
Abstract
Atrial fibrillation (AF) is a major cause of ischaemic stroke. The majority of these strokes can be prevented by treatment with oral anticoagulation therapy. The advent of non-vitamin K antagonist oral anticoagulants (NOACs) has resulted in a choice of therapeutic agents available to physicians for anticoagulation for stroke prevention in patients with AF beyond the long-established vitamin K antagonists (VKAs). Pivotal trials have demonstrated non-inferiority of NOACs compared with VKAs, and in some cases superiority, for the prevention of stroke and systemic embolism in non-valvular AF. Yet there are no direct head-to-head comparator trials for the efficacy of NOACs. Therefore, the question of which oral anticoagulant for each individual patient can present a challenge to physicians. In this review article, we assess which patients with AF require anticoagulation, review the available therapeutic options, assessing the evidence base for each and offering guidance as to patient-specific factors that can influence this choice.
Keywords
Introduction
Atrial fibrillation (AF) is the most prevalent sustained cardiac arrhythmia. The prevalence of AF is higher in developed countries, with an estimated prevalence of approximately 3% in adults aged 20 years and over.1–3 The prevalence of AF increases with age. 2 AF is an established independent risk factor for ischaemic stroke and as such, is a significant cause of morbidity and mortality. 4 It confers a five-fold increase in the risk of ischaemic stroke and is thought to be responsible for 15–20% of all strokes.5,6 Oral anticoagulation (OAC) therapy reduces the risk of ischaemic stroke in patients with AF who have an additional stroke risk factor. 7 Traditionally, anticoagulation has been achieved through the use of vitamin K antagonists (VKAs), such as warfarin. Recent advances in the field have seen the introduction of the non-vitamin K antagonist oral anticoagulants (NOACs), also termed novel oral anticoagulants, as an alternative to VKAs, thereby broadening the armamentarium available to physicians for stroke prevention in AF.
Which patients with atrial fibrillation require anticoagulation?
AF increases the risk of stroke and systemic embolism. The extent of this risk is incrementally related to the presence of additional risk factors, including previous stroke or systemic embolism, heart failure (irrespective of ejection fraction), hypertension, advanced age, diabetes mellitus, concomitant vascular disease and female sex. 8 OAC therapy can prevent the majority of ischaemic strokes in patients with AF and as such, can be a life-saving intervention. 9 The overall clinical benefit of OAC is significant in all patient demographics with AF except those with a very low stroke risk-factor profile. 7 Current guidance advocates the use of stroke risk stratification methodology to guide whether patients should be anticoagulated or not. The CHA2DS2-VASc scoring system (Table 1) assesses for stroke risk factors in patients with AF. The CHA2DS2-VASc scoring system was first introduced in 2010 and has subsequently been integrated into national guidelines across the world including the European Society of Cardiology (ESC) and American Heart Association (AHA)/American College of Cardiology (ACC)/Heart Rhythm Society (HRS) guidelines.7,10 Current guidance advocates anticoagulation should be considered for any patient with AF with at least one single additional risk factor for ischaemic stroke; in real terms, this means a CHA2DS2-VASc score of 1 or more for men or 2 or more for women.7,11,12 The CHA2DS2-VASc scoring system has better discriminating power compared with the CHADS2 scoring system, a preceding simplified stratification system, in identifying low-risk patients who may still benefit from anticoagulation. 13 The HAS-BLED scoring system (Table 2) offers a method for estimating the risk of bleeding on OAC, 14 yet where possible, OAC should not be withheld on account of higher HAS-BLED scores, unless there is deemed an unacceptably high risk of bleeding. 7 Treatable bleeding risk factors identified in HAS-BLED assessment should be treated. There is now evidence that percutaneous left-atrial appendage closure is non-inferior to warfarin for stroke prevention in patients with AF and therefore should be considered as an alternative to OAC therapy in patients in whom anticoagulation is contraindicated due to unacceptable bleeding risk. 15 In spite of the well-established association of AF with ischaemic stroke, registry-based and observational real-world data consistently demonstrate underuse of OAC therapy in patients with AF in whom it is indicated. 16
CHA2DS2-VASc scoring system [congestive heart failure, hypertension, age ⩾ 75 (doubled), diabetes, stroke (doubled), vascular disease, age 65–74, sex (female)].

HAS-BLED scoring system.
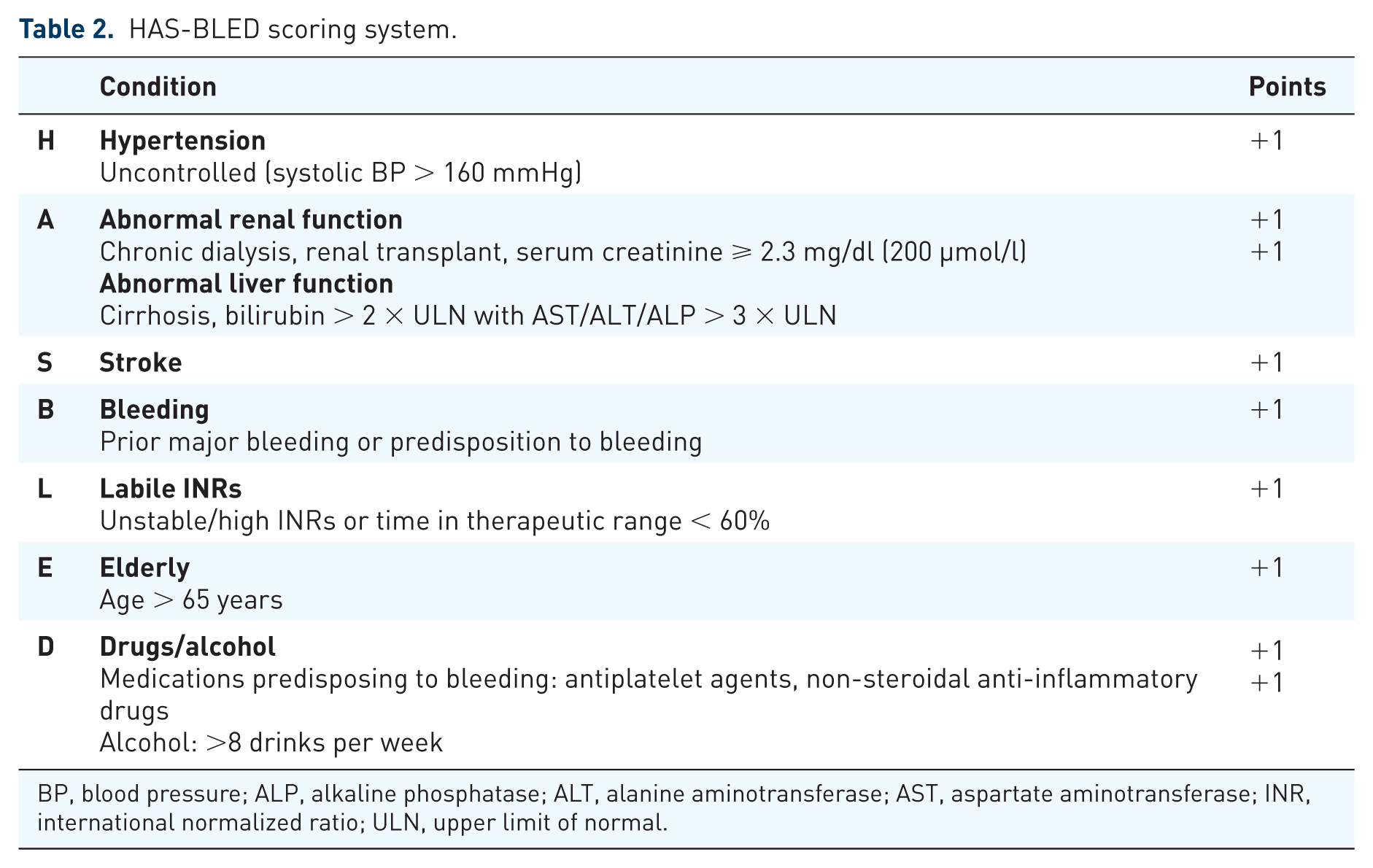
BP, blood pressure; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; INR, international normalized ratio; ULN, upper limit of normal.
Therapeutic options for anticoagulation in atrial fibrillation
The current options for anticoagulation fall into two broad categories. The first category is VKAs, the most commonly used of which is warfarin. The second category is NOACs, of which there are currently four drugs licensed for use for anticoagulation in AF: dabigatran, rivaroxaban, apixaban and edoxaban. Aspirin is not effective for use in stroke prevention in patients with AF and in fact, may increase the risk of stroke in elderly patients, so it is therefore no longer recommended for this purpose. 17
Vitamin K antagonists
Warfarin has been used as an OAC since 1954. 18 Meta-analysis has demonstrated a reduction in stroke of two-thirds in patients with AF who are anticoagulated with warfarin and a reduction in mortality by one quarter compared with control subjects treated with aspirin or placebo. 9 As such, it had become the cornerstone of anticoagulation in AF and was the only therapeutic option until the advent of NOACs.
There are, however, a number of well-described limitations to warfarin use. Warfarin has a slow onset of action. Additionally, the therapeutic window is narrow, necessitating blood monitoring and dose adjustments, which can lead to reduced time in therapeutic range (TTR) and can be cumbersome for patients. Drug interactions are relatively commonplace with warfarin and can compromise efficacy. Additionally, dietary interactions with warfarin can necessitate dietary restrictions.
In spite of these limitations, many patients with AF are long established on VKAs with stable therapeutic monitoring and drug dosing. Where patients sustain a TTR over 70%, VKAs remain an acceptable, effective and safe modality for anticoagulation; regular monitoring should be undertaken to ensure that the TTR remains over 70%. 19 The SAMe-TT2R2 (Table 3) scoring system has been proposed as a method for predicting which patients will achieve acceptable TTR and therefore achieve satisfactory protection against ischaemic stroke from VKA therapy. SAMe-TT2R2 scores 0–1 are associated with good INR control with satisfactory TTR, whereas a score of 2 or greater indicates patients are less likely to achieve satisfactory TTR. 20
SAMe-TT2R2 Score.

There are a number of circumstances in which VKAs are a preferred choice over NOACs for anticoagulation. These include: patients with so-called ‘valvular’ AF, and patients with AF and severe renal impairment.
Valvular AF is a contentious term, with a degree of heterogeneity relating to its precise definition.21,22 The concept of ‘valvular’ versus ‘non-valvular’ AF has been borne of studies identifying a higher risk of stroke in patients with AF and concomitant mitral stenosis or a mechanical prosthetic heart valve. It is hypothesized that there is a different mechanism of thrombus formation in patients with AF and mitral stenosis or mechanical prosthetic heart valves. 22 A study evaluating the efficacy of dabigatran in stroke prevention in patients with mechanical valve replacements versus warfarin was terminated early due to excess thromboembolic and bleeding events in the dabigatran arm. 23 Not all patients in this study had confirmed AF, however it provides evidence that in patients with mechanical valve prostheses, anticoagulation with warfarin is more effective and safer than anticoagulation with a NOAC. There remains a lack of uniformity over the accepted definition of ‘valvular AF’ issued in international guidance. The 2016 ESC guidelines recognize the historic classification of ‘valvular AF’ as relating to patients with coexisting rheumatic valvular disease (predominantly mitral stenosis) or mechanical heart valves, and advocates VKAs as the only safe OAC treatment for these patients. 7 The AHA/ACC/HRS guidelines describe ‘non-valvular’ AF as cases in which the rhythm disturbance occurs in the absence of rheumatic mitral valve disease, a prosthetic heart valve or mitral valve repair. 10
The recent pivotal phase III trials investigated the efficacy of NOACs in stroke prevention specifically in patients with ‘non-valvular’ AF, yet the exclusion criteria for patients deemed to have significant valvular disease differed significantly between trials. In the RE-LY trial, which assessed the efficacy of dabigatran versus warfarin for stroke prevention in AF, patients with prosthetic valves or ‘haemodynamically relevant’ valve disease were excluded, leading to the exclusion of patients with AF and other valvular lesions such as severe mitral regurgitation or severe aortic valve disease.24,25 By contrast, the other three phase III NOAC trials only excluded patients with moderate-to-severe mitral stenosis and mechanical prosthetic heart valves.26–30 Therefore, although the pivotal NOAC trials varied in their exclusion criteria for patients with valvular disease, all trials excluded patients with moderate or severe mitral stenosis and patients with mechanical prosthetic valves. NOACs are therefore not validated for use in patients with moderate or severe mitral stenosis or mechanical prosthetic valves, and VKAs are the anticoagulant of choice. 7
The next important circumstance in which VKAs are the recommended choice of anticoagulation is in patients with AF and severe renal impairment. Chronic kidney disease (CKD) is associated with increased risk of ischaemic stroke or systemic embolism in patients with AF compared with patients with AF and normal renal function. 31 VKAs can be used in all patients with CKD, including patients requiring renal replacement therapy. 32 This relates to the fact that there is minimal renal elimination of the bioavailable drug with VKAs. NOACs, in contrast, have a higher proportion of renal elimination: 80% for dabigatran, 50% for edoxaban, 33% for rivaroxaban and 27% for apixaban. 33 Thus, patients with CKD treated with NOACs are at risk of higher plasma drug concentrations due to reduced drug elimination. 34 The pivotal phase III trials investigating NOACs for stroke prevention in AF excluded patients with advanced CKD and at present, therefore, there is no validated outcome data for the use of NOACs in patients with a creatinine clearance of less than 30 ml/min, including patients on haemodialysis. VKAs are therefore the anticoagulant of choice in this patient group. In patients with CKD who have a creatinine clearance greater than 30 ml/min, NOACs can be used with dose reductions. 33 Apixaban and rivaroxaban are currently licensed for use in patients with creatinine clearance as low as 15 ml/min with dose reduction, however, the use of these drugs in patients with creatinine clearance between 15 and 30 ml/min is not backed up by phase III trial data.
Non-vitamin K antagonist oral anticoagulants
Four NOACs are currently licensed for stroke prevention in patients with AF. These include the direct thrombin inhibitor dabigatran and the factor Xa inhibitors rivaroxaban, apixaban and edoxaban. The advantages of NOACs include predictable pharmacokinetics, with rapid onset and offset of action. There is no need for therapeutic monitoring and dose adjustments, as is the case with VKAs. There are no dietary interactions, but there are some clinically relevant drug interactions. 8 The pivotal NOAC trials have demonstrated that NOACs are at least as effective as warfarin in the prevention of stroke or systemic embolism in patients with non-valvular AF. Consequently, the most recent ESC guidelines on AF recommend use of a NOAC over a VKA in patients who are to be newly initiated on OAC therapy, provided there are no contraindications to NOAC therapy. 7 The key findings of the pivotal trials comparing NOACs against warfarin for stroke prevention are summarized in Table 4.7,25,26,28,30,34 Patients on VKAs with poor TTR control in spite of drug adherence may be considered for a switch to a NOAC provided there is no contra-indication. Patients on warfarin may also be considered for a switch to a NOAC due to patient preference. 7
Summary of the pivotal trials assessing non-vitamin K antagonist oral anticoagulant versus warfarin in patients with non-valvular atrial fibrillation.

TTR, time in therapeutic range; CI, confidence interval.
Dabigatran
Dabigatran was the first NOAC to be licensed for use in stroke prevention for non-valvular AF. In contrast to the other pivotal NOAC trials, the RE-LY (Randomized Evaluation of Long-term anticoagulation therapY) study was an open-label trial. Patients were randomized to dose-adjusted warfarin or blinded doses of dabigatran (150 mg twice daily or 110 mg twice daily). The mean CHADS2 score of patients was 2.1.
The 150 mg twice-daily dabigatran dose was superior to warfarin in reducing stroke or system embolism [risk reduction (RR) 0.66; 95% confidence interval (CI) 0.53–0.82; p < 0.001]; this was due to both a significant reduction in ischaemic stroke (RR 0.76; 95% CI 0.60–0.98; p = 0.03) and in haemorrhagic stroke (RR 0.26; 95% CI 0.14–0.49; p < 0.001). There were fewer intracranial haemorrhages (RR 0.40; 95% CI 0.27–0.60; p < 0.001), a higher rate of gastrointestinal bleeds (RR 1.50; 95% CI 1.19–1.89; p < 0.001) but overall, no difference in major bleeding events (RR 0.93; 95% CI 0.81–1.07; p = 0.31) in the 150 mg twice-daily dosing compared with warfarin.
The 110 mg twice-daily dabigatran dose was non-inferior to warfarin for prevention of stroke or systemic embolism (RR 0.91; 95% CI 0.74–1.11; p < 0.001). There was a significantly lower rate of haemorrhagic strokes (RR 0.31; 95% CI 0.17–0.56; p < 0.001) with no significant reduction in ischaemic strokes (RR 1.10; 95% CI 0.89–1.40; p = 0.35) compared with warfarin. The dabigatran 110 mg twice-daily group demonstrated favourable bleeding outcomes with fewer intracranial haemorrhages (RR 0.31; 95% CI 0.20–0.47; p < 0.001), no observed difference in the rate of gastrointestinal bleeding (RR 1.10; 95% CI 0.86–1.41) and overall, a lower risk of major bleeding (RR 0.80; 95% CI 0.69–0.93; p = 0.003) compared with warfarin. 25
Rivaroxaban
ROCKET-AF (Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation) was a randomized, double-blinded trial that assigned patients to receive rivaroxaban 20 mg once daily or dose-adjusted warfarin. The mean CHADS2 score of patients was 3.5. Rivaroxaban was non-inferior to dose-adjusted warfarin for prevention of stroke or systemic embolism in the intention-to-treat analysis [hazard ratio (HR) 0.88; 95% CI 0.75–1.03; p < 0.001]. In the per protocol on treatment analysis, rivaroxaban achieved statistical superiority over dose-adjusted warfarin in reducing stroke or systemic embolism (HR 0.79; 95% CI 0.66–0.96; p = 0.01). There was no significant difference in ischaemic stroke in patients treated with rivaroxaban compared with warfarin (HR 0.94; 95% CI; 0.75–1.17; p = 0.581). A significant reduction in haemorrhagic stroke (HR 0.59; 95% CI 0.37–0.93; p = 0.024) and intracranial bleeds (HR 0.67; 95% CI 0.47–0.93; p = 0.02) was observed with rivaroxaban compared with warfarin. There was an increase in gastrointestinal bleeding events (HR 1.61; 95% CI 1.30–1.99; p < 0.001) with rivaroxaban compared with warfarin, but no significant difference in the rate of major bleeding events (HR 1.04; 95% CI 0.90–1.20; p = 0.58). 26
The European Medicines Agency (EMA) subsequently released an assessment report voicing concerns over the accuracy of the point of care (POC) INR readings in the warfarin arm of the ROCKET-AF trial; however, further post hoc analysis has refuted the significance of this and demonstrated results consistent with the overall original outcomes of the trial.35,36
Apixaban
The ARISTOTLE (Apixaban for Reduction In STroke and Other ThromboemboLic Events in atrial fibrillation) trial was a randomized, double-blinded trial that compared apixaban 5 mg twice daily with dose-adjusted warfarin. The mean CHADS2 score was 2.1. Apixaban was superior to warfarin in preventing stroke or systemic embolism (HR 0.79; 95% CI 0.66–0.95; p = 0.01). The rate of haemorrhagic stroke was lower with apixaban compared with warfarin (HR 0.51; 95% CI 0.35–0.75; p < 0.001) and again, there was no significant reduction in ischaemic strokes between groups (HR 0.92; 95% CI 0.74–1.13; p = 0.42). Intracranial bleed rates were lower with apixaban compared with warfarin (HR 0.42; 95% CI 0.30–0.58; p < 0.001). There were less major bleeds in the apixaban group compared with the warfarin group (HR 0.69; 95% CI 0.60–0.80; p < 0.001) and the number of gastrointestinal bleeds between the two groups was comparable (HR 0.89; 95% CI 0.70–1.15; p = 0.37). The rate of death from any cause was lower in the apixaban group than the warfarin group (HR 0.89; 95% CI 0.8–0.99; p = 0.047). 28
Edoxaban
The ENGAGE AF-TIMI 48 (effective Anticoagulation with Factor Xa Next Generation in Atrial Fibrillation-Thrombolysis in Myocardial Infarction 48) trial was a randomized, double-blinded trial assessing two doses of edoxaban (30 mg once daily and 60 mg once daily) against dose-adjusted warfarin. The mean CHADS2 score was 2.8.
High-dose edoxaban (60 mg once daily) was non-inferior to warfarin in reducing stroke and systemic embolism (HR 0.87; 95% CI 0.73–1.04; p < 0.001), with comparable rates of ischaemic strokes with the warfarin group (HR 1.00; CI 0.83–1.19; p = 0.97) and a reduction in haemorrhagic stroke (HR 0.54; 95% CI 0.38–0.77; p < 0.001). In addition, there was a reduction in intracranial haemorrhage (HR 0.47; 95% CI 0.34–0.63; p < 0.001) and a reduction in major bleeds (HR 0.80; 95% CI 0.71–0.91; p < 0.001) but a higher rate of gastrointestinal bleeds (HR 1.23; 95% CI 1.02–1.50; p = 0.03) in the high dose edoxaban group compared with the warfarin group. 30
Low dose edoxaban (30 mg once daily) demonstrated non-inferiority versus warfarin in reducing stroke and systemic embolism (HR 1.13; 95% CI 0.96–1.34; p = 0.005), with reduced haemorrhagic strokes (HR 0.33; 95% CI 0.22–0.50; p < 0.001), but a higher rate of ischaemic strokes (HR 1.41; 95% CI 1.19–1.67; p < 0.001) compared with warfarin. Low-dose edoxaban also demonstrated favourable bleeding outcomes, with an observed reduction in intracranial bleeding rates (HR 0.30; 95% CI 0.21–0.43; p < 0.001), a reduction in major bleeds (HR 0.47; 95% CI 0.41–0.55, p < 0.001) and a reduction in gastrointestinal bleeds (HR 0.67; 95% CI 0.53–0.83; p < 0.001) compared with the warfarin group. In view of the higher rates of ischaemic stroke, edoxaban 30 mg once daily is only recommended for patients with body weight less than 60 kilograms, impaired renal function or concomitant use of P-glycoprotein inhibitors ciclosporin, dronedarone, erythromycin or ketoconazole as these can result in higher plasma drug concentrations.30,37
Meta-analysis of pivotal NOAC trials
Meta-analysis of the four pivotal phase III clinical trials assessing anticoagulation with NOACs versus warfarin in non-valvular AF demonstrated a significant reduction in stroke and systemic embolism with NOACs (RR 0.81; 95% CI 0.73–0.91; p < 0.0001). This was principally driven by a reduction in haemorrhagic stroke (RR 0.49; 95% CI 0.38–0.64; p < 0.0001) with comparable rates of ischaemic stroke observed between groups. There was reduced intracranial haemorrhage with NOACs (RR 0.48; 95% CI 0.39–0.59; p < 0.0001), higher rates of gastrointestinal bleeding (RR 1.25; 95% CI 1.01–1.55; p = 0.04) and overall, no significant difference in major bleeding rates between groups (RR 0.86; 95% CI 0.73–1.00; p = 0.06). There was reduced all-cause mortality (RR 0.90; 95% CI 0.85–0.95; p = 0.0003) with NOACs. This meta-analysis found the reduction in stroke and systemic embolism with NOACs to be consistent across all individual patient subgroups when patient-specific factors were taken into account. There was a greater relative reduction in major bleeds observed with NOACs when compared with warfarin when the TTR was less than 66% than in centers where the TTR was greater than 66%. 39
Separate analysis of the lower-dose NOAC regimes (dabigatran 110 mg twice daily and edoxaban 30 mg once daily) demonstrated that although the overall rates of stroke and systemic embolism are comparable with warfarin (RR 1.03; 95% CI 0.84–1.27; p = 0.74), this is largely made up of a large reduction in haemorrhagic stroke and in fact, the lower-dose regimes have a higher rate of ischaemic stroke than warfarin (RR 1.28; 95% CI 1.02–1.60; p = 0.045). The lower-dose NOAC regimes do, however, offer a safer bleeding profile (RR 0.65; 95% CI 0.43–1.00; p = 0.05). 39
Which NOAC for which patient?
Many of the outcomes of the pivotal phase III NOAC trials were comparable. There are no direct head-to-head comparator trials for the NOACs against one another to facilitate a direct comparative evaluation between agents. Additionally, there are differences in the study populations of each of the pivotal NOAC trials. These factors make deciding between NOACs a challenge in patients with AF once a decision has been made to treat with a NOAC over a VKA. There is no significant evidence base to preference one NOAC over another and consequently, no recognized guidelines on how to choose one over another. Further studies into this are indicated but ultimately may not be feasible. In the absence of this, one can assess the individual evidence and outcomes from each of the pivotal NOAC trials and apply this to individual patient-specific circumstances. Without direct comparative evaluation between agents, this strategy is the next-best alternative. The following patient-specific considerations are summarized in Figure 1.
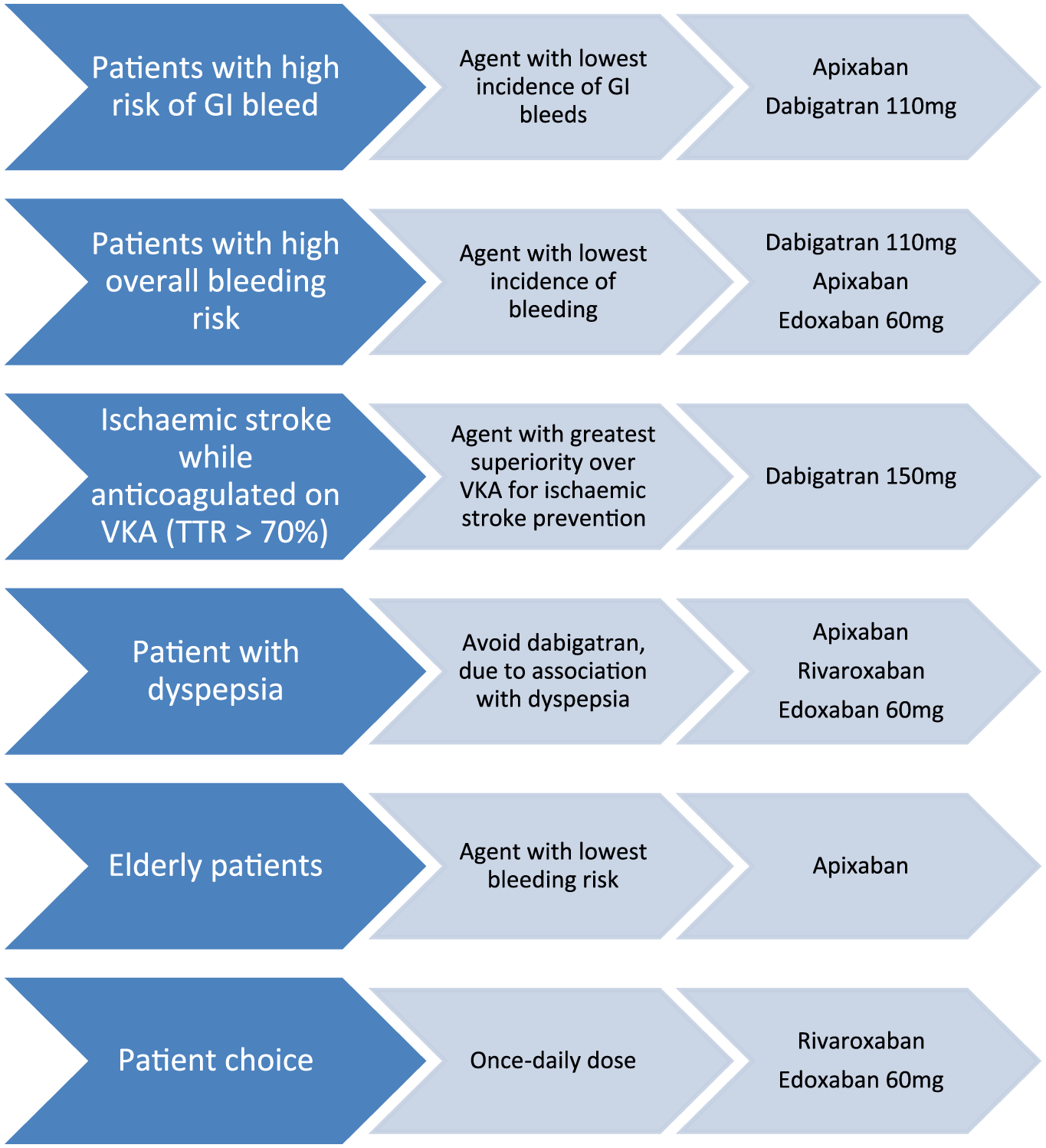
Patient-specific considerations applied to outcomes from the pivotal phase III non-vitamin K antagonist oral anticoagulant trials.
In patients with a high risk of gastrointestinal bleeding, the logical choice of NOAC would be to choose the agent with a lower rate of gastrointestinal bleeding reported in the pivotal phase III trials. Apixaban and dabigatran 110 mg twice daily had comparable rates of gastrointestinal bleeding with warfarin. These two agents should therefore be considered in such a patient group. The other NOACs all demonstrated a higher rate of GI bleeding compared with warfarin in the pivotal trials.8,34
In patients with a high overall risk of bleeding on OAC therapy, for example, patients with a HAS-BLED score ⩾ 3, it would be appropriate to choose an agent with a lower overall risk of major bleeding. As such, dabigatran 110 mg twice daily, apixaban and edoxaban 60 mg once daily would be suitable choices, as these agents demonstrated significantly lower rates of major bleeding compared with warfarin in the pivotal NOAC trials while all providing protection against stroke that is at least as effective as warfarin.8,34
Meta-analysis of the RE-LY, ROCKET-AF and ARISTOTLE trials, assessing specifically patients suffering stroke, systemic embolism or transient ischaemic attack while already anticoagulated demonstrated superiority of NOACs compared with warfarin. Of note, in the analysis, the TTR was on average <70%. Therefore, patients undergoing secondary stroke, systemic embolism or transient ischaemic attack while anticoagulated with a VKA with suboptimal TTR are likely to benefit from a switch to a NOAC.33,39 In patients with a recurrent stroke, systemic embolism or transient ischaemic attack while on warfarin, in spite of effective anticoagulation control (TTR > 70%), a switch to dabigatran 150 mg twice daily might be considered, as this dose demonstrated marked superiority (RR 0.65; 95% CI 0.52–0.81; p < 0.001 for superiority) over warfarin for prevention of stroke and systemic embolism in the RE-LY trial.8,34 This benefit in stroke prevention with dabigatran 150 mg twice daily comes at the cost of a higher risk of gastrointestinal bleeding, which must be factored into the decision-making process.
Dabigatran has documented gastrointestinal side effects, including dyspepsia. Subgroup analysis of the RE-LY trial demonstrated that dabigatran was inferior to warfarin with regard to gastrointestinal side-effects. One in ten patients prescribed dabigatran developed dyspepsia, which was a major cause of noncompliance and drug discontinuation. 25 One study has subsequently found that dyspepsia is responsible for 30% of cases in which dabigatran has been discontinued. 40 Thus, if a patient requires anticoagulation for non-valvular AF and already suffers with dyspepsia, another NOAC agent which does not have this side-effect profile is likely preferable.
NOACs are frequently indicated in the elderly population due to the increase in incidence of AF with advanced age. Subgroup analysis of the pivotal phase III NOAC trials confirmed a higher incidence of bleeding on OAC therapy in older subjects (>75 years) compared with younger subjects. Only apixaban had a significantly lower rate of significant bleeds in older subjects compared with warfarin. In the other pivotal NOAC trials, the treatment with a NOAC conferred a comparable or higher rate of significant bleeds amongst elderly patients compared with warfarin. This favourable bleeding profile of apixaban may in part be due to the recommendation to dose reduce to 2.5 mg twice daily if two of the following criteria are met: age ⩾ 80 years, weight ⩽ 60 kg and creatinine ⩾ 1.5 mg/dl (133 µmol). Apixaban may therefore be a preferable agent for use in the elderly in view of its favourable safety outcomes in this age group in terms of minimizing significant bleeding.33,41,42
Patients may express a wish to keep their pill burden to a minimum and therefore may wish to have a taken-once-daily NOAC regime. In such cases, clearly rivaroxaban and both doses of edoxaban are the available NOAC options. Edoxaban 60 mg once daily, however, has the advantage of superior protection against ischaemic stroke over the 30 mg once-daily regime.
NOAC use with antiplatelet therapy
An area of much research focus has been on the concomitant use of NOACs with antiplatelet drugs in patients undergoing percutaneous coronary intervention (PCI) with AF. Standard therapy in patients without an indication for anticoagulation necessitates a period of dual antiplatelet therapy, followed by long-term single-antiplatelet monotherapy. In patients with AF, there is an indication for a period of ‘triple therapy’ with an anticoagulant and dual-antiplatelet therapy, however, this is associated with higher bleeding risks. The exact role of NOACs in this patient subgroup is evolving. The PIONEER AF-PCI trial has recently indicated that there may be a role for low-dose rivaroxaban (15 mg daily) plus a P2Y12 inhibitor for 12 months or alternatively very-low-dose rivaroxaban (2.5 mg twice daily) plus a period of dual-antiplatelet therapy for 1, 6 or 12 months, as these treatment regimens were associated with lower rates of significant bleeds and comparable rates of cardiovascular events (cardiovascular mortality, myocardial infarction and stroke) compared with standard therapy with VKA plus dual-antiplatelet therapy for 1, 6 or 12 months. 43 Trials evaluating the other NOACs (dabigatran, edoxaban and apixaban) in this capacity are ongoing and will soon be reported.
Reversal agents
One initial advantage of VKAs over NOACs was the ready availability of reversal agents in the event of major bleeding complications. Recent advances have seen the approval of idarucizumab, a humanized monoclonal antibody fragment, which binds and is an effective reversal agent for dabigatran. 44 At present, there are no licensed reversal agents for the factor Xa inhibitors. Andexanet is a recombinant factor Xa protein currently under investigation for use as a potential reversal agent, however, its clinical efficacy and safety is as yet unproven.45,46 Of significance, is the proportionally shorter half-lives of NOACs compared with VKAs, meaning the requirement for reversal is likely to be less with NOACs than with VKAs.
Conclusion
AF is a major cause of stroke. In patients with AF and at least one additional risk factor, OAC is indicated and is effective in reducing the risk of ischaemic stroke. OAC can be achieved either with VKA or NOAC therapy. VKAs are indicated in patients with AF and a mechanical valve prosthesis or moderate-to-severe mitral stenosis, or in patients with severe renal impairment. NOACs are at least as effective as VKAs in the prevention of stroke and systemic embolism in patients with non-valvular AF, in whom there are no contraindications. There are no head-to-head comparator trials for NOACs, however, assessment of the clinical outcomes of the pivotal phase III NOAC clinical trials, in conjunction with consideration of individual patient-specific factors can help to guide the choice of NOACs in patients with non-valvular AF.
Footnotes
Conflict of interest statement
DH has received meeting sponsorship from Bayer, Pfizer and Boehringer. MS has received educational and meeting sponsorship, lecturing and advisory boards for Bayer, Pfizer and Boehringer.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.