
Abstract
The locked-in syndrome (LiS) is defined as the loss of most voluntary muscle movements with preserved cognitive abilities due to a ventral pontine lesion. However, some patients may also have severe impairment of consciousness [locked-in plus syndrome (LiPS)]. Here we aimed to explore structural differences between LiS and LiPS patients of vascular aetiology, focusing on lesion patterns and locations to better delineate the clinical spectrum of LiS and LiPS. In this retrospective case series study, we report nine patients (two women), ages 29–74 years (median 50) with LiS and LiPS who were diagnosed between 2007 and 2021. Clinical parameters, MRI findings including the lesioned structures, and a shape feature calculation are presented for every patient. The lesioned structures were determined by a senior neuroradiologist. Two of nine patients had fully retained consciousness (LiS) and seven showed various degrees of impaired consciousness (LiPS). Lesions of LiS patients are round and confined to the pons, whereas lesions of LiPS patients are more elongated and reach neighbouring areas such as the mesencephalon, thalamus or ascending reticular activating system. Lesions involving the mesencephalon and the thalamus are strong indicators of LiPS, whereas for lesions restricted to the pons, the dorsal extension and the associated damage to the ascending reticular activating system are crucial to differentiate LiS from LiPS. Recognizing LiPS using clinical and radiological findings is important as these patients may need different therapies and care and, most importantly, should not be mistaken as unresponsive wakefulness syndrome.
Keywords
Introduction
The locked-in syndrome (LiS) is one of the severest chronic neurological conditions, defined as a loss of all voluntary muscle movements (complete de-efferentation) except vertical eye movements and blinking motions combined with preserved cognitive abilities. 1 The clinical entities of total and incomplete LiS were characterized by Bauer et al. 2 in 1979 reflecting the fact that some patients present with loss of all motor abilities (i.e. total LiS) or additional preserved motor activity compared to the classical form (incomplete LiS). Moreover, involuntary movements were described in LiS patients which have to be differentiated from voluntary motor activity. 3 In a review of 139 cases, 89 patients were diagnosed as classical, 46 as incomplete and 3 as total LiS. 4
The most common aetiologies of LiS are either ischemic infarction or haemorrhage in the vertebrobasilar artery territory 4 but mechanical brainstem herniation, 5 aortic dissections, 6 invasive fungal rhinosinusitis, 7 primary 8 or metastatic 9 brainstem tumour, pneumococcal meningitis, 10 basilar migraine 11 and others have been reported. Recently, LiS cases were associated with the COVID-19 disease. 12 Mortality is significantly lower in cases of non-vascular origin 4 and reversal of LiS may be achieved in cases of mechanical brainstem indentation, due to increased intracranial pressure or tumour growth.5,13 Moreover, locked-in-like states that show the same symptoms but no brainstem lesion can be caused for instance by late-stage amyotrophic lateral sclerosis. 14
Despite the fact that most patients do not recover, the survival rate is quite high if a patient can be medically stabilized, especially if s/he survives the first few months after the onset. 15
In 2013, the term locked-in plus syndrome (LiPS) was introduced to describe patients who on top of symptoms of classical or total LiS suffer from impaired consciousness 16 (Figure 1). Here we aim to revisit the subcategorization of LiS based on clinical grounds and structural MRI lesion pattern of vascular aetiology LiS cases to better delineate the spectrum of LiS and to improve the understanding of this syndrome and its varieties.
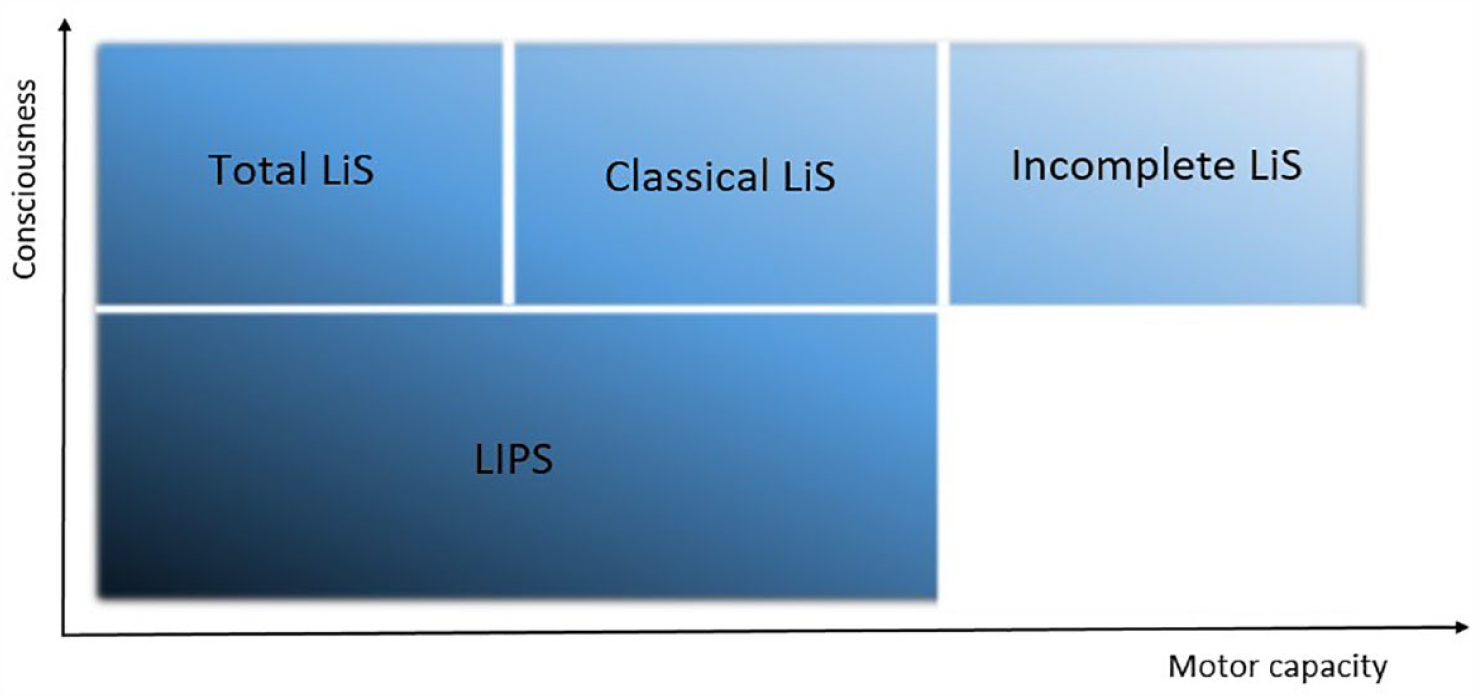
Schematic illustration of the locked-in syndrome and its varieties.
Methods
We identified nine patients with LiS or LiPS through electronic charts of a medical centre that specializes in intensive neurological care and neurorehabilitation. Nine women and men of all ages were included, who all had at least one MRI scan and showed a pontine lesion. No locked-in-like states (e.g. late-stage amyotrophic lateral sclerosis cases) were included.
A senior neuroradiologist (MMcC), blinded to the clinical picture of the patients, examined the available cerebral CT and MRI scans. All patients showed structural damage of the ventral pons; lesions beyond that were no reason for exclusion. The lesioned structures were documented, on each MRI, in case there were repeated investigations in a patient and the best quality MRI images extracted [T1 or FLAIR (fluid-attenuated inversion recovery)] for further analysis. In patient 5, only an acute MRI was available and therefore an apparent diffusion coefficient (ADC) measure was displayed. At least one axial image in the thalamic, mesencephalic and pontine plane is reported here for each patient; the exact planes were chosen individually for each patient to show the lesion optimally.
Clinical data of these patients were reviewed including medical reports, Coma Recovery Scale-Revised (CRS-R) 17 Scores and electroencephalograms (EEGs). After extracting the clinical data, the patients were classified as LiS (patients whose consciousness was fully retained) or LiPS (patients with impaired consciousness in addition to typical LiS symptoms).
MRI scans including a 3D sequence, obtained in the subacute or chronic phase, were further analysed. The scans were segmented semiautomatically using the grow from seeds algorithm of 3D Slicer software package18–20 to identify the lesions and calculate different 2D and 3D shape features, for example, the elongation. 21 A physicist (JS) and a senior neuroradiologist (MMC) controlled the output for errors.
Results
Nine patients (two women) were identified, and the median age at the onset of the disease was 50 years (range 29–74). Two patients showed normal consciousness (LiS), whereas seven had impairments in consciousness (LiPS). In the following, we describe the relevant lesions in the brainstem and thalamus of each patient and the most important clinical findings. More details on demographic information and the course of the disease of these patients are shown in Table 1. The complete imaging findings are reported in Table 2.
Patients’ demographic and clinical information.

BT, basilar thrombosis; CRS-R, Coma Recovery Scale-Revised; LiS, locked-in syndrome; LiPS, Locked-in Plus Syndrome; M, man, NSAID, non-steroidal anti-inflammatory drug; PPI, proton pump inhibitor; TICI, Thrombolysis in Cerebral Infarction Scale; W, woman.
Patient imaging.

of the lesion.
CT/CTA, computed tomography/computed tomography angiography; MRI, magnetic resonance imaging.
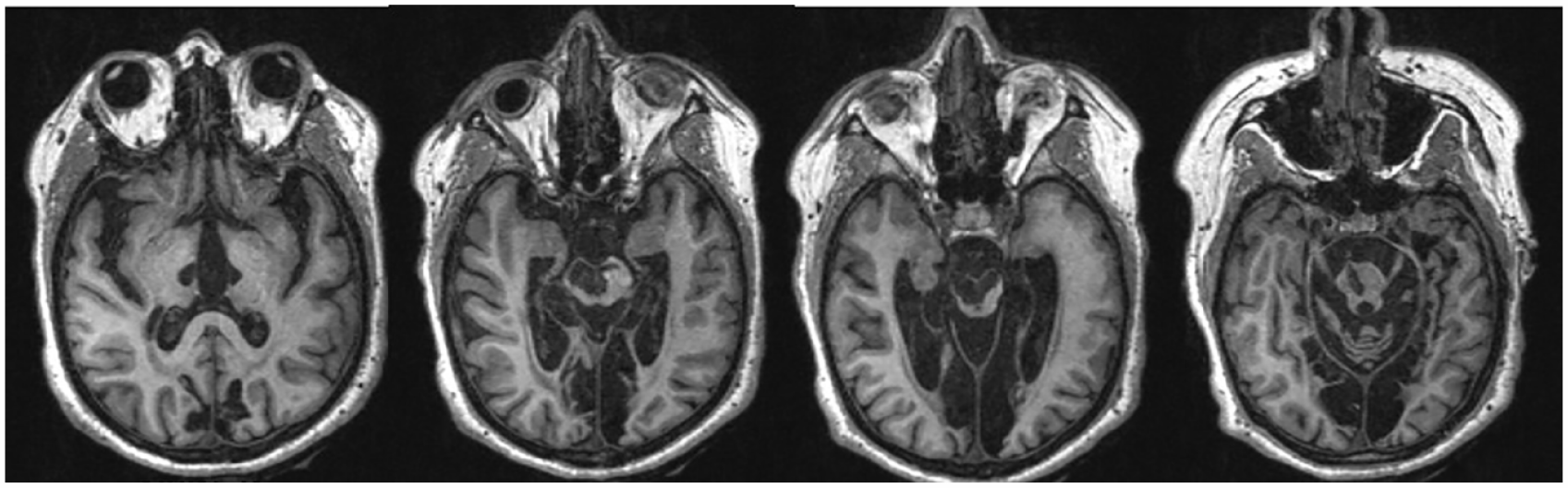
Patient 1 had bilateral and extensive lesions in the pons, the mesencephalon, the thalamus, and possibly the reticular formation (see Figure 2). Furthermore, a small haemorrhage ventral in the pons and enlargement of the aqueduct, and the fourth ventricle, secondary to the ischemic infarction in the pons and mesencephalon. Consciousness was severely impaired with CRS-R Score 3 at discharge. Spontaneous eye opening was observed but no signs of conscious awareness could be detected despite multimodal testing neither in the acute nor in the chronic phase. More than 1 month after onset, EEGs repeatedly showed diffuse slowing with occasional reactivity after painful stimuli. An EEG 3 years after onset showed a pathological alpha activity with minimal reactivity to painful stimuli. This patient suffered from LiPS on the most severe end of the spectrum.

MRI image (T1) of patient 1 showing axial planes of the thalamus, the upper/lower mesencephalon and the pons (from left to right). Lesions can be seen in the thalamus, mesencephalon and pons bilaterally.
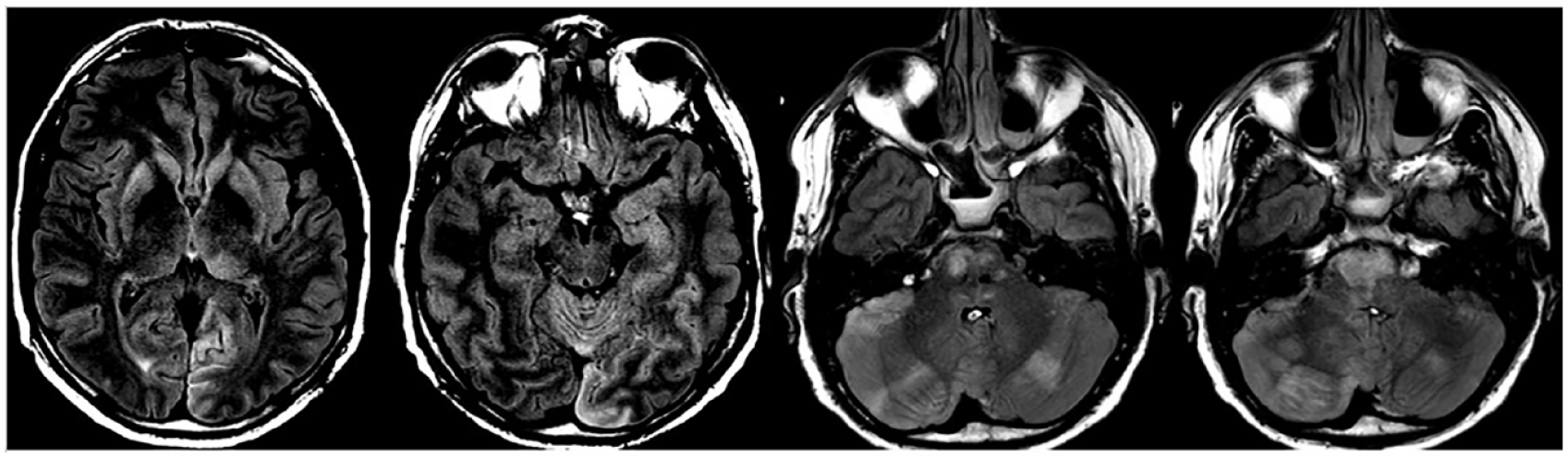
Patient 2 had an extensive bilateral lesion in the pons, reaching the aqueductal area of the mesencephalon (see Figure 3). Movements were incompletely disrupted and communication was possible to some extent through blinking but was inconsistent. EEG 2 months after onset showed generalized slowing with frontal intermittent rhythmic delta activity but prompt reactivity to external stimuli. The marked fluctuation of vigilance led to the diagnosis of an incomplete form of LiPS.

MRI image (FLAIR) of patient 2 showing axial planes of the thalamus, mesencephalon, upper and lower pons (from left to right). Lesions can be seen in the aqueductal area of the mesencephalon, in the pons bilaterally and in the right cerebellum.
Patient 3 had widespread lesions in the thalamus and mesencephalon bilaterally and the pons right-sided (see Figure 4). Initially, the patient presented with a fluctuating ability to communicate through slight hand movements but at the re-evaluation 2.5 years later, was unable to establish any communication. Another 2.5 years later, inconsistent command following and communication was again possible through nodding for a short period but ceased quickly. EEGs in the subacute phase, more than 1 month after onset, revealed an alpha rhythm, theta activity frontotemporal on the left side and reactivity of the basic rhythm. An EEG 5 years after onset showed diffuse theta activity without reactivity. Taken together, these findings suggested the diagnosis of an incomplete form of LiPS.
MRI image (T1) of patient 3 showing axial planes of the thalamus, upper/lower mesencephalon and the pons (from left to right). Lesions can be seen in the thalamus and mesencephalon bilaterally, the pons right-sided and the posterior flow areas.
Patient 4 had a pontine lesion (see Figure 5). An EEG in the subacute phase, more than 1 month after onset, revealed a nearly normal rhythm with slight, diffuse abnormalities, discrete, intermittent, frontal delta activity and reactivity to exogenous stimuli. As communication through eye movements worked well and consistently and some movements were possible with the right arm, this patient was diagnosed with incomplete LiS.

MRI image (T1) of patient 4 showing axial planes of the thalamus, upper and lower mesencephalon and the pons (from left to right). Lesions can be seen in the pons bilaterally.
Patient 5 had a large lesion in the pons bilaterally, possibly including the reticular formation. As only an acute MRI was available, the exact extent of the lesion could not be delineated exactly due to the increased slice thickness and lower resolution, although the extensive lesion in the pons was easily detectable (see Figure 6). The patient displayed inconsistent periods of communication through eye blinking but no other movements. Only an acute EEG (2 days after onset) was available which showed an alpha/theta rhythm and diffuse bilateral theta and delta activity with partial reactivity to external stimuli. Findings suggested LiPS.
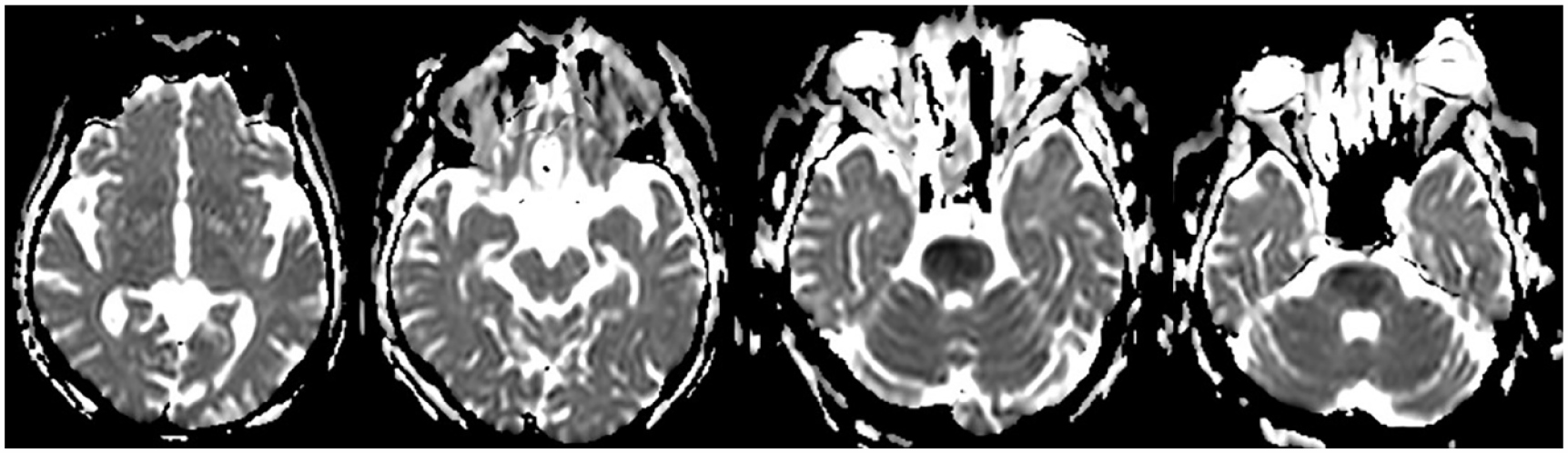
MRI image (ADC measure as only an acute MRI is available) of patient 5 showing axial planes of the thalamus, mesencephalon, upper and lower pons (from left to right). Lesions can be seen in the pons bilaterally.
Patient 6 had bilateral lesions in the pons, involving also the reticular formation (see Figure 7). EEGs in the subacute phase, more than 1 month after onset, showed pathological, diffuse slowing, with predominant theta activity with little reactivity to exogenous stimuli. No movements except eye movements and tracking and no command following or communication was possible. The most likely diagnosis was LiPS.

MRI image (T1) of patient 6 showing axial planes of the thalamus, upper/lower mesencephalon and pons (from left to right, the contrast was enhanced in the pons plane to improve the visibility of the lesion). Lesions can be seen in the pons bilaterally.
Patient 7 presented with a pontine lesion (see Figure 8) disrupting most voluntary movements. A subacute EEG, 2 months after onset was close to normal with slight diffuse abnormalities and diffuse theta activity. Reliable communication through eye movements was possible, and the patient was also able to display head movements. Therefore, the patient was in the state of an incomplete LiS.

MRI image (T1) of patient 7 showing axial planes of the thalamus, upper/lower mesencephalon and pons (from left to right). Lesions can be seen in the pons bilaterally.
Patient 8 showed bilateral lesions in the pons and medulla oblongata and a lesion in the left pulvinar of the thalamus (see Figure 9). EEGs in the subacute phase, more than 1 month after onset, showed a diffuse pathological activity with increased cortical excitability, theta activity, spike-slow-wave paroxysms and reactivity to exogenous stimuli. Eye movements and command following at the bedside were inconsistently possible but no communication could be established. The patient was in LiPS.
MRI image (FLAIR) of patient 8 showing axial planes of the thalamus, mesencephalon, upper and lower pons (from left to right; the contrast of the two planes on the left was enhanced to improve the visibility of the lesions). Lesions can be seen in the pons, basal ganglia and cerebellum bilaterally, the left thalamus and the cuneus.
Patient 9 had lesions in the pons, mesencephalon and thalamus bilaterally (see Figure 10). EEGs in the subacute phase, more than 1 month after onset, revealed slight diffuse abnormalities with a generalized slowing, partial reactivity to exogenous stimuli and a high amount of theta waves. Eye and left upper extremity movements were possible, and so were command following and communication, but very inconsistently. The most likely diagnosis was an incomplete form of LiPS.

MRI image (T1) of patient 9 showing axial planes of the thalamus, upper/lower mesencephalon and pons (from left to right). Lesions can be seen in the pons, mesencephalon and thalamus bilaterally.
The results of the shape feature calculation are presented in Table 2. The average elongation of lesions in LiS patients was 1.161 (range = 1.098–1.223, n = 2), in LiPS patients it was 1.588 (range = 1.226–1.893, n = 7). The average sphericity of lesions in LiS patients was 0.481 (range = 0.439–0.532, n = 2), in LiPS it was 0.411 (range = 0.289–0.731). Finally, the average volume of lesions in LiS patients was 3.25 cm3 (range = 2.75–3.75 cm3, n = 2), in LiPS patients it was 3.47 cm3 (range = 0.38–10.37 cm3, n = 7). Due to the small sample size and different group sizes, further statistical analysis would not produce meaningful results. Figure 11 shows the segmented lesion of a LiS patient, whereas Figure 12 shows that of a LiPS patient.

MRI of a locked-in patient (no. 7) presenting with an approximately round lesion (purple) in the ventral pons.

MRI of a locked-in plus patient (no. 9) presenting with a rostro-caudally elongated lesion (purple) reaching the mesencephalon and thalamus.
Discussion
LiS and LiPS differ in their clinical presentation and the extent of structural lesions. We found that structural lesions in LiS patients are round and confined to the ventral pons, whereas lesions of LiPS patients tend to be more elongated and reach neighbouring areas, such as the mesencephalon and medial thalamic nuclei.
Our findings support the hypothesis about the anatomical foundation of the LiPS. The occlusion of the paramedian arteries which originate shortly distal to the bifurcation of the basilar artery (top of the basilar syndrome) results in lesions of the medial and intralaminar thalamic nuclei and parts of the mesencephalon which play an important role for consciousness and other cognitive functions.22–25 Especially, a rare variant of the paramedian arteries, called the Artery of Percheron, 26 where one single branch supplies the described region bilaterally, is prone to this pattern of ischemia.27–29 Therefore, lesions in LiPS patients can stretch from the pons rostral, involving the mesencephalon and reaching as far as into the thalamus when the rostral part of the basilar artery and the bifurcation is occluded.
Another structure that could be involved in the ascending reticular activating system (ARAS) and the fibres connecting it to other brain structures is the medial and intralaminar thalamic nuclei. As part of the reticular formation, ARAS is situated in the dorsal brainstem and is important for arousal and therefore consciousness.30,31 Especially the rostral part of the reticular formation, above the entry zone of the trigeminal nerve, is assigned to ARAS. 32 One of the main pathways of the ARAS from the rostral pons ascends through the mesencephalic tegmentum, terminating on the intralaminar thalamic nuclei. 33 It has been reported that an exclusive lesion of the pons can disrupt ARAS and cause a disturbance of consciousness. 34 However, this structure is not easy to differentiate from surrounding brainstem structures in MRI, which makes the classification of LiS, and LiPS solely based on imaging findings in patients with lesions restricted to the pons very difficult. This problem could be solved using diffusion tensor tractography, as it was utilized in a single case report. 34 The importance of the exact location of the lesion in the brainstem on the prognosis of the patient was shown neuropathologically. 35 Moreover, brainstem coma, an acute state that only lasts for a few days or weeks, where wakefulness is completely disrupted, has to be clearly differentiated from chronic LiPS. 31 Patient 1 of our study could be mistaken as being in brainstem coma but the length of the state stretching over many years and the fact that the patient opens his eyes excludes this diagnosis. The diagnosis of unresponsive wakefulness syndrome (UWS) is also not suitable, as the lesions are focused on the brainstem. Finally, a complete LiS has to be considered; however, EEG findings suggest disruption of consciousness and eye-opening is possible, which leaves us with the diagnosis of LiPS.
As a consequence of the anatomical considerations, LiPS is characterized rather by the extent of the lesion and not by the multiplicity of distant lesions in addition to the classical lesion in the ventral pons. One may also assume that the bigger the volume of the lesion, the worse the clinical state and level of consciousness of the patient, but this was not the case in our small series. The location and spread of the lesion seem to have more impact on the severity of the disorder than the pure volume alone. A small lesion involving a critical structure can have more drastic effects than a much larger lesion concerning structures whose dysfunction has not as severe and far-reaching consequences. The shape feature calculation showed that the lesions of LiS patients tend to be less elongated and rounder than those of LiPS patients; however, due to the small sample size, no further statistical analysis could be conducted and more patients are needed to verify a significant correlation.
A study on 100 patients with vascular LiS from a tertiary centre, which investigated their clinical and cognitive spectrum, found multiple ischemic lesions in 28% of all patients and these patients had significant impairment in perception and executive function, especially complex command follow, attention span, concentration and intelligible verbalization. However, patients with impaired consciousness were excluded in this study36,37 but they could show that additional lesions in the thalamus and midbrain worsened the cognitive outcome. In another study on LiS survivors, cognitive deficits were described in a small subgroup with additional cortical and thalamic lesions. 37
The differentiation of LiS and LiPS patients is important, as the patients of these two groups need different therapies and care. 38 Recommendations on the rehabilitation management of LiS patients exist, which, besides the treatment of pain, spasticity, incontinence and the management of nutrition, tracheostomy, vision, vegetative and vestibular functions, emphasize the importance of communication. 39 In another study the benefits of early interdisciplinary therapy including physical, speech, occupational therapy and assistive devices are mentioned. 15 Patients who additionally suffer from problems concerning cognition or consciousness need special treatment. As one study concludes, the rehabilitation of LiS patients with cognitive impairments is still a complex problem. 36 However, all LiS subcategorizations are part of a gradient, not completely separable or independent from each other (see Figure 1) and the status of every patient has to be defined individually. Nevertheless, the term LiPS and the other LiS subgroups can help to communicate and categorize the condition of the patient more precisely to ease the way to the right treatment and care.
Furthermore, LiPS must not be confused with disorders of consciousness, such as UWS and the minimally conscious state (MCS), as the pathophysiology, location of the lesion and therefore possible future therapeutic approaches differ. Disorders of consciousness are very heterogeneous due to different aetiologies and lesion locations. While UWS and MCS show diffuse cortical atrophy, ventricular enlargement, sulcal widening and white matter lesions, LIS and LiPS patients have lesions confined to the brainstem (plus/minus thalamus). The prevalence of brainstem lesions differs according to the severity of consciousness impairment 40 and also showed prognostic value. 41 A further subcategorization by differentiating LiPS allows a more precise description and enables a more refined investigation.
Although it was reported that prognosis and mortality improved over the last years in LiS patients, 15 data on LiS patients with additional symptoms are very scarce. One study suggests that patients with additional cognitive impairment have a poorer prognosis compared to classical LiS patients. 36 More studies are needed on these differences.
The CRS-R is not the optimal tool to examine LiS patients, as it was designed for patients suffering from disorders of consciousness and does not include the diagnosis of LiS. Classical and incomplete LiS patients would be misclassified as ‘recovered’ by the CRS-R, whereas complete LiS patients would be misclassified as ‘UWS’ as they are not able to exhibit any of the behaviours examined by the CRS-R. LiPS patients would also be misclassified as ‘MCS’ or ‘UWS’. Therefore, the results of CRS-R in LiS are misleading and should be interpreted only in the context of the whole clinical picture, EEG, structural and functional MRI.
The major concern and shortcoming of this study is the small sample size. As the LiS is a very rare condition, it is difficult to include more patients. Multi-centre studies are needed in this field to confirm our results; however, our findings show the direction towards a more exact diagnosis and subcategorization for LiS patients.
Finally, we also want to mention that only LiS and LiPS patients of vascular aetiology were included in the study and other aetiologies (e.g. trauma, tumour) and locked-in-like states could not be considered.
Conclusion
In conclusion, it can be stated that LiPS is a clinical entity, which enlarges the spectrum of LiS patients and allows for more accurate treatment and care plans to better address the needs of the patients. Although our sample is very small and more research needs to be done, our findings nevertheless can help to improve the understanding of the LiS and disorders of consciousness and will raise awareness of the differences between classical LiS and LiPS. This knowledge can help to adjust the treatment for each patient to his or her level of functioning and enable personalized and more effective therapy and rehabilitation.
Footnotes
Acknowledgements
We would like to commemorate the late Univ.-Prof. Dr. Franz Gerstenbrand and Univ.-Prof. Dr. med. Dipl.-Ing. Stefan Golaszewski for establishing coma and locked-in research in Salzburg, for teaching and inspiring us and for honour their ground-breaking work in this field of research.