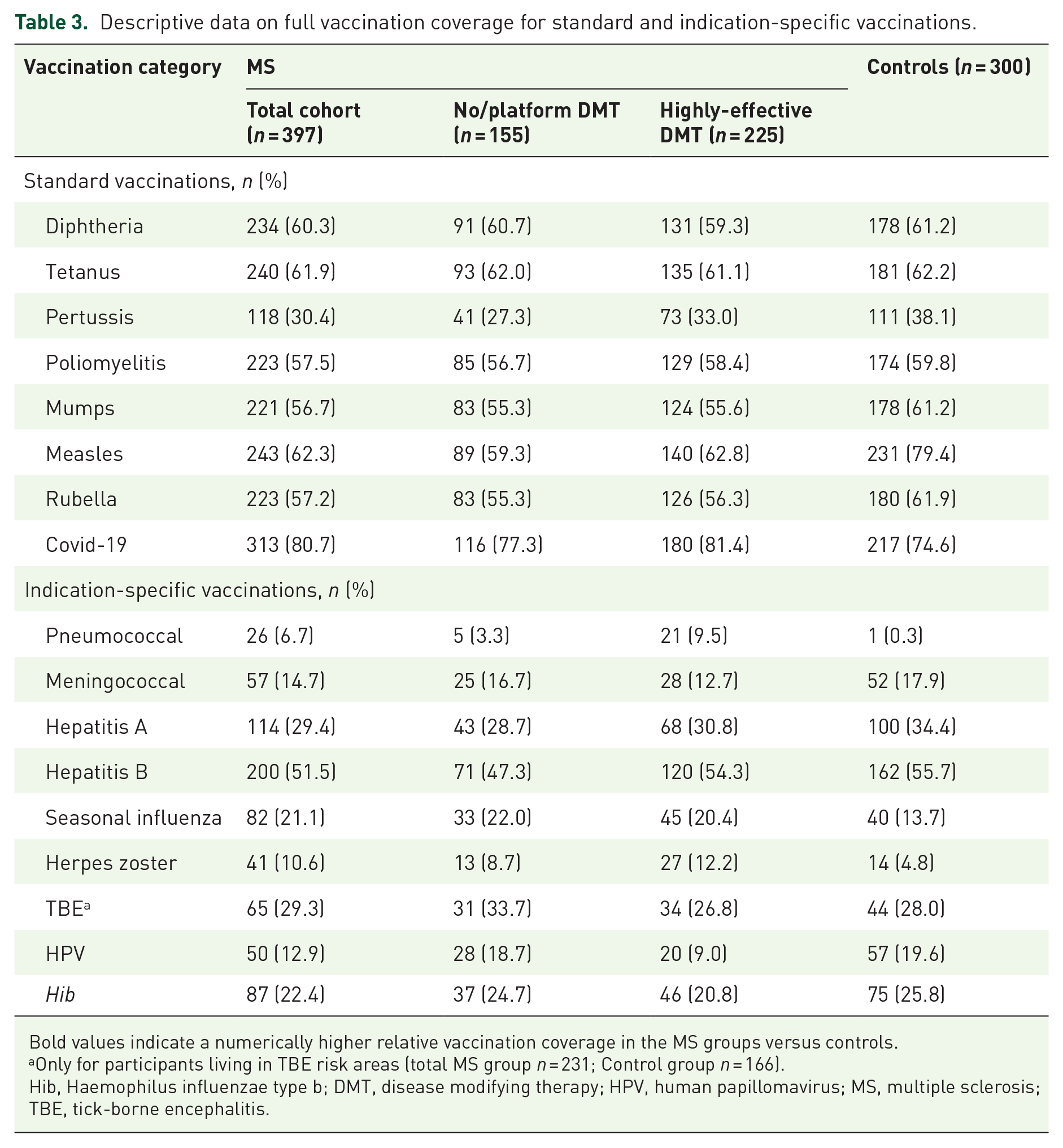
Bold values indicate a numerically higher relative vaccination coverage in the MS groups versus controls.
Only for participants living in TBE risk areas (total MS group n = 231; Control group n = 166).
Hib, Haemophilus influenzae type b; DMT, disease modifying therapy; HPV, human papillomavirus; MS, multiple sclerosis; TBE, tick-borne encephalitis.
For indication-specific vaccinations against pneumococcal diseases, influenza, herpes zoster, and tick-borne encephalitis, vaccination coverage in pwMS was numerically higher than in controls (Table 3). In subgroups, pwMS on highly effective DMTs had better vaccination coverage than controls for three out of nine indication-specific vaccinations (Table 3). Again, there was no relevant difference in vaccination coverage for indication-specific vaccinations between pwMS receiving highly effective DMTs and no/platform DMTs, except for HPV vaccination (18.7% vs 9%; Table 3).
Vaccination hesitancy
Vaccine hesitancy, as measured by the 7C scale, did not differ between the study groups for any of the seven psychological antecedents or the total score (Table 4).
Vaccination hesitancy (7C scale).

Responses are based on a seven-point Likert scale. Lower scores indicating higher vaccination hesitancy.
Based on a two-sided t-test.
Level of information and MS specific vaccination beliefs among MS patients
A total of 68% of pwMS reported being adequately informed about vaccinations and MS, and 76% were generally willing to receive all recommended vaccinations. Additionally, 69% believed they had complete vaccination coverage (Figure 1(a)). Regarding MS relapses, 57% agreed that infections could trigger relapses, and 23% that vaccinations could do the same (Figure 1(a)). Only 11% and 19%, respectively, feared that vaccinations interfere with their DMT or be ineffective due to DMT treatment (Figure 1(a)).

Vaccination information status, beliefs, and trust in information sources in patients with MS. “Disagree” comprises the categories: I do not agree at all, I do not agree, I somewhat disagree; “Agree” comprises the categories: I somewhat agree, I agree, I fully agree. (a) To what extend do you agree or disagree with the following statements about MS and vaccinations? and (b) When it comes to the topic of MS and vaccinations, I trust in the recommendations of . . .
Trust of MS-patients in information sources
The majority of pwMS trust the vaccination recommendations of their neurologist (93%), primary care physician (81%), or the German MS Society (75%; Figure 1(c)).
Factors predicting VI
The three regression models accounted for only 10%–16% of the variance in the VI (Table 5). In the knowledge and vaccine-related beliefs model, the general fear of vaccination side effects negatively predicted VI (β = −0.04, p = 0.01). In the trust in information sources model, trust in vaccination recommendations by GPs (β = 0.04, p = 0.01) and by pharmaceutical companies (β = 0.03, p = 0.03) positively predicted VI, while trust in vaccination recommendations by friends and family negatively predicted VI (β = −0.03, p = 0.03). None of the components of the 7C scale in the vaccination hesitancy model were found to be significant predictors of VI.
Regression models.

Each of the above models was additionally adjusted for age, sex, education, size, and geographical region.
MS, multiple sclerosis.
MS-specific vaccination recommendations among GPs of pwMS
About 28% of GPs agreed that vaccinations trigger MS relapses, while 24% remained neutral (Figure 2(a)). Between 76% and 95% of GPs frequently recommend standard inactivated vaccines to pwMS, regardless of their immunotherapy status (Figure 2(b)). Only 50% suggested mumps, measles, or rubella vaccines. Indication-specific vaccination recommendations, such as for human papillomavirus (least recommended at 16%) and pneumococcal vaccines (most recommended at 86%), were lower than those for standard vaccinations (Figure 2(c)). Notably, 89 (82%) GPs cited significant reluctance to vaccinate pwMS, primarily due to concerns about potential side effects related to MS (42.5%) and interactions with DMTs (40.7%; Table 6).

MS-specific vaccination recommendations of general practitioners. “Disagree” comprises the categories: I do not agree at all, I do not agree, I somewhat disagree; “Agree” comprises the categories: I somewhat agree, I agree, I fully agree. (a) To what extent do you agree or disagree with the following statements?, (b) How often do you recommend the following basic vaccinations to your MS patients without adequate vaccination coverage, independently of immunotherapy?, and (c) How often do you recommend the following indication-specific vaccinations to your MS patients without adequate vaccination coverage who receive/will receive immunotherapy?
General practitioners’ reasons for not vaccinating patients with MS (n = 89).

DMT, disease modifying therapies; MS, multiple sclerosiss.
Discussion
This study is the first comprehensive multicenter analysis comparing vaccination coverage in pwMS to healthy individuals while examining factors that influence vaccination status, including a survey among their GPs who vaccinate pwMS. Previous research has largely been limited to specific vaccines,22–28 single study centers,23,25,29 or small23,25 and localized cohorts,23–25,29,30 without considering determinants of vaccination coverage, which hampers generalizability.
Our main finding revealed that vaccination coverage for standard vaccinations in pwMS, as measured by the VI, is disconcertingly low and not significantly different from that of healthy individuals. In fact, the VI tended to be lower in pwMS compared to healthy controls. This result contradicts the expectation that pwMS, who are under close medical supervision, would have higher vaccination rates. Notably, pwMS reported more frequent monitoring of their vaccination status by physicians than controls. Although most of the standard vaccines included in the VI are routinely administered during childhood, prior to MS diagnosis, any missing or undocumented vaccinations should be supplemented or boosted in adulthood. However, this supplementation appears to occur no better—or even worse—among pwMS compared to healthy controls. These findings are consistent with those observed in other autoimmune diseases. For instance, a Slovenian study found that only 64.7% of young adults with rheumatological diseases had coverage for mandatory vaccines, significantly lower than the general population. 31 Similarly, a German study showed that vaccination coverage for tetanus and diphtheria in adolescents with idiopathic arthritis was 24% and 79%, respectively, compared to 46% and 95% in healthy peers, mainly due to doctors advising against vaccination. 32
A comparison of our findings with previous studies revealed discrepancies in the coverage rates for certain standard and indication-specific vaccines. For example, a single-center study from Austria reported about 30% higher vaccination rates for diphtheria, tetanus, pertussis, and poliomyelitis in pwMS than in our cohort. 29 These differences likely stem from methodological variations. Berek et al. considered a single booster sufficient for full vaccination, whereas our study included basic vaccinations. Similarly, a local study from Eastern Germany, which also considered basic vaccinations, reported a 64.5% tetanus vaccination rate in pwMS, 24 aligning with our results. However, this study also reported a 74.8% pertussis vaccination rate, which is higher than our rates (30.4% in pwMS, 38.1% in controls) and those in the general German population (49.8%). Reports on influenza vaccination coverage vary widely, ranging from 13.5% in a cohort from Eastern Germany 24 to 42% in Spain, 25 and up to 80% among elderly pwMS in the United States, 30 reflecting geographic and cohort differences. Consistent with our findings, data from German health insurance claims estimated that about 19% of pwMS receive seasonal influenza vaccinations. 22
National and international guidelines recommend complete vaccination coverage, especially for MS patients on highly effective DMTs, to mitigate the increased infection risk due to immunosuppression.3–8 Recent studies have shown that sufficient seroconversion can be achieved even under most DMTs without significant safety concerns, as demonstrated for influenza, COVID-19, and other vaccines.33–35 In our cohort, more than 50% of patients were on highly effective DMTs. Despite these recommendations, our study found that vaccination coverage for standard vaccines in these patients was not significantly different from that in healthy controls or other pwMS. Additionally, coverage for six out of nine indication-specific vaccines recommended for immunocompromised individuals was even lower in pwMS on highly effective DMTs compared to healthy controls. This discrepancy is notable, as few participants in the control group were likely eligible for most indication-specific vaccinations, unlike pwMS on highly effective DMTs.
To determine potential reasons for the lower vaccination coverage in pwMS, we analyzed three clusters of intrinsic factors hypothesized to be associated with vaccination coverage.
First, we assessed general vaccine hesitancy using the validated 7C scale. 15 A mean 7C score above 4 indicates high vaccination readiness or low hesitancy, 36 which was observed in both study groups. Furthermore, there were no significant differences between the MS and control groups in total 7C scores or subscales. Our regression analysis revealed that none of the 7C components were significant predictors of VI, suggesting that general vaccine hesitancy is unlikely to be a relevant factor influencing actual vaccination coverage. This contrasts with results from a smaller Irish study conducted at the beginning of the SARS-CoV-2 pandemic, which reported vaccine hesitancy as a common phenomenon in pwMS, affecting 10%–20% of the cohort using nonvalidated questionnaires. 37 It is conceivable that, in our study conducted later in the pandemic, increased public awareness of infection risks and vaccine benefits contributed to lower hesitancy. 33
Second, we investigated the level of information and MS-specific vaccination beliefs. Over two-thirds of pwMS reported being well informed and willing to receive necessary vaccinations, confirming the low vaccination hesitancy as measured by the 7C scale. However, beliefs about MS-specific vaccinations varied among the participants. Although the majority of pwMS accurately recognized that infections can trigger relapses, a significant proportion (43%) were unsure or disagreed. Similarly, while most MS patients correctly disagreed that vaccinations trigger relapses, a considerable percentage (44%) were unsure or agreed. Concerns regarding DMT treatment were generally low, with only 11%–19% assuming that vaccinations may interfere with their DMT or may be ineffective. In our second regression model, none of the MS-specific vaccination beliefs were significant predictors of VI. In contrast, the general fear of vaccination side effects was a significant predictor, although it accounted for a relatively small proportion of the variance in VI. The results suggest that, despite a relatively high number of pwMS believing in MS-specific vaccination myths, these beliefs likely do not significantly affect their vaccination coverage.
Third, we examined trust in various information sources. PwMS showed the highest levels of trust in physician recommendations and official sources. Our regression analysis indicated that trust in GP recommendations and pharmaceutical companies was a positive but weak predictor of VI, aligning with studies in healthy subjects. 38 Despite high trust in neurologists’ recommendations, this was not associated with VI, possibly because vaccinations in Germany are administered by GPs, not neurologists. This finding may also indicate an interface problem between these two medical specialties. It is conceivable that neurologists’ recommendations are not implemented by GPs, potentially due to their own hesitancies and misconceptions with regard to MS or DMTs. In this context, a French study reported that general vaccine hesitancy is prevalent among GPs. 13 Specifically, 37% of the GPs surveyed in the study did not regularly recommend hepatitis B vaccines to seronegative adults, and 12% considered MS to be a potential side effect of this vaccine.
To explore this assumption further, we surveyed the GPs of our pwMS cohort and found that, like the pwMS themselves, over half of the respondents either mistakenly believed or were uncertain that vaccinations could trigger MS relapses. Additionally, only half of the GPs felt confident in their knowledge about the interactions between vaccines and DMTs. This lack of confidence was reflected in their MS-specific vaccination recommendations. A majority of GPs did not regularly recommend live attenuated or indication-specific vaccines to their pwMS due to concerns about potential MS-specific side effects and interactions with DMTs. This reluctance may be partly due to the very small number of pwMS each GP manages, compounded by the complexity of managing numerous licensed DMTs that fall outside their specialty. These results are particularly concerning, as previous studies have shown that recommendations of GPs play a key role in promoting acceptance of vaccinations, including among patients receiving immunotherapies.39,40
Our study has some limitations. The MS cohort was recruited from specialized MS centers, which may limit generalizability, as general neurologists may handle vaccinations and DMTs differently. Second, excluding MS patients without vaccination cards could lead to an overestimation of vaccination coverage. 41 However, since more than 90% of contacted MS patients had vaccination cards, significant bias is unlikely. Conversely, vaccination card records might underestimate coverage since not all vaccinations may be documented. Nonetheless, a comprehensive meta-analysis found only an 11% discrepancy between card-based and medical provider records. 42 Additionally, using a VI instead of individual vaccinations in the regression analysis may result in some loss of information, as patient attitudes toward different vaccinations can vary. Lastly, while the 47% response rate in our GP survey is generally regarded as satisfactory, a nonresponder bias cannot be excluded.
Conclusion
Vaccination coverage for pwMS is worryingly inadequate, with roughly half of the patients lacking full standard vaccination coverage. Despite more intensive monitoring of vaccination status, coverage in pwMS tended to be even lower than in a control group of healthy individuals. Additionally, pwMS receiving highly effective DMTs do not show better vaccination coverage compared to healthy controls or other pwMS, thereby increasing their risk for vaccine-preventable infections. General vaccination hesitancy and other intrinsic factors do not sufficiently explain the low vaccination rates. Instead, our findings suggest a significant influence of GPs, who may provide inadequate or inconsistent vaccination recommendations due to uncertainties about the safety of vaccinations and interactions with DMTs. To enhance vaccination coverage in pwMS, a structured training program for GPs could be implemented to ensure familiarity with MS-specific vaccination needs. However, given the limited number of pwMS seen by individual GPs, centralized vaccination units – either as independent centers or integrated within MS clinics – may offer a more effective and sustainable approach. This model would ensure consistent, specialized care, and reduce the risk of vaccine-preventable infections in this vulnerable population.
Supplemental Material
sj-docx-1-tan-10.1177_17562864241309806 – Supplemental material for Vaccination coverage and its determinants in patients with multiple sclerosis—a multicenter cross-sectional study
Supplemental material, sj-docx-1-tan-10.1177_17562864241309806 for Vaccination coverage and its determinants in patients with multiple sclerosis—a multicenter cross-sectional study by Paula Schade, Hai-Anh Nguyen, Julia Steinle, Kerstin Hellwig, Teodor Pelea, Philipp Franken, Birte Elias-Hamp, Veit Becker, Stefan Merkelbach, Stephan Richter, Bert Wagner, Christian Geis, Matthias Schwab and Florian Rakers in Therapeutic Advances in Neurological Disorders
Footnotes
Appendix
Acknowledgements
We would like to thank Christine Rau, Dörthe Niemeyer, and Mrs. Stumpf for their help with the organization of the study visits, their contact with the patients and their complete dedication to the project. We gratefully acknowledge Dr. Benjamin Schleenvoigt for his valuable input on the study design and Dr. Veit König for facilitating access to the control group participants. We would also like to thank the study participants for their transparency and their time.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.