
Abstract
A 34-year-old female patient presented during the 10th week of her second gravidity with headache, nausea and vomiting 2 weeks before admission. Her medical history was remarkable for a heterozygous factor V Leiden mutation, elevated lipoprotein A, and a cerebral venous thrombosis (CVT) after oral contraceptive intake 15 years before. Magnetic resonance imaging (MRI) suggested acute and massive intracranial sinus thrombosis. Despite full-dose anticoagulation, the patient deteriorated clinically and eventually became comatose. Now, MRI/magnetic resonance angiography revealed vasogenic edema of both thalami, of the left frontal lobe, and of the head of the caudate nucleus, with venous stasis and frontal petechial hemorrhage. She was referred for endovascular treatment. Diagnostic angiography confirmed a complete superficial and deep venous sinus occlusion. Endovascular access to the straight and superior sagittal sinus was possible, but neither rheolysis nor balloon angioplasty resulted in recanalization of the venous sinuses. Monitored heparinization was continued and antiaggregation was initiated. The patient remained comatose for another 5 days and MRI showed progress of the cytotoxic edema. On day 6, infusion of eptifibatide at body-weight-adapted dosage was started. The following day, the patient improved and slowly regained consciousness. MRI confirmed regression of the edema. The eptifibatide infusion was continued for a total of 14 days. Thereafter two doses of 180 mg ticagrelor per os (PO) daily were started. The patient remained on acetylsalicylic acid (ASA), ticagrelor, and enoxaparin on an unchanged dosage regimen. She was discharged home 26 days after the endovascular treatment without serious neurological deficit, with the pregnancy intact. At the 30th week of pregnancy the dosage of ASA was reduced to 300 mg once PO daily. Cesarian delivery was carried out at the 38th week of pregnancy. The newborn was completely healthy. Ultima ratio therapeutic options for severe intracranial venous sinus thrombosis refractory to anticoagulation are discussed, with an emphasis on platelet-function inhibition.
Keywords
Introduction
Acute cerebral venous thrombosis (CVT) is an infrequently encountered disease. Local infection, trauma of the skull, genetically determined thrombophilia and acquired prothrombotic conditions (e.g., paraneoplastic hypercoagulability) are known predisposing factors. Possible clinical manifestations include increased intracranial pressure (headache, papilledema, visual disturbances), focal neurological deficits with or without seizure and encephalopathy. 1 The underlying reason for these symptoms is the impaired venous drainage of the brain which increases venous pressure, leading to focal parenchymal edema or intracranial hemorrhage.2,3 The severity of the clinical symptoms is related to the extent and location of the venous occlusion. Massive CVT is a cerebrovascular emergency and an established cause of rapid clinical deterioration due to elevated intracranial pressure, intracerebral hemorrhage, and brain herniation, eventually resulting in death. The mainstay of CVT treatment is therapeutic anticoagulation, although even on this regime, 9–13% of patients will have a poor outcome. Thrombolytic therapy is usually performed if clinical deterioration occurs despite being on an anticoagulation regime, or if a patient has elevated intracranial pressure that has evolved despite taking another management approach. 4
Chronic intracranial CVT is a poorly understood condition and usually the sequel of the acute phase of this disease. Many, but not all, patients have previously suffered a clinically apparent acute CVT. 5 Some of these patients come to the attention of interventional neuroradiologists since they have developed dural arteriovenous fistulae in the aftermath of an acute CVT.
CVT and other venous thromboembolic events may reoccur, which is the reason for secondary preventive medication. Recurrent acute CVT in patients with chronic CVT is infrequent (2.2–3.2%)6,7 and can become a therapeutic challenge, as described in the presented case.
Case report
A 34-year-old female patient presented to the neurology department of the referring hospital during the 10th week of her second pregnancy. She had been suffering from headaches, nausea and vomiting for the 2 weeks leading up to admission. A graphical depiction of the development of her symptoms is illustrated in Figure 1. She was first diagnosed with either hyperemesis gravidarum or a gastrointestinal viral infection because of similar symptoms in her child. Her medical history was remarkable for a heterozygous factor V Leiden mutation, hyperactivity of factor VIII and elevated lipoprotein A. Around 15 years earlier, she had been diagnosed with an acute CVT, manifesting in a headache with no other deficits, and with thrombosis of her right transverse and sigmoid sinuses and left proximal transverse sinus[Figure 2(a)], after taking oral contraceptives. This CVT was managed with an anticoagulation regime which involved taking the vitamin K antagonist phenprocoumon for 1 year. The transverse and sigmoid sinuses on the right-hand side had not totally recanalized in the magnetic resonance imaging and angiography (MRI/MRA) performed 1 year after the initial CVT; a complete recanalization occurred after 3 years. During her current pregnancy, she was receiving thrombosis prophylaxis with 80 mg enoxaparin subcutaneously (SC) daily adapted to a body weight (BW) of 95 kg. The first MRI/MRA showed no parenchymal lesion with no flow signal in the straight sinus, as well as bilateral discontinuity in flow signal intensity in the superior sagittal sinus and both transverse and sigmoid sinuses [Figure 2(b)]. Two days before referral to our hospital (day 7) she developed behavioral changes and motor aphasia, progressing to a global aphasia, and mild tetraparesis accentuated on the right-hand side. This was despite being on full-dose anticoagulation therapy of low-molecular-weight heparin (LMWH) since the day before referral (two doses of 80 mg enoxaparin SC daily, for a BW of 95 kg). MRI/MRA at referral showed vasogenic edema of both thalami [Figure 2(c)], of the left frontal lobe, and of the head of the caudate nucleus, with venous stasis and frontal petechial hemorrhage. All intracranial venous sinuses and deep internal cerebral veins were occluded [Figure 2(b, c)]. She was referred for endovascular treatment, which we attempted on the day of admission (day 9). Diagnostic angiography (DSA) confirmed a complete superficial and deep venous occlusion with the brain draining via alternate pathways. Endovascular access to the straight and superior sagittal sinuses was possible by inserting an 8F guiding catheter into the right-hand jugular vein and then the left-hand side. A 4F diagnostic catheter was inserted via the right-hand femoral artery for diagnostic DSA runs and road map images. Neither rheolysis [i.e. alternate flushing and aspiration via a Sofia Plus aspiration catheter (MicroVention, Aliso Viejo, CA, USA)] nor balloon angioplasty of the superior sagittal, transverse, and sigmoid sinuses of both sides [conventional balloon, pITA 4 ×40 mm (phenox, Bochum, Germany)] resulted in recanalization. Injecting contrast medium into the said sinuses showed contrast gaps in the lumen which looked like fibrous structures and stenosis, together with a small amount of thrombus [Figure 2(d)]. The endovascular procedure was, apart from the failure to recanalize the sinuses, tolerated by the patient without further complications. The patient was kept on two doses of 80 mg enoxaparin SC daily. After 2 days, 500 mg acetylsalicylic acid (ASA) intravenously (IV) daily was added, as the patient was comatose. The ASA dosage was monitored using Multiplate (Roche Diagnostics, Munich, Germany), VerifyNow (Accriva, San Diego, CA, USA), and the PFA-200 system (Siemens, Erlangen, Germany). The enoxaparin dosage was adjusted as required by the values from antifactor Xa (anti-Xa) activity measurement (prophylactic anticoagulation level: >0.1–0.4 U/ml; therapeutic anticoagulation: 0.4–1 U/ml). On day 11, it was increased to two doses of 100 mg enoxaparin SC daily, adjusted to the BW and after a decrease of anti-Xa on days 13 and 15, subsequently raised to two doses of 120 mg enoxaparin SC daily (see Figure 1). Renal function was normal and therefore LMWH could be used and increased after the dosage had been adjusted. A nonconvulsive epileptic state was ruled out with an electroencephalogram (EEG). The patient remained comatose for another 5 days and on day 14, MRI showed growing cytotoxic edema of the left frontoparietal parenchyma. Given this desperate situation, on day 14, after a thorough discussion with the family, we decided to apply a BW-adapted infusion of eptifibatide (11.2 mg/h IV) as part of an individual treatment attempt. On day 15, the patient showed a clinical improvement. On day 20, the patient slowly regained consciousness, while imaging started showing some improvement to wit, a regression of the edema in the caudate nucleus, and better flow in the straight sinus, vein of Galen, and internal cerebral veins [Figure 2(e)]. Decompressive craniectomy was not considered beneficial at any point. The eptifibatide infusion was continued for a total of 14 days. Then, continuing the individual treatment attempt, a regime of ticagrelor, two doses of 180 mg PO daily were started, with its dosage adjusted per the results of the aforementioned tests for platelet-function monitoring. The patient remained on ASA, ticagrelor, and enoxaparin on unchanged dosages. She was discharged home 26 days after the endovascular treatment (day 35 since she had first been admitted) with only mild neurological deficits (mild facial asymmetry and mild problems with fine motor movements in the right hand, modified Rankin Scale 2), and with the pregnancy intact. On MRI/MRA, the intracranial venous sinuses appeared unchanged with permeability of the straight sinus, vein of Galen and internal cerebral veins [Figure 2(f)]. In the 30th week of pregnancy, the ASA dosage was reduced to 300 mg PO daily. Cesarian delivery was planned for the 38th week of gestation. Ticagrelor was discontinued a week beforehand and ASA and enoxaparin were discontinued 48 h before delivery. Delivery occurred without complications and the newborn baby was completely healthy. IV unfractionated heparin (UFH) and 100 mg ASA PO daily were initiated 6 h after delivery. The patient decided not to breastfeed. After 48 h, UFH was discontinued, two doses of 90 mg enoxaparin SC daily were initiated and ASA was increased to two doses of 100 mg PO daily. After 10 days, the enoxaparin was replaced by two doses of 150 mg dabigatran PO daily. No adverse events occurred in the postpartum period. The most recent MRI follow up performed after delivery (6 months after the initial treatment) confirmed complete recanalization of the sinuses and the deep venous system [Figure 2(g, h)]
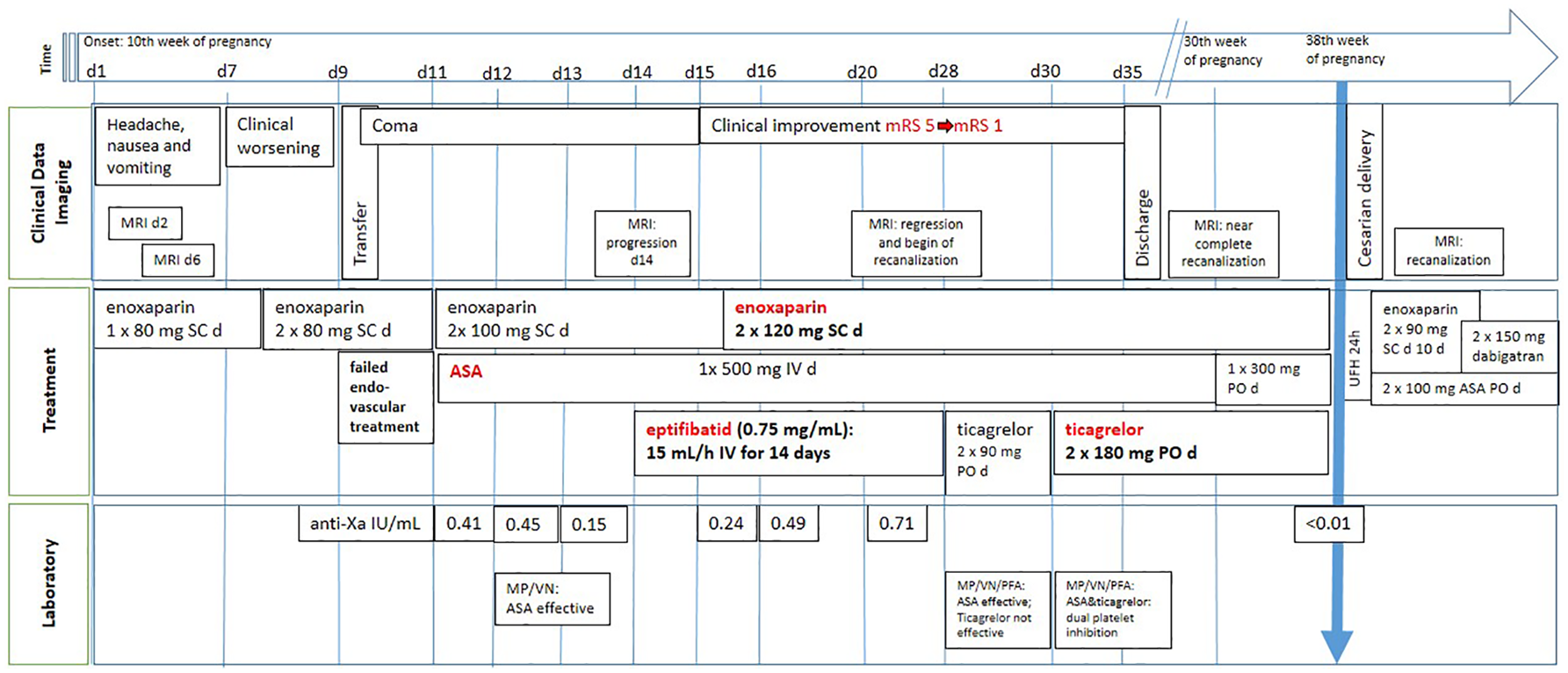
Graphical illustration of the clinical case over time: clinical data, treatment and laboratory findings.

MR venography of the patient from 2004, [(a) oblique MIP image of a TOF] showing an occlusion of the right transverse to sigmoid sinus (asterisk). Filling defect consistent with clot is also noted in the left transverse sinus (arrow). This episode was treated by anticoagulation with total recanalization and without clinical sequelae. MR venography of the patient in 2019, after presenting with behavioral changes and motor aphasia, revealing absence of flow in the superior sagittal and both transverse to sigmoid sinuses. The internal cerebral veins and straight sinus are also not visualized [b) lateral MIP image of a TOF MR venography]. Focal edema within both thalami (arrows) was observed due to thrombosis of deep venous system [(c) axial T2-weighted imaging]. Direct contrast medium injection into the superior sagittal sinus showed contrast gaps in the sinus lumen, which looked like chronic changes with only a small amount of fresh thrombus [(d) angiographic lateral view]. After starting with a BW-adapted infusion of eptifibatide (11.2 mg/h IV) the patient showed some clinical improvement. Subsequent MRI showed partial recanalization of the sinuses and deep venous system [(e) lateral MIP images of TOF MR venography]. MRI performed 3 months after treatment showed near-complete recanalization with persistent filling defects in superior sagittal and both transverse sinuses [(f) lateral MIP image of TOF MR venography]. The most recent MRI follow up performed after delivery (6 months after the initial treatment) confirmed complete recanalization of the sinuses and the deep venous system [(g) lateral MIP image of a TOF MR venography] with complete resolution of the previous edema within both thalami [(h) axial T2-weighted imaging].
Discussion
The patient reported herein had, to the best of our understanding, previously suffered a superficial CVT with, initially, only partial recanalization; however, with development of adequate venous collaterals and good recovery, and finally a complete recanalization. During the endovascular procedure, angiography showed the aforementioned contrast gaps in the lumen of the sinuses, fibrous structures, and stenosis, with only a very small amount of thrombus. This could suggest that the partial recanalization of the previous CVT had left changes in the venous endothelium and partially organized clot in the lumen of the affected sinuses. Drainage of intracranial venous sinuses can be taken over by superficial and deep draining veins. In our patient, the combination of a heterozygous factor V Leiden mutation and hormonal stimuli might have triggered the thrombus formation, since the first event occurred while starting oral contraceptives, and the second CVT took place during the initial phase of her second pregnancy. Resistance to activated protein C is mainly caused by the presence of a factor V Leiden gene mutation, which has an odds ratio of CVT of 3.38 (95% confidence interval 2.27–5.05), similar to its association with venous thromboembolism in general. 8 Recurrence after a CVT is infrequent (2.2–3.2%),6,7 although the annual risk of any type of recurrent thrombosis is 6.5%. 4 Four studies have investigated the risk of recurrent venous thrombosis in patients with thrombophilia, all with a considerable sample size varying from 145 to 706 patients, but with inconsistent results. In two studies, the association between thrombophilia and recurrent venous thrombosis showed no effect,5,9 while an increased risk effect was described in another two studies.10,11 Patients with severe thrombophilia (deficiency of antithrombin, protein C or protein S, homozygous prothrombin G20210A, homozygous factor V Leiden, combined defects, and antiphospholipid syndrome) have an increased risk of recurrence (19% recurrence at 2 years, 40% at 5 years). The most common hereditary thrombophilia, such as heterozygous factor V Leiden and prothrombin G20210A, or elevated factor VIII, have a much lower risk of recurrence (7% at 2 years, 11% at 5 years). 4
Thrombosis of the deep venous cerebral system veins, internal cerebral veins, vein of Galen, or the straight sinus occurs in approximately 16% of patients with CVT 2 and is considered a risk factor for poor clinical outcome. 12 Thalamic edema is the imaging hallmark of this condition, and it may extend into the caudate regions and deep white matter. Mortality rates among patients with this condition are reported to be between 22% and 37%, while 54% of patients may have no neurologic sequelae. 2 Our patient had a chronic superficial venous thrombosis, making the prognosis even worse. Keeping the pregnancy intact was also a concern. It was, however, agreed early on within the medical team and with the patient’s family that attempts to save the patient’s life would have to overrule all possible aspects concerning the pregnancy. Abortion was considered a viable option should there be gynecological complications from the complex neurovascular management.
Prophylactic LMWH treatment during pregnancy after a CVT associated with a hormonal risk factor is recommended 13 at a dose of 40 mg enoxaparin SC daily or 60 mg SC daily for obese patients. 14 Our patient, with a body mass index of 32.8 kg/m2 (obesity grade I), received 80 mg of enoxaparin SC daily.
The mainstay of treatment for an acute CVT is anticoagulation with heparin at a therapeutic dosage (quality of evidence: moderate; strength of recommendation: strong). 15 With regards choosing which anticoagulant to use, guidelines suggest treating patients with acute CVT with LMWH instead of UFH. The evidence behind this recommendation is weak, because of the high risk of bias in the relevant studies. 15 One randomized trial directly compared LMWH to UFH with some methodological limitations, and showed significantly lower hospital mortality in CVT treated with LMWH compared with patients under UFH. 16 A nonrandomized study suggested better efficacy and safety of LMWH compared with UFH. 17 After a systematic review and meta-analysis of the published studies, a trend towards improved mortality and functional outcome in patients treated with LMWH was displayed, although this trend could not be considered statistically significant due to the small number of studies available for inclusion. 18
In pregnancy, anticoagulation with LMWH is preferred to UFH due to lower side effects, the ease of dosing, and the fact that this is not associated with either teratogenicity or increased risk of fetal bleeding.4,13,14 The neurological deterioration in our patient in spite of therapeutic LMWH pressed us to consider endovascular treatment. Due to the presence of a petechial hemorrhage, mechanical endovascular treatment was planned. In contrast to typical acute CVT, the venous sinuses of this patient were not being occluded by coagulated blood, which can often be efficiently removed by endovascular rheolysis. Instead, local contrast medium injection into the venous sinuses showed contrast gaps of the lumen of said venous sinuses, possibly representing a network of fibrous tissue, with very small amount of fresh thrombus intermingled. This was true for all superficial venous sinuses and prevented any efficacious endovascular recanalization. Angioplasty was carried out but was also not helpful. The fact that the current extent of the chronic sinus thrombosis with suspected fibrous tissue by far exceeded the known previous thrombosis (e.g. superior sagittal sinus) can be explained by further recurrent asymptomatic CVT that could have happened in the meantime, as the last control MRI had been done 12 years before the current illness. The patient only became symptomatic once the deep venous system was also affected and the balance of collateral drainage pathways was dramatically compromised.
The European Stroke Organization guidelines recommend decompressive craniectomy for patients with acute CVT and parenchymal lesions with impending herniation to prevent death. 15 The lesions in our patient (both thalami, left frontal lobe, and head of the caudate nucleus) were associated with coma. Neither a local space-occupying effect of the congestive infarcts nor a midline shift was present, and decompressive craniectomy was not expected to be beneficial.
The continuous medication regime including ASA and therapeutic anticoagulation with enoxaparin did not improve the condition of the patient during 5 days of continuous coma. Local fibrinolysis was contemplated, but eventually rejected, since there was little thrombus that could be liquefied. Stenting all accessible sinuses was another option we considered as a last resort.
Antiaggregation using ASA as an adenosine diphosphate (ADP) receptor inhibitor was initiated in order to prepare the patient for further endovascular procedures. The therapeutic anticoagulation with enoxaparin was initially only just BW-adapted (two doses of 80 mg enoxaparin SC daily for 95 kg), and could have been insufficient; 3 days later, on day 11, it was increased to two doses of 100 mg SC daily, with therapeutic anti-Xa levels, but still no clinical improvement was observed. After 6 days, halfway through day 15, it was increased to two doses of 120 mg SC daily per the results of anti-Xa activity measurements that had reduced on days 13 and 15. Clinical improvement occurred on day 15, after 24 h of eptifibatide perfusion and under a twice-daily dose of 100 mg enoxaparin SC. Monitoring anti-Xa activity in pregnancy is controversial and is not generally recommended, but consideration should be given to initial monitoring of anti-Xa activity during just the first month of treatment, to aim at a level of 0.6–1.0 U/ml 4 h after injection.14,19 The dosage of ASA (500 mg via IV daily) and afterwards, ticagrelor (180 mg ticagrelor PO twice daily) was adjusted following multiple Multiplate, VerifyNow, and PFA-200 tests.
A suboptimal response to antiplatelet therapy may be associated with cardiovascular, cerebrovascular, and peripheral arterial events, and platelet-function testing is performed routinely for monitoring this therapy. 20 A ‘resistance,’ or the more accepted term, ‘high on-treatment platelet reactivity (HTPR),’ has been described as referring to a lack of therapeutic levels of inhibition from a drug as measured by well-validated tests. 20 HTPR is a marker for thrombotic events and has been seen with clopidogrel in up to 40% 21 and up to 66% of neurointerventional procedures. 33 Available evidence does not support the routine use of laboratory tests to guide the dose of ASA, clopidogrel, or other inhibitors of the P2Y12 receptor in clinical practice, probably because of the low-risk profile of the patients included in the studies, but it has been shown to be useful in some clinical settings. 21
ASA is reliable and predictable, and HTPR is rare but does exist. Problems in drug absorption play a role. 22 The three tests that we use require whole blood. VerifyNow (Accriva, San Diego, CA, USA) is a point-of-care system that utilizes anticoagulated blood for optical (turbidimetric) detection of platelet aggregation, using cartridges with fibrinogen-coated beads and different-platelet agonists: arachidonic acid in the aspirin assay, and ADP in the P2Y12 assay. It is the simplest, most rapid, and most reliable way of assessing response to P2Y12 inhibitors. The Multiplate, also referred to as multiple-electrode plate aggregometry, measures increases in electrical resistance or impedance, caused when activated platelets attach to electrodes. It requires skills and training, as pipetting is required. These two tests are performed routinely in our department before all endovascular procedures requiring antiaggregation. The Platelet Function Analyzer, (PFA)-200, (PFA-200; Siemens, Erlangen, Germany) measures the time to closure of an aperture by platelet aggregates; it is dependent on the von Willebrand factor and hematocrit, requires pipetting, and does not correlate well with clopidogrel therapy.20,22,23 We use the PFA-200 system when there is discrepancy in the tests that we have already performed.
During pregnancy, the required dosage for ADP-, P2Y12-, and Gp IIb/IIIa antagonists can be significantly increased, but there are no adequate studies available in this clinical setting. 19 Blind administration of standard dosages, as in the scenario of an acute illness, would most likely be unsuitable for achieving a therapeutic effect. With the BW-adapted standard dosage of eptifibatide (0.75 mg/kg BW), the TRAP module in the Multiplate test confirmed significant platelet-function inhibition.
Gp IIb/IIIa antagonist eptifibatide was added on day 14 when the patient remained comatose after all of our measures following current medical guidelines in addition to ASA had failed to improve the patient’s condition. 4 Our initial plan was to start the perfusion of eptifibatide for 3 days and to stent the closed superficial sinus as an ultima ratio. As the patient began to improve on day 15, this turned out not to be necessary. Eptifibatide, tirofiban, and abciximab have not been studied in pregnant patients, and randomized trials normally excluded these patients.24,25 Therefore, their use is not recommended during pregnancy. 26 We had chosen eptifibatide because of its reversible effect with recovery of platelet activity within 2–4 h. 27 In several trials for acute coronary syndrome, enoxaparin and glycoprotein IIb/IIIa inhibitors could be safely used together. 28 Although the acute coronary syndrome (ACS) guidelines recommend a maximal eptifibatide therapy length of 96 h, our patient was treated for 15 days. Some cases have been reported involving the prolonged use of eptifibatide as a bridging therapy before surgery, alone 29 or in addition to anticoagulation. 30 In our case, we maintained eptifibatide for almost 15 days because of clinical improvement after 24 h of infusion and because other antiplatelets have problems of absorption via nasogastric tube. Our patient was in a coma and we did not want to take any further risks.
ASA crosses the placenta barrier and has no teratogenic effects; there is insufficient clinical experience regarding the use of doses between 100 mg and 500 mg ASA per day. 26
After clinical improvement, ticagrelor, one of the newer antiplatelet drugs, was introduced, replacing eptifibatide. There are inadequate human data and it is not recommended in pregnancy. Studies in rats have shown minor developmental anomalies at maternal toxic dosages, and in rabbits, a slight delay in hepatic maturity and skeletal development was seen at maternal nontoxic doses. In rats and rabbits, slightly reduced maternal BW, reduced neonatal viability and birthweight with delayed growth has been shown. 26 First use of ticagrelor in human pregnancy for myocardial infarction has already been reported. 31 Clopidogrel has been used in pregnancy but its use is also controversial, with no demonstrated teratogenicity, and also without studies having been done in humans.26,32 A multidisciplinary board decided in our case to use ticagrelor to achieve consistent platelet inhibition with maximal effect and eventually to avoid drug resistance.20,33 as this had been proved in ACS, where the only proven method to reduce thrombotic events was to initiate more potent P2Y12 inhibitor therapy with prasugrel or ticagrelor. 21
During the postpartum period and for breastfeeding women, LMWH, UFH, and warfarin are all acceptable. Direct nonvitamin K oral anticoagulants (direct thrombin and factor Xa inhibitors) should be avoided in breastfeeding women, as they may be secreted into breastmilk. 15 Currently, direct nonvitamin K oral anticoagulants are not recommended as acute anticoagulant treatment because of very low quality of evidence (observational studies with high risk of bias) in the latest guidelines published. 15 Dabigatran, a direct thrombin antagonist replacing enoxaparin, was initiated 10 days after delivery as long-term off-label therapy, as the patient had decided not to breastfeed. Recently published data from a randomized study suggested that both dabigatran and warfarin may be safe and effective for preventing recurrent venous thromboembolisms in patients with CVT, both being initiated after 5–15 days of UFH or LMWH. 34
The key to understanding this case is to discover why the eptifibatide infusion was associated with such a dramatic improvement in the patient. To the best of our knowledge, there have not yet been any other reports on cases in which anticoagulation treatment of an acute CVT was complemented by an antiaggregation regime involving a Gp IIb/IIIa receptor antagonist. First of all, the success of this approach could have been a pure coincidence. Given the clinical improvement of the patient, however, we did not dare stop the eptifibatide infusion in order to test this hypothesis. It appears more likely to us that alongside Gp IIb/IIIa receptor inhibition, a certain thrombolytic effect was being exerted by the eptifibatide, especially in the combination with the other medications described above. We would like to draw attention to a possible role being played by platelets in venous thrombus formation in CVT, and to antithrombotic treatment being a co-adjuvant therapy option for poor-outcome patients resistant to an established treatment regimen. Gp IIb/IIIa receptor inhibitors have been approved for use in ACS, and as an adjunct to percutaneous coronary interventions. They are also used in intraprocedural thrombosis and ischemic events during neuroendovascular procedures. 35 Although the limited evidence that exists for the use of eptifibatide in acute ischemic strokes cannot be transferred wholesale to a venous disease, prospective, randomized, open-label phase II trials of tirofiban and eptifibatide have suggested it is safe to use in treating patients with an acute ischemic stroke. 36
Arterial and venous thrombosis are traditionally considered two very different conditions. Arterial thrombosis is formed under high-shear stress, typically after the rupture of atherosclerotic plaque or other damage to the blood vessel wall. 37 It requires antiaggregation therapy, as this is a platelet-driven thrombus, with platelets being the cellular components closest to vessel wall. 38 Previous analysis of the histopathologic composition of cerebral arterial thrombi in acute stroke patients found that all lytic (1–5 days) and organized (>5 days) thrombi also contained a component that was fresh (less than 1-day old) and all analyzed thrombi had a combination of red blood cells, platelets, and fibrin in variable amounts. 39
Venous thrombosis is formed under lower-shear stress on the surface of a largely intact endothelium, 37 and requires anticoagulation therapy as this is red thrombus, rich in fibrin, the substance that attaches the thrombus to the vessel wall with platelets attaching to the fibrin downstream.38,40 Layers of fibrin, red blood cells, platelets and leukocytes form venous thrombi, with platelet count being low compared with the other cells involved. Venous thrombosis occurs under conditions of low-shear rate, low oxygen tension, oxidative stress, pro-inflammatory gene upregulation and impaired endothelial-cell regulatory capacity. 41
Our current understanding of venous thrombosis is based on a conceptual model called Virchow’s Triad, in which a combination of abnormalities in the blood (proteins and cells), blood vessels (endothelial-cell activation and vessel architecture), and blood flow (disturbed flow or stasis) contribute to venous thrombus formation. 42 The contribution of plasma hypercoagulability to venous thrombosis is well characterized. However, the way in which red blood cells, platelets and leukocytes contribute remains poorly defined by either epidemiologic or basic studies. 42
Platelets play a role in the formation of venous thrombi by releasing polyphosphates and pro-inflammatory mediators, phosphatidylserine or tissue-factor-exposing microparticles (MPs), as well as by stimulating the formation of the neutrophils extracellular traps (NETs). Activated platelets induce neutrophils to release their nuclear material in forms of NETs (made of DNA, histones, and neutrophil granule constituents). Extracellular histones activate platelets, probably through the induced increase in von Willebrand factor release. 41 It has been reported that venous thrombi do not form in either platelet-depleted mice 43 or mice deficient in von Willebrand factor. 41 Platelet-derived MPs enhance clotting propagation after being initiated by tissue factor pathways and initiated thrombin generation. Increased spontaneous platelet aggregation and circulating platelet aggregates have been found in patients with idiopathic recurrent deep vein thrombosis (DVT). 41 ASA inactivates cyclooxygenase activity of prostaglandin H synthase 1 (COX-1) and synthase 2 (COX2), thereby blocking thromboxane A2 generation. It has been demonstrated that ASA reduces NET formation, also under different inflammatory or stress conditions, and a decreased deposition of platelets suggests that aspirin could be useful in avoiding undesired effects from neutrophil activation. ASA has also shown a reduction in platelet-derived MPs. 41
Recently, a new in vitro model of venous thrombosis has addressed a stepwise process leading to thrombus formation, and confirmed some of the aspects previously mentioned: first, that immobilized tissue factor initiates coagulation and fibrin deposition in the region of low wall-shear rates; second, that red blood cells are required for platelet accumulation and that platelets are required for fibrin expansion beyond the valve pocket; and third, that platelets adhere to fibrin, activate through glycoprotein VI, express phosphatidylserine and support thrombin generation, resulting in thrombus growth.42,44 However, the ability to extrapolate this experimental data to humans is limited. 39 Clinical trials have shown that low-dose aspirin reduces recurrent venous thrombosis45–47 and venous thrombosis after hip or knee arthroplasty. 48 In patients with antiphospholipid antibodies and recurrent pregnancy loss, or unexplained late pregnancy loss, a primary prophylactic regime of low-dose ASA and heparin is recommended. 13
Activated platelets, induced by atheromatous plaque disruption, interact with fibrinogen, and a thrombus is formed by fibrinogen-mediated cross-linking leading to platelet–platelet aggregation. 27 Eptifibatide, a glycoprotein IIb/IIIa antagonist, inhibits the binding of fibrinogen to the αIIb β3 receptor on human platelets, the final common pathway of platelet–platelet aggregation. In our case, as we thought that platelets may be involved in venous thrombus formation, after treatment with anticoagulation and antiaggregation with aspirin had not been successful, we added dual antiplatelet therapy, following the concept of cardiology, expecting to fight the thrombus via a different target.
Vessel-wall injury is not a prerequisite for venous thrombosis 38 but a chronic nonrecanalized CVT with fibrous septations, like the ones found on the DSA of this patient, could be a surface which promotes local thrombosis and produces impaired venous drainage and blood stasis, favoring thrombosis in the previously nondamaged endothelium. As a side note, during the transvenous treatment of dural arteriovenous fistulae, which are thought to appear after a CVT, septations of the affected venous sinus are a frequent finding. 49 The same idea could be applied to DVT, as the pathophysiology of recurrent unprovoked DVT may be different from that of primary DVT, due to damage on the vein wall from the initial thrombus insult. 40 In veins with regenerated endothelium, recurrent thrombosis is more likely. 40 Increased spontaneous platelet aggregation and circulating platelets aggregates have been shown in patients with idiopathic recurrent deep vein thrombosis. It may be that platelets play a more central role in recurrent DVT than in primary DVT, 41 and also in recurrent, rather than primary, CVT.
With this case, we would like to raise doubts as to whether anticoagulation therapy alone is sufficient for certain severe and refractory cases of CVT like the one presented here, and to ask whether platelets and antiaggregation could play a role in the therapy and prevention of recurrent CVT after these fibrous septations and stenoses have occurred. As we felt that there was a high risk of recurrence, our patient remained under dual-platelet inhibition in addition to anticoagulation for the duration of her pregnancy.
Conclusion
A woman with chronic CVT fell comatose during the first trimester of her second pregnancy. An impairment of the whole cerebral venous drainage system was confirmed by MRI/MRA and DSA. While therapeutic anticoagulation, endovascular rheolysis, and balloon angioplasty of the intracranial venous sinuses, as well as ADP platelet receptor inhibition all failed, inhibiting Gp IIb/IIIa platelet receptors with an eptifibatide infusion resulted in a rapid and almost complete recovery for the patient. This is an anecdotal experience with a low level of evidence. This treatment strategy could be associated with significant hemorrhagic risks. For the time being, it may only be considered as an option for patients with severe and progressive CVT after all other therapeutic measures have failed.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
HH is co-founder and shareholder of phenox GmbH and femtos GmbH. MAP has a proctoring and consulting agreement with phenox. VH has a consulting agreement with phenox. The other authors declare no potential conflict of interest.
Adherence to ethical standards
The ethics committee responsible (Ethik-Kommission bei der Landesärztekammer Baden-Württemberg) has stated in written form that ethics committee approval is not required for case reports.
The husband agreed to his wife’s treatment after being informed of the off-label nature of this procedure, including the potential and further possibly unknown risks. All therapeutic alternatives alongside their associated risks and benefits were explained to him.
After clinical recovery, the patient agreed to anonymized publication of her case history, understanding that the peculiar circumstances might still allow her to be identified.