
Abstract
Sialorrhoea is a frequent symptom of neurological diseases (e.g. Parkinson’s disease, motor neuron disease, cerebral palsy, and stroke) and is defined as excessive saliva accumulation leading to unintentional loss of saliva from the mouth. Sialorrhoea increases the overall burden on the patient and their caregivers, the impact of which can be both physical and psychosocial. Treatments for sialorrhoea range from lifestyle and behavioural guidance, to medications, surgery or radiation. Nonpharmacological interventions include advice on posture, swallowing control, cough management, dietary changes, eating and drinking techniques, and behavioural modification; however, these conservative measures may be ineffective for people with progressive neurological conditions. The pharmacological treatment of sialorrhoea is challenging because medications licensed for this purpose are limited, but treatments can include anticholinergic drugs and botulinum toxins. Surgical treatment of sialorrhoea is typically reserved as a last resort for patients. IncobotulinumtoxinA (Xeomin®) is the first botulinum toxin type A to receive US and UK marketing authorization for the symptomatic treatment of chronic sialorrhoea due to neurological disorders in adults. In this review, we discuss and compare the frequency and method of administration, location of treatment delivery, approximate annual costs and main side effects of botulinum toxin and different anticholinergic drugs. Management of patients with chronic neurological conditions requires input from multiple specialist teams and thus a multidisciplinary team (MDT) approach is considered fundamental to ensure that care is consistent and tailored to patients’ needs. To ensure that adult patients with neurological conditions receive the best care and sialorrhoea is well managed, we suggest a potential clinical care pathway for sialorrhoea with a MDT approach, which healthcare professionals could aspire to.
Defining sialorrhoea
Saliva is the substance produced and secreted from the three paired major salivary glands (parotid, submandibular and sublingual) and comprises water, electrolytes, mucus, antimicrobial compounds and enzymes. 1 Hypersalivation, sialorrhoea and drooling are often used interchangeably, 2 but they refer to different aspects of salivary continence. Hypersalivation refers to the increased production of saliva, whereas sialorrhoea refers to excessive saliva accumulation and the unintentional loss of saliva from the mouth. 3 Sialorrhoea can be caused by excessive production of saliva, or swallowing disturbances, which ultimately lead to an inability to retain saliva within the mouth. 4 This is also known as drooling, 5 defined as the presence of saliva beyond the margin of the lip. 1 Sialorrhoea is considered pathologic after the age of 4 years, as salivary continence is typically established by the age of 15–36 months,2,6 and may be a frequent symptom of neurological diseases (Figure 1). 3

Mechanism and consequences of sialorrhoea in adult neurological diseases.
The swallowing process is divided into voluntary (oral preparation and propulsion) and involuntary (pharyngeal and oesophageal) stages. 7 The involuntary stages of swallowing are under complex neural control, requiring coordinated contraction and inhibition of muscles located around the mouth, larynx, pharynx and oesophagus.8,9 Lack of coordination of the orofacial and palate–lingual musculature can inhibit the swallowing reflex and cause pooling of saliva in the oral cavity. 2 This, coupled with other symptoms of neurological conditions such as poor head control, constantly open mouth, poor lip control and impaired tongue mobility can result in an inability to retain saliva within the mouth. 1
In this review, we discuss the burden of sialorrhoea in the context of adult patients with neurological conditions and their caregivers, and current treatment options, including recent evidence on treatment with incobotulinumtoxinA (Xeomin®, Merz Pharmaceutical GmbH, Frankfurt am Main, Germany).
Impact of sialorrhoea in adult neurological diseases
Anterior sialorrhoea (unintentional loss of saliva specifically from the mouth) can have distressing consequences, such as damaging books and computers, soiling of clothes, rejection by friends and caregivers, and perioral infections.9,10 Less frequently, the spillage of saliva over the tongue and into the pharynx can occur (posterior sialorrhoea), which can result in aspiration pneumonia.10,11
Sialorrhoea is usually managed alongside other challenging symptoms caused by chronic neurological conditions and increases the overall burden on patients and caregivers. The physical and psychosocial burden for patients can result in a substantial impact on quality of life (QoL).2,3,12 Caregivers’ physical and mental health is also affected by sialorrhoea, since it can make assistance with feeding even more challenging and can lead to feelings of isolation, especially if sialorrhoea makes communication with the patient difficult. 13 We summarize the impact of sialorrhoea by specific disease below.
Motor neuron disease
Degeneration of bulbar neurons in motor neuron disease (MND) causes weakness in orofacial and lingual muscles which can result in difficulties in clearing oral secretions, leading to perioral ulcerations and risk of aspiration pneumonia. 14 The latter of these is the most harmful complication of MND, and has been associated with increased rates of hospitalization and reduced duration of survival.15,16 Non-invasive ventilation (NIV) can prolong survival in patients with amyotrophic lateral sclerosis (ALS), 17 particularly in patients with spinal-onset ALS. 18 However, bulbar impairment and the presence of secretions in the airways can reduce patients’ tolerance to NIV. 19
Evidence from current clinical practice has shown that sialorrhoea is suboptimally treated in patients with MND. An observational study conducted among UK neurologists reported sialorrhoea in 42% of patients (n = 193) attending their last MND clinic; almost half of the treating physicians considered sialorrhoea to be poorly controlled. 20 Despite sialorrhoea being a common symptom for MND patients, studies assessing its burden on patients and their caregivers, and potential contribution to speech difficulties, are lacking. 21 Consensus guidelines from the European Federation of Neurological Societies (EFNS) recognized that loss of communication skills by ALS patients can cause caregivers to become emotionally and intellectually isolated. 13 Additional responsibilities of caregivers, such as suctioning a patient’s airway and management of mechanical ventilators, 13 and potentially, tracheostomies, may contribute to anxiety and reduce time for socializing.
Parkinson’s disease
Nonmotor symptoms of Parkinson’s disease (PD) are common and disabling, 22 and associated with poorer QoL. 23 Sialorrhoea or ‘dribbling saliva’ is a frequent complaint in early, 24 and advanced, PD. 23 Prevalence rates of drooling vary from 32% to 74%, depending on the definition used, with a pooled prevalence rate of 56%. 5 In an early PD population [disease duration 3.5 years in patients with drooling (n = 320)], male sex, motor severity, excess daytime sleepiness, impaired sleep quality, constipation, and nontremor-dominant subtype were among the clinical factors associated with worsened drooling. 25 With advanced PD [disease duration 5 years in patients with drooling (n = 273)], drooling was associated with higher frequencies of speech disturbances and dysphagia, and increased severity of motor and nonmotor symptoms, depression and anxiety. 26 The mechanism of drooling in PD is multifactorial and includes reduced salivary swallowing and facial hypomimia, that, when severe, can lead to dribbling of accumulated saliva. 27 A small pilot study using videofluoroscopy has suggested that an underestimated consequence of sialorrhoea in PD is silent aspiration, which, along with diurnal sialorrhoea, may increase the risk of respiratory infection (3/19 patients). 28 However, such findings have not yet been replicated in larger cohorts.
In patients with PD, PD Questionnaire-39 (PDQ-39) subscores for stigma and difficulties with communication, mobility and activities of daily living, indicated greater impairment in QoL for patients experiencing sialorrhoea compared with patients without sialorrhoea. 26 In a small case–control study [PD patients: n = 58 (mean disease duration 11.0 ± 8.7 years); healthy participants: n = 51], drooling was present in 59% of patients with PD, the majority of whom were bothered by drooling in social situations. 29 Among PD patients who had sialorrhoea, one third reported that they had to swallow frequently to avoid difficulties in speaking, compared with <5% of PD patients without sialorrhoea. 29
A semistructured interview of 37 patients with PD in a community setting revealed that some patients with sialorrhoea felt guilty for the added burden of additional meal preparation time required by carergivers. 30 More than a third of Turkish primary caregivers (n = 50) reported symptoms of anxiety, and sialorrhoea was shown to negatively impact caregiver QoL scores (environment domain of the abbreviated version of the World Health Organization QoL assessment), during face-to-face interviews with a neurologist. 31
Cerebral palsy
Cerebral palsy (CP) manifests in early childhood and persists throughout life. 32 The worldwide prevalence of CP is estimated to be 2.0–2.5 per 1000 live births. 9 The majority of patients with CP in the UK can be expected to survive to 30 years of age if they have no severe impairments; however, survival is substantially impaired in patients with at least two disabilities. 33 Despite this, there is limited information available about the development of CP into adulthood and the accompanying needs of the adult patient. The majority of studies recruit only children and young adults with CP.
Data from the Northern Ireland Cerebral Palsy Register showed that 22% of children experienced excessive drooling, associated with more severe motor limitations (Gross Motor Function Classification System level IV or V) and intellectual impairment. 34 Videofluoroscopic evaluations of swallowing in children have shown that silent aspiration can be a problem in these patients.35,36 Although these data cannot be directly applied to adult patients with CP, the burden of dysphagia is likely to extend into adulthood. Results from a small-scale interview-based study showed that adults with CP (n = 32) with confirmed dysphagia reported increased difficulty during mealtimes. 37 Many patients reported a reluctance to change their diet to a softer consistency. 37 Adult CP patients with dysphagia may therefore experience longer meal times, reduced overall food intake, and difficulty in achieving optimal nutrition.
Stroke
Stroke patients have an increased risk of posterior sialorrhoea and aspiration pneumonia due to swallowing difficulties, increasing the burden on patients, their caregivers and healthcare professionals. Patients need close monitoring and may require admission to a stroke care unit, which is associated with additional healthcare costs. 38 The prevalence of swallowing disorders in stroke patients is 51–64%. 39 Of particular concern are the observations during videofluoroscopy studies,39,40 in which over two thirds of stroke patients with dysphagia experienced silent aspiration. 41
Acquired brain injury
Posterior drooling can delay weaning of patients from tracheostomies and rehabilitation following acquired brain injury,42,43 limiting the availability of optimal multidisciplinary care as access to the relevant departments and correct rehabilitation care is reduced. Tracheostomy formation can introduce significant physical and psychological barriers for patients in terms of functional outcomes. This, in turn, can substantially increase health and social care costs, since the admission of a patient with an acquired brain injury to specialist rehabilitation would cost £567/day (UK National Health Service [NHS]). 44
Up to 44.4% of patients with acquired brain injuries and tracheostomies, admitted to a rehabilitation department between April and December 2011, experienced salivary aspiration, many of whom required frequent manual suctioning of saliva (>10 times per day). 42 This requires an additional time commitment for nursing staff, equipment costs and long-term costs for a bed within the rehabilitation department.
Current treatment options for sialorrhoea
Current guidance for the clinical management of sialorrhoea
Initial treatment for sialorrhoea involves relevant lifestyle and behavioural changes that may be unfeasible for patients with progressive neurological conditions. If lifestyle changes are not possible or fail to adequately manage symptoms, options include medications, surgery or radiation.1,2 The majority of drug therapies used to treat sialorrhoea over the past decade are not licensed for this purpose, so must be prescribed off-label. The anticholinergic drug, glycopyrronium bromide, for example, is only licensed for the treatment of severe sialorrhoea in children and adolescents aged 3 years and older with chronic neurological disorders, in the UK. 45
Current National Institute for Health and Care Excellence (NICE) guidance for the management of PD suggests that pharmacological management should only be considered if nonpharmacological management is unavailable or ineffective. 46 For MND, current NICE guidance recommends that provision of advice on swallowing, diet, posture, positioning, oral care and suctioning should be considered first. 47 After this, NICE guidance currently suggests that antimuscarinic medicines should be considered as a first-line treatment for patients with MND. At present, NICE guidance suggests that glycopyrrolate (glycopyrronium bromide) should be considered as the first-line treatment for sialorrhoea in both PD, and MND patients with cognitive impairment; if ineffective, patients can be referred to a specialist service for botulinum toxin type A (BoNT-A).46,47 On 30 May 2019, incobotulinumtoxinA received UK marketing authorization for the symptomatic treatment of chronic sialorrhoea due to neurological disorders in adults.
Evidence-based recommendations from neurological scientific societies are also available but may differ from the guidance provided by regulatory agencies. Most recently, the International Parkinson and Movement Disorder Society highlighted that there was insufficient evidence regarding the safety of ipratropium bromide spray and glycopyrrolate for the treatment of drooling in patients with PD, while BoNT-A and -B were considered clinically useful with an acceptable risk profile if used with specialized monitoring. 48 The task force for ALS of the American Academy of Neurology acknowledged that anticholinergic drugs are generally tried first despite no proven effectiveness, and recommended that BoNT-B should be considered for patients with medically refractory sialorrhoea. Low-dose radiation therapy to the salivary glands may also be considered. 49 It should be noted, however, that these recommendations were published in 2009, so do not consider the most recent evidence from randomized controlled trials (RCTs).
Treatment decision making should also consider the classification of sialorrhoea as either transitory or chronic. Since transitory sialorrhoea is likely to resolve over time, the use of irreversible interventions would be inappropriate, in patients with acquired brain injuries, for example. 1 The choice of treatment could also have substantial downstream implications on healthcare resource utilization and costs. Treatment considerations for patients with sialorrhoea may be further complicated by the medications prescribed to control their underlying disease, or associated symptoms. This results in a high treatment burden for patients, with a range of the potential side effects that may require the prescription of further medications (polypharmacy). Indeed, the underlying primary disease requires treatment and clinical review by many different specialists (e.g. ear, nose and throat specialists, neurologists, specialist nurses, physical, occupational and speech therapists, pulmonologists, dietitians, psychologists, rehabilitation physicians, stroke consultants), as well as general practitioners (GPs) and social workers. 50 Caregivers have a crucial role in facilitating communication between the patient and healthcare provider, providing emotional support, and coordinating attendance at medical appointments; 51 all of which require a substantial time commitment and may require caregivers to take additional days off work or to arrange childcare. This is further complicated if patients have to attend separate appointments with each discipline on different days. 51
Nonpharmacological treatment options to reduce or prevent sialorrhoea
Nonpharmacological treatment options for sialorrhoea may require referral to specialists such as occupational therapists, physiotherapists, dietitians, and speech and language therapists who can provide advice on methods to control or manage salivary secretions (Figure 2).1,52

Nonpharmacological interventions for the management of sialorrhoea.
Speech and language therapists may encourage patients to make dietary changes (e.g. avoiding citrus fruits and alcohol) and introduce techniques to improve eating and drinking skills (lip closure, tongue movement and swallowing ). 1 Suctioning of saliva may be used to assist with removing secretions from the mouth and throat, 3 particularly in patients with an ineffective cough. The ability of patients to manage salivary secretions in their own home may be dependent on the loan of a suction unit from the patient’s GP or district nurse. 52 However, evidence to support the use of nonpharmacological interventions for sialorrhoea management remains limited, and approaches may be unsuitable for patients with progressive, chronic conditions, where longer-term solutions may be more appropriate.
Pharmacological therapies to reduce or prevent sialorrhoea
If nonpharmacological approaches are ineffective, inappropriate or not accessible (e.g. the healthcare service may not be available in the local healthcare setting), drug therapies (Table 1) can be trialled to reduce the secretion of saliva, thereby improving the mood and QoL of patients with sialorrhoea, as well as reducing the associated care burden.
Comparison of pharmacological treatment classes commonly used in the management of sialorrhoea in MND, PD and stroke.
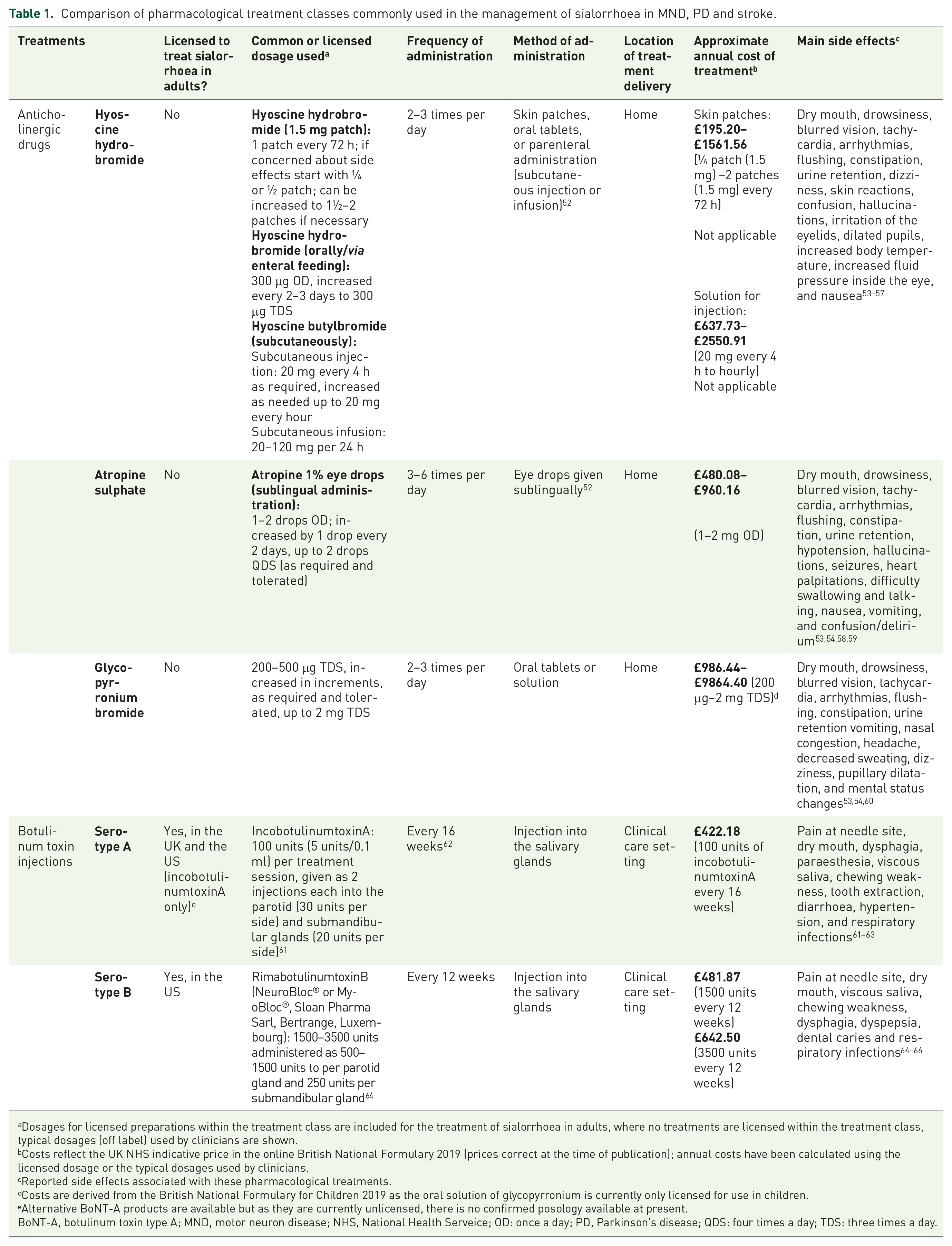
Dosages for licensed preparations within the treatment class are included for the treatment of sialorrhoea in adults, where no treatments are licensed within the treatment class, typical dosages (off label) used by clinicians are shown.
Costs reflect the UK NHS indicative price in the online British National Formulary 2019 (prices correct at the time of publication); annual costs have been calculated using the licensed dosage or the typical dosages used by clinicians.
Reported side effects associated with these pharmacological treatments.
Costs are derived from the British National Formulary for Children 2019 as the oral solution of glycopyrronium is currently only licensed for use in children.
Alternative BoNT-A products are available but as they are currently unlicensed, there is no confirmed posology available at present.
BoNT-A, botulinum toxin type A; MND, motor neuron disease; NHS, National Health Serveice; OD: once a day; PD, Parkinson’s disease; QDS: four times a day; TDS: three times a day.
There is limited evidence to guide clinicians in their choice of drug across neurological disorders, 20 apart from the recently published International Parkinson and Movement Disorder Society’s recommendations for PD treatments. 48 Pharmacological options include local and systemic anticholinergic drugs and BoNT injections.
Anticholinergic drugs
Anticholinergic drugs inhibit the action of the neurotransmitter acetylcholine at muscarinic receptors, which reduces the production of saliva. 3 Drugs such as atropine, hyoscine, glycopyrronium bromide, benzatropine and tropicamide can improve sialorrhoea in severely disabled patients and patients with PD.2,48,67–69
Glycopyrronium bromide response rates are between 12% and 81% (at a variety of doses; at least a 3-point improvement in drooling scores) in children,70,71 but limited evidence is available for use in adults. PD patients randomized to receive oral glycopyrrolate for 4 weeks, in a small-scale trial (n = 23), demonstrated improvements in the severity of sialorrhoea compared with placebo, using a self-reported sialorrhoea scoring scale. 68 Transdermally applied hyoscine hydrobromide has been shown to reduce salivary secretions by 50–100% in patients with a wide range of disorders causing sialorrhoea, with patient-reported improvements in drooling frequency.67,72 One administration can remain stable within serum for 72 h; this is beneficial to patients, as frequent administrations are not required, which may also translate into healthcare cost savings. 1
Botulinum toxins
BoNTs, when injected in the salivary glands, selectively bind to cholinergic nerve terminals and temporarily inhibit the release of acetylcholine, blocking salivary secretions. 2 Until recently, injection of the salivary glands with BoNTs was suggested as a specialist (off-label) second-line treatment for sialorrhoea in MND and PD in the 2016/2017 NICE guidelines: Motor Neurone Disease: Assessment and Management and Parkinson’s Disease in Adults.46,47 Recently, the US Food and Drug Administration (FDA) approved the use of incobotulinumtoxinA and rimabotulinumtoxinB for the treatment of chronic sialorrhoea in adult patients in the US.62,64 In August 2019, NICE recommended incobotulinumtoxinA as an option for treating chronic sialorrhoea caused by neurological conditions in adults. 73 BoNT injections may be administered every 16 weeks; however, there is limited information to inform recommendations of the optimal timing of subsequent injections. 74 The reduced frequency of administration is a key advantage of BoNT treatment, in comparison with anticholinergic medications that are typically taken multiple times every day. Treatment with BoNT injection is typically well tolerated, and reported side effects appear to be less common than for anticholinergic treatments.53,54,63,75
Injection of BoNT-A into the salivary glands has been shown to improve the severity and frequency of sialorrhoea in patients with neurologic diseases including PD and ALS, with evidence from double-blind, placebo-controlled studies,75,76 and real-world evidence studies.77,78 Three formulations of BoNT-A and one formulation of BoNT-B are currently available, but only one of these formulations is currently licensed in the UK; 79 both treatments exhibited similar effectiveness and safety in a prospective, double-blind, crossover RCT of ALS and PD patients. 80
In a blinded RCT in patients with a range of neurologic disorders, greater improvement in sialorrhoea was observed upon injection of more salivary glands with BoNT. 81 The choice of salivary gland to inject may also influence the efficacy of BoNT, but more evidence is required. 63 The duration of effect of BoNT-A and -B ranged between 2 and 5 months in a retrospective study and an RCT.82,83 These findings suggest that substantial financial savings could be made since longer-term improvements in sialorrhoea could enable high-risk inpatients to be transferred from specialist to ward-based care (Box 1).
BoNT injections could reduce utilization of healthcare resources.
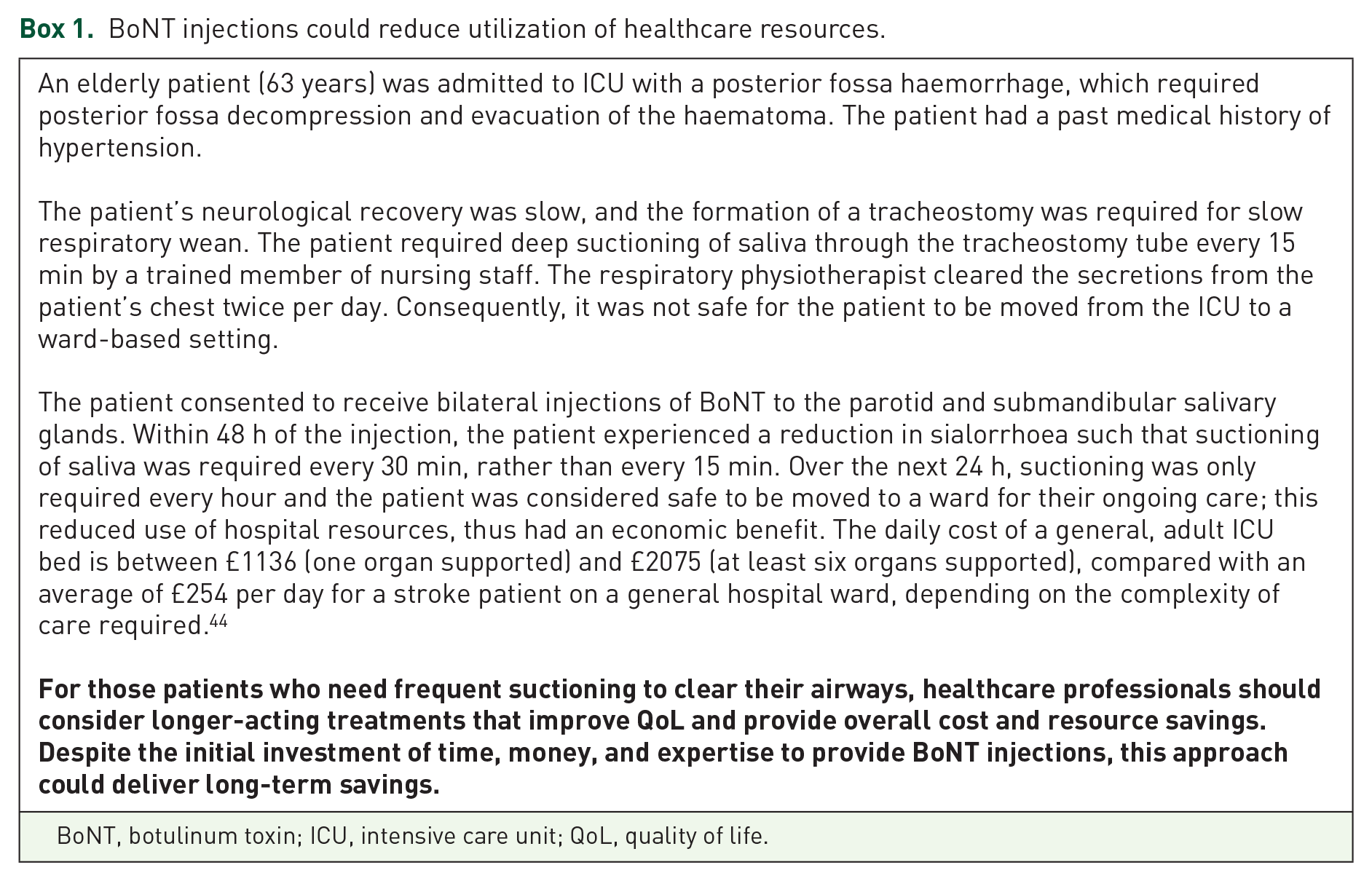
BoNT, botulinum toxin; ICU, intensive care unit; QoL, quality of life.
Improvements in the severity and frequency of sialorrhoea were reported by patients with neurological disorders during an RCT, 84 a dose comparison study, 85 and a real-world evidence study. 77 Patients with PD in Estonia reported thickening of saliva 1 month after injection with BoNT-A when interviewed, and a reduction in sialorrhoea severity from very intensive to moderate. 86 Retrospective analysis of patients in a movement disorders clinic showed that all patients treated with BoNT-A experienced improvements; a minimum of 50% improvement in sialorrhoea was observed using the Drooling Severity and Frequency Scale (DSFS). 87 The majority of PD outpatients completing an RCT reported satisfaction with BoNT treatment [moderate to dramatic improvement (77.7%; n = 18)] compared with placebo [no changes to mild improvement (94.4%; n = 18)]. 83 All patients receiving BoNT injections stated that they would receive repeated injections. 83
Patient-reported improvements in quality of daily living have also been reported in an open-label, prospective study, with improved outcomes including how often clothes and pillows were stained by saliva 4 and 12 weeks after injection with BoNT-B. 65 Similarly, a small-scale, open-label, prospective study reported improvements in Drooling Impact Scores in ALS patients treated with BoNT-A; patients scored factors that included how much sialorrhoea had influenced their speech, clothing, social activities and skin on their lower face. 88 A 3-year retrospective analysis showed that the total number of patients with CP treated with BoNT-A who required hospitalization decreased by >50% up to 21 months after receiving treatment; however, it is not possible to conclude that BoNT-A treatment was the only reason for this observation. 82 The administration of BoNT may improve the day-to-day QoL of patients, and their caregivers, which could substantially improve mood and independence (Box 2).
Improvements in quality of life following injection with BoNT.

BoNT, botulinum toxin; MDT, multidisciplinary team; PEG, percutaneous endoscopic gastrostomy; QoL, quality of life.
In patients who have not responded to nonpharmacological treatment or for whom these options are not feasible, BoNT injections may be an appropriate next step to manage sialorrhoea. We suggest a treatment algorithm (based on clinical practice in the UK) for the licensed BoNT, incobotulinumtoxinA, based on current information: a proposed algorithm for BoNT treatment of sialorrhoea in patients with ALS and the summary of product characteristics for incobotulinumtoxinA (Figure 3).63,61

Proposed treatment algorithm for the treatment of sialorrhoea with incobotulinumtoxinA.
IncobotulinumtoxinA in the management of sialorrhoea
IncobotulinumtoxinA (Xeomin®, Merz Pharmaceutical GmbH, Frankfurt am Main, Germany) is a purified BoNT-A, free from complexing proteins, and administered by injection into the salivary glands. IncobotulinumtoxinA acts as a neuroglandular blocking agent by inhibiting the release of acetylcholine 90 and consequently reducing the production of saliva, thus reducing sialorrhoea. The action of BoNT-A involves a four-step process: 90 (a) the heavy chain of the BoNT binds to the presynaptic membrane of cholinergic nerve endings; (b) the toxin complex is internalized; (c) the light chain is released into the cytoplasm; and (d) the light chain cleaves selected proteins [N-ethylmaleimide-sensitive factor attachment protein receptor (SNARE) proteins] that are critical for the release of acetylcholine into the synapse (Figure 4). A typical regimen for the administration of BoNT-A is two injections into the parotid gland and one injection into a single site of each submandibular gland. 53

Mechanism of action of botulinum toxin type A.
The SIAXI trial was the largest prospective, randomized, double-blind, placebo-controlled multicentre study investigating the use of incobotulinumtoxinA (75 or 100 U) for the treatment of sialorrhoea in patients with neurologic disorders. Patients injected bilaterally (parotid and submandibular glands; 3:2 dose ratio) with 100 U incobotulinumtoxinA showed significant reductions in unstimulated salivary flow rate from baseline, compared with placebo by week 4, which was maintained to week 16. 92 Patient-reported Global Impression of Change Scale (GICS) scores improved after 4 weeks of treatment with both dosages, compared with placebo. 92 IncobotulinumtoxinA (75 and 100 U) was well tolerated by patients and no new safety concerns were reported. 92 Overall, adverse events were reported in 32 (43.2%) and 34 (45.9%) patients treated with incobotulinumtoxinA, 75 U and 100 U, respectively, compared with 15 (41.7%) patients in the placebo group. The most frequent treatment-related AEs were dry mouth [incobotulinumtoxinA 75 U: 4 (5.4%) patients; incobotulinumtoxinA 100 U: 2 (2.8%) patients] and dysphagia [incobotulinumtoxinA 75 U: 2 (2.7%) patients; incobotulinumtoxinA 100 U: 0 patients].
A crossover RCT in the US (n = 10) found no significant difference in saliva weights 1 month after injection of BoNT compared with placebo; however, the small sample size is a limitation of this study. 93 Placebo-controlled and real-world evidence studies of incobotulinumtoxinA have demonstrated improvements in sialorrhoea and chronic troublesome sialorrhoea in patients with neurological conditions.77,78,81 A small-scale (n = 20), real-world-evidence study showed that injection of incobotulinumtoxinA under ultrasound guidance [parotid gland 12.5 ± 3.9 U (PD patients), 14.25 ± 4.3 U (ALS patients); submandibular gland 12.2 ± 4.5 U (PD patients), 13.3 ± 4.1 U (ALS patients)] reduced sialorrhoea by approximately 50% in gauze, sugar lump and patient-reported measurements (visual analogue scale) after 30 days in patients with PD and ALS. 78 Patients with sialorrhoea (n = 36) treated with incobotulinumtoxinA in community-based or tertiary hospital-based outpatient clinics, reported significant improvements in sialorrhoea using DSFS. 77
IncobotulinumtoxinA is the only BoNT not requiring refrigerated storage prior to reconstitution, making this a practical option for use in community-based clinics.77,94 In some countries, such as the UK, the frequency of use of anticholinergic drug treatments (e.g. glycopyrronium bromide) may increase the overall annual cost of treatment, when compared with repeat injections with incobotulinumtoxinA every 16 weeks (Table 1). The cost effectiveness of incobotulinumtoxinA is currently being assessed.
IncobotulinumtoxinA first received marketing authorization in the UK for the symptomatic treatment of blepharospasm, cervical dystonia of a predominantly rotational form (spasmodic torticollis) in adults in 2007, 61 and spasticity of the upper limbs in adults in 2009. IncobotulinumtoxinA received European Medicines Agency and UK approval for the treatment of chronic sialorrhoea due to neurological disorders in adults in May 2019. 61 In August 2019, IncobotulinumtoxinA was recommended by NICE, within its marketing authorization, as an option for treating chronic sialorrhoea caused by neurological conditions in adults. 73
Challenges of pharmacological therapies for sialorrhoea in neurological diseases
Pharmacological therapies for sialorrhoea can lead to significant improvements in patients’ symptoms, but the side effects and administration methods present some challenges. The additional burden may deter some patients from taking medications (and some carers from giving medication) to control their sialorrhoea.
Physicians and caregivers should monitor patients treated with anticholinergic drugs for associated adverse side effects 95 (Box 3), which include urinary retention, blurred vision, hallucinations and confusion. 96 Patients with PD who have cognitive impairments are more susceptible to developing these side effects, 3 or increased Alzheimer’s disease pathology. 97 Furthermore, care must be taken to avoid an excessively dry mouth in patients treated with anticholinergic drugs, 96 as this could further impair patients’ QoL. Thus, use of an anticholinergic burden scale is important when making treatment choices, to highlight when medications with a lower cognitive burden should be considered (Box 4). 98 Dryness of the mouth is a known side effect of both anticholinergic drugs and BoNTs,55,56,58,60,61,66 and should be carefully managed to avoid deterioration in patients’ dental health. 99 Since the protective effects of saliva are reduced in patients with hyposalivation, this can lead to an increase in dental caries, halitosis, and oral infections such as candidosis and sialadenitis. 99 Hyoscine hydrobromide patches can cause behavioural changes and visual disturbances (including blurred vision and accommodation problems). The observed behavioural changes were seen to resolve 12–24 h after removing the patch in a prospective RCT. 67
Adverse events associated with anticholinergic drug treatment. 95

PD, Parkinson’s disease.
Anticholinergic burden scales.

One of the key considerations of BoNT injection administration is whether the use of ultrasound guidance improves the effectiveness of sialorrhoea treatment; improvements have been observed in some studies.104,105 The availability of sufficiently trained staff to administer BoNT injections may also prevent patients from receiving this treatment. 20 However, authorization of onabotulinumtoxinA (BOTOX®, Allergan plc, Dublin, Ireland) as a prophylactic treatment for chronic migraine in the UK, in 2012, 106 may enable access to trained staff in established clinics. Improvements in sialorrhoea after administration of BoNT injections are temporary and repeat injections are necessary. The approved dosing guidance for incobotulinumtoxinA is every 16 weeks;62,61 repeat injections of BoNT within different timeframes may increase the chance of patients forming neutralizing antibodies against the BoNT. 107 Some serotypes are associated with greater risk of forming antibodies than others, so alternative serotypes may be trialled if antibodies against BoNT develop. 107 It is still unknown if injection intervals of less than 3 months can be safely used,74,107 but the risk of forming antibodies is considered to be relatively low in clinical practice. Clinicians may decide not to treat sialorrhoea with BoNT injections if they are concerned that dysphagia may worsen; 20 despite a paucity of research in this area, some small-scale studies suggest that swallowing dynamics are unaffected.108,109 A potential limitation to the use of some BoNTs in community-based clinics is the absence of refrigerators to store the drug; 77 however, the BoNT-A, incobotulinumtoxinA, does not require refrigerated storage prior to reconstitution.
Surgical treatment options
Due to the side effects and challenges associated with pharmacological treatments for sialorrhoea, some patients may prefer to take an alternative approach. Surgical treatment options are destructive and irreversible (Table 2), so are typically reserved as the last resort for patients.
Comparison of the surgical treatment options for the management of sialorrhoea.
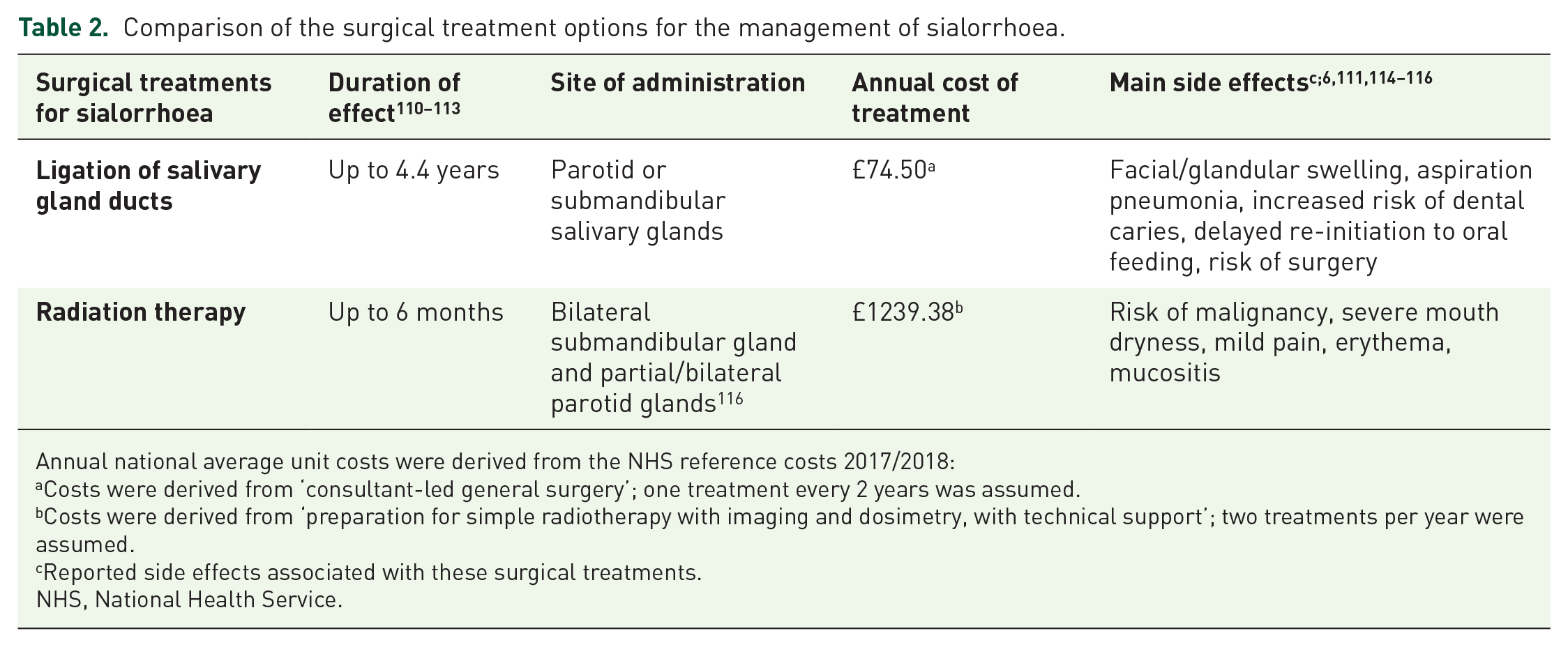
Annual national average unit costs were derived from the NHS reference costs 2017/2018:
Costs were derived from ‘consultant-led general surgery’; one treatment every 2 years was assumed.
Costs were derived from ‘preparation for simple radiotherapy with imaging and dosimetry, with technical support’; two treatments per year were assumed.
Reported side effects associated with these surgical treatments.
NHS, National Health Service.
Current surgical options for patients with sialorrhoea include the removal of the salivary glands (typically the parotid and submandibular glands), surgery to ligate or reroute salivary gland ducts, or interrupt the parasympathetic nerve supply to the salivary glands.1,117,118 Due to their invasive nature, these options are unsuitable for patients with transitory sialorrhoea. Intraductal laser photocoagulation of the bilateral parotid ducts is a less invasive option with positive results from early reports.1,119 Patients may also require the formation of a tracheostomy for long-term assisted ventilation, due to loss of bulbar tone and difficulty in clearing salivary secretions that makes use of NIV ineffective. 120 Reported outcomes following surgical management of sialorrhoea are mostly limited to studies in children, and evidence may not be relevant to adult patients.110,111,114 However, dental caries can occur following surgical treatment for sialorrhoea in children, so this risk should be considered when making treatment decisions.121,122
Radiation therapy of the salivary glands is a rarely used treatment option and is typically reserved for elderly patients who cannot undergo surgery or tolerate available drug therapies. 2 Administration of palliative single-dose radiotherapy to the parotid salivary gland of patients with ALS significantly reduced salivary secretion, compared with salivation prior to treatment in a prospective study of 20 patients in Norway. 123 Similar observations were made in a retrospective US case series study of 10 consecutive patients with ALS. 124 Comparison between BoNT and salivary gland radiotherapy showed no differences in patient-reported burden of sialorrhoea. 125
Models of care
As highlighted above, patients with chronic neurological conditions have complex symptoms that require input from multiple specialist teams. A multidisciplinary team (MDT) approach is considered fundamental to ensure that care is consistent and tailored to a patient’s needs.
The EFNS guidelines recommend multidisciplinary care for MND patients, including hospital- and community-based services. 13 The provision of MDT clinics for patients with ALS in the Republic of Ireland, Sheffield and the Netherlands have demonstrated improvements in the prognosis and mental QoL of patients, when compared with those attending general neurology clinics.50,126,127 The study conducted in the Netherlands may provide useful insights for ALS care, but the researcheres were required to follow the Dutch ALS consensus guidelines, so may not be generalizable to other regions. 127 The MDT approach is also important to ensure that all the patient’s concerns are addressed, including the needs of their family and primary caregivers. 128
Mean monthly healthcare costs were similar for patients with ALS receiving MDT (€1336 per patient) or general care (€1271 per patient) in a cost-of-illness analysis conducted in the Netherlands. 129 Early referral of ALS patients to a MDT could prevent unnecessary procedures and consultations, with an estimated saving of €2072 per patient receiving MDT care. 130 Therefore, implementing an MDT approach in other complex conditions (e.g. PD and stroke) might be cost effective, especially if symptoms such as sialorrhoea could be addressed earlier. At present, patients do not follow a specified clinical route, as the services available to patients often vary by location. An example of a possible clinical pathway with an MDT approach including sialorrhoea management is provided in Figure 5.
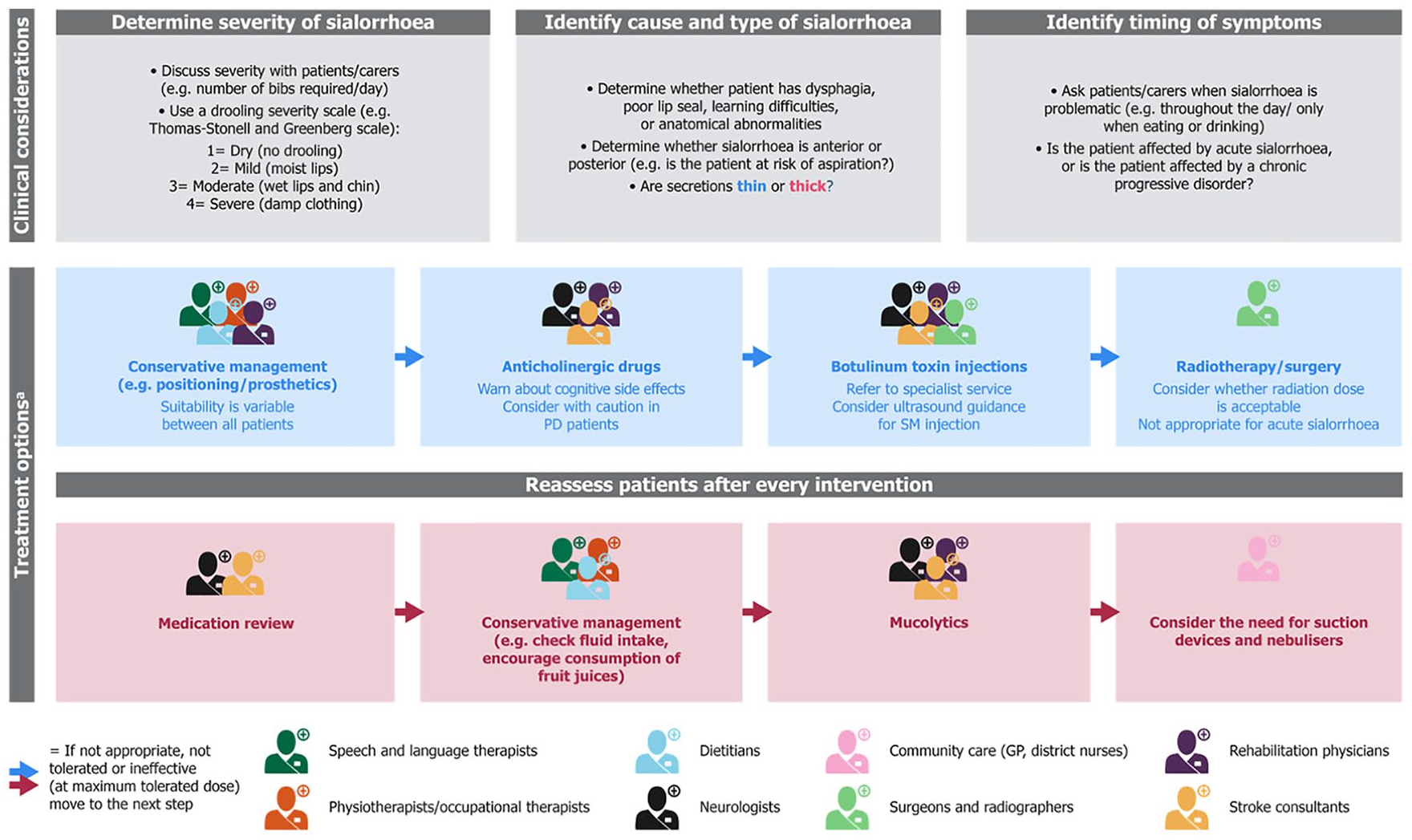
An example of a holistic model of care with an MDT approach in patients with neurological diseases and sialorrhoea.
Expert opinions and recommendations
Sialorrhoea is a frequent and disabling symptom of adult neurological diseases, which often results in polypharmacy. Despite being associated with poorer QoL, speech difficulties, and harmful complications such as aspiration pneumonia, sialorrhoea is still an under-recognized and undertreated symptom. In addition, treatment pathways currently used for neurological conditions such as CP, stroke and acquired brain injury or neurodegenerative diseases such as ALS and PD, rarely include sialorrhoea management within the patient’s care plan. An example of a clinical pathway for sialorrhoea with an MDT approach that patients and clinicians could aspire to, is provided in Figure 5.
Here, we provide recommendations for management of sialorrhoea in adult neurological conditions:
(1) Increasing awareness of the burden of sialorrhoea on patients and their caregivers, among healthcare professionals, could lead to improved patient care.
(2) More research is needed to demonstrate the benefits, side effects, and cost effectiveness of treatment options in the various conditions causing sialorrhoea.
(3) Greater awareness among healthcare professionals of the treatment options available for sialorrhoea management could improve patient care. The options range from nonpharmacological to pharmacological treatments, which have varying levels of supporting evidence.
(4) The provision of training in the administration of BoNT injections to clinicians could increase the availability of this treatment and reduce delays in the referral of patients to this service.
(5) Additional funding (e.g. from the Clinical Commissioning Group in England) for sialorrhoea could help to reduce significant delays in treatment.
Supplemental Material
APPROVED_Xeomin_Prescribing_information_UKIE_combined_June_2019_v4 – Supplemental material for The burden of sialorrhoea in chronic neurological conditions: current treatment options and the role of incobotulinumtoxinA (Xeomin®)
Supplemental material, APPROVED_Xeomin_Prescribing_information_UKIE_combined_June_2019_v4 for The burden of sialorrhoea in chronic neurological conditions: current treatment options and the role of incobotulinumtoxinA (Xeomin®) by Francesca Morgante, Ganesh Bavikatte, Fahim Anwar and Biju Mohamed in Therapeutic Advances in Neurological Disorders
Footnotes
Acknowledgements
The authors would like to thank the patients who very kindly gave their permission for their case studies to be included within this publication. The authors also acknowledge Sarah Jayne Clements, PhD, from Costello Medical, Cambridge, UK, for medical writing and editorial assistance in preparing this publication, based on the authors’ input and direction.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication sponsorship, medical writing support and compensation for authors’ time were funded by Merz Pharma GmbH (Frankfurt).
Conflict of interest statement
FM: honoraria for advisory board/consultancy from Medtronic and Merz; speaker’s fees from Merz, BIAL, UCB Pharma, Medtronic, Chiesi, AbbVie and Zambon; editorial board member of Movement Disorders and Movement Disorders Clinical Practice; receipt of royalties from Springer for the book Disorders of Movement; Consultancy fees for expert review and guidance in the development of this supplement as an independent contractor for Merz Pharma GmbH; GB, FA: consultancy fees for providing expert review and guidance in the development of this supplement as an independent contractor for Merz Pharma GmbH; BM: grants from NeuroDerm, Bevan Commissions and Parkinson’s UK; honoraria for lectures from UCB Pharma and Profile Pharma; consultancy fees from AbbVie, Profile Pharma, Britannia and BIAL; consultancy fees for expert review and guidance in the development of this supplement as an independent contractor for Merz Pharma GmbH.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.