
Abstract
In 2014, the definition of embolic strokes of undetermined source (ESUS) emerged as a new clinical construct to characterize cryptogenic stroke (CS) patients with complete vascular workup to determine nonlacunar, nonatherosclerotic strokes of presumable embolic origin. NAVIGATE ESUS, the first phase III randomized-controlled, clinical trial (RCT) comparing rivaroxaban (15 mg daily) with aspirin (100 mg daily), was prematurely terminated for lack of efficacy after enrollment of 7213 patients. Except for the lack of efficacy in the primary outcome, rivaroxaban was associated with increased risk of major bleeding and hemorrhagic stroke compared with aspirin. RE-SPECT ESUS was the second phase III RCT that compared the efficacy and safety of dabigatran (110 or 150 mg, twice daily) to aspirin (100 mg daily). The results of this trial have been recently presented and showed similar efficacy and safety outcomes between dabigatran and aspirin. Indirect analyses of these trials suggest similar efficacy on the risk of ischemic stroke (IS) prevention, but higher intracranial hemorrhage risk in ESUS patients receiving rivaroxaban compared to those receiving dabigatran (indirect HR = 6.63, 95% CI: 1.38–31.76). ESUS constitute a heterogeneous group of patients with embolic cerebral infarction. Occult AF represents the underlying mechanism of cerebral ischemia in the minority of ESUS patients. Other embolic mechanisms (paradoxical embolism via patent foramen ovale, aortic plaque, nonstenosing unstable carotid plaque, etc.) may represent alternative mechanisms of cerebral embolism in ESUS, and may mandate different management than oral anticoagulation. The potential clinical utility of ESUS may be challenged since the concept failed to identify patients who would benefit from anticoagulation therapy. Compared with the former diagnosis of CS, ESUS patients required thorough investigations; more comprehensive diagnostic work-up than is requested in current ESUS diagnostic criteria may assist clinicians in uncovering the source of brain embolism in CS patients and individualize treatment approaches.
Theoretical concept of embolic strokes of undetermined source
Even though no etiopathogenic mechanism can be identified in more than one-third of all ischemic strokes (IS), the definition of cryptogenic cerebral ischemia still remains very vague, given that the characterization of a cerebral ischemic event as cryptogenic depends largely on the diagnostic investigations performed, the quality of these exams, and the subjective assessment of the treating physician.1,2 The most frequently used definition of cryptogenic stroke (CS) to date is based on the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria, which were first published in 1993. 3 TOAST criteria classify an IS as cryptogenic when no cause can be identified after baseline diagnostic work-up. However, IS with incomplete work-up or cerebral infarctions with two or more possible underlying causes are also characterized as cryptogenic. The lack of specified mandatory diagnostic testing and work-up algorithm imple-mentation of TOAST criteria results in huge variations in the reported prevalence of CS across hospital registries, as a consequence of poor agreement between physicians to classify a cerebral ischemic event as cryptogenic.4,5
In 2007, the Causative Classification of Stroke system proposed to subdivide strokes of undetermined cause further into cryptogenic embolism, other cryptogenic, incomplete evaluation, and unclassified groups. 6 In 2014, the definition of embolic strokes of undetermined source (ESUS) emerged as a new clinical construct to characterize nonlacunar (>1.5 cm on CT or >2 cm on MRI), nonatherosclerotic (absence of significant ipsilateral vessel stenosis ⩾50%) strokes of an undetermined embolic source, in the absence of a high-risk for embolism cardiac disease or any other specific cause. 4 ESUS working group investigators further proposed that the minimal stroke work-up should include brain neuroimaging with CT or MRI, 12-lead ECG, transthoracic echocardiography (TTE), 24 h Holter-ECG and imaging of both extracranial and intracranial vessels with any available imaging modality (DSA, MRA, CTA, or US). Transesophageal echocardiography (TEE) and long-term ECG monitoring were not included as mandatory investigations in the diagnostic work-up of ESUS patients. Approximately 9–25% of IS patients fulfil ESUS diagnostic criteria with any variance attributed to the characteristics of the patient population.7,8
Outcomes in ESUS and CS
Atrial fibrillation (AF), either paroxysmal or persistent, is associated with a fivefold increase in IS risk, while paroxysmal AF appears to be implicated in at least 30% of patients with CS.9–11 Antiplatelet treatment, advocated by current guideline recommendations for patients with CS, 12 is known to provide inadequate protection from future cardioembolic events in patients with AF. 13 On the contrary, it has been estimated that the administration of anticoagulant therapy reduces the annual IS recurrence risk by 8.4% compared with antiplatelet therapy in IS patients with AF. 14
Population-based studies suggest that CS harbor a non-negligible risk of recurrence and mortality, which are both comparable to the magnitude of IS attributed to cardioembolism.15–17 ESUS patients also have comparable cumulative probability of 5-year stroke recurrence as cardioembolic strokes, with an estimated annual stroke recurrence risk of 4.5% (range 2.3–6.8%).7,18 However, mortality risk in ESUS patients is suggested to be lower compared to strokes attributable to cardioembolism or other etiologies, with a reported annual mortality rate of 5.2%. 19 ESUS patients are not only younger compared to AF patients, but baseline stroke severity in ESUS cases is also lower than in patients with cardioembolic stroke, and this may indicate that ESUS is associated with smaller cerebral emboli compared with patients with a definite cardiac source. 7
The importance of this life-time risk for recurrence and lack of an efficacious treatment is further exacerbated by the increased incidence of CS in young patients less than 50 years of age, and the relative mean young age (65 years) of ESUS patients.7,20 Notably, a recent Finnish study reported that ESUS represented 21% of all cases of first-ever IS amongst patients aged 15–49 years. ESUS patients were younger, had milder cardiovascular risk factor burden, and more favorable long-term outcomes compared with other causes of stroke in the young. 17
Vitamin K antagonists versus aspirin in secondary prevention of CS
The Stroke Prevention in Reversible Ischemia Trial (SPIRIT) was the first multicenter RCT to assess the utility of oral anticoagulation with an INR target of 3.0–4.5 compared with antiplatelet treatment in the secondary prevention after a cerebral ischemic event of presumed noncardiac origin. 21 The trial was prematurely terminated at the first interim analysis, after inclusion of 1316 patients with a mean follow-up of 14 months, due to the unfavorable effect of warfarin [hazard ratio (HR) = 2.3; 95% confidence interval (95% CI): 1.6–3.5] on the primary outcome of interest (death from all vascular causes, nonfatal stroke, nonfatal myocardial infarction, or nonfatal major bleeding complication). 21 The investigators reported that each 0.5 unit increase of the achieved INR increased the bleeding risk by a factor of 1.43 (95% CI, 0.96–2.13). 21
Warfarin-Aspirin Recurrent Stroke Study (WARSS) was the second multicenter RCT to compare warfarin to aspirin 325 mg in the secondary prevention of patients with noncardioembolic stroke within 30 days. 22 After including a total of 2206 patients, no difference between the two groups was found in the primary endpoint of recurrent IS or death (HR = 1.13, 95% CI: 0.92–1.38). 22 Although INR target was lower than the usual therapeutic range (INR target of 1.4–2.8), major bleeding events were still more frequent in the warfarin group compared to the aspirin group (2.22 versus 1.49 per 100 patient-years; Risk Ratio = 1.48, 95% CI: 0.93–2.44). 22 In an exploratory analysis benefit of warfarin over aspirin was suggested in a subgroup of CS patients in whom neuroimaging revealed infarcts of potential embolic origin. 23
Taking into account the safety concerns of SPIRIT trial and the negative efficacy results of WARSS trial, the European/Australasian Stroke Prevention in Reversible Ischaemia Trial (ESPRIT) trial randomized 1089 patients with noncardioembolic stroke to receive medium intensity warfarin treatment (INR between 2 and 3) or ASA (30–325 mg) within 6 months of onset. 24 After a mean follow-up of 4.6 years, no difference was detected between the two groups in the primary efficacy composite outcome (HR = 1.02, 95% CI 0.77–1.35) or the risk of recurrent ischemic events (HR = 0.73, 95% CI: 0.52–1.01). Again, warfarin was associated with increased risk of major bleeding complications (HR = 2.56, 95% CI: 1.48–4.43). 24 In brief, any theoretical benefit of recurrent IS reduction with vitamin K antagonists has been offset by the increased risk of major and intracranial bleeding with coumadin or warfarin compared with aspirin.
In view of the more favorable safety profile of direct thrombin inhibitors or factor Xa inhibitors (relative risk reduction of approximately 50% in any or fatal intracranial hemorrhage compared with VKA), 25 it has been postulated that non-vitamin K antagonist oral anticoagulants (NOACs) may represent a promising therapeutic option in CS patients with an embolic source as their underlying stroke mechanism. 4
Non-vitamin K antagonist oral anticoagulants (NOACs) versus aspirin in the secondary prevention of ESUS
NOACs have emerged as an effective alternative with less bleeding complications compared to warfarin in patients with nonvalvular AF. 26 The appealing efficacy and safety profile of NOACs was further confirmed in the Apixaban Versus Acetylsalicylic Acid to Prevent Stroke in Atrial Fibrillation Patients Who Have Failed or Are Unsuitable for Vitamin K Antagonist Treatment (AVERROES) trial, which provided unflinching evidence that apixaban is more effective in the prevention of stroke or systemic embolism without significantly increasing the risk of major bleeding or intracranial hemorrhage compared with aspirin in patients with atrial fibrillation deemed unsuitable for VKA (vitamin K oral anticoagulant) treatment. 27
New Approach Rivaroxaban Inhibition of Factor Xa in a Global Trial versus ASA to Prevent Embolism in Embolic Stroke of Undetermined Source (NAVIGATE ESUS) was the first trial to compare the efficacy and safety of rivaroxaban (15 mg oral daily) with aspirin (100 mg oral daily) for the secondary prevention of ESUS patients. 28 The trial was prematurely terminated at the recommendation of the data and safety monitoring committee since rivaroxaban resulted in higher rates of major bleeding compared to aspirin (HR = 2.72; 95% CI, 1.68–4.39) and without clear efficacy for the primary outcome (first recurrence of IS, hemorrhagic stroke, or systemic embolism) after a median follow up of 11 months and enrollment of 7213 patients. 28 Except for the lack of efficacy in the primary outcome (first recurrence of ischemic or hemorrhagic stroke or systemic embolism), rivaroxaban was associated with increased risk of major bleeding (HR = 2.72; 95% CI: 1.68–4.39) and hemorrhagic stroke (HR = 6.50, 95% CI: 1.47–28.8) compared with aspirin. 28 The Randomized, Double-blind, Evaluation in Secondary Stroke Prevention Comparing the EfficaCy and Safety of the Oral Thrombin Inhibitor Dabigatran Etexilate (110 mg or 150 mg, oral b.i.d.) Versus Acetylsalicylic Acid (100 mg Oral q.d.) in Patients With Embolic Stroke of Undetermined Source (RE-SPECT ESUS) trial has recently presented neutral results with similar efficacy and safety outcomes between dabigatran and aspirin; however, there was no increase in the risk of bleeding events. 29 More specifically, the main findings of RE-SPECT ESUS were presented in 11th World Stroke Congress that took place in Montreal, October 17–20, 2018. However, it should be noted that the trial results have not yet been published in a peer-reviewed medical journal.
The study designs of NAVIGATE ESUS and RE-SPECT ESUS trials are summarized in Table 1. The two trials differed in NOAC dose (fixed dose of 15 mg for rivaroxaban; dose of dabigatran adjusted for age and renal function), inclusion criteria (patients were excluded from NAVIGATE ESUS if they were scheduled to undergo implantable cardiac monitoring or closure of patent foramen ovale; patients with the former characteristics were eligible in RE-SPECT ESUS; intracranial imaging was optional in NAVIGATE ESUS and mandatory in RE-SPECT ESUS) primary endpoint and statistical analysis plan. Table 2 outlines substantial similarities in the baseline characteristics of patients randomized to rivaroxaban in NAVIGATE ESUS and dabigatran in RE-SPECT ESUS. Table 3 presents indirect analyses on the risk of the cerebrovascular events between the NOAC groups of NAVIGATE ESUS and RE-SPECT ESUS trials, 30 while Table 4 presents indirect estimates on the safety outcomes of major bleeding and hemorrhagic stroke between the NOAC group of RE-SPECT ESUS trial and the NOAC subgroup of patients in the AVERROES trial with history of prior stroke or TIA. These indirect analyses indicate no difference in the risk of stroke and cerebral infarction between dabigatran and rivaroxaban for the secondary prevention of ESUS (Figure 1). Nevertheless, the risk of intracranial hemorrhage was higher in ESUS patients randomized to rivaroxaban compared to those randomized to dabigatran (indirect HR = 6.63, 95% CI: 1.38–31.76; Table 3). This observation is in line with a previous network meta-analysis of available RCTs for secondary stroke prevention in patients with nonvalvular AF, presenting indirect evidence that dabigatran is associated with a lower risk of hemorrhagic stroke compared to rivaroxaban. 31 Interestingly, another meta-analysis comparing individual NOACs to aspirin across all indications reported that, although rivaroxaban at doses 15 mg or 20 mg once daily is associated with an increased risk of intracranial hemorrhage compared with aspirin, lower doses (10 mg once daily or 5-mg twice daily) were not. 32 Finally, we documented no differences in the risk of IS, hemorrhage and overall stroke between IS patients with atrial fibrillation randomized to apixaban in AVERROES and ESUS patients randomized to dabigatran in RE-SPECT ESUS (Table 4). Nevertheless, it should be noted that indirect comparisons between different trials with disparities in study protocols should be used only for hypothesis generation. Specifically, indirect comparisons between RE-SPECT ESUS and AVER-ROES trials are particularly susceptible to unmeasured confounding due to markedly different trial designs and inclusion criteria. Addi-tionally, the higher annualized rates of hemorrhagic stroke reported in the ASA group of RE-SPECT ESUS trial compared with the ASA group of NAVIGATE ESUS trial (0.7% versus 0.1%; Table 3) should also be highlighted and be taken into account when performing indirect comparisons between the two RCTs.
Overview of the differences of study design between the NAVIGATE and RESPECT ESUS randomized clinical trials.
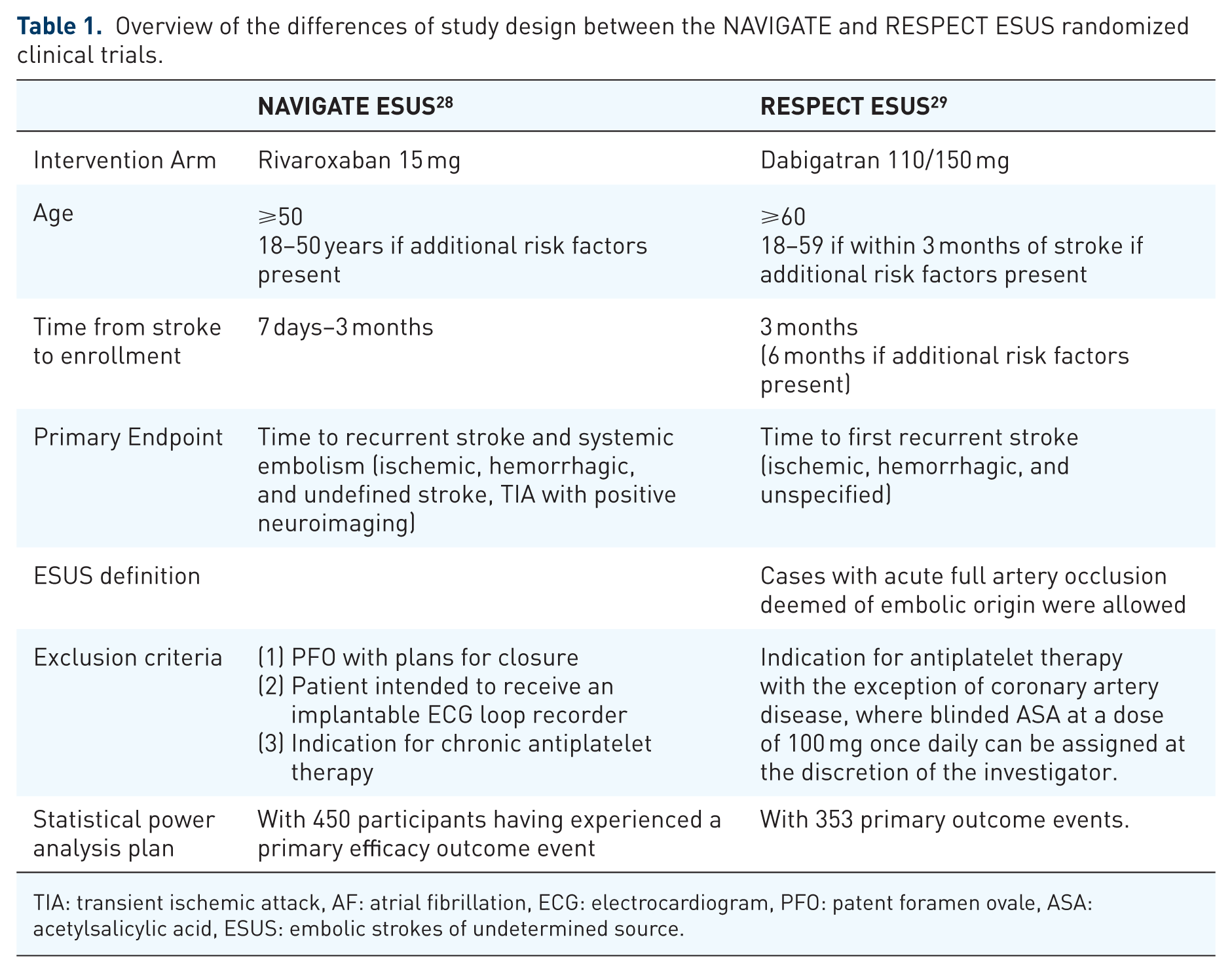
TIA: transient ischemic attack, AF: atrial fibrillation, ECG: electrocardiogram, PFO: patent foramen ovale, ASA: acetylsalicylic acid, ESUS: embolic strokes of undetermined source.
Overview on the baseline patient characteristics of patients treated with non-vitamin K oral anticoagulants (VKA) within the NAVIGATE and RESPECT ESUS randomized clinical trials.

SD: standard deviation, TIA: transient ischemic attack, NIHSS: National Institute of Health Stroke Scale, IQR: interquartile range, N/A: not available.
Indirect analyses on the annualized risk of the cerebrovascular events between randomized clinical trials evaluating the safety of non-vitamin k oral anticoagulants (VKA) in the secondary prevention of patients with embolic stroke of undetermined source.

Percentages present the annualized rates of the outcomes of interest.
RVX: rivaroxaban, ASA: acetylsalicylic acid, DBG: dabigatran, HR: hazard ratio, N/A: not available.
Indirect analyses on the risk of the safety outcomes of major bleeding and hemorrhagic stroke between randomized clinical trials evaluating the safety of non-vitamin k oral anticoagulants (VKA) in the secondary prevention of cerebral ischemia.
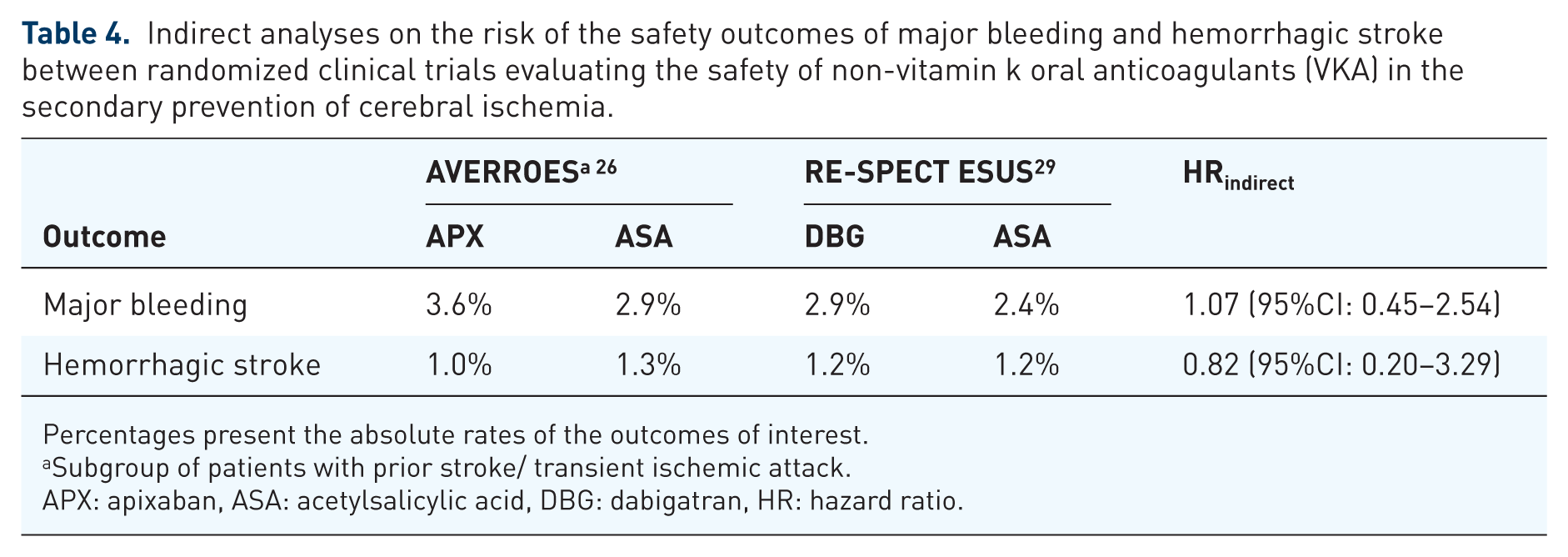
Percentages present the absolute rates of the outcomes of interest.
Subgroup of patients with prior stroke/ transient ischemic attack.
APX: apixaban, ASA: acetylsalicylic acid, DBG: dabigatran, HR: hazard ratio.

Forest plot presenting the recurrent stroke risk of patients with embolic strokes of undetermined source randomized to non-vitamin K antagonist oral anticoagulants or aspirin.
Discussion
Several observational studies have arbitrarily postulated occult cardioembolism as the main underlying mechanism in the majority of patients with cryptogenic cerebral embolism, by portraying for example the high prevalence of ischemic lesions in multiple arterial territories in patients with CS compared with other IS subgroups. 33 However, a wider range of potential sources for embolism are possible, and a comprehensive stroke work-up, employing further diagnostic testing, can drastically reduce the percentage of patients classified as CS, particularly in younger ages (⩽45 years).34,35
TEE is an example of a diagnostic test mandated neither by the ESUS criteria nor by the randomized clinical trials NAVIGATE ESUS and RE-SPECT ESUS,27,28 which has been estimated to further disclose abnormalities in more than half of patients with CS and negative baseline work-up. 36 In such cases, TEE can not only uncover the underlying pathogenic stroke mechanism, but can also guide therapeutic management in 9% of the cases.37,38 In ESUS patients, TEE examination was found to uncover abnormal findings in more than half, and significantly impact a change in management other than anticoagulant initiation in 8%, of patients (closure of patent foramen ovale, antibiotic administration due to infective endocarditis). 39 Especially in the case of endocarditis, TTE is known to have very low diagnostic yield, and thus TEE investigation is mandated. 40 Patent foramen ovale (PFO) was found in almost one-third of patients with ESUS, constituting the second more common finding after investigation with TEE. 39 Both NAVIGATE ESUS and RE-SPECT ESUS presented prespecified analyses in ESUS patients with PFO, reporting that neither rivaroxaban (HR = 0.54, 95% CI: 0.22–1.36) nor dabigatran (HR = 0.88, 95% CI: 0.45–1.71) were superior compared to aspirin,28,29 with no significant difference in the effect magnitude between the two drugs (indirect HR = 0.61, 95% CI: 0.20–1.90). Taking into account the results of recently reported RCTs providing solid evidence of superiority for PFO closure compared with medical treatment41–44 and the long-term bleeding risk from anticoagulant treatment it becomes evident that PFO closure currently presents as the optimal treatment option for selected ESUS patients with PFO <60 years and no other identifiable cause for the ischemic event.45,46
Interestingly, a cross-sectional observational study provided evidence that nonstenotic (<50%) carotid atherosclerotic plaques with ⩾3 mm thickness were significantly more prevalent ipsilateral to the ESUS event. 47 In another pilot imaging study, one out five ESUS patients were found to harbor ipsilateral intraplaque hemorrhages in their nonstenotic (<50%) carotid artery atherosclerotic plaques. 48 The aforementioned evidence suggest that arterio-arterial embolism is potentially feasible even in the absence of significant (>50%) lumen stenosis, and thus can represent another potential mechanism of ESUS that is not optimally manageable with anticoagulation. 49 Furthermore, microatheromatosis of basilar artery branches may result in pontine infarctions, with diameters exceeding 2.0 cm in diffusion weighted imaging that may be misclassified as ESUS and inadvertently be treated with oral anticoagulants (Figure 2). 49 Retrograde embolization from complex plaques in the proximal descending aorta during early diastole has also been highlighted as an alternative embolic source,50,51 which should be taken into consideration in patients with cerebral ischemic events of unknown source as a possible etio-pathogenic mechanism and marker of generalized atherosclerosis. 52 This notion has also been corroborated by a small, single-center study suggesting that ESUS patients can be distinguished in two opposite phenotypes according to the load of atherosclerotic pathology. 53 Taking into account that VKAs in all doses have failed to prove superiority for the secondary prevention of patients with ischemic cerebral events of presumed arterial origin, while medium and high intensity anticoagulation has been associated to a significant increase of major bleeding complications, 54 it becomes evident that anticoagulation, even with NOACs, is presumably not the optimal therapeutic approach in the ESUS subgroup of patients with a potential atherothrombotic mechanism. In addition, coagulation disorders in patients with malignancy, mild, or moderate heart valve abnormalities and carotid artery webs may also represent alternative embolic mechanisms in ESUS patients that may be underappreciated due to suboptimal diagnostic work-up.47,55

Characteristic example of a patient fulfilling the diagnostic embolic strokes of undetermined source (ESUS) criteria (maximum diameter of infarction diffusion-weighted imaging: 23 mm). The underlying mechanism of cerebral ischemia in this patient is microatheromatosis of basilar artery perforating branch and not brain embolism.
Given the comparatively mild stroke severity of ESUS compared with cardioembolic strokes, as reported by observational studies (mean NIHSS-score: 5 points), 28 the concept of occult cardioembolism being the major pathophysiologic mech-anism in ESUS has inevitably been disputed. 56 Additionally, the even milder strokes included in the NAVIGATE ESUS trial (median NIHSS: 1) raise further questions on the probability of potential selection bias. In NAVIGATE ESUS atrial fibrillation was reported in 2% of patients during the follow-up period of the trial. Interestingly, only one-third of patients in the CRYSTAL AF trial who met the inclusion criteria for NAVIGATE ESUS and RE-SPECT ESUS trials were diagnosed to have underlying AF after receiving continuous 3-year implantable cardiac monitoring (ICM).57,58 A similar AF detection rate has also been reported after 1 year of ICM in an observational study of 75 cryptogenic IS/TIA and presence of at least one AF risk factor. 59 Interestingly, embolic stroke patterns on neuroimaging with either CT or MRI were found to be associated neither with the diagnosis of ESUS nor with a short- or long-term diagnosis of AF. 60 However, advanced age and moderate-to-severe left atrial enlargement on echocardiography were highlighted as valuable predictors of AF detection in outpatient monitoring of ESUS patients. 61 Except for age, other vascular risk factors (obesity, congestive heart failure, hypertension, coronary artery disease, peripheral vascular disease, valvular disease) also emerged as significant predictors in the AF risk stratification of patients with cryptogenic cerebral embolism that underwent prolonged cardiac monitoring. 62 In any case, results from available observational studies suggest a diagnostic yield of AF detection with the use of ICMs in patients with CS or ESUS that is lower than 50%, with a positive association between the prevalence of AF and monitoring time (Table 5).10,63–72
Incidence of atrial fibrillation detection in cryptogenic stroke studies using implantable cardiac monitors.

ICM: insertable cardiac monitor, AF: atrial fibrillation, N/A: not available.
The Apixaban for Treatment of Embolic Stroke of Undetermined Source (ATTICUS) 73 and the atrial Cardiopathy and Antithrombotic Drugs In Prevention After Cryptogenic Stroke (ARCADIA) 74 are two ongoing RCTs that will evaluate the utility of apixaban compared with aspirin for the secondary stroke prevention of patients with ESUS or CS and concomitant large atrial enlargement or atrial cardiopathy, respectively.
Conclusion
ESUS constitutes a heterogeneous group of patients with presumably high likelihood of an occult embolic source. Except for undetected paroxysmal AF, present in the minority of ESUS patients, there are other embolic mechanisms (PFO, aortic plaque, nonstenosing unstable carotid plaque, cardiac valve disorders, coagulation disorders in patients with occult cancer) that mandate different management. Optimal secondary prevention for ESUS or CS still remains unknown, with current evidence from RCTs suggesting that indiscriminant anticoagulant treatment (with VKAs or NOACs) is neither effective nor safe (Table 6). Despite this, patients with CS/ ESUS should receive an extensive and individualized investigation, including high-resolution vessel imaging, TEE investigation and long-term cardiac rhythm monitoring to identify specific conditions such as paroxysmal AF or other cardioembolic sources that justify placing patients on anticoagulants. In view of the former considerations, the potential clinical utility of ESUS to guide clinicians towards a specific treatment is challenged by the findings of two RCTs revealing no benefit for NOAC versus aspirin. Excluding patients with infarctions due to branch disease with underlying intracranial microatheromatosis and using a more comprehensive diagnostic work-up (than the current diagnostic requirements included in the original ESUS diagnostic criteria) including TEE and at least 48-h Holter monitoring, may assist clinicians in uncovering the subgroup of ESUS that are caused by occult cardioembolism and individualize optimal treatment approaches in secondary prevention.
Results of randomized clinical trials assessing the efficacy of oral anticoagulant treatment in the secondary prevention of patients with stroke of undetermined etiology.

CS: cryptogenic stroke, ESUS: embolic stroke of undetermined source, VKA: vitamin K oral anticoagulant, ASA: acetylsalicylic acid, RVX: rivaroxaban, DBG: dabigatran.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.