
Abstract
Background:
Stent retriever, contact aspiration, and combined treatment are crucial mechanical thrombectomy strategies for patients with acute ischemic stroke (AIS).
Objectives:
The aim of this study was to compare and rank three different mechanical thrombectomy strategies for AIS due to large vessel occlusion by means of a Bayesian network meta-analysis.
Design:
A systematic review and Bayesian network meta-analysis based on PRISMA guidelines.
Data sources and methods:
Relevant randomized controlled trials (RCTs) were identified in Embase, MEDLINE, the Cochrane Library database, and Clinicaltrials.gov from inception to 15 March 2022. We used random effect models to estimate corresponding odds ratios (ORs) and rank probabilities using pairwise and Bayesian network meta-analysis. We applied the grading of recommendations assessment, development, and evaluation (GRADE) methodology to rate the certainty of evidence.
Results:
We identified 10 RCTs enrolling 2098 participants. As for modified Rankin Scale (mRS) 0–2, moderate certainty evidence established all mechanical thrombectomy strategies that were more effective than standard medical treatment [combined: log OR 0.9288, 95% credibility intervals (CrI) 0.1268–1.7246; contact aspiration: log OR 0.9507, 95% CrI 0.3361–1.5688; stent retriever: log OR 1.0919, 95% CrI 0.6127–1.5702]. The same applied to mRS 0–3 (combined: log OR 0.9603, 95% CrI 0.2122–1.7157; contact aspiration: log OR 0.7554, 95% CrI 0.1769–1.3279; stent retriever: log OR 1.0046, 95% CrI 0.6001–1.4789). Combined treatment was superior to stent retriever in substantial reperfusion (log OR 0.8921, 95% CrI 0.2105–1.5907, high certainty). Stent retriever had the highest probability of being optimal for mRS 0–2 and mRS 0–3. Standard medical treatment had the lowest risk of subarachnoid hemorrhage. For all other outcomes, combined treatment was most likely the best treatment.
Conclusion:
Our results indicated that, with the exception of functional outcome, combined treatment might be the outstanding strategy. Apart from subarachnoid hemorrhage, all three mechanical thrombectomy strategies proved better strategies than standard medical treatment.
Registration:
PROSPERO (CRD42022351878).
Keywords
Introduction
Stroke is one of the leading causes of death and disability globally. 1 Meanwhile, it is the most significant contributor to neurological disability-adjusted life-years. 2 Acute ischemic stroke (AIS) accounts for approximately 90% of strokes per year. 3 Until now, recanalization treatment involving intravenous thrombolysis and mechanical thrombectomy has been supported by class I level A recommendation as treatment strategies for AIS. 4
Previous research demonstrates that mechanical thrombectomy can significantly reduce disability and improve clinical outcomes for patients with AIS compared with standard medical treatment.5,6 Even the guidelines have recommended mechanical thrombectomy for large vessel occlusion in the anterior circulation up to 24 h from symptom onset.4,7 Nevertheless, the benefits of successful revascularization using various mechanical thrombectomy strategies as the first-line therapy approach remain uncertain to date. For mechanical thrombectomy, previous guidelines recommended a stent retriever as the first-line approach. 7 Meanwhile, contact aspiration has gained growing acceptance. In the 2019 updated guidelines, contact aspiration and stent retriever are considered as equally crucial. 4 Contact aspiration is also proposed to shorten the time for successful reperfusion and reduce the total cost of hospitalization. 8 However, three randomized controlled trials (RCTs), including ASTER, 9 COMPASS, 10 and a study by Tsang et al., 11 confirmed that stent retriever compared with contact aspiration did not result in a greater functional outcome or higher successful revascularization rate. In accordance with several retrospective studies, contact aspiration combined with stent retriever can boost revascularization rate and may have a synergistic effect.12,13 Nogueira et al. 14 observed combined treatment versus contact aspiration alone did not significantly improve efficacy and safety outcomes. Furthermore, the ASTER2 trial revealed that stent retriever was non-inferior to combined treatment. 15
As a result, clinicians and patients were perplexed by the selection of treatment strategies. Few RCTs directly compared multiple mechanical thrombectomy strategies to our knowledge. Moreover, previous researches were either conventional pairwise meta-analysis 16 or network meta-analysis 17 that excluded combined treatment and were published early. In this study, we systematically evaluated three different mechanical thrombectomy strategies. We conducted the pairwise meta-analysis and first Bayesian network meta-analysis to, directly and indirectly, compare their efficacy and safety as the first-line approach for the treatment of patients with AIS.
Methods
Study design
After we formulated the clinical question and drafted an initial research protocol, a multidisciplinary team (Department of Neurosurgery, Department of Neurology, and Department of Interventional Radiology) of clinicians with previous experience in mechanical thrombectomy discussed together provided suggestions. The systematic review and Bayesian network meta-analysis followed the PRISMA extension statement for network meta-analysis 18 and the updated PRISMA statement. 19 The research protocol has been registered in PROSPERO (CRD42022351878).
Search strategy
The terms related to mechanical thrombectomy, AIS, and RCT were used for searching. The detailed search strategy was shown in the supplementary materials (Table S1). All researches were systematically searched in Embase, MEDLINE, the Cochrane Library database, and Clinicaltrials.gov from inception to 15 March 2022. To avoid omissions, we also checked the references of any other relevant articles, including meta-analyses, reviews, and RCTs.
Selection criteria
Researches that met the following inclusion criteria were included: (a) study type: RCT; (b) language restriction: our study had English language restriction; (c) participant: patient with AIS from large vessel occlusion; (d) intervention: comparing one mechanical thrombectomy strategy (stent retriever, contact aspiration, or contact aspiration combined with stent retriever) with another mechanical thrombectomy strategy or standard medical treatment alone (if eligible, patient would be treated with intravenous alteplase) as the first-line treatment; (e) outcome: any efficacy outcome to assess successful revascularization or the degree of independence and any safety outcome to evaluate death, secondary intracranial hemorrhage, or adverse event. We excluded researches that met the following exclusion criteria: (a) single-arm study; (b) there was no clear indication of which mechanical thrombectomy strategies were used, or multiple mechanical thrombectomy strategies were available. What needed to be emphasized was that previous literature has demonstrated that direct mechanical thrombectomy was non-inferior to bridging therapy.20,21 Hence, we did not distinguish between them in this investigation.
Study selection and data extraction
Two independent authors (J.M. and Z.Y.) separately searched the four electronic databases and the references of relevant articles based on the inclusion and exclusion criteria outlined above. The duplicate researches were excluded by automation tool (EndNote 20). To eliminate studies that did not fulfill the eligibility criteria, we used EndNote 20 to screen titles and abstracts first, then reports that could not be retrieved, and finally the full text of the literatures. For studies that have been published multiple times, we only included the most comprehensive and complete report. After carefully selecting and assessing, the following data were extracted: basic information (study name, countries, number of centers, treatment comparisons, and number of participants), characteristics of participants (age, sex ratio, scores of the National Institutes of Health Stroke Scale at baseline, values of the Alberta Stroke Program Early Computed Tomography Score at baseline, proportion of anterior circulation occlusion, proportion of treatment with intravenous thrombolysis, time from stroke onset to treatment), inclusion criteria, exclusion criteria, treatment procedures, and outcomes. The outcome data were all presented as dichotomous data. In addition, any disagreements that arose in the process of study selection and data extraction were discussed with the third author (J.Z.) for a consensus.
Outcome measures
We focused on two sets of crucial efficacy outcomes: the degree of independence in daily life at 90 days [modified Rankin Scale (mRS)] and the score to grade revascularization at the end of mechanical thrombectomy [expanded Thrombolysis in Cerebral infarction (eTICI)]. In terms of mRS, patients with mRS 0–2 represented functional independence, 22 while mRS 0–3 defined as favorable clinical prognosis. 23 The revascularization was measured by eTICI 2b-3 (substantial reperfusion) and eTICI 3 (complete reperfusion). The safety outcomes of interest were all-cause mortality at 90 days, symptomatic intracranial hemorrhage (sICH) at 24 h, subarachnoid hemorrhage (SAH) within 24 h, and procedure-related adverse events. eTICI and procedure-related adverse events were solely used to assess different mechanical thrombectomy strategies.
Study quality assessment
The Cochrane collaboration uniform criteria 24 were used to assess the risk of bias of RCTs, including selection bias, performance bias, detection bias, attrition bias, reporting bias, and other possible biases in the criteria. Each bias criteria were categorized as ‘low’, ‘unclear’, and ‘high’. The risk of bias plot was analyzed using the Review Manager 5.4.1 software.
We used the grading of recommendations assessment, development, and evaluation (GRADE) methodology to rate the certainty of the evidence for each comparison.25,26 The evidence was categorized as high certainty, medium certainty, low certainty, and very low certainty by GRADE. For direct estimate, we downgraded the evidence from high certainty to varying degrees based on limitations, such as risk of bias, inconsistence, indirectness, imprecision, and publication bias. If no obvious limitations were identified, the evidence would be rated as high certainty. The following indirect estimate was evaluated on the basis of direct estimates. We must first choose the optimum comparison path. If the two treatment strategies shared a common control, the indirect estimate was obtained from the two direct estimates of the two treatment strategies compared with the common control. After considering imprecision and intransitivity, the lower certainty of evidence would be the indirect estimate. In the case of network estimate, we used the higher certainty of evidence as the final network estimate once both direct and indirect estimates were available and consistent. It was the equivalent network estimate when direct or indirect comparison was the only comparison between two treatment options.
Statistical analysis
We used Markov chain Monte Carlo (MCMC) simulation methods within a Bayesian framework to perform the random effects network meta-analysis. The statistical analyses of it were conducted by R (version 4.0.3) and gemtc package.27,28 The network plots revealed the direct comparison between the mechanical thrombectomy strategies and standard medical treatment. Width of connecting line represented the number of RCTs and size of circle related to the number of participants. The trace and density plots were applied to evaluate convergence of MCMC simulation. We performed consistency analyses between the direct and indirect estimates when two groups were compared in direct and indirect ways at the same time. A statistically significant inconsistency was defined as p value less than 0.05. 29 We presented the outcomes of network meta-analysis by log odds ratio (log OR) and 95% credibility intervals (95% CrI). To rank the outcomes of each strategy, we calculated the surface under cumulative ranking curve (SUCRA) and the probability of every ranking. A higher SUCRA value meant a greater likelihood in the top rank. The ranking curves indicated the probability of each treatment strategy in different rankings.
In pairwise meta-analysis, a random effect model was used to assess the dichotomous variables of direct comparisons using Review manager (version 5.4.1). The relative effect was measured by OR and 95% confidence intervals (95% CIs). A statistically significant difference was defined as p value less than 0.05. The anticipated absolute effects were calculated using GRADEpro GDT application. Statistical heterogeneity in pairwise and network meta-analyses was all estimated by the I2 statistic. I2 > 50% represented a substantial heterogeneity.
Results
Study characteristics
A total of 3737 articles from Embase, MEDLINE, the Cochrane Library database, and Clinicaltrials.gov were related to this topic. We removed 640 articles due to duplicates. After screening, seeking for retrieval, and assessing for selection eligibility, we ultimately included 10 RCTs9–11,14,15,30–34 enrolling 2098 participants. Figure 1 shows the PRISMA flow diagram for selection. We acquired the data of the study by Tsang et al. 11 from the World Stroke Congress Abstracts 2020 11 and Clinicaltrials.gov. Table 1 provides patient characteristics of the included studies. Table S2 outlines the eligibility criteria, treatment procedures, and outcomes.

Study search, selection, and inclusion process.
Patient characteristics of the included studies.
ASPECTS, the Alberta Stroke Program Early Computed Tomography Score; CA, contact aspiration; Combined, contact aspiration combined with stent retriever; IVT, intravenous thrombolysis; MED, standard medical treatment; N/A, not applicable; NIHSS, the National Institutes of Health Stroke Scale; No., number; SR, stent retriever.
Mean ± SD.
Median (inter-quartile range, IQR).
The plus–minus values are mean ± SD.
When one mechanical thrombectomy strategy is compared with standard medical care, this represents the time from symptom onset to intravenous alteplase. When two mechanical thrombectomy strategies are compared, this represents the time from symptom onset to puncture.
This represents the time from first observation of symptoms to randomization.
A conference abstract reporting the results of an RCT (NCT03328403).
Pairwise meta-analysis
Any two pairs of mechanical thrombectomy strategies or standard medical treatment were directly compared using the pairwise meta-analyses. Stent retriever had significantly higher probability of functional independence and favorable clinical prognosis compared to standard medical treatment (mRS 0–2: OR 3.29, 95% CI 1.99–5.44, p < 0.01, low certainty; mRS 0–3: OR 2.94, 95% CI 1.83–4.75, p < 0.01, moderate certainty) (Figure S1A). Meanwhile, stent retriever increased mRS 0–2 by 98.5% than standard medical treatment (anticipated absolute effects: 278 more per 1000 participants) (Table S3), mRS 0–3 by 55.8% (anticipated absolute effects: 259 more per 1000 participants) (Table S3). However, no difference was detected between any other two groups (Figure S1A). Stent retriever reduced substantial reperfusion compared with combined treatment (OR 0.42, 95% CI 0.25–0.69, p < 0.01, high certainty) (Figure S1B). The number of participants treated with stent retriever to achieve eTICI 2b-3 decreased by 138 per 1000 than combined treatment (Table S3). Contact aspiration alone was less likely to achieve complete reperfusion than combined treatment (OR 0.53, 95% CI 0.30–0.94, p = 0.03, moderate certainty) (Figure S1B). In absolute terms, the reduction was 157 participants per 1000 (Table S3).
To all-cause mortality, sICH, SAH, and procedure-related adverse events, we found no significant differences between any two groups (Figure S1C and S1D). Table S3 summarizes quality of evidence, anticipated absolute effects, and statistical heterogeneity. All detailed forest plots were presented in Figures S2–S9. As for the heterogeneity, only the I2 value of mRS 0–2 was over 50% when comparing stent retriever with standard medical treatment. Therefore, we performed a sensitivity analysis, which confirmed that the result was stable (Figure S10).
Bayesian network meta-analysis
To compare the efficacy and safety of different mechanical thrombectomy strategies further, we conducted this Bayesian network meta-analysis. Figure 2 shows the participants of eligible RCTs and linkage of treatment strategies. The trace and density plots indicated good model convergence (Figure S11).

Network plots of available direct comparisons. (a) mRS 0–2. (b) mRS 0–3. (c) eTICI 2b-3. (d) eTICI 3. (e) all-cause mortality. (f) sICH. (g) SAH. (h) Procedure-related adverse events.
For efficacy outcomes, combined treatment (log OR 0.9288, 95% CrI 0.1268–1.7246, moderate certainty), contact aspiration (log OR 0.9507, 95% CrI 0.3361–1.5688, moderate certainty), and stent retriever (log OR 1.0919, 95% CrI 0.6127–1.5702, moderate certainty) had significantly higher rate of mRS 0–2 at 90 days than standard medical treatment (Figure 3(a)). All mechanical thrombectomy strategies outperformed standard medical treatment for mRS 0–3 at 90 days (combined treatment: log OR 0.9603, 95% CrI 0.2122–1.7157, moderate certainty; contact aspiration: log OR 0.7554, 95% CrI 0.1769–1.3279, moderate certainty; stent retriever: log OR 1.0046, 95% CrI 0.6001–1.4789, moderate certainty) (Figure 3(b)). However, there was no significant difference between any two pairs of mechanical thrombectomy strategies for mRS 0–2 (Figure 3(a)) and mRS 0–3 (Figure 3(b)) at 90 days. Combined treatment was more likely to achieve substantial reperfusion defined as eTICI 2b-3 compared to stent retriever alone (log OR 0.8921, 95% CrI 0.2105-1.5907, high certainty) (Figure 3(c)). Beyond that, eTICI 2b-3 (Figure 3(c)) and eTICI 3 (Figure 3(d)) were not statistically different between any two pairs of mechanical thrombectomy strategies. Supplementary material shows detailed forest plots (Figure S12).

League tables and corresponding SUCRA values of efficacy outcomes. (a) mRS 0–2. (b) mRS 0–3. (c) eTICI 2b-3. (d) eTICI 3.
As for safety outcomes, the three mechanical thrombectomy strategies did not differ from standard medical treatment nor did the two pairs of mechanical thrombectomy strategies (Figure 4). Similarly, Figure S13 shows detailed forest plots.

League tables and corresponding SUCRA values of safety outcomes. (a) All-cause mortality. (b) sICH. (c) SAH.(d) Procedure-related adverse events.
Figures 3 and 4 reveal the corresponding SUCRA values of various treatment strategies for different efficacy and safety outcomes. Among the two efficacy outcomes and three safety outcomes involving standard medical treatment, standard medical treatment had the lowest probability of SAH within 24 h (SUCRA 0.0902) (Figure 5(g)). In addition, standard medical treatment was likely to be the worst treatment strategy for all other outcomes (mRS 0–2: SUCRA 0.0068; mRS 0–3: SUCRA 0.0069; all-cause mortality: SUCRA 0.8360; sICH: SUCRA 0.7521) (Figure 5(a), (b), (e), and (f)).
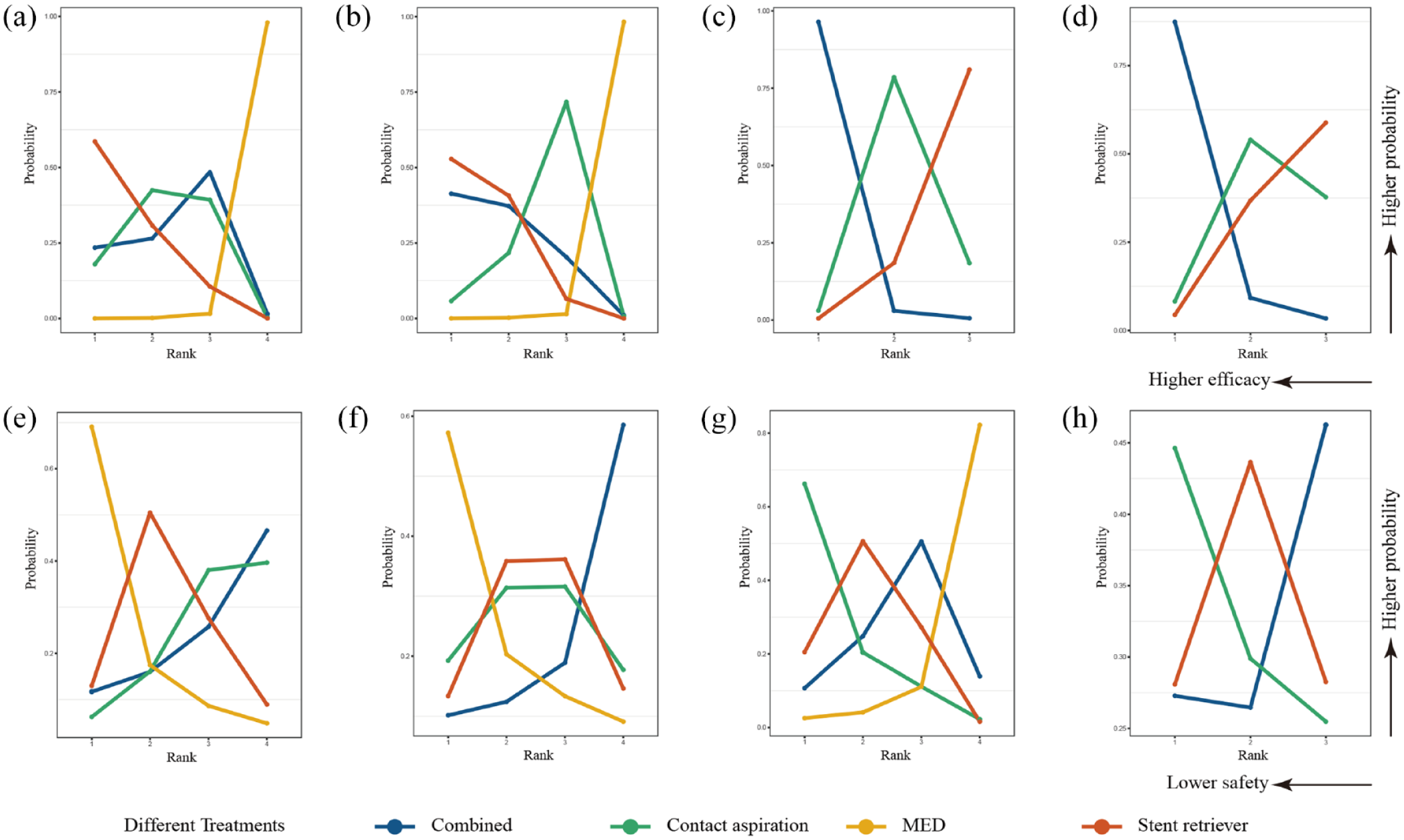
Probability ranks of efficacy and safety outcomes. (a) mRS 0–2. (b) mRS 0–3. (c) eTICI 2b-3. (d) eTICI 3. (e) All-cause mortality. (f) sICH. (g) SAH. (h) Procedure-related adverse events.
For three mechanical thrombectomy strategies, combined treatment had the highest efficacy and safety in eTICI 2b-3 (SUCRA 0.9790) (Figure 5(c)), eTICI 3 (SUCRA 0.9198) (Figure 5(d)), all-cause mortality (SUCRA 0.3092) (Figure 5(e)), sICH (SUCRA 0.2474) (Figure 5(f)), SAH (SUCRA 0.4411) (Figure 5(g)), and procedure-related adverse events (SUCRA 0.4052) (Figure 5(h)). However, stent retriever had the lowest possibility of eTICI 2b-3 (SUCRA 0.0979) (Figure 5(c)) and eTICI 3 (SUCRA 0.2278) (Figure 5(d)), and the highest likelihood of all-cause mortality (SUCRA 0.5585) (Figure 5(e)). Contact aspiration presented the highest probability of SAH (SUCRA 0.8353) (Figure 5(g)) and procedure-related adverse events (SUCRA 0.5958) (Figure 5(h)). In terms of mRS 0–2, stent retriever ranked first (SUCRA 0.8264), followed by contact aspiration (SUCRA 0.5937), and combined treatment was the worst (SUCRA 0.5729) (Figure 5(a)). The ranking analysis showed that the efficacy rating for mRS 0–3 (highest to lowest rank) was stent retriever (SUCRA 0.8211), followed by combined treatment (SUCRA 0.7301) and then contact aspiration (SUCRA 0.4418) (Figure 5(b)).
Supplementary material summarizes the quality of evidence (Table S4). The main reasons for decrease in certainty of the evidence were risk of bias and imprecision. Apart from the absence of head-to-head trial between the combined treatment and standard medical treatment, we performed consistency tests for other comparisons. All the direct and indirect evidence were sufficiently consistent, and the meta-analysis appeared justifiable (Figure S14). We observed the heterogeneity of the network estimates was all acceptable (mRS 0–2: I2 = 30.5%; mRS 0–3: I2 = 21.5%; eTICI 2b-3: I2 = 0%; eTICI 3: I2 = 38.3%; all-cause mortality: I2 = 9.3%; sICH: I2 = 4.4%; SAH: I2 = 23.5%; procedure-related adverse events: I2 = 0%). The detailed I2 values were presented in Figures S15 and S16.
Risk of bias
We examined the risk of bias in each RCTs (Figure S17). Five studies30–34 comparing mechanical thrombectomy strategies with standard medical treatment could not remain completely blind, hence performance bias was high. The investigators at the research sites did the data analysis and collection for EXTEND-IA, 30 increasing the risk of blinding of outcome. However, 60% of the studies14,30–34 were financed by medical device manufacturers or discontinued early, indicating substantial likelihood of other bias. The study by Tsang et al. 11 lacked information to evaluate the risk of bias.
Discussion
For patients with AIS caused by large vessel occlusion, previous RCTs indicated that standard medical treatment was inferior to mechanical thrombectomy.30–34 However, there seemed no notable benefits or drawbacks among the various mechanical thrombectomy strategies in terms of functional outcomes and rate of reperfusion,9–11,14,15 and head-to-head RCTs were rare. As a result, we conducted this pairwise and network meta-analysis to assess their efficacy and safety. This study was based on 10 RCTs including 2098 participants in total. In the pairwise meta-analysis comparing mechanical thrombectomy to standard medical treatment, stent retriever was linked to improvements in mRS 0–2 and mRS 0–3 at 90 days, but no significant differences were detected in all-cause mortality, sICH, and SAH. For every 1000 patients with AIS who underwent stent retriever, 278 more would experience substantial clinical benefits in functional independence. Due to the lack of study directly comparing combined treatment with standard medical treatment and the limited sample size of THERAPY comparing contact aspiration and standard medical treatment did not achieve its primary outcome, we further performed a Bayesian network meta-analysis. Functional independence and favorable clinical prognosis were also more easily achieved in contact aspiration and combined treatment. All of the above results had at least moderate certainty by GRADE methodology. According to the SUCRA values and probability ranks, standard medical treatment had the worst results in mRS 0–2, mRS 0–3, all-cause mortality, and sICH. However, we observed that it had the lowest SAH probability than all mechanical thrombectomy strategies. Previous study had reported that the high probability of SAH following mechanical thrombectomy, ranging from 5% to 16%. 35 Microwire perforation, tearing of the vessel, changes in vascular permeability, or reperfusion damage were all conceivable mechanisms. 36 Besides, numerous device passes and a distal location of artery occlusion were associated with a higher rate of SAH. 36
As for three mechanical thrombectomy strategies, moderate to high certainty evidence suggested that combined treatment was more effective than stent retriever alone for substantial reperfusion and contact aspiration for complete reperfusion in pairwise meta-analysis. Likewise, in comparison to contact aspiration, it showed a considerable trend toward significance for eTICI 2b-3. None of the other efficacy and safety outcomes were significantly different between any two pairs. By network comparison, only combined treatment outperformed stent retriever for eTICI 2b-3 with high certainty of evidence. According to Goyal et al., 5 stent retriever was the primary device used in several previous RCTs and should be considered as the benchmark for following alternative mechanical thrombectomy strategies. Stent retriever was most likely to be the best treatment for functional outcome. Ranking analysis indicated combined treatment had the highest probability of being the best mechanical thrombectomy strategies for successful revascularization rate and all safety outcomes.
The ASTER2 also demonstrated that combined treatment was more effective to obtain successful recanalization after the initial intervention. 15 This could be explained by the fact that combined treatment was able to reduce the fragmentation of primary embolus and fresh thrombi. 12 The use of stent retriever increased the mechanical capture of thrombus compared with contact aspiration alone. 12 In addition, the stent retriever or contact aspiration group was also thought to require more further rescue therapy,15,37 which confirmed the relative superiority of combined treatment. Combined treatment had the advantages of lower total number of passes and shorter puncture-to-reperfusion time. 37 However, the increase in total device cost due to combined treatment could not be ignored. In particular, with the rapid development of mechanical thrombectomy equipment and techniques, the gap between different mechanical thrombectomy strategies was expected to reduce. It is worth debating if the additional treatment cost rise was necessary at the time.
Okuda et al. 37 confirmed that internal carotid artery and middle cerebral artery M2 segment occlusions were more suitable for combined treatment than M1 segment occlusion, which might be explained by the size of thrombus and artery diameter. The site of large vessel occlusion was predictor for successful revascularization. 38 Therefore, stent retriever, contact aspiration, and combined treatment were all effective and essential treatment strategies. Clinicians needed to adopt a more appropriate strategy based on the individual characteristic of each patient.
This meta-analysis has several limitations. First, the time from stroke onset to treatment and the proportion of treatment with intravenous thrombolysis varied slightly in different RCTs, which might impact on the accuracy of results. Especially, the DAWN trial enrolled the patients who was last known to be well 6–24 h. Second, almost all of the patients in this study had anterior circulation occlusions. The only RCT investigating vertebrobasilar artery occlusion was excluded because it did not distinguish between specific mechanical thrombectomy strategies. 39 Despite the low prevalence of posterior circulation occlusion, the majority of patients experienced severe disability or even death as a result of it. 39 To determine the best treatment strategy for posterior circulation occlusion, more researches were needed. Third, mechanical thrombectomy equipment and techniques were rapidly developing, so the major devices used in included RCTs were not identical. For example, the aspiration catheters used in the COMPASS trial had larger luminal diameters than those used in the ASTER study. Fourth, total device cost, long-term follow-up, time from puncture to final revascularization, reperfusion outcomes after the initial intervention alone, and utilization of rescue treatment were all crucial for mechanical thrombectomy. However, because of the paucity of equivalent trials, these factors were not measured in this study. Finally, some trials were funded by medical device manufacturers and terminated early for various reasons. Although the authors claimed that manufacturers were not involved in the design and conduct of the study, this might lead to a potential reduction in the credibility of evidence.
Conclusion
In conclusion, our meta-analysis supported that stent retriever, contact aspiration, and contact aspiration combined with stent retriever were all superior to standard medical treatment for mRS 0–2, mRS 0–3, all-cause mortality, and sICH. However, standard medical treatment was capable of reducing the occurrence of SAH. Stent retriever resulted in the most mRS 0–2 and mRS 0–3. Contact aspiration combined with stent retriever proved the best mechanical thrombectomy strategy in substantial reperfusion, complete reperfusion, all-cause mortality, sICH, SAH, and procedure-related adverse events. Mechanical thrombectomy evolved over time and the disparity between different strategies would probably diminish.
Supplemental Material
sj-docx-1-tan-10.1177_17562864231181180 – Supplemental material for Comparative efficacy and safety of various mechanical thrombectomy strategies for patients with acute ischemic stroke: a Bayesian network meta-analysis
Supplemental material, sj-docx-1-tan-10.1177_17562864231181180 for Comparative efficacy and safety of various mechanical thrombectomy strategies for patients with acute ischemic stroke: a Bayesian network meta-analysis by Jiahao Meng, Zeya Yan, Jie Zhang, Wei Wang, Xinyu Tao, Feng Gu, Xingyu Yang, Tao Xue, Wanchun You, Zhouqing Chen, Zhong Wang and Gang Chen in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.