
Abstract
Background:
The diagnosis of and life-sustaining treatment (LST) for patients with disorders of consciousness (DoC) and locked-in syndrome (LIS) have been the subject of intense debate.
Objective:
We aim to investigate the application of diagnostic knowledge, opinions about the administration of LST, and ethical challenges related to DoC and LIS.
Design:
A cross-sectional study.
Methods:
A survey was conducted among Chinese neurologists. Questionnaires included three vignettes (unresponsive wakefulness syndrome (UWS); minimally conscious state (MCS), and LIS). They were randomly distributed among neurologists from August 2018 to December 2019.
Results:
A sample of 360 questionnaires was included (response rate: 78%). Overall, 63% of the participants chose the correct diagnostic category. The neurologists who received the MCS case chose the category more accurately than the neurologists with the UWS (p < 0.001) and LIS case (p = 0.002). Most neurologists preferred never to limit LST for their patients (47%, 63%, and 67% in UWS, MCS, and LIS groups, p = 0.052). A large group of neurologists believed UWS patients could feel pain (73%), with no difference from MCS and LIS patients (p > 0.05). Deciding for patients in the absence of surrogates was rated extremely challenging.
Conclusion:
A large proportion of Chinese neurologists in our study didn’t apply the accurate diagnostic categories to the description of DoC and LIS patients. This calls for more education and training. Most Chinese neurologists were reluctant to limit LST for patients. This may indicate that there may be a need to emphasize the allocation of more resources toward long-term care in China.
Plain language summary
The diagnosis of and life-sustaining treatment (LST) for patients with disorders of consciousness (DoC) and Locked-in syndrome (LIS) have been the subject of intense debate. To describe the knowledge and attitudes of physicians regarding patients with some DoC and LIS in Eastern countries we conducted a vignette-based survey among Chinese neurologists. This study reveals significant differences from previous studies, namely, lower diagnostic accuracy and less limitation of life-sustaining treatment. This may be closely related to policies, cultures, economies, and laws among countries. A deeper understanding of neurologists’ moral beliefs and attitudes can inform healthcare policy and might point to areas of research and healthcare practice that need further regulatory attention. A normative orientation through institutional, regional, or national policies for decision-making can increase the likelihood of reaching consistent and transparent decisions about the care of patients with severe brain injury across different regions and cities.
Introduction
After severe brain injury, some patients may experience a period of coma followed by conditions known as disorders of consciousness (DoC). When patients’ sleep-wake cycle returns, but they do not show any signs of awareness, the condition is called unresponsive wakefulness syndrome (UWS), which was previously referred to as a vegetative state.1,2 If patients’ level of consciousness improves further and they exhibit nonreflexive behaviors in response to surroundings or stimuli, they are in a minimally conscious state (MCS). 3 A specific neurobehavioral diagnosis called locked-in syndrome (LIS) can be confused with a DoC. Patients with LIS suffered pontine lesions while preserving cognitive abilities. Apart from eye movements, they cannot speak or give a motor output in an independent way. 4
Neurologists base their diagnosis mostly on behavioral responses at the bedside. The diagnostic categories subsequently inform the clinical management of the patient. The Coma Recovery Scale-Revised (CRS-R), as the current gold standard for the diagnosis of DoC, has been widely used in some large medical centers and neurological rehabilitation units. 5 Yet, the clinical diagnosis of DoC has been criticized. In a previous assessment of 89 and 48 patients with the clinical diagnoses of UWS and MCS, respectively, the diagnoses were revised in part when using the CRS-R. 6 Schnakers et al. had also reported previously that 18 (41%) of 40 patients diagnosed with UWS based on clinical consensus were found to be in MCS following an assessment with the CRS-R. 7 Making accurate diagnoses still poses significant challenges to neurologists and misdiagnoses may misinform the medical decision-making for patients with DoC.
The administration of life-sustaining treatment (LST) for patients who have lost almost all capacity to do daily life activities involves a medical as well as an ethical justification. The attitudes of professionals toward deciding about LST are influenced by their social backgrounds and shaped by other influences, such as public policy, and social, cultural, and religious beliefs.8–10 For example, China’s harmonious- and family-oriented philosophy emphasizes Confucian social norms such as filial piety and family relations, which are different from Western traditions.8,9 There is currently no relevant law to regulate the end-of-life decision-making process on the Chinese mainland. The government of China has implemented a universal health insurance policy that reimburses 60%–80% of hospitalization costs allowing families to decide in favor of long-term care if they have the financial resources. 11
Only little is known about the current practices and attitudes of medical professionals in different countries as well as within those countries. 12 Most surveys from Western countries indicated that physicians seem rather in favor of the option of limiting LST, as more than two-thirds of healthcare professionals in almost all studies expressed the attitude to limit some treatment options for patients with DoC (e.g., Canada, the United States, Germany, and Italy).13–18 On the contrary in Eastern countries, there is a greater reluctance to limit LST in general. A recent cross-national study of end-of-life care in intensive care units in South Korea, Japan, and China suggested that most physicians are reluctant to limit LST. 19 However, there is limited data on neurologists’ attitudes toward the limitation of LST for patients after severe brain injury in the Chinese healthcare setting. Insights into the attitudes of physicians in different medical areas and regions are crucial to evaluating whether health care is justly distributed. Furthermore, attitudes in favor of or against the limitation of LST could inform the development of a healthcare policy on the issue.
To further the understanding of the attitudes toward limiting LST, we introduce a case vignette questionnaire to explore the following questions about patients with DoC and LIS: (1) How correctly do neurologists choose among the diagnostic categories of UWS, MCS, and LIS? (2) How do neurologists assess the options for (limiting) LST in patients with DoC and LIS? (3) What are the ethical, clinical, and practical challenges when providing healthcare for patients with DoC and LIS?
Methods
Questionnaire
We conducted a cross-sectional study using a self-administered questionnaire for Chinese neurologists who manage patients with (and in) conditions following severe brain injury. To investigate the application of diagnostic knowledge as well as ethical challenges in the care of patients with DoC and LIS, we used a vignette-based questionnaire. The questionnaire originated from a publication that reported the comparative analysis of data sets from Germany and Canada.17,20 Backward-forward translation was used to translate the English questionnaire into Chinese. 21 The English-to-Chinese translation was done by a native Chinese speaker (Y.Y.). The Chinese version was then translated back into English by another translator (W.H.). The original and translated English versions were then compared by an impartial assessor (H.D.). Three researchers in the field of DoC pretested the questionnaire and provided suggestions for improvement. Finally, the English and Chinese translations agreed, after the Chinese version was slightly adjusted.
Three case vignettes which had been drafted based on clinical consensus guidelines were presented randomly at the beginning of the questionnaire (see Supplemental Material 1: case vignettes). Then we explored the following domains of practice experiences and opinions:
According to the case vignette and based on participants’ prior knowledge of the management of patients with DoC and LIS, participants were asked to choose the correct diagnosis for a described patient. The categories UWS, MCS, LIS, brain death, coma, and an open text field could have been chosen. No definitions of diagnoses were provided. Then participants were asked to assess 6-month survival and probability of functional recovery with a modified Rankin scale. Then they rated how certain they have been about choosing the diagnostic category of their assigned case (numeric rating scale (NRS), 0–10, 10 = extremely certain).
Then the patients’ residual capabilities and quality of life (NRS, 0–10, 10 = extremely great, 0 = no quality of life, and “I don’t feel able to rate the patient’s quality of life”) were assessed.
Respondents were also asked their opinions on limiting LST (with the options including never, always, and under certain circumstances), and which specific treatment measures they would consider limiting.
Further, they rated the clinical, practical, and ethical challenges related to the management of the respective patients.
Data collection
The questionnaire was distributed at conferences focused on neurology or brain disorders in China from August 2018 to December 2019. The three cases vignettes of UWS, MCS, and LIS were distributed randomly and equally. To prevent plagiarism, we ensured that neighboring individuals received different questionnaires. The questionnaire cases were randomly distributed with a probability of 33.33%, and each respondent received only one case. The paper and pencil questionnaires were collected after being filled out. Inclusion criteria for participants were (1) Specialist doctors engaged in the diagnosis and treatment of DoC or LIS; (2) Doctors engaged in the diagnosis and treatment of brain injuries, including neurologists, neurosurgeons, neurointensivists, or intensivists; (3) Doctors providing chronic rehabilitation for patients with severe brain injuries, including physiotherapists and rehabilitation specialists. Exclusion criteria were medical staff who do not directly provide diagnosis and treatment for DoC or LIS patients, such as nursing staff, rehabilitation technicians, and research-oriented medical personnel.
Statistical analysis
Unfinished questionnaires were taken out of the analysis. Filled-out questionnaires with the assignment of an inaccurate diagnostic category to the patient described in the case vignettes were excluded after the analysis of part 1. We assumed that the incorrect knowledge of the syndromes may have then distorted the participants’ judgments of the other questions. Also, we were uncertain, whether participants were answering concerning the described condition or concerning the diagnostic category that they misidentified.
The statistical analysis flow program is shown in Supplemental Material 2. Statistical analysis used IBM Statistical Package for the Social Sciences 20 statistics software (SPSS Inc., Chicago, IL, USA). Frequency and percentage were used for descriptive statistics. The mean, first, and third quartiles were used to describe the ordinally scaled variables. The chi-square test was performed to assess the differences in opinion of limiting LST between the three case groups. With regard to demographics such as age, experience, gender, religion, primary discipline, and professional experience with patients, Tukey test analyses were used in the postevent pairwise tests. Logistic regression is used to verify the results again. For numerical or ordinal data, the Mann–Whitney U test was performed to compare two groups. The Kruskal–Wallis H test was applied to compare three groups, and Bonferroni test analyses were used in the postevent pairwise tests. A statistically significant difference was set at p < 0.05 (two-sided).
Results
Participants’ characteristics
Of the 461 participants that took part in the survey, 360 questionnaires were included in this study from the following cities and provinces: Nanjing (44), Guangzhou (53), Beijing (71), Hangzhou (52), Xiamen (55), and Nanchang (85), with a completion rate of 78.1%. One hundred one (21.9%) questionnaires were excluded due to incomplete participation. The sample consists of 122 (33.9%) of UWS-related questionnaires, 126 (35.0%) of MCS-related questionnaires, and 112 (31.1%) of LIS-related questionnaires.
Table 1 describes the respondents’ characteristics. Of all the respondents (n = 360), 213 (59.2%) were male. The mean age of the neurologists was 35 years. The mean number of years of clinical practice was 11 years, with a maximum of 56 years, contributed by a participant who was rehired after retirement. Most of the respondents were not religious (84.4%), which is consistent with the known information.
Personal and professional characteristics of participants (n = 360).
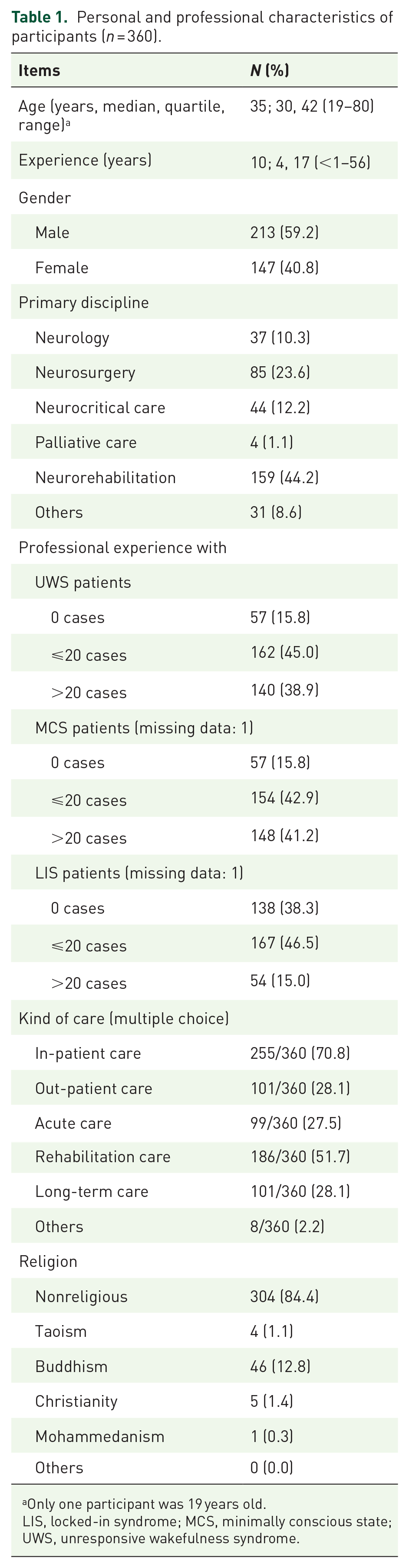
Only one participant was 19 years old.
LIS, locked-in syndrome; MCS, minimally conscious state; UWS, unresponsive wakefulness syndrome.
Application of diagnostic knowledge
In total, 62.8% of neurologists chose the accurate diagnostic category, while 37.2% selected an inaccurate diagnostic category or did not respond (Figure 1). According to the UWS case, 50.0% gave the correct diagnosis, 3.3% of respondents chose coma, 37.5% chose MCS, 8.3% chose LIS, and 0.8% chose another category. For neurologists receiving the MCS-vignette questionnaire, 78.2% chose the correct diagnostic category, with 0.8% of respondents choosing coma, 2.4% choosing UWS, 16.1% choosing LIS, and 2.4% choosing another category. In the LIS case, 59.5% of the participants chose the correct diagnosis LIS, 32.4% chose MCS, 4.5% UWS, 2.7% chose coma, and 0.9% chose another category. Overall, the participants who received the MCS case were more accurate in the selection of a diagnostic category than those who received the UWS (χ2 = 21.177, p < 0.001) and the LIS case (χ2 = 9.706, p = 0.002).
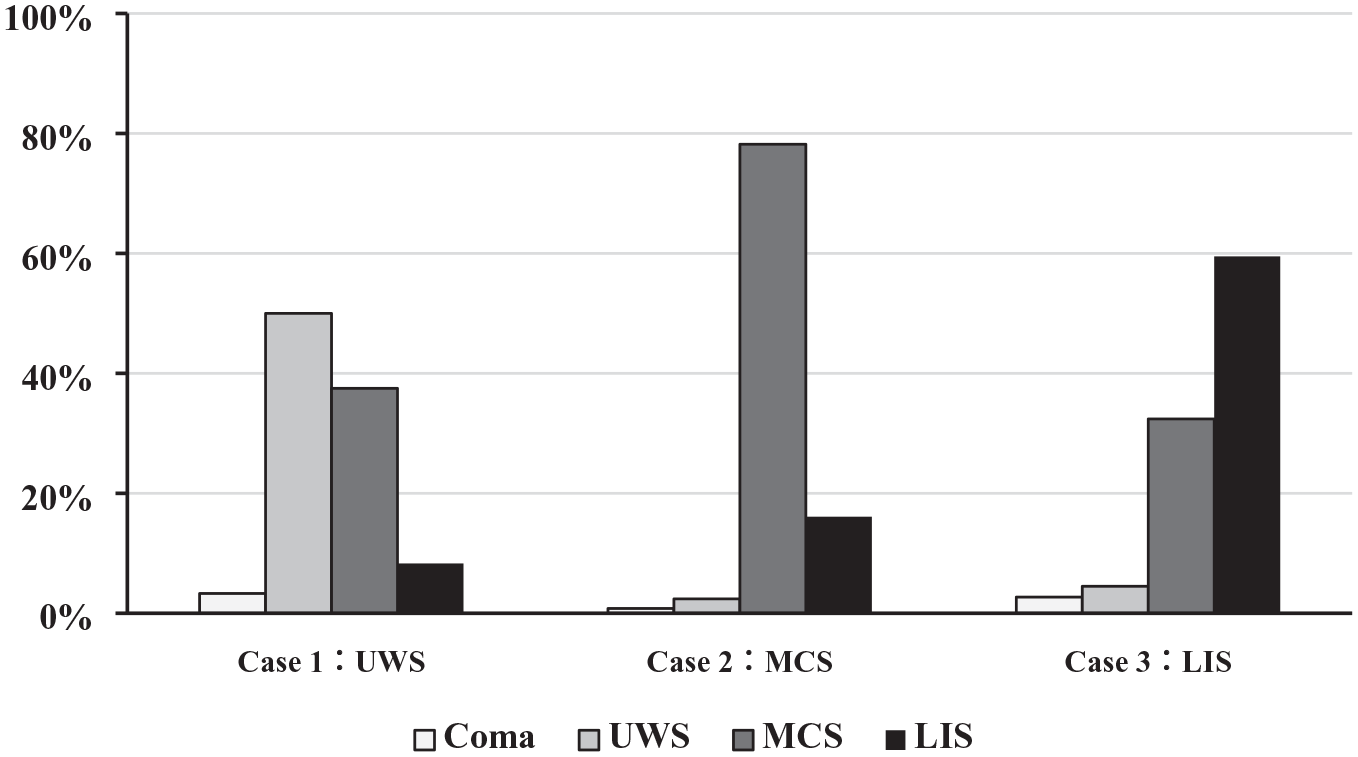
Diagnostic accuracy according to the three cases; the UWS, MCS, and LIS group (n = 360). Case 1: n = 120, two participants did not answer; Case 2: n = 124, two participants did not answer; Case 3: n = 111, one participant did not answer; nobody chose brain death in neither case.
Neurologists who have cared for a high number of patients with DoC and LIS have a higher chance of choosing the correct diagnosis category for the UWS case (U = 1361.0, p = 0.018) and the LIS case (U = 1021.0, p = 0.003), with no significant influence upon MCS (U = 1021.0, p = 0.233). Especially neurologists who have cared for more than 40 patients with UWS (OR = 4.29, 95% CI: 1.23–16.27, p = 0.032) and MCS (OR = 3.53, 95% CI: 1.06–11.70, p = 0.039) are more likely to assign the correct diagnostic category in the UWS cases. Neurologists with many years of professional experience had a lower chance of misdiagnosis in the UWS case (U = 2196.0, p = 0.037), with no significant influence in the MCS and the LIS case. Gender (χ2 = 0.833, p = 0.361) and primary discipline (χ2 = 7.195, p = 0.207) did not influence diagnostic accuracy. There was a statistically significant difference in the certainty scores of the different participants in the different diagnostic groups (F = 3.147, p = 0.045), with Tukey’s test showing lower certainty scores in case of being challenged with the assignment of the diagnostic category for the UWS cases (p = 0.045), and no statistical difference between the other groups.
Prognosis and quality of life
In terms of assessing the quality of life of patients, among participants who accurately diagnosed cases, 5.8% (n = 13, UWS: 3, MCS: 5, LIS: 4) believed that they were unable to assess the quality of life of patients. After removing participants who were unable to assess the quality of life of patients, compared with the MCS group, the average quality of life scores of the UWS group (x¯ = 1.68, range 0–7, p = 0.001) and LIS group (x¯ = 1.97, range 0–6, p = 0.025) were lower.
In terms of assessing the prognosis of patients, 10.8% (n = 24, UWS: 11, MCS: 8, LIS: 5) of participants believed that “it was difficult to make a prognosis assessment for patients.” After removing participants who found it difficult to make a prognosis assessment for patients, almost all participants believed that patients had varying degrees of disability, with 58.3% of participants believing that UWS patients had severe disabilities, 40.2% in MCS group, and 71.2% in LIS group. After the Kruskal–Wallis H test, it was found that participants believed that the prognosis of MCS patients was better compared with UWS patients (mean rank = 109.40, p = 0.005) and LIS patients (mean rank = 120.11, p < 0.001). No statistical differences were found in the assessment of future survival opportunities (H = 0.553, p = 0.758).
Respondents’ perceptions of a patient’s residual capabilities
Most respondents who correctly diagnosed the patients agreed that MCS patients and LIS patients can be aware of themselves and surroundings, UWS patients cannot. However, 73.3% of respondents agree that UWS patients can feel pain and compared with MCS group (73.3%) and LIS group (59.1%), no significant differences were found. More than half of respondents believe that MCS patients and LIS patients have emotions, can experience hunger/thirst, and have sexual desire (Table 2).
Frequency of agreement with the presence of capabilities of patients in the UWS group, MCS group, and LIS group (n = 223).

Those who correctly diagnosed the patients in the respective cases. Bold fonts indicate statistical differences.
LIS, locked-in syndrome; MCS, minimally conscious state; UWS, unresponsive wakefulness syndrome.
Attitudes toward limiting LST
When queried about whether limiting LST was necessary, the results revealed that 46.7% of respondents in the UWS group, 62.8% in the MCS group, and 66.7% in the LIS group opted for never limiting LST (Figure 2). There was no significant difference between the three groups (χ2 = 5.93, p = 0.052) but a trend toward a difference (p = 0.024). Compared to the MCS group (p = 0.050) and the LIS group (p = 0.024), more participants would limit LST in the UWS group. There was no significant influence on the participants’ descriptive characteristics (age, experience, gender, religion, primary discipline, and professional experience). Logistic regression repeatedly verified the result and found no significant influencing factors.

Attitudes toward the limitation of life-sustaining treatment of those participants who accurately assigned the diagnostic category in the respective cases (n = 223). Overall, there was no significant difference between the UWS, MCS, and LIS groups (χ2 = 5.81, p = 0.052), but a trend toward a statistical difference (p = 0.024); UWS group (n = 60), MCS group (n = 94, missing data: 3), LIS group (n = 66). The respondents who said they would “always” limit LST (all the participants in three groups: n = 3) were combined with those who chose to limit LST “under certain circumstances.”
Of all respondents who assigned the correct diagnosis, 42.6% said they would have made the same choice for themselves if they were in a UWS/MCS/LIS, respectively, 43.0 % would have chosen fewer measures, and 12.6 % said they wished they would receive more measures.
Circumstances in favor of or against a limitation of LST
Table 3 shows the number of participants who agreed or disagreed with the limitation of LST under certain circumstances, with their agreement level rated on a five-point scale (0 = disagreement with the limitation of LST). In most situations, the different diagnostic groups did not affect the participant’s choices (p > 0.05). Only when patients obviously suffered intensely, participants were more likely to limit LST in the MCS group than in the LIS group (p = 0.001).
Absolute numbers of distribution of the levels of agreement with the limitation of life-sustaining treatment under certain circumstances (n = 223).

Those who correctly diagnosed the patients in the respective cases; UWS group (n = 60), MCS group (n = 94, missing data: 3), LIS group (n = 66). Kruskal–Wallis test (patient obviously suffers intensely: the rating score in MCS was higher than LIS, p = 0.01); numbers in this table are displayed in absolute in this table. Bold fonts indicate statistical differences.
LIS, locked-in syndrome; LST, life-sustaining treatment; MCS, minimally conscious state; UWS, unresponsive wakefulness syndrome.
Appraisal of ethical, clinical, and practical challenges
Figure 3 shows arithmetic mean ratings of ethical, clinical, and practical challenges in the care of patients with UWS, MCS, and LIS. Deciding for patients in the absence of a surrogate was rated as extremely challenging for all three groups. Reaching an agreement as a team and multidisciplinary discussions were rated as the least challenging issues. Finding the correct diagnosis was rated as more challenging in the MCS group than in the LIS group (p = 0.050). Evaluating resource allocation was rated as more challenging in the UWS group than in the MCS group (p = 0.012).

Appraisal of ethical, clinical, and practical challenges in the decision-making process and health care for patients like the patient in the presented case (n = 223). The bars indicate the arithmetic mean of ethical challenges with regard to each diagnostic group: UWS (black), MCS (gray), and LIS (white). 0 = not challenging, and 10 = extremely challenging; all the participants: n = 223, UWS group (n = 54, missing data: 6), MCS group (n = 92, missing data: 5), LIS group (n = 66 missing data: 3); asterisks significant difference between the three groups of respondents to the case, Kruskal–Wallis test (making correct diagnosis: H = 7.13, p = 0.028, after Bonferroni test, the scores in MCS is higher than LIS, p < 0.05; Evaluating resource allocation: H = 8.34, p = 0.015, after Bonferroni test, the scores in UWS is higher than MCS, p = 0.012).
Discussion
To describe the knowledge and attitudes of physicians regarding patients with some DoC and LIS in Eastern countries, we conducted a vignette-based survey among Chinese neurologists. This study reveals significant differences from previous studies conducted (in Germany and Canada), namely, lower diagnostic accuracy and less limitation of LST. This may be closely related to policies, cultures, economies, and laws among countries. A deeper understanding of neurologists’ moral beliefs and attitudes can inform healthcare policy and might point to areas of research and healthcare practice that need further regulatory attention. A normative orientation through institutional, regional, or national policies for decision-making can increase the likelihood of reaching consistent and transparent decisions about the care of patients with severe brain injury across different regions and cities.
The correct assignment of diagnostic categories to case vignettes
The overall accuracy rate of the assignment of a diagnostic category was lower in this study (62.8%) than in the studies in Germany (86%) and Canada (the latter only included UWS: 80.0%).17,20 The current medical practice in China plays an essential role in the explanation of this result. In Chinese traditional medicine, there were several relevant diagnoses related to the conditions now categorized as DoC, such as mental confusion, and coma. 5 Since the transference of the concept of DoC to the Chinese healthcare setting only started in the 1990s, 5 our study may have revealed a knowledge dissemination lag. At present, most Chinese medical institutions mainly use the Glasgow Coma Scale (GCS) total score to assess patients with severe brain injuries.22,23 It is well-known that the GCS cannot distinguish between coma, the UWS, and MCS.24,25 In some hospitals in developed cities and regions of China, the CRS-R in the translation by Zhang et al. is recognized as the standard tool to assess patients’ levels of consciousness.26,27 Meanwhile, the simplified evaluation of consciousness disorders (SECONDs) scale has been applied in China as an alternative to CRS-R.28,29 As more and more Chinese clinicians are researching patients with DoC, other tools have been created and developed for the identification of the residual physical and cognitive functioning of patients, such as the China Nanjing Persistent Vegetative State Scale. 30 These neurobehavioral assessment tools have nuanced assessment criteria and sometimes contain subscales for different dimensions. Experience with such assessment tools most likely influences not only the competencies but also the conceptualizations of neurologists. An advantage of using different scales to capture signals of consciousness is to minimize the risk of misdiagnosis, but it can also lead to contradictory results due to the differing criteria for judgment. Whether all reactions to stimuli represent signs of consciousness is still under debate.31–33 Through the dissemination of such tools, we can expect soon, that more neurologists will be aware of the differences between UWS and MCS. Furthermore, due to the low prevalence of LIS, 34 some Chinese physicians often confuse LIS with amyotrophic lateral sclerosis and provide the same treatment, which may be a potential factor contributing to the low accuracy of reported LIS diagnoses.
Neurologists more accurately assigned the diagnostic category of MCS to the paper case than UWS. The finding indicates that neurologists were very sensitive to behavioral signals of consciousness. They could correctly identify signals of awareness as meaningful responses to stimuli, whereas the description of reflexive behaviors may have been mistaken as signs of responsiveness. In a previous study, the highest diagnostic error rate has also been found according to the UWS. 6 Since in this study, more experience with patients with UWS was accompanied by a higher chance of choosing the correct diagnosis, creating opportunities for training at the bedside of such patients could be beneficial. Higher diagnostic accuracy rates could be achieved more quickly through a structured, patient-oriented training program for neurologists. 17
The residual capabilities of patients with UWS, MCS, and LIS
A large number of studies have shown that patients with UWS have impaired and disconnected residual brain activity, which reduces the likelihood of experiencing awareness of painful stimuli consciously. 35 However, when being asked about a patient’s residual capabilities in this study, most neurologists believed that patients with UWS are just as capable of sensing pain as patients with MCS and LIS. Our results are in line with previous findings regarding neurologists’ opinions on pain in UWS patients. 17 Several studies have shown that when patients with UWS are exposed to an electrical noxious stimulus or nociceptive-specific laser-evoked potentials, patients show activation of the affective pain network involving the sensory cortex and cingulate cortex, sometimes resulting in pain cries.36,37 Furthermore, 83% of patients with DoC displayed potential signs of pain during physiotherapy sessions. 38 Given these insights, it is questionable that patients with UWS cannot feel pain. 35 Potential pain could severely affect the patient’s response to commands, which can lead to misdiagnosis of a patient with UWS, whereas the patient is more likely to be in an MCS. Patients in the LIS can certainly experience pain. A recent study by Bonin et al. noted that 49% of the patients with LIS reported experiencing pain that interfered with sleep, quality of life, and cognition. 39 Such results emphasize the necessity of providing appropriate pain analgesic treatment to a person who is unable to communicate verbally and may be experiencing pain. Because they chose the presence of this residual capability, it is probable that the neurologists in this study are aware of the need for pain medication.
It is noteworthy that 21.7% and 38.3% of participants reported that UWS patients could be aware of themselves and their surroundings, which was much higher than that in Germany (9% and 6%) 17 and Canada (6% and 6%). 20 The high misdiagnosis in clinical practice may potentially affect this understanding because some MCS patients and LIS patients are sometimes mistakenly regarded as being in a state of UWS. At the same time, this raises concerns about the identification of covert consciousness and new classifications (such as cognitive motor dissociation, high-order cortex motor dissociation, and minimally conscious state stare). Because based on behavioral assessment, they are frequently misdiagnosed as UWS, it is qualitatively encouraged to use neuroimaging and electrophysiology as auxiliary means in Chinese medical centers.
Opinions about the limitation of LST
Chinese neurologists preferred not to limit LST for patients with DoC and LIS at a much higher rate than those in the German study (Germany: UWS group: 8%, MCS group: 18%, LIS group: 9% compared to China: UWS group: 46.7%, MCS group: 62.8%, LIS group: 66.7%) as well as North American and Europe.13–18 The Chinese sociocultural and legal context may account for this difference. East Asian culture, based on Confucianism, emphasizes charity-oriented and family-oriented social relations. Making medical decisions for patients that could lead to death is seen as contrary to such virtues. 8 China currently has no relevant laws that explicitly permit or justify withholding or withdrawal of LST. If neurologists stop providing LST to patients without the explicit permission of family caregivers, doctors may face legal charges. In cases where economic conditions permit, family members prefer to maintain the integrity of the family by opting for LST. In contrast to the German or other Western country context, there is also no promoting advance directives through which patients can decide for themselves how they want to be treated if they were faced with a chronic UWS. Although a small number of Chinese neurologists report that they would limit treatment under certain circumstances, they mostly show a low level of agreement when being asked about certain circumstances (Table 3). Even some neurologists, who stated they never limit patient treatment, provided contradictory responses when asked about certain circumstances.
Neurologists seem to be more in favor of limiting LST for patients with MCS than for patients in an LIS when they experience obvious suffering. Due to pontine lesions, patients with LIS are often unable to move their limbs in response to painful stimuli, which may potentially influence a neurologist’s assessment of pain in LIS patients. Following the previous work of members of our group, few neurologists might agree with limiting LST for patients in a LIS because the condition itself is not terminal. It might even be reversible, and the treatment might still be evaluated as beneficial by patients. 40 Yet, from a Western perspective, it might be morally challenging to prolong LST for a patient who does not give their current informed consent to the treatment.
When Chinese neurologists were asked about their treatment wishes, 42.2% of the participants said they would have made the same decision for themselves, while even a higher proportion 43.3% would have opted for less treatment, and 12.6% said they would have liked to receive more treatment. When compared to the results from Germany (where 71% chose the same decision, 29% chose less treatment, and 1% chose more LST), it becomes apparent that Chinese neurologists distinguish more between their attitudes toward themselves and others. 17 Chinese neurologists might prioritize the determination of what is in the best interests of patients with DoC over other considerations (e.g., the patient’s perspective or presumed will). Determining the best interest of a patient who is unable to communicate is always difficult. Doctors who manage to prolong a patient’s life are seen to be morally praiseworthy in the Chinese healthcare environment. Another interpretation would be that neurologists might fear legal consequences if they make the same decisions for their patients that they made for themselves. The lack of regulations may force some of them to agree with the prolongation of LST, even though they do not see the treatment as effective or beneficial for themselves. Legislation on advance directives has sparked a heated debate about patient autonomy in the Chinese city of Shenzhen in 2022. Although advance directives are currently only enshrined in local laws in developed cities, they still play a role in reducing medical decision-making disputes for patients who have lost their ability to execute their actual autonomy due to severe illness. 41
Ethical, clinical, and practical challenges
Deciding for patients in the absence of surrogates is considered an extremely challenging situation for the Chinese neurologists in our study. People in East Asian cultures place more value on family relationships than on individual rights.8,19 Therefore, medical decision-making is usually based on the principle that doctors provide families with medical information about patients, that they provide suggestions, and that family members make surrogate decisions based on a variety of factors (e.g., finances, prognosis, burden of care). In addition to this, other ethical challenges seem to be similarly present in China. This implies that, despite the differences in differing cultural and legal contexts, there could be universal challenges related to the treatment of these highly vulnerable patients.
Limitations
We had to exclude 137 (37.2%) questionnaires from the follow-up analyses due to the low percentage of correct diagnoses made by participants. This resulted in a one-third reduction in the sample size and burdened participants with giving answers to questions that did not result in interpretable data. According to Kendall’s principle, given the difficulty of the items in this questionnaire, we increased the sample size by 50%, which should be 188–375, so that the final sample size (N = 223) is still within a manageable range. Moreover, Nanjing, Guangzhou, Beijing, Hangzhou, Xiamen, and Nanchang, the cities where we distributed the questionnaires, are relatively fast-growing economies. Previous studies have suggested that the level of economic development is a potential factor influencing the development of medical and ethical practices. 42 Therefore, a similar study needs to be carried out in more regions in China to investigate whether in rural areas there are different patterns of experiences and attitudes. Our methodology only allows for comparing the application of neurologists’ knowledge to a hypothetical paper case, rather than utilizing structured neurobehavioral assessment tools or neuroimaging in real-world scenarios.
Conclusion
Our results highlight the need for more specific education and training on DoC and related conditions for neurologists in China. In contrast to neurologists in Western countries, most Chinese neurologists are reluctant to limit LST for their patients. With regard to UWS, only half of the neurologists are open to questioning LST under certain circumstances.
Supplemental Material
sj-doc-1-tan-10.1177_17562864241283328 – Supplemental material for Clinical and ethical challenges in decision-making for patients with disorders of consciousness and locked-in syndrome from Chinese neurologists’ perspectives
Supplemental material, sj-doc-1-tan-10.1177_17562864241283328 for Clinical and ethical challenges in decision-making for patients with disorders of consciousness and locked-in syndrome from Chinese neurologists’ perspectives by Meiqi Li, Yifan Yan, Katja Kuehlmeyer, Wangshan Huang, Steven Laureys and Haibo Di in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.