
Abstract
Eculizumab has improved recovery from ventilatory support in myasthenic crisis (MC) cases. However, the safety and efficacy profiles from prospective studies are still lacking.
This study aimed to explore eculizumab’s safety and efficacy in a prospective case series of patients with refractory MC. We followed a series of anti-acetylcholine receptor (AChR) antibody-positive myasthenia gravis (MG) patients who received eculizumab as an add-on therapy for 12 weeks during MC to facilitate the weaning process and reduced disease activity. Serum anti-AChR antibodies and peripheral immune molecules associated with the complement pathway were evaluated before and after eculizumab administration. Compared to the baseline Myasthenia Gravis Foundation of America (MGFA)-quantitative MG test (QMG) scores (22.25 ± 4.92) and MG-activities of daily living (MG-ADL; 18.25 ± 2.5) scores at crisis, improvements were observed from 4 weeks (14.5 ± 10.47 and 7.5 ± 7.59, respectively) through 12 weeks (7.5 ± 5.74 and 2.25 ± 3.86, respectively) post-treatment. Muscle strength consistently improved across ocular, bulbar, respiratory, and limb/gross domain groups. One patient died of cardiac failure at 16 weeks. Three cases remained in remission at 24 weeks, with a mean QMG score of 2.67 ± 2.89 and ADL score of 0.33 ± 0.58. No significant side effects were reported. Serum CH50 and soluble C5b-9 levels significantly declined, while there were no significant changes in serum anti-AChR antibody levels, C1q, C5a levels, or peripheral lymphocyte proportions. Eculizumab was well tolerated and showed efficacy in this case series. Large prospective cohort studies with extended follow-up periods are needed to further explore the safety and efficacy profile in real-world practice.
Introduction
Myasthenia gravis (MG) is the most common autoimmune disorder affecting the neuromuscular junction (NMJ), predominantly characterized by antibodies against the acetylcholine receptor (AChR). The pathogenic autoantibodies inactivate the AChR primarily by blocking acetylcholine binding, promoting AChR internalization, and inducing complement-mediated tissue damage. Clinically, this results in muscle weakness and fatigability due to impaired NMJ signaling. An epidemiological study indicated a growing global incidence of AChR antibody-positive MG, estimated at up to 29 per million people annually. 1 According to the onset age and thymoma concurrence, anti-AChR antibody-positive generalized MG (gMG) can be further classified into early-onset MG (EOMG), late-onset MG (LOMG), and thymoma-associated MG (TMG). A national population-based study in China found that the age-standard mortality rate of MG was estimated at 1.86 per million people in 2020. The predominant underlying cause of death was MG, mostly from myasthenic crisis (MC), accounting for 87.19%. 2
MC occurs in approximately 15–20% of MG patients and is characterized by respiratory failure requiring mechanical ventilation (MV). 3 Currently, there is no high-level evidence supporting specific treatment options for MC, although intravenous immunoglobulin (IVIg) and therapeutic plasma exchange (TPE) are first-line rescue therapies.4,5 The disease burden for recurrent MCs is significantly higher than for those with mild-to-moderate MG. Patients who experience crisis events exhibit markedly increased healthcare resource utilization and costs in the 12 months leading up to the crisis. 6 Additionally, some patients respond poorly to rescue therapies, becoming ‘refractory’ and had experiencing prolonged dependence on MV.7,8
The precise molecular mechanisms underlying MC remain elusive, but current understanding suggests a complex interplay between immune dysregulation and neuromuscular dysfunction. Notably, a marked increase in AChR antibody levels may be associated with the onset of MC in certain patients. 9 Additionally, studies have reported a higher mean AChR antibody concentration in patients with MC than those with milder disease manifestations. 10 Further, our previous study identified pro-inflammatory CD4+ T cell signatures, particularly elevated Th1 and Th17 subsets during MC, highlighting the involvement of T cell-mediated immune responses in this condition. 11 Hypercytokinemia, driven by the innate immune system, has also been implicated in the pathogenesis of MC in our previous studies. 12 Moreover, evidence of classical complement pathway activation has been observed in anti-AChR antibody-positive gMG.9,13,14 Complement activation also plays a crucial role in MC pathogenesis, as indicated by the widespread destruction of the postsynaptic membrane at the NMJ in the intercostal muscles of MC patients. 15
Eculizumab, the inaugural complement inhibitor approved in the United States for treating anti-AChR antibody-positive gMG, offers alternative treatment options for patients with refractory gMG who show inadequate response or intolerance to conventional immunosuppressive therapy in the EU and China, or for those in Japan whose symptoms are poorly controlled with high-dose IVIg or TPE. 16 Real-world evidence substantiates the substantial benefits of eculizumab in managing refractory gMG. 17 Moreover, eculizumab has increasingly been explored as an adjunct therapy in patients with MC.8,18,19 However, prior evidence has primarily been derived from case reports. Prospective studies that thoroughly evaluate the safety and efficacy profile, particularly in terms of effects on various muscular domains and peripheral immune molecules, remain conspicuously absent.
The current study reported four anti-AChR antibody-positive gMG patients who experienced recurrent failures with routine rescue treatments during the MC. They were subsequently treated with eculizumab to inhibit the complement pathway. We conducted a prospective follow-up at 4-week intervals from the crisis (before eculizumab treatment) through 24 weeks after the initiation of eculizumab. The study assessed the safety and efficacy profile, along with changes in anti-AChR antibody levels, peripheral lymphocyte subsets, and immune molecules associated with the complement pathway.
Methods
Study subjects
In this study, we recruited patients diagnosed with AChR-antibody positive MG at Huashan Hospital, Fudan University, who had either refractory MC or a highly active MG course characterized by repeated MC episodes. Eculizumab administration began at the same time as an episode of MC. MG was diagnosed according to the established guidelines, 20 with positive AChR antibody testing, and congenital myasthenic syndrome and Lambert–Eaton syndrome were excluded.
Refractory MC was defined as patients who experienced repeated treatment failures despite receiving rescue therapies yet were unable to achieve complete weaning from MV. Common rescue therapies for MC included either monotherapy or a combination of IVIg and TPE. For those patients with MC who were refractory to these rescue therapies, intravenous methylprednisolone (IVMP) was used as an add-on therapy.
Highly active MG with repeated MC was defined as patients who had two or more recurrent MC episodes requiring rescue therapies such as TPE and/or IVIg, in line with the updated German treatment guidelines. 21 Patients who had difficulty in achieving complete weaning, mainly due to severe pulmonary infections, cardiac failure, or phrenic nerve palsy, were excluded from the study.
Baseline clinical features such as sex, age at the crisis, disease duration, gMG subtype, antibody type, thymus pathology, status with thymoma concurrence or history, comorbidities (hypertension, diabetes, hyperlipidemia, and other autoimmune diseases), and treatments administered during the crisis before eculizumab were collected at the time of crisis. Disease duration was defined as the onset of symptoms comparable to the gMG and the current MC event.
Prospective study design
The protocol for eculizumab treatment was set as 900 mg weekly for the first 4 weeks (induction therapy), followed by 1200 mg every 2 weeks (for maintenance therapy). All patients undergoing eculizumab treatment were administered prophylactic antibiotics until at least 2 weeks post-meningococcal vaccination. Clinical scores pertinent to MG were prospectively assessed at several time points: prior to initiating eculizumab and at 4, 8, 12, 16, 20, and 24 weeks thereafter. The assessments were conducted within a ±3-day window for each visit. These assessments primarily consisted of the Myasthenia Gravis Foundation of America (MGFA)-quantitative MG test (QMG) and MG-activities of daily living (MG-ADL).22,23 The total QMG score was divided into five sub-scores: (1) Extraocular muscle score, covering the first three items (double vision on lateral gaze, ptosis, and facial muscles); (2) Bulbar muscle, encompassing the fourth and fifth items (swallowing 4 oz. water, and the onset of dysarthria); (3) Gross motor score, including 6th, 7th, 9th, and 10th, 12th, and 13th items (arms outstretched, hands grip, and legs outstretched); (4) Axial motor score, for the eleventh item (head lifted); (5) Respiratory score, for the eighth item (Vital capacity, % predicted). The MG-ADL score was divided into four sub-scores: (1) Ocular score: double vision and eyelid droop; (2) Bulbar score: talking, chewing, and swallowing activities; (3) Respiratory score: breathing activity; (4) Limb score: the ability to brush teeth or comb hair, and arise from a chair. Minimal symptom expression (MSE) was defined as an MG-ADL score of 0 or 1. 24
Patient safety was assessed by monitoring various factors, including infectious episodes, laboratory diagnostics, and patient-reported adverse events. During their hospitalization, patients underwent weekly laboratory tests, which included routine hematologic evaluation, measurements of C-reactive protein levels, liver and kidney function tests, electrolyte panels, and urinalyses. Pulmonary CT scans were conducted during the crisis (before the eculizumab) and subsequently every 4 weeks in patients diagnosed with pneumonia. Ventilator-associated pneumonia (VAP), a subtype of ICU-acquired pneumonia, is characterized by an infection of the pulmonary parenchyma in patients exposed to invasive MV for at least 48 h.
Serum antibody testing, the 50% hemolytic complement (CH50), C1q, C5a, and soluble C5b-9
Serum samples were collected from patients for complement and antibody analysis prior to and 12 weeks post-eculizumab treatment. The anti-AChR antibody levels were measured by radioimmunoassay (Kindstar Global, Wuhan, China), with a cut-off value that was set at 0.50 nmol/L. The hemolytic activity of the classical pathway (CH50) was assessed using a liposome immunoassay (Wako Autokit CH 50; FUJIFILM Wako Chemicals, Osaka, Japan) according to the manufacturer`s instructions. The C1q concentration was measured using an immunoturbidimetric assay (Meikang, Zhejiang, China). Serum C5a and terminal complement component soluble C5b-9 (sC5b-9) were quantified using commercial enzyme-linked immunosorbent assay (ELISA) kits (Human C5a ELISA, Thermo Fisher Scientific, Waltham, MA, USA; Human sC5b-9 ELISA, Novus Biologicals, Littleton, CO, USA).
Flow cytometry immunophenotyping of cell subsets
Blood samples were drawn from each participant 12 weeks after initiating eculizumab treatment. The samples were collected into tubes containing EDTA and immediately sent for flow cytometry analysis from crisis (prior to the eculizumab) to 12 weeks post-treatment. The blood sample processing followed the protocol described in our previous study. 11 The frequency of CD4+T subsets was identified as follows: Treg (CD25hiCD127dim), Th1 (CXCR3+CCR6−), Th2 (CXCR3−CCR6−), Th17 (CXCR3−CCR6+), and Tfh (CXCR5+). Apart from the CD4+T profile, we performed flow cytometry following a similar protocol to define B cell and Natural killer (NK) cell as follows: total B (CD3−CD19+), Naïve B (CD19+CD27−), Memory B: (CD19+CD27+), Breg (CD19+CD24+CD38+), Plasmablast (CD19+CD27+CD38+), and NK (CD3−CD16+).
Standard protocol approvals and patient consent
The study was approved by the ethics committee of Huashan Hospital and joint institutional review boards (2020-883). Informed consent was obtained from each participant or their guardian if the enrolled patient was unable to assign the consent at crisis. Personal information or any personal identifiers, including names and dates of birth, were de-identified before database input to maintain privacy.
Statistical analysis
Data were presented as mean ± SD for continuous variables or n (%). Differences in the paired samples were assessed using a paired t test. Statistical significance was defined as a two-tailed adjusted p value <0.05. Statistical analysis was performed using GraphPad Prism 10.0 software (GraphPad Software, LLC, San Diego, CA, USA).
Results
Baseline clinical features and prior immunomodulatory therapies
Among all MG patients who had MC enrolled in 2023 (n = 53), we followed four AChR-antibody positive MC who had refractory MC or highly active MG course with repeated MC with the eculizumab initiation from the crisis. The clinical features are summarized in Table 1.
Basic clinical features and treatments prior to the eculizumab of the AChR-MC cohort.

Duration represents the onset of gMG symptoms to the development of MC.
AChR-Ab, acetylcholine receptor-antibody; EOMG, early-onset myasthenia gravis; gMG, generalized myasthenia gravis; IVIg, intravenous immunoglobulin; IVMP, intravenous methylprednisolone; LOMG, late-onset myasthenia gravis; MC, myasthenic crisis; TMG, thymoma-associated myasthenia gravis; TPE, therapeutic plasma exchange.
Case 1 (LOMG, refractory MC)
A 71-year-old male presented progressive respiratory distress for over 30 days and eventually developed respiratory failure requiring tracheal intubation in the local emergency room (ER). Physical examination revealed mild ptosis and diplopia, leading to a suspected and subsequently confirmed diagnosis of gMG via a positive anti-AChR antibody level of 6.066 nmol/L. During the crisis, he received repeated IVIg (0.4 g/kg over 5 days) and prednisolone (30 mg, daily). However, weaning him off the ventilator proved challenging so he was then referred to our hospital. This case was diagnosed as LOMG since no thymoma was detected by a pulmonary CT scan. After admission, the patient expressed concerns about high-dose prednisolone treatment, leading to the prompt initiation of TPE (five sections with 1 volume every other day). However, the patient was still MV-dependent. Then, we started eculizumab along with cefoperazone and sulbactam sodium (3.0 g, q12h) for treating VAP. The patient remained dependent on MV for 46 days before starting eculizumab treatment. Remarkably, just 1 week after initiating eculizumab, he was successfully weaned off the ventilator. Two weeks following his weaning, he was discharged from the hospital with a status of MSE. He then completed the meningococcal vaccination and continued the antibiotic prophylaxis with penicillin for another 14 days. After being discharged, he continued eculizumab biweekly, and his prednisone dose was gradually reduced to 5 mg daily over 24 weeks of eculizumab therapy.
Case 2 (EOMG, highly active MG course with frequent MC episodes)
A 34-year-old female had a history of pure ocular symptoms for 10 years before developing gMG which included difficulty in raising the neck and swallowing. She was positive for anti-AChR antibody (14.802 nmol/L) and was diagnosed as EOMG. Thymus hyperplasia was confirmed by the pathology after thymectomy. Notably, she experienced her first MC episode 30 days ago, which was successfully managed after undergoing one cycle of TPE, followed by low-dose steroid maintenance. However, she rapidly developed a second MC episode, necessitating emergent intubation. Repeated TPE and high-dose prednisolone (1 mg/kg/day) were given promptly. Unfortunately, she failed to respond to the rescue therapies, and thus eculizumab was initiated as an add-on treatment. Prior to starting eculizumab, she required MV for 17 days. The highly active MG course was rapidly controlled on the seventh day after eculizumab initiation, leading to successful tracheal extubation. She was discharged in the third week of eculizumab and received the meningococcal vaccine. Continuing with anti-meningococcal prophylaxis using oral penicillin for 2 more weeks, she persisted with eculizumab therapies. By the 12th week, she achieved MSE status and her prednisone dose was reduced to 10 mg daily after the 24th week.
Case 3 (TMG, refractory MC)
A 37-year-old male, suffering from progressive swallowing difficulties and respiratory failure for 3 months, was referred to our hospital while on MV. He tested positive for anti-AChR antibody (20.422 nmol/L). A pulmonary CT scan revealed an unresectable thymoma previously classified as pathology B3. Initial treatment included a course of TPE (1.0 volume for each session every other day, five sections) followed by IVIg at a dosage of 0.4 g/kg/day for 5 days. Despite these interventions, the patient was still MV-dependent, prompting the administration of IVMP. After 1 month, as he still required ventilatory support, eculizumab was initiated along with ceftriaxone. Before the eculizumab treatment, he had been on MV for 32 days. Thirteen days after starting eculizumab, the patient began attempts for weaning and successfully weaned by day 27 post-treatment. Noticeable enhancement in muscle strength was observed in both the limbs and the swallowing muscles. After improving and weaning off the ventilator, the patient received a meningococcal vaccine and continued with ceftriaxone for 2 weeks to prevent meningococcal infections. Another 2 weeks later, he was discharged and continued to receive eculizumab infusions every 2 weeks. Additionally, the patient underwent radiotherapy to treat an unresectable thymoma. At the 24th week, his prednisone dosage had been reduced to 15 mg daily.
Case 4 (TMG, refractory MC)
A 64-year-old female exhibiting ptosis and progressive respiratory distress over 3 months was diagnosed with a large thymoma via pulmonary CT scan. She underwent surgical resection (confirmed B3 pathology) and was prescribed prednisolone (20 mg/day) for 2 weeks. Her serum anti-AChR antibody level was 10.528 nmol/L. Three days after the thymectomy, she developed MC and cardiac dysfunction at a local hospital. Despite receiving repeated IVIg and IVMP treatments, she remained MV- dependent for over a month before being transferred to our hospital. Upon admission for MG management, the patient was promptly treated with intravenous eculizumab. Concurrently, the patient also had a severe pulmonary infection which was treated with meropenem, guided by antimicrobial susceptibility testing. As the pulmonary infection improved, the antibiotic regimen transitioned to ceftriaxone for ongoing prophylaxis against Neisseria meningitis. The patient’s muscle strength in limbs and swallowing significantly enhanced. Before starting eculizumab treatment, the patient had been on MV for 35 days. After 3 weeks of eculizumab treatment, she started weaning attempts and was transitioned from the ICU to the regular Neurological ward. At 12 weeks, she was no longer on a ventilator during the daytime. Strength in ocular, bulbar, and limb muscles gradually improved after 4 weeks with eculizumab. As a result, the nasogastric tube was removed while the patient was not on ventilation during the daytime. Despite the VAP and the MG being well controlled, she experienced hypotension and eventually passed away due to cardiac failure at 16 weeks.
The clinical outcome and MG-relevant score changes
All four cases maintained Eculizumab with good tolerance. All patients were successfully weaned without further need invasive MV, except for Case 4, who still required it during the nighttime. The changes in QMG and MG-ADL scores every 4 weeks after the addition of eculizumab are listed in Table 2.
Changes in QMG and MG-ADL score of the AChR-MC cohort.


AChR, acetylcholine receptor; MC, myasthenic crisis; MG-ADL, myasthenia gravis-activities of daily living; QMG, MGFA-quantitative MG test.
The baseline QMG score for four cases was 22.25 ± 4.92 and the baseline MG-ADL was 18.25 ± 2.5. After starting eculizumab, there was an improvement in total QMG and MG-ADL from four weeks (14.5 ± 10.47 and 7.5 ± 7.59, respectively) through 12 weeks (7.5 ± 5.74 and 2.25 ± 3.86, respectively). Three out of four (Cases 1–3) patients achieved MSE after completing nine infusions with eculizumab. They remained in remission at 24 weeks with a mean QMG score of 2.67 ± 2.89 and ADL score of 0.33 ± 0.58. Improvements in muscle strength across ocular, bulbar, respiratory, and limb/gross domain muscle groups were demonstrated in four cases, which is consistent with the findings from the Phase 3 registration trial of eculizumab in patients with refractory gMG (REGAIN study).25,26 Relatively speaking, the strength in ocular and bulbar muscles significantly ameliorated in comparison to respiratory and gross/limb muscles (Figures 1 and 2).

The changes in QMG after eculizumab treatment for 24 weeks and the impact on different muscle subdomains were presented.

The changes in MGFA-ADL after eculizumab treatment for 24 weeks and the impact on different muscle subdomains were presented.
The safety profile of eculizumab was consistent with REGAIN. No cases of meningococcal infection were reported during the 24-week follow-up period. Three patients had VAP (Cases 1, 3, and 4) and were identified with pseudomonas aeruginosa and klebsiella pneumoniae from sputum or bronchoalveolar fluid culture. Based on the drug sensitivity analysis, cefoperazone sulbactam and meropenem infusions were given, respectively. VAP was regularly monitored and well controlled. Transient joint pains in hands and ankles were reported in Case 2 for eculizumab infusion for 2 days and did not require any intervention.
Serum antibody, serum CH50, and sC5b-9 changes
In all four patients with MC, there was a significant decrease in serum levels of CH50 (36.25 ± 2.90 U/mL versus 13.65 ± 4.02 U/mL; p = 0.016) and sC5b-9 (3207 ± 591 ng/mL versus 179.7 ± 28.70 ng/mL; p = 0.0018) following 12 weeks of eculizumab treatment (Figure 3(a) and (b)). However, no significant changes were observed in anti-AChR antibody levels (12.95 ± 6.13 versus 9.85 ± 9.40 nmol/L; p = 0.6857), C1q (159.30 ± 55.89 versus 166.10 ± 17.35 mg/L; p = 0.6857), and C5a (28.40 ± 4.80 versus 26.80±6.11 ng/mL; p = 0.4496) after eculizumab treatment (Figure 3(c) and (d)).

Serum complement activation parameters at baseline (prior to eculizumab treatment) and 12 weeks post-eculizumab administration. The levels of CH50 (a), soluble C5b-9 (sC5b-9) (b), C1q (c), and C5a (d) were demonstrated in the four patients.
Peripheral immune subset changes
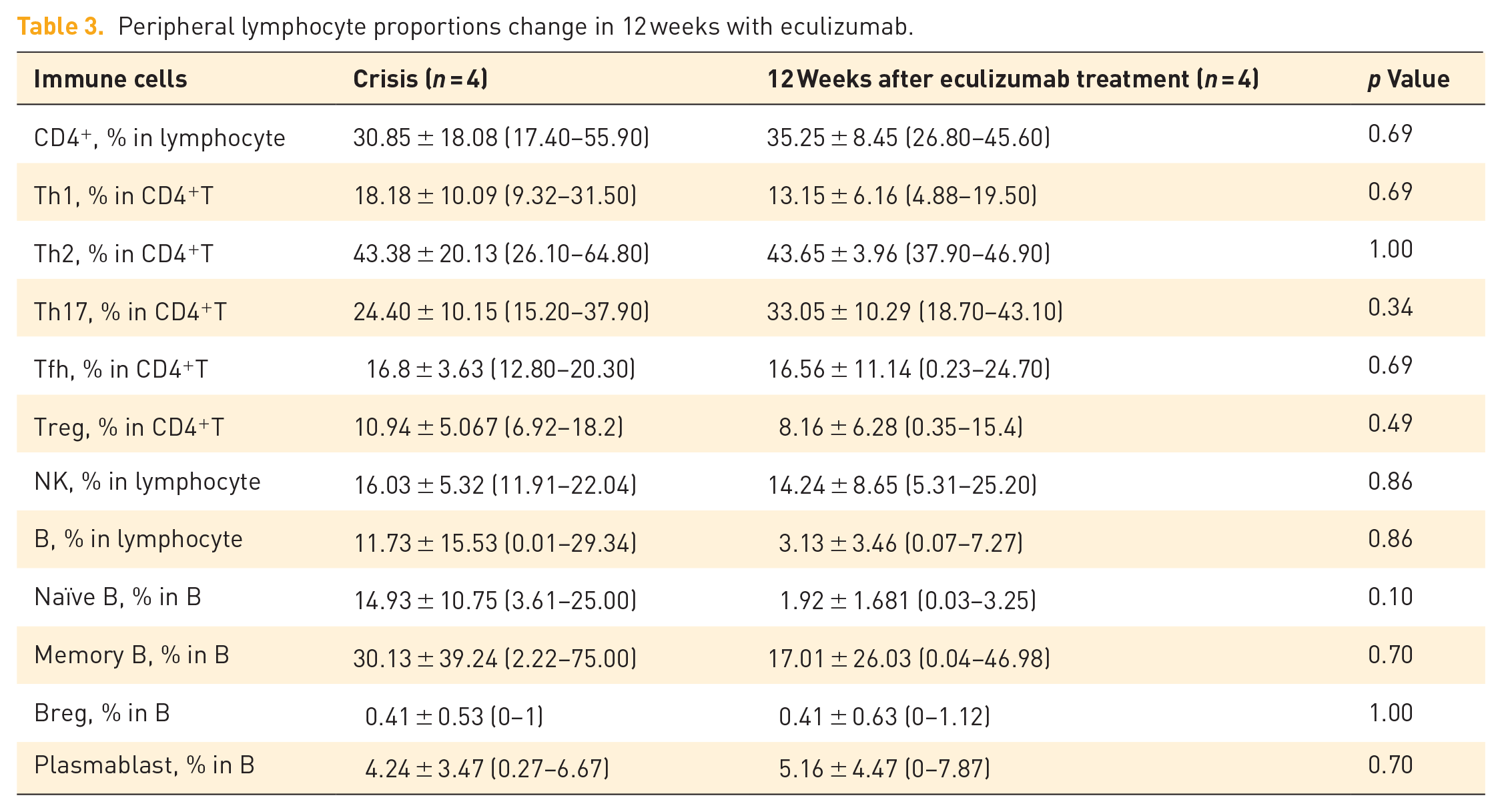
The proportion of lymphocytes, including CD4+ T, B cells, and NK cells, exhibited no significant changes before and after eculizumab treatment. Moreover, CD4+ T subtypes, including Th1, Th2, Th17, Tfh, and Treg, did not change significantly after 12-week eculizumab treatment (Table 3).
Peripheral lymphocyte proportions change in 12 weeks with eculizumab.
Discussion
Patients with refractory MC and highly active MG face a significant disease burden and thus require comprehensive management to prevent the occurrence of long-term sequelae and death. Eculizumab has been reported to be beneficial in facilitating the weaning process for several patients with MC. However, its effects on different muscle domains are not yet fully understood. To the best of our knowledge, this study is the first prospective case series of MC treated with eculizumab, documenting longitudinal changes in clinical scores and peripheral immune molecules related to the complement pathway.
Eculizumab received approval from the National Medical Products Administration in China in June 2023. There are concerns about the safety of using eculizumab in patients with MG who require MV. The main risk is the high likelihood of developing infectious events, particularly pneumonia. 27 MG patients, especially those with a history of long-term immunotherapies, thymoma, or previous radiotherapies and chemotherapies, often exhibit a reduced response to antibiotics compared to healthy individuals. Given that pneumonia significantly contributes to mortality in MG patients − even with timely diagnosis and treatment − caution is essential when administering eculizumab as a rescue therapy, as it may worsen these or other infectious conditions. 28 Moreover, patients undergoing eculizumab treatment cannot receive the anti-meningococcal vaccination due to their severe health condition and the use of MV during MC. Our previous study discussed the microbial spectrum and drug resistance of pneumonia in MG patients, 29 revealing that nonfermentative Gram-negative bacilli were the predominant pathogens, with a notable 42.86% demonstrating resistance to carbapenem. Therefore, early empirical intervention and close monitoring for pneumonia in MC patients undergoing eculizumab treatment are critical to ensure their safety.
The impact of eculizumab on different muscle domains of MC remains unexplored. Ocular, bulbar, respiratory, and limb/gross motor muscle groups are the four main domains of symptoms. The four domain scores of each of the MG activities of ADL and QMG scores were analyzed based on the results of REGAIN study (NCT01997229) and the open-label extension trial (NCT02301624). 25 During the REGAIN study, the peak improvements in MG-ADL scores were observed by week 16 in ocular, bulbar, and limb/gross motor muscle groups, except the respiratory domain, in which it was observed by week 4. The QMG scores of the four domains also showed significant improvement, and the respiratory domain also showed the highest improvement, followed by the bulbar domain. Peak improvements were observed by week 26 in the ocular and gross motor domains. In our cases, we revealed that there was a significant improvement in the ocular and bulbar domains after using eculizumab. However, we observed that the improvement in respiratory and limb/gross motor muscle groups may have been slower to react to the treatment. This could be due to the refractory nature of MC cases and the fact that respiratory muscles are more prone to being affected. Additionally, animal models with experimental MG showed that the intrinsic complement regulatory activity decreased in extraocular muscles, which suggests that eculizumab treatment may be more effective in improving the ocular domain. 30
Multiple studies have reported the effects of eculizumab on peripheral molecules in the complement pathway. 31 Using the Wieslab activity ELISA assays for measurement of classical and alternative pathways activity of complement,32,33 CH50 has been shown to reflect C5 blockade in patients treated with eculizumab and is directly related to eculizumab concentrations. 34 The definition of complete blockage was defined as <10% of complement activity using CH50 Wieslab ELISA or the hemolytic assays, as endorsed by a consensus guideline. 35 The spiked sera and patient samples showed complement blockage with CH50 when eculizumab >100 μg/mL. Although the use of activation products such as C5a and serum membrane-associated complex (sMAC) was also suggested, 36 it was proven to be unsuitable for monitoring because of the shorter half-life for C5a and inconsistency of in vitro and in vivo results for sMAC. In contrast, sC5b-9 levels exhibited a good correlation with the anticomplement therapies.
It has been reported that eculizumab treatment modulates the proportions of peripheral lymphocytes in MG patients. 37 For instance, CD4+ effector memory T cells decrease and CD4+ central memory T cells increase, while there are no significant changes in CD4+ and CD8+ T cells. In addition, Th1/Th17 responses are closely related to MG immunopathogenesis38,39 and the function of complement activation in this process has been indicated in infection, allergy, and transplant models.40–43 In this study, we observed an increase in the Th1 response during the crisis, followed by a decrease after eculizumab treatment. The Th17 response was augmented after treatment, which is consistent with the findings in our previous prospective studies on peripheral CD4+ T profile from the crisis to post-crisis state. 11 However, the combination of corticosteroids, IVIg, and plasma exchange would largely impact the peripheral immune subsets.
Our study encountered a limitation in its methodology that involved the timing of clinical evaluations following the initial administration of eculizumab. These assessments were postponed preventing interference from the effects of MV. In future work, we will implement immediate evaluations to promptly discern the effects of eculizumab on MC. Additionally, this study was restricted by the small size of the participant group and the brief duration of observation. Pre-treatment factors also played a role in patient recovery, particularly in the context of weaning from MV. The assessment of bulbar function was another challenge, often confounded by the use of nasogastric tubes that led to inflated scores. Upcoming research will focus on a comparative analysis of eculizumab and standard treatments, its combined application with immunosuppressants for prolonged efficacy, and an investigation into the baseline characteristics of MG to further delineate the role of eculizumab in treating MC.
Conclusion
Eculizumab exhibited a tolerable and efficacious profile in treating patients with MC. The drug has been found to improve muscle strength in various muscle groups across ocular, bulbar, respiratory, and limb/gross domain muscles. Additionally, eculizumab treatment resulted in a decline in serum CH50 and sC5-b levels. Larger sample sizes and longer follow-up periods are needed for future prospective cohort studies.