
Abstract
Late recovery of consciousness in vegetative state is considered as an exceptional outcome and has been reported prevalently in patients who suffered a traumatic brain injury. In these patients, the benefits of prolonging the rehabilitation, aimed at the recovery of autonomy in basic everyday activities, has been demonstrated. Here, we describe the application of an intensive multi-professional rehabilitation program carried out on a young female patient, with exceptionally late recovery of consciousness, specifically, after 7 years of vegetative state due to severe brain hemorrhage. Neuropsychological and functional assessment was conducted before and after the end of the rehabilitation program. In addition, functional magnetic resonance imaging (fMRI) and diffusion tensor imaging (DTI)-based probabilistic tractography were performed. Two follow-up neuropsychological and functional assessments were also conducted 6 and 29 months after the conclusion of the program. Functional results showed an improvement, maintained over time, in walking with assistance, cognitive efficiency, visual acuity and visual field, dysarthria, and execution of activities of daily living. Moreover, functional and structural magnetic resonance imaging (MRI) data documented the existence of preserved neural networks involved in sensory, motor, and linguistic tasks, which in all likelihood support the recovery process. This report suggests the possibility of undertaking an intensive rehabilitation program in patients who remain for long periods in altered states of consciousness, in spite of early negative prognosis.
Introduction
Much clinical research has focused on rehabilitation outcomes in relation to the period of time elapsed since severe acquired brain injury. 1 According to the historic study of the Multi-Society Task Force on Persistent Vegetative State, 1 the probability of recovery of consciousness could be considered negligible after 12 months of vegetative state in the case of traumatic brain injury and 3 months in the case of non-traumatic brain injury. Since then, many papers describing anecdotal cases of late recovery of consciousness have been published,2–6 and recently case series have been reported of patients who regained consciousness after an interval greater than 12 months in the case of traumatic brain injury and greater than 6 months in the case of non-traumatic brain injury (anoxic and vascular brain injury). 7
When patients come out of vegetative state, in most cases they enter minimal conscious state or a state of severe disability. 8 In this phase, 2 strong predictors of further functional recovery are transition time from vegetative state to minimal conscious state, which has been correlated with the probability of recovery of functional autonomy,9,10 and the duration of post-traumatic amnesia, which is correlated, in particular, with final cognitive impairment.11,12 Regarding the relation between the interval elapsed since the acute event and efficacy of rehabilitation, it is widely believed that early rehabilitation is a factor enhancing the quality of outcome after severe acquired brain injury,13–15 as well as the quality of recovery of cognitive abilities. However, the time to start intensive rehabilitation may depend on the severity of initial brain injury and comorbidity, rather than being an independent determinant of rehabilitation prognosis. 16
The repeated publication of single cases with a late positive course after severe acquired brain injury has led to the identification of a sub-population of patients, often young, defined as “slow to recover.” In these patients, the utility of prolonging rehabilitation aimed at promoting recovery of autonomy in basic everyday activities and self-determination through improved cognitive and behavioral skills17,18 has been demonstrated. Thus, 3 patterns of evolution can be identified after severe acquired brain injury: persistence of vegetative state, rapid recovery of consciousness, and slow recovery. The third category poses important medical, ethical, and economic sustainability questions about extending long-term access to rehabilitation programs to patients with protracted disorders of consciousness. 19
The aim of this article is to describe the outcome of a late recovery patient after the application of an intensive multi-professional rehabilitation program carried out on a young female patient about 9 years after brain hemorrhage due to rupture of an arteriovenous malformation. The event left the patient with severe disorders of consciousness for more than 7 years. The clinical history has been described extensively in a previous article. 20 Here, we also describe the results of 2 follow-up assessments conducted 6 and 27 months after conclusion of the program, as well as a neuroradiological investigation.
Materials and Methods
Case report
The female patient, of white race, now 28 years of age, suffered sudden loss of consciousness in March 2004, when she was 15 years old. 20 When she reached the hospital, she was scored in Glasgow Coma Scale 3; computed tomography (CT) scan showed a large intraparenchymal cerebellar hemorrhage from rupture of an arteriovenous malformation supplied by the posterior circle. The patient underwent surgery to remove the hematoma and malformation. The operation was complicated by repeated hemorrhage at the operation site, requiring multiple blood transfusions, and by 2 cardiocirculatory arrests. A second operation was necessary 3 days later to enlarge the craniotomy in the posterior cranial fossa due to increased intracranial pressure. Post-operative recovery was complicated by many infections and ventriculoperitoneal shunt obstruction, requiring repeated replacements. The patient remained in vegetative state with eyes fixed in central position, showing severe spasticity and repeated generalized epileptic seizures. The extent of the disorder of consciousness (DoC) was confirmed by the scores attributed to the patient through the assessment scales used in Italy in those years: Los Amigos Levels of Cognitive Functioning (LCF), 21 Level II, Disability Rating Scale (DRS), 22 Score 25, Glasgow Outcome Scale: vegetative state, 23 Modified Barthel Index (MBI) 24 Score 0/100, Category 1.
For about 7 years, she stayed in a nursing home near where her parents live. The score obtained in the evaluation scales and the clinical judgment were confirmed in 2 successive formal evaluations performed by a neurologist expert in the field of DoC in March 2006 and October 2010, confirming the apparent stability of the neurological picture. Her parents continued to care for and stimulate her, with the support of the staff. The first signs of recovery of consciousness were observed in February 2011: the patient was wakeful, did not respond to simple instructions but followed the examiner with gaze, first evidence of transition to minimally conscious state (MCS). In March 2013, after resolution of ongoing cranioplastic complications, the patient was admitted to our rehabilitation center where a first multidimensional assessment of her motor, visual, and cognitive status was made. 20
On admission, the patient was wakeful, conscious, and able to perform simple and complex requests. Severely impaired vision in both eyes, nystagmus in all directions of gaze, convergence insufficiency, exotropia and hypertropia of the right eye with deficit of adduction and depression of the right eye and deficit of elevation with slight abduction restriction of the left eye, left homonymous hemianopia, right homonymous upper quadrantopsia, dysarthria, mnestic deficit, and executive functions deficit with reduced illness awareness were recorded. Neuromotor status showed severe left spastic hemiparesis and right cerebellar hemisyndrome with dysmetria and kinetic tremor, reduced antigravity control of trunk, total dependence for basic activities of daily life. The Percutaneous Endoscopic Gastronomy (PEG) tube had previously been removed and the patient was able to feed without risk of inhalation, but she needed assistance because she could not bring food to her mouth. Full sphincter control had not been achieved yet, and episodes of incontinence were present.
Considering the exceptional conditions and the young age of the patient, we decided to apply immediately the rehabilitative intervention, sacrificing a possible research design (eg, A-B-A-B), that could have ensured, with high reliability, the link between the effects of the training and the possible improvement. The patient underwent a program of intensive multi-professional rehabilitation from April 2013 to December 2014, first as a full-time inpatient and then on a day hospital basis. After discharge the patient returned home, where she lives with her mother, and regularly attends a day center for brain injury patients. The family then activated a basic daily life autonomy support program and a socialization program in stimulating extra-family contexts, with the support of a peer tutor.
Procedures of testing
Before starting the program (T0), all fields to be rehabilitated were assessed. At the end of the program (T1), a second overall assessment was performed. Six (T2) and 27 months (T3) after the end of the intensive rehabilitation program, the patient underwent 2 further multi-professional follow-up assessments.
The patient was assessed using standardized assessment instruments, validated for the reference population. For the neuromotor evaluation, we used Trunk Control Test, 25 Tinetti Scale–Balance, 26 Tinetti Scale–Gait, 27 Motricity Index (right/left), 25 and Time Walking Test 28 (10 m, with operator).
The neuropsychological evaluation explored the domains of attention, visuo-spatial exploration, memory, abstract reasoning, problem-solving skills, by means of the tests Attentive Matrix, 29 Verbal Span, 30 Phonological fluency, 30 Abstract verbal judgment, 29 Street completion test, 29 Stroop Test, 31 Apple Test, 32 Wisconsin Card Sorting Test, 33 Verbal fluency, 34 Rey 15 words, 35 Raven Progressive Matrices (RPM), 36 Verbal IQ (Wechsler Adult Intelligence Scale–Revised [WAIS-R]), 37 and Visual Perceptual Test (TPV). 38 When possible, equivalent scores (ES) were calculated, in accordance with the Italian scoring system. 39 The ES allows the comparison between various tests and the following evaluation; it varies from 0 to 4, with “0” usually standing as “pathological” since it is seen in less than 5% of the control population; “ES 1” can be considered pathological in some cases considering the clinical context; “ES 2” and “ES 3” correspond to the mean of the control sample; “ES 4” corresponds to the values of the correct scoring, greater or equal to the mean of controls.
Visual functions assessment was performed with a standard visual acuity test, Goldman kinetic perimetry, 40 and Goal Attainment Scale (GAS). 41 GAS is a sensitive individualized, criterion-referenced method measuring specific outcomes on individual goals after a period of treatment and widely used to supplement standardized measures of outcome that investigated, pre/post treatment and in follow-up, the modification of specific parameters; in our article, we have analyzed compliance with the treatment, visual acuity, visual field, and visual fixation. The assessment of dysarthria was performed by means of dysarthria profile.42,43 For the assessment of functioning, we used LCF, 21 DRS, 22 Extended Glasgow Outcome Scale (GOS-E), 23 and MBI. 24 Activities and Participation Assessment was evaluated in accordance with the International Classification of Functioning, Disability and Health (ICF) standards.44,45
Multi-professional rehabilitative program
In line with evidence-based data,46,47 the intensive rehabilitation program was distributed over a period of 20 months, consisting of a first period of 20 weeks as a full-time inpatient (5 sessions per week) and a second one of 64 weeks as day hospital patient (155 sessions overall). In both periods, each session lasted at least 3 hours. The daily neuromotor program included supine mobilization and stretching of the cervical spine and left upper limb, and selective pelvic girdle strengthening; in sitting position, 48 selective activation exercises for muscles of the trunk, abdominal muscle strengthening, exercises for antigravitational control of the head and trunk; postural transition strategy exercises; in standing position, prolonged verticalization exercises, autonomous standing exercises for increasing periods with supervision and support of the right upper limb, standing weight-shifting and balance exercises. Then step training was conducted with an assistant; ascending and descending steps aided by 2 assistants; stimulation of sensory perception of body areas with and without visual control and verbal feedback to improve body image and oculomotor coordination in peri-personal space; fine motor exercises of the right hand, with grasping of objects, in preparation for occupational therapy.
The patient also underwent daily neuropsychological rehabilitation focused initially on recovering spatio-temporal coordinates by visual anchorage (eg, signs hung in her room), and then on verbal information learning and recall capacity. Facilitating strategies were used, such as absurd visual and mental images 49 and errorless learning. 50 Compensating techniques were used as external aids to memorization, 51 developed with the help of the Occupational Therapy Service: a smartphone to obtain the date and time, a weekly planning sheet to manage her calendar and a diary created with her mother’s help during the summer holidays, with photos and reference to experiences. Exercises to improve working memory were also proposed. 52 Emotional support and containment sessions were also held when the patient exhibited verbal content indicating emotional disquiet linked to increasing illness awareness. However, major amnestic difficulties prevented any structured psychotherapy.
The orthotic setting envisaged three 20-minute sessions per week with exercises to stimulate eye movements in various gaze positions to reduce the secondary effect of contracture of muscles antagonistic to the paretic ones, spatial exploration exercises consisting in seeking various stimuli (letters and words) on A4 and A3 sheets and on the PC, nystagmus control exercises involving contraction of the medial rectus muscles, treatment of poor vision and visual field deficit by stimulation with a Retimax Vision Trainer (CSO).53–55
Since language comprehension was sufficiently spared, daily speech therapy was mainly speech-oriented with activities to improve the different underlying systems (breathing, phonation, resonance, articulation). Regarding respiration, the focus was on increasing the duration of expiration and pneumo-phonic coordination through basic exercises for restoring phonation and resonance. Phonation involved lengthening phonation time, intensity control and variation of tone through exercises based on vocalization, sustained or varied in manner and time, or in the parameter considered. Articulation was mostly treated by repetition of groups of consonants and words, with or without hyper- and hypo-articulation or with contrasts like minimum pairs.
The patient participated in daily occupational therapy individually and in a group in the various laboratories of the center. The therapeutic program was aimed at achieving maximal functional autonomy compatible with complex residual disability, 46 seeking to personalize activities according to patient motivation and home life context. Focus was on personal care (personal hygiene, dressing upper part of body, make-up), cooking (preparation and creation of simple recipes), brief self-driven wheelchair trips to train orientation, spatial exploration, and memorization of useful routes. The patient was trained to use paper and IT devices (cell phone, tablet, PC) as support for planning and memorizing her activities, as well as to enable social interactions (email, social media). She also performed music therapy and art therapy and acted in the annual laboratory play.
Neuroradiological investigation
The patient underwent neuroradiological evaluation at T1 by functional magnetic resonance imaging (fMRI) and diffusion tensor imaging (DTI) to record the anatomo-functional substrate of the observed behavioral improvement. The paradigm performed in the fMRI session included a linguistic, a visual, and a motor task. The patient gave written and oral consent to participate in the study, in accordance with the Declaration of Helsinki, and for the medical information to be published. The protocol was approved by the local ethics committee (Comitato Etico Unico per la Provincia di Parma), code UNIPRMR750v1, reference n. 22511.
fMRI paradigm
Data for the fMRI acquisitions were obtained during 3 sessions in which 3 different tasks were performed: (1) verbal production task (VP), (2) visual stimulation task (VS), and (3) simple finger tapping motor task (FT). All tasks were arranged using a block-design paradigm, alternating a 30-second rest condition block with a 30-second active condition block, repeated 5 times. During the VP active condition, the patient was asked to continuously formulate in her mind sentences describing actions related to an object word displayed on LCD goggles. The object words included common objects and tools (eg, door, cigarette, ball, bike, pencil, and glasses). Six words were presented per block, one word every 5 seconds. The rest condition consisted in observation of a gray screen. In both active and rest conditions, the subject was asked to fixate a central red fixation cross. During the VS session, black and white chessboard squares (16 cm × 12 cm) were presented at a video rate of 25 frames per second (f/s). Black and white squares alternated at a rate of about 8 Hz. Rest condition was identical to that of the VP task. In the FT session, during the 30-second active condition, the subject was asked to perform simple finger tapping with the right, unaffected hand, at a frequency of 1 Hz, with eyes closed. In this session the goggles were switched off, and auditory instructions (GO, STOP) were given through the built-in MR scanner headphones. See Supplementary Materials for a detailed description of scanning procedures and magnetic resonance imaging (MRI) sequences’ parameters.
Results
Tables 1 to 4 show the scores of neuromotor, cognitive-behavioral, visual, and speech assessment at the different time points, including the 2 follow-ups. Tables 5 and 6 show the results of the functional assessment.
Motor assessment performed from 2013 to 2017 (T0-T3).

Neuropsychological assessment.

Abbreviations: CO, cut off; ES, equivalent score; LTM, long-term memory; NE, not executable; QVP, Visual Perceptual Quotient; RPM, Raven progressive matrices; SS, standard score; TPV, Visual Perceptual Test; WAIS-R, Wechsler Adult Intelligence Scale–Revised; WS, weighted score.
Borderline.
Pathological.
Assessment of visual functions with Goal Attainment Scale (GAS).

Abbreviation: ADL, activities of daily living.
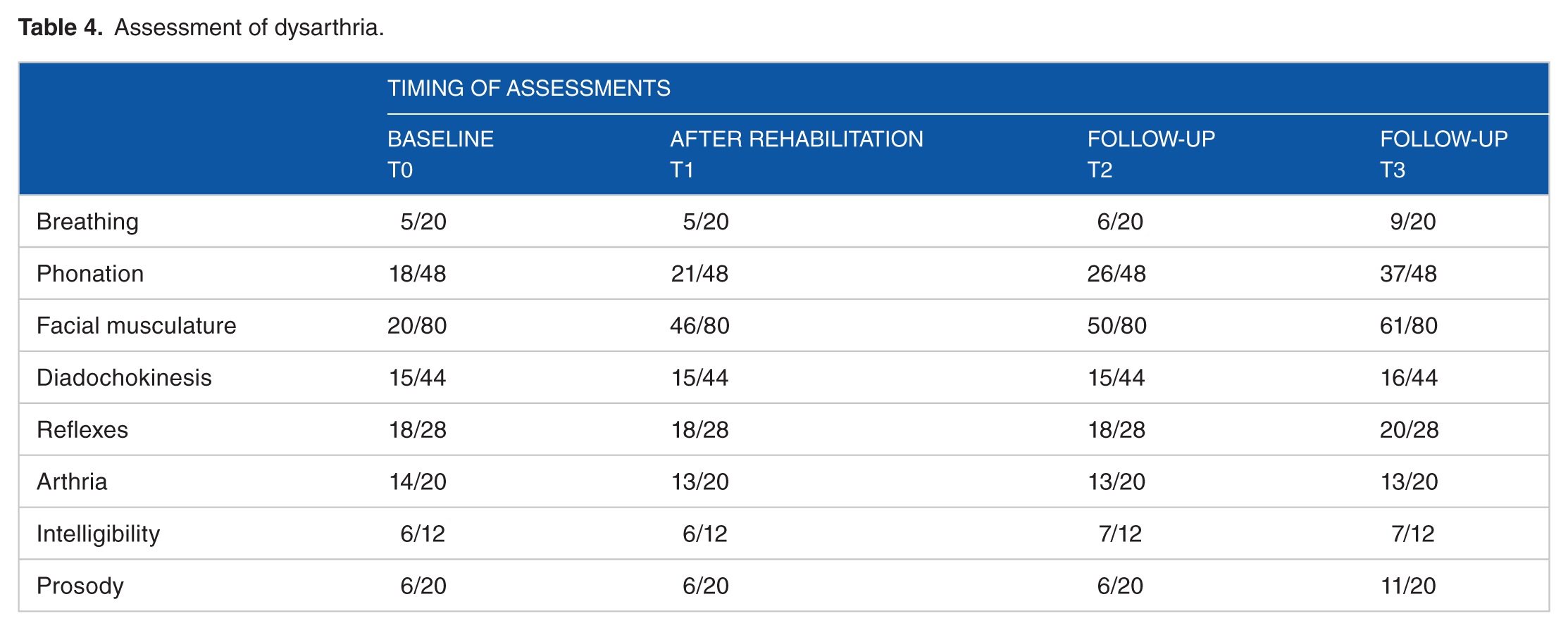
Assessment of dysarthria.
Assessment of functioning.
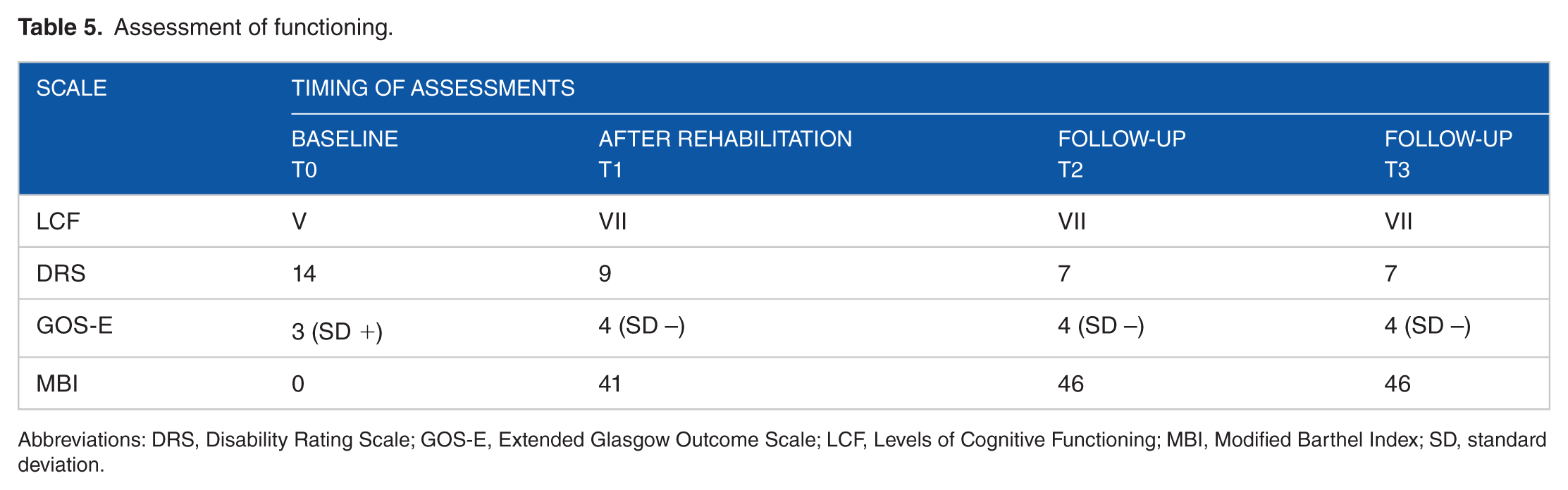
Abbreviations: DRS, Disability Rating Scale; GOS-E, Extended Glasgow Outcome Scale; LCF, Levels of Cognitive Functioning; MBI, Modified Barthel Index; SD, standard deviation.
Activities and Participation Assessment, in accordance with the International Classification of Functioning, Disability and Health (ICF).

(A) Activities and participation. The reported activities consist in the execution of a task or action by an individual and involvement in a life situation. The score indicates how much difficulty the person has in: P = performance; C = capacity. Score: 0 = no difficulty; 1 = mild difficulty; 2 = moderate difficulty; 3 = severe difficulty; 4 = complete difficulty; 8 = not specified; 9 = not applicable. (B) Environmental factors. F = facilitator; B = Barrier. Score: 0 = no barriers or no facilitator; 1 = mild barriers; +1 = mild facilitator; 2 = moderate barriers; +2 = moderate facilitator; 3 = severe barriers; +3 = substantial facilitator; 4 = complete barriers; +4 = complete facilitator. The letters in the leftmost column indicate the ICF domains (d) and environmental factors (e), followed by the item number.
Assessment of motor functions
At neuromotor level, improved anti-gravity control of the trunk was achieved at T1, as documented by the improvement of the score in the Trunk Control Test 25 (Table 1). The motor recovery of the lower limbs was modest (see right and left Motricity Index 25 in Table 1), but the patient learned how to use extensor spasticity of the left lower limb to maintain standing posture with anterior support from the upper limbs. As documented by the Time Walking Test, 28 the patient could walk for 30 m using a walker with forearm support and the aid of 2 assistants. Advancement of the right lower limb was good, but pelvic control was still poor. Upper limb movement had only a moderate improvement but, despite major cerebellar dysmetria, the patient learned to use the left upper limb to block objects that she could hold and handle with the right hand.
The motor performance remained stable in the 2 follow-up evaluations regarding the recovery of the antigravity control of the trunk and the voluntary motility of the lower limbs, while at the last follow-up the patient was no longer able to walk (Time Walking Test score = 0; see also Table 1).
Neuropsychological assessment
The neuropsychological assessment performed at T0, focused on verbal skills due to the visual deficit described above, showed a prevalent deficit of memory’s abilities and fragility of executive functions. At T1, severe amnesic and working memory deficit (encoding and recall) persisted, associated with visuo-perceptive and visuo-motor difficulties. Reasoning, logic, and attention were spared to a greater extent. Lexical processing and lexical semantic skills were normal. Temporal orientation continued to be poor and the patient needed semantic prompting to align correctly with time. Perceptive-cognitive assessment 38 showed that the patient could perform some tests that had been impossible in the first assessment. The results indicate major perceptive deficits in all the subtests presented.
Attention was satisfactory and accuracy good in barrage tasks. 29 In verbal memory, 30 span was normal, whereas learning and recall of verbal material were satisfactory for immediate recall and poor for delayed recall. At ecological level, major memory inefficiency in the management of certain activities was confirmed, including routine activities of daily life. Among executive functions, reasoning and cognitive flexibility tests were in the normal range, whereas organizational capacity, monitoring, and complex planning were penalized by mnestic and working memory difficulties. Verbal quotient in the WAIS-R tests 37 was on the whole within normal limits. Humor was generally good, although the patient sometimes manifested disquiet and a tendency to focus on recurrent ideas.
At the 2 follow-up evaluations, cognitive profile was overall maintained the same with respect to T1. Some slight improvements were observed at T2 in 1 of the 2 administered tests of phonological fluency, in the late recall part of a memory test and in digit span. Further evolution was observed at T3 for attentional capacity and speed of visual scanning.
Visual functions assessment
Concerning vision, an improvement in visual acuity was observed between T0 and T1, as well as increased contrast sensitivity and wider visual field as documented by the GAS 41 which highlights an improvement at T1 that affects significantly the activities of daily living (ADL) (see Table 3). Compared to baseline (2/10 for distance, 6 DW for near), the patient achieved a visual acuity of 3/10 for distance and fluctuated between 3 DW and 1 DW for near vision when she was better able to control nystagmus. Visual field, measured by Goldman kinetic perimetry, showed an enlargement of the perceived top and bottom right space and the ability to discriminate smaller luminous targets (from V/4 at T0 to III/4 at T1).
This made it easier to watch television, use a smartphone with its various functions (dialing numbers, writing messages, Internet navigation), and read texts with font size 12. The patient also achieved a wider field of spatial exploration, which improved her ability to orientate herself in her surroundings. In the 2 follow-up evaluations, the patient’s performance was identical to that of T1.
Speech control assessment
Regarding speech control, improvements in the number of expirations and in their coordination with words were recorded (Table 4). This made it possible to introduce more interesting activities (music, poetry, and rhymes) that were also useful for improving/maintaining the results obtained in speech articulation and intelligibility, as well as prosody: singing at the rhythm of her favorite songwriter, and reciting poetry, tongue-twisters and roles. At T1, even in the absence of significant changes to the scores at the Dysarthria Profile,42,43 improvements were recorded in the mean length of vocalization, pneumo-phonic coordination, and control of vocal intensity during conversation, with good initial repercussions on the fluency and intelligibility of her speech. The best performances were mostly recorded during exercises, whereas, in more natural situations of conversation, control of the different elements proved too complex. Although oro-facial musculature was not specifically treated, chewing and swallowing improved (see Table 4).
Analyzing the performance in the 2 follow-up evaluations, we noticed a progressive improvement in “Phonation” and a more evident improvement in the second follow-up in “Facial musculature” and “Prosody.”
Global functional assessment
Validated assessment scales for people with severe Acquired Brain Injury (Table 5) showed a steady improvement from the comparison of performance between T0 and T1. At the LCF Scale, 21 the patient passed from the “Level 5” (Confused, inappropriate, non-agitated) to the “Level 6” (Confused-appropriate). At the DRS, 22 she passed from “Severe Disability” (Score 14) to “Moderately Severe Disability” (Score 9). At the GOS-E 23 scale, the patient has evolved from “Lower Severe Disability” (Score 3) to Upper Severe Disability (Score 4). The assessment with MBI 24 demonstrated a change from a score of 0/100 at T0 to a score of 41/100 at T1.
Occupational therapy performance was evaluated by means of ICF recommended by the World Health Organization to describe the functioning of the person (Table 6). At T1, the patient continued to need help with basic ADL. However, she achieved modest autonomy in feeding herself with specially prepared food, in the use of a fork and in drinking from a glass. Supervision was required for minor bathroom hygiene with specially prepared articles. The patient collaborated actively with the aid of a guide rail when using the toilet.
Concerning complex activities, kitchen performance improved with the aid of certain auxiliaries for opening jars, cutting, and mixing (eg, special cutting board, non-slip film). To overcome the mnestic deficits, she used a recipes book made of rhymes to organize actions and correctly plan/carry out recipes. In guided personal computer use, performance was initially inhibited by mnestic, visual, and motor deficits that called for aids and strategies: keyboards with large, shield-shaped keys, large screen, and no mouse.
Performance gradually improved, and she was able to use the PC on a stand and the mouse, with size 12 characters and no other aids. She knew the main PC functions and procedures and at present performs them with constant supervision but minimal verbal help. She had personal email and Skype accounts and access to music websites. She used Facebook with guidance for the purpose of stimulating residual memory with photos and videos, eg, of her weekend activities. She independently managed calls and messages on her personal smartphone with magnified text. She still has severe difficulty in writing by hand, although a special pen is helpful.
Follow-up at 6 and 29 months after discharge (T2, T3; Tables 1 to 6) showed good capacity to maintain the achieved results, even more than 2 years after the end of the specific rehabilitation program, with a substantially stable score in all the domains explored with the “Short List of Activities and Participation” of ICF.44,45
Neuroradiological findings
Lesion analysis: the MRI anatomical acquisition (see Figure 1) revealed severe encephalomalacia, resulting in brain atrophy involving the right frontal lobe and the right supramarginal gyrus, with relative sparing of the rest of the parietal cortex. The damage also involved the superior temporal gyrus in the right temporal lobe with massive dilation of the temporal horn. The right occipital cortex appeared to be spared. There was localized atrophy of the left limbic isthmus and the splenium of the corpus callosum was also severely atrophic. Subcortically, there was clear extensive encephalomalacia of both cerebellar hemispheres and the vermis. There was also trapping of the fourth ventricle, causing compression of the brainstem and evidence of atrophy of the ventral portion of the pons.

T1-weighted MRI image, acquired at T0, is shown in 3 representative axial, coronal, and parasagittal slices.
fMRI results
During the VP task, there was significant activation of the anterior and posterior nodes of the language network in the left hemisphere, corresponding to the posterior part of the inferior frontal gyrus (Broca’s area, IFG) and the posterior part of the superior temporal gyrus (Wernicke’s area, pSTS), respectively (Figure 2). There was also activation of the anterior cingulate cortex (ACC) and of the occipital cortex plus the inferior temporal gyrus (ITG).

Brain activations during the performance of each experimental conditions: top, visual stimulation (VS) task; center, motor finger tapping (FT) task; bottom, verbal language production (VP) task. The activations, reported on both hemispheres and 5 axial representative slices, result from the contrast between each experimental condition and Rest. All activations are rendered in subject space and visual 3D rendering of gray matter (P < .05 FWE-corrected at voxel level). LH indicates left hemisphere; RH, right hemisphere.
Finally, subcortical activation was found at the head of the caudate nucleus. The VS task produced significant bilateral activation of the occipital cortex, presumably including the primary and secondary visual cortex. In the left hemisphere, there was posterior activation of the middle temporal lobe plus a small cortical sector linking the middle and superior temporal cortex. Thus, activation encompassed the primary visual and extrastriate areas. The FT task showed significant activation of the hand field of the sensorimotor cortex (M1/S1), the supplementary motor area (SMA), cingulate gyrus, the ventral part of the inferior parietal cortex (IPL), probably corresponding to the secondary somatosensory area (SII), and the ventral part of precentral gyrus, presumably the ventral premotor cortex (PMv) (Figures 2 and 3).

Brain activations resulting from the experimental conditions contrasted with Rest, reported in 5 representative parasagittal and coronal slices. Three different color scales show the activity associated with VS task (yellow), FT task (red), and VP task (green). All activations are overlaid in subject native space (P < .05 FWE-corrected at voxel level). LH indicates left hemisphere; RH, right hemisphere.
DTI-based tractography results
Figure 4 shows each tracked fasciculus in the left and right hemisphere. Tractography and orientated color DTI maps allowed us to define the large damaged cortico-subcortical region including the frontal and temporal lobes in the right hemisphere. An associative bundle with long and short fibers, presumably the inferior longitudinal fasciculus (ILF), connecting the occipital and temporal lobes was preserved (Figure 4A, blue tract). Trajectories of the corticospinal (CS) tract were still present but only in the left hemisphere (Figure 4B, green tract). The superior longitudinal fasciculus (SLF) was identified only in the left hemisphere, connecting the Wernicke territory with the IPL and the posterior part of the middle frontal gyrus (Figure 4C, red tract). Altogether, these data suggest that the recovery of visual function after intensive multi-professional program could be supported by the partial integrity of right occipito-temporal connections.

3D rendering of patient native gray matter space illustrating the DTI MR tractography results. Trajectories of the 3 identified main tracts in both hemispheres are shown. The bundles are color-coded: (A) blue, short, and long inferior occipital bundles connecting occipital and temporal areas (IOF), identified in both hemispheres; (B) green, corticospinal tract (CS) and its main fronto-parietal connections in the left contralesional hemisphere; (C) red, reconstruction of the superior longitudinal fasciculus (SLF) in the left contralesional hemisphere, connecting the temporo-parietal and frontal areas related to language processing.
Discussion
This study shows the improvements in several neuro-functional domains of a patient with a very late recovery of consciousness, supported by a multi-professional treatment and an active involvement of the parents. Specifically, the patient showed an improvement in walking with assistance, cognitive efficiency, visual acuity and visual field, dysarthria, and ADL execution. Most of these outcomes were maintained over time. Although the severe disability persisted, we hypothesize that the patient achieved important goals thanks to the combination of the rehabilitation program, parents’ care and, possibly, continuous spontaneous recovery.
Relevant factors for patient’s functional recovery
The results obtained in the various assessments made before and after treatment show improvement in the various functional domains that were the focus of the rehabilitation program. We believe that although protracted intensive rehabilitation was delayed due to the patient’s exceptionally late recovery of consciousness (7 years after the acute event), its efficacy probably had much to do with the convergence of many positive elements. The patient’s youth, the good level of education, and good health prior to the acute event certainly played a positive role. 56 The excellent standard of care during the years spent in a nursing home was certainly important, making it possible to avoid fatal complications and limiting secondary damage to the musculoskeletal system. Parental support was fundamental: the parents never ceased to believe that recovery was possible and were the first to observe the transition from vegetative to MCS. The program designed by our rehabilitation center followed the fundamental evidence-based recommendations for rehabilitation after severe brain injury. It was managed by a well-integrated multi-professional team from the beginning, 57 including active involvement of the family 58 and patient self-determination as soon as this was possible. It gave priority to task-specific therapeutic exercises to encourage independence in ADL.46,47 In relation to the patient’s impairments and their only partial reversibility (Tables 1 to 4), we gave priority to a program of occupational therapy aimed at maximizing autonomy (Table 5), also relying on aids and environmental adaptations and having the patient work in an ecological exercise context to favor generalization of the skills learned.
Although all the above reported factors have a very relevant role in the patient’s improvement, we cannot exclude that part of it could be accounted for by spontaneous recovery. This is mainly due to the fact that the patient was involved in a large multi-domain rehabilitation program, so that it is very difficult to quantify the possible contribution of spontaneous recovery by directly comparing the domains that underwent specific rehabilitation with untreated areas of disability.
Our hypothesis is that positive social factors such as family and other caregivers’ support, plus the patient’s strong compliance with the treatment, led to improvements in the overall functional and personal autonomy scores (Tables 5 and 6). This demonstrates the possibility of increasing performance under real-life conditions and of exploiting at their best the facilitating environmental factors (adaptation, mechanical and technological aids, removal of architectural barriers and social/family environment), in line with the principles of the ICF system. 44
Among the treated domains, not all of them showed a stabilized improvement at follow-up, eg, some aspects of motor control. In this respect, we suggest that the worsening of walking ability at the follow-up (still possible with much help at T1 and then no longer possible at T2 and T3) confirms the importance of motivation and performance effectiveness. In fact, the implicit patient’s evaluation of the cost/benefit ratio of a slow, strenuous, and non-functional walking has probably contributed to the abandonment of this movement modality in favor of the wheelchair.
Relation between preserved cortical networks and functional recovery
In this patient, the fMRI acquisition was performed only after the end of the rehabilitation program (T1) as no previous imaging data were available. Therefore, it is not possible to demonstrate specific post-therapy effects of brain reorganization. However, fMRI results allowed us to investigate the function of neural networks involved in sensory, motor, and linguistic tasks, providing further elements for the evaluation of patient preserved abilities.
The visual task was aimed at evaluating the network that could explain the patient’s improvement with the Retimax-based treatment, using the same type of stimulation also during fMRI acquisition. The activations are congruent with the data on improvement of visual acuity, showing, as expected, enhanced BOLD signal in the left primary and high order visual areas, suggesting that MT/V5 could play an important role in patient’s performance. Quite surprisingly, occipital areas of the right ipsilesional hemisphere also resulted strongly activated by visual stimulation. This activation could be due to partially preserved right optic radiation and/or to the transfer of visual information from the left hemisphere, although the corpus callosum tract was quite atrophic. Note, however, the lack of activation, in the right hemisphere, of high order occipito-temporal areas; it is therefore likely that the visual improvement on the treatment-specific task was mainly attributable to the left hemisphere activity. Beyond the activation of visual areas, there was a further cluster of activity in the left dorsolateral prefrontal cortex. This activation could be related to the need to inhibit saccadic movements toward the right visual hemispace, 59 mostly preserved in the patient, due to the task requirement to maintain fixation on the central cross. Interestingly, the probabilistic DTI-based tractography revealed the presence of the inferior longitudinal fasciculus, a ventral associative bundle with long and short fibers connecting the occipital and temporal lobes. The long fibers run medially to the short fibers and connect visual areas to the amygdala and hippocampus. 60 Indeed, the inferior longitudinal fasciculus is considered to be involved in visual perception,61,62 face recognition, 63 visual memory, 64 reading, 65 and other functions related to language. 66 Thus, the demonstration of the presence of the inferior longitudinal fasciculus appears to be in line with the behavioral outcome.
The motor task was quite simple (finger tapping) and revealed a classical network of sensorimotor areas in the left hemisphere, although the activation is probably lower than what one would expect in a normal subject. In the right hemisphere, due to the absence of these sensorimotor areas and of their connection, no activation was present. The DTI results clearly confirm the clinical data. Indeed, only the left corticospinal tract is preserved, showing all the parietal and frontal components from which it originates. This is in line with the described spasticity of the left hemi-body.
In the verbal production task, there is a clear activation of the classical language-related network, ie, the posterior IFG, the posterior Superior Temporal Gyrus (STG), the posterior frontal operculum and, in part, the insula. As the task requires the formulation of action sentences using names of objects and tools, it is not surprising to see the activation of movement-related areas, such as ventral premotor cortex, and high order visual areas, devoted to the elaboration of object meaning, such as the inferior occipital gyrus and posterior Middle Temporal Gyrus (MTG). The DTI results confirm the presence of the left SLF that includes the connection between posterior and anterior language-related areas. In healthy subjects, direct and indirect pathways compose the SLF. The direct pathway is known to connect Wernicke’s area territory (including areas belonging to the posterior part of MTG and STG) with Broca’s area territory including the IFG and the ventral premotor cortex. This segment of the SLF presents a hemispheric asymmetry, being larger in the left hemisphere, and is considered to play a relevant role in language-related processing. 67 The indirect branch of the SLF is composed by 2 segments: the posterior one connecting the Wernicke territory with the inferior parietal cortex and the anterior one linking the inferior parietal lobe with frontal areas including the ventral premotor cortex and middle frontal gyrus. 68 In the patient, all the major branches of SLF were preserved in the left hemisphere while it was not possible to identify any of these branches in the right, lesioned, one. Note, however, that, in spite of its presence, no activation possibly related to a pragmatic object representation was observed in the posterior parietal cortex. In principle, such an activation could feasibly be observed as many of the words used as stimuli referred to either graspable objects or usable tools.
Summing up, the fMRI study reveals activations compatible with those one would expect in normal subjects during the performance of visual, motor, and linguistic tasks. In addition, it shows the neural basis that likely underlies the effects of the multi-professional rehabilitation program. In this respect, it is worth to note that both the very plastic properties of the patient’s brain when the lesion occurred and the continuous multisensory stimulation received during the vegetative state period could constitute the main factors that kept the undamaged neural networks active.
Conclusions
The exceptionality of the case, characterized by late and complete recovery of consciousness in a young patient after 7 years of vegetative state due to severe acquired brain injury, allowed us to provide a longitudinal description of the long-lasting rehabilitation program put in place to support the path of progressive recovery of sensory, motor, and cognitive skills. At the time of discharge, we observed an overall improvement of the patient’s level of functional autonomy that has favored her reintegration into her social-family context with adequate support of her caregivers, even if we were unable to demonstrate with evidence-based approach a causal relationship between the rehabilitative treatment administered and the level of functional recovery. Nevertheless, we believe that this observational case report confirms the possibility and necessity of undertaking long delayed intensive rehabilitation programs even in slow-to-recover patients. The usefulness of repeated follow-up after the end of rehabilitation programs is confirmed, to document, as in this clinical case, the stabilization of the results obtained during the treatment process and to verify the patient’s functioning even in real-life contexts.
It is important to underline that the great organizational and economic burden for the national health system and the patient’s family calls for strict assessment of the prognostic factors of all candidates for such programs, and of their family social context, before committing patients to them. Wide prospective studies are needed on patients who remain for long periods in altered states of consciousness, 69 especially on the functional evolution of subgroups of slow-to-recover patients about whom only single case reports2–6,20 and a few case series8,56 are currently available. Research should focus on identifying reliable prognostic factors and tools for evaluating efficacy with respect to the use of specific rehabilitative methods (also through the use of neuroimaging investigations) that can be applied to single cases to help their families, clinicians, and policy makers in choosing long-term care and/or rehabilitation.
Supplemental Material
Supplementary_Material – Supplemental material for Application of an Intensive Rehabilitation Program After Very Late Recovery of Consciousness: A Single-Case Neurorehabilitation and Neuroimaging Study
Supplemental material, Supplementary_Material for Application of an Intensive Rehabilitation Program After Very Late Recovery of Consciousness: A Single-Case Neurorehabilitation and Neuroimaging Study by Antonino Errante, Donatella Saviola, Fabrizio Fasano, Benedetta Basagni, Serena Alinovi, Sara Bosetti, Margherita Chiari, Rita Minardi, Chiara Pinardi, Girolamo Crisi, Leonardo Fogassi and Antonio De Tanti in Journal of Central Nervous System Disease
Footnotes
Acknowledgements
The authors thank Debora Bertoni for help during the revision of the text. We also thank Gavin Burgess for proofreading the article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AE, LF and ADT designed and conceptualized the study; DS and BB collected neuropsychological and functional data; SA collected and analyzed neuromotor data; SB collected and analyzed occupational therapy data; MC performed the neuro-ophthalmologic assessment; RM collected and analyzed speech therapy data; GC performed the morphological investigation and lesion analysis. AE, FF and CP acquired and analyzed the fMRI and DTI tractography data; AE, FF and LF interpreted the fMRI and DTI data; all the authors contributed in drafting and revising the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.