
Abstract
During the last 30 years, deep brain stimulation (DBS) has evolved into the clinical standard of care as a highly effective treatment for advanced Parkinson’s disease. Careful patient selection, an individualized anatomical target localization and meticulous evaluation of stimulation parameters for chronic DBS are crucial requirements to achieve optimal results. Current hardware-related advances allow for a more focused, individualized stimulation and hence may help to achieve optimal clinical results. However, current advances also increase the degrees of freedom for DBS programming and therefore challenge the skills of healthcare providers. This review gives an overview of the clinical effects of DBS, the criteria for patient, target, and device selection, and finally, offers strategies for a structured programming approach.
Introduction
Parkinson’s disease (PD) is a common neurodegenerative disease, which affects about 1% of the population older than 65 years. 1 It comprises two major neuropathologic findings: the loss of dopaminergic cells of the ventrolateral compartment of the substantia nigra and the presence of Lewy bodies, at least in the brain stem, but with progressive cerebral distribution in the course of the disease. 2
Despite the complexity of symptoms in PD, which comprise cognitive and affective dysfunction, as well as sensory and vegetative disturbances, the impairment of motor control (i.e. Parkinsonian syndrome) is still considered as a main clinical feature to make the diagnose. As such, Parkinsonian syndrome is clinically defined as the presence of bradykinesia in addition to other cardinal symptoms like rigidity, rest tremor, or postural instability. The progressive loss of dopaminergic neurons may be partially compensated by dopaminergic substitutive therapy and hence allow for symptom control, especially for motor symptoms. However, medical treatment becomes challenging in the course of the disease due to the development of motor fluctuations, the presence of therapy refractory motor symptoms, or the adverse effects of medical treatment.
Even before the establishment of dopaminergic treatment regimens for PD, neurosurgical procedures of basal ganglia have been considered to treat PD motor symptoms. 3 Because of complication rates, especially with bilateral procedures, pharmacological advances in terms of the availability of levodopa as an effective drug for PD almost completely replaced surgical treatment. 4 While improvement of PD tremor using high frequency thalamic stimulation was already described in 1963, Irvine Cooper was the first who utilized chronic deep brain stimulation (DBS) for sustained tremor control. Finally, the work of Benabid and colleagues paved the way for DBS for worldwide applications (initially in clinical studies and later in clinical routine) and hence revitalized the application of neurosurgical procedures more than 30 years ago. 5 Following encouraging experiences with thalamic DBS, the insights of basal ganglia involvement in the pathophysiology of PD, DBS of the subthalamic nucleus (STN) in particular but also the globus pallidus internus (GPI) was suggested and eventually successfully applied as targets for DBS.6,7 In contrast to lesioning techniques of pallidofugal fibers or thalamic areas, advantages of DBS are adaptability, reversibility, less tissue damage, and the option to perform bilateral surgery without a significant increase of adverse effects.
Nowadays, DBS has turned into one of the most successful treatment strategies in advanced stages of the disease. In recent years, cutting-edge features of both the implantable pulse generators (IPGs) and the DBS electrodes have been introduced, which increase the degrees of freedom to customize DBS settings and hence optimize the efficacy of treatment. This review summarizes the procedural standards in DBS for PD and how to optimally utilize recent technical advances in clinical practice.
Current state (STN DBS)
Indications and patient selection
Among different available targets, the STN is predominantly selected in the clinical standard of PD care, even though comparative analyses do not indicate superiority towards the second most common target, the GPI. However, since scientific literature describing observations of DBS in PD is clearly dominated by the STN as the chosen target, this update mainly addresses clinical practice for STN DBS.
Careful selection of applicable patients is one of the hallmarks in avoiding the risk of unsatisfactory outcome following DBS surgery. As such, only patients suffering from PD, but not secondary or atypical Parkinsonian syndromes, are candidates for DBS surgery. PD itself predominantly comprises sporadic/idiopathic forms, which are most likely caused by polygenic and environmental factors, but also monogenic forms of PD, which are estimated to represent <10% of PD cases. 8 While current data do not allow for robust statements about the efficacy in single monogenic forms of PD, studies with small patient sizes on monogenic PD patients reported good responses to DBS and a considerable percentage of PD patients who undergo DBS may incidentally suffer from monogenic forms of PD anyway. 9 We propose that while clinical hallmarks such as rather aggressive disease progression in patients with GBA gene mutations should kept in mind, patients with (known) monogenic forms of PD may be considered as candidates for DBS, similar to patients suffering from idiopathic PD.
Current German guidelines recommend that the following criteria are mandatory to consider DBS in PD: (a) presence of motor fluctuations including levodopa-sensitive off symptoms or treatment-induced dyskinesia; (b) tremor, which cannot be satisfactorily treated with medication; (c) a levodopa-induced reduction of motor symptoms by >33% of the Unified Parkinson Disease Rating Scale (UPDRS), where tremor may be disregarded from the calculation as it may be refractory to levodopa treatment while still responding well to DBS; and (d) exclusion of dementia, relevant psychiatric or somatic comorbidity, or general contraindication to undergo neurosurgical interventions. 10 Even more restrictive inclusion criteria are recommended for patients not older than 60 years and the presence of motor fluctuations for not longer than 3 years. 10
However, clinicians have to keep in mind that such a restrictive selection of DBS candidates may be problematic, as discussed in the following: excellent response to dopaminergic treatment, a lower degree of levodopa-refractory symptoms, and a younger age increase the likelihood of highly efficacious DBS treatment. 11 As such, a levodopa-induced reduction of motor symptoms by >30% of the UPDRS motor score has been suggested as criterion to identify optimal candidates for surgery. 12 Recent studies however, question the value of initial degree of levodopa response to predict a sustained DBS improvement on motor symptoms or quality of life (QOL) measurements.13,14
Several studies indicated that a high biological age is associated with less efficacy 15 and a reduced QOL improvement 16 following DBS surgery. Additionally, an increased intraoperative risk has been controversially discussed.17,18 However, age was not identified to be an independent factor to influence motor improvement in randomized controlled trials, 19 and the risk of surgical complications is rather increased by comorbidities, for which age is a surrogate. 20 So far, there is no established threshold as to whether elderly patients are candidates for DBS.
Severe comorbidities which do not allow patients to undergo DBS surgery as well as relevant psychiatric conditions, such as acute psychosis, major depression, or dementia, are generally considered as exclusion criteria. 10 With regard to dementia, surgery may be associated with an increased risk to safely seed the electrodes (due to cerebral atrophy) and postoperative delirium, including persistent deterioration of cognitive and psychological functionality. Hence, current guidelines state that DBS surgery in patients with dementia is contraindicated. 10 Additionally, PD dementia frequently manifests at an advanced stage of disease, which is often accompanied by axial symptoms that predominantly contribute to the burden of the disease but may be refractory to DBS. However, DBS has been shown to be efficacious in patients with mild cognitive impairment, 21 and established screening parameters such as the Mattis Dementia Rating Scale alone may not be suitable to predict QOL or motor outcomes after DBS, 22 even if cognitive scales were below the threshold for dementia. Therefore, both a careful medical and extensive neuropsychological evaluation not exclusively relying on screening tests is mandatory before the final decision of applicability for DBS.
Finally, structural magnetic resonance imaging (MRI) of the brain is needed for precise planning of a safe trajectory of the DBS electrodes. Additionally, it allows the ruling out of cerebral conditions associated with an increased risk during brain surgery, such as relevant atrophy, or highly vascularized structures.
As outlined above, clinical criteria suggested for identification of DBS candidates cannot precisely predict the outcome of DBS. As a consequence, there cannot be a dichotomous criterion for a clinician to either recommend or deny DBS surgery. Hence, such recommendations for patient selection may rather provide a guide for patient selection but cannot be regarded as strict cutoff parameters. Furthermore, clinical outcomes can be assessed as measurable scales and values in clinical studies for statistical analyses. But from an individual patient’s perspective, the outcome of DBS surgery may be perceived as beneficial even if objective evaluation would reveal just a very mild response.
Therefore, patients and healthcare providers together should discuss on an individual basis, what patients expect from DBS and if presumable benefits outweigh the risks of DBS surgery. Finally, shared decision-making with the patient is warranted, since only the patient or the legal guardian can know, which benefit–risk ratio is acceptable for them to undergo such a procedure.
Time of surgery
Traditionally DBS is offered to PD patients with severe and medication refractory on–off motor fluctuations, dyskinesia, or tremor. As a consequence, patients who underwent DBS surgery in the first years of application in the clinical standard of care were characterized by long disease durations. For these advanced stages of the disease, several randomized studies showed an advantage of DBS compared with best medical treatment alone.23,24 However, very late stages of PD are often accompanied by axial motor symptoms and nonmotor symptoms like cognitive decline, which may not benefit from DBS and potentially even impede the overall improvement from DBS treatment. As such, improvement of appendicular motor symptoms does not necessarily result in a return of independency. 25
Based on these insights, the efficacy of STN DBS treatment in PD patients suffering from early motor fluctuations and hence a less advanced stage of the disease was compared with the best medical treatment in the EARLYSTIM study. 26 The results providing evidence for superiority of STN DBS eventually led to approval by the United States Food and Drug Administration (US FDA) for use in the early presence of motor fluctuations. Patients enrolled in the EARLYSTIM trial were relatively young (mean age 52 years) and had a short disease duration (7.3 years on average). 26 So how do age at surgery and disease duration contribute to beneficial results?
Age itself does not seem to be a predictor of outcome in terms of motor function, since similar improvement in that domain can be detected in both younger and older PD patients.23,26–28 However, age was identified to be a relevant factor to predict beneficial effects on QOL. Patients younger than 60 years showed a more pronounced improvement of QOL in a recent study by Dafsari and colleagues, where the relevant improvement of QOL as measured by the PD Questionnaire-8 was detected in 68% of patients younger than 60 years, as opposed to only 45% in patients with an age of at least 70 years. 28 Other studies revealed significant QOL improvement in younger (<65 years only) but not elderly patients. 16 These findings, even though conducted in a relatively small cohort, indicate that DBS surgery should be especially offered to younger patients as long as relevant motor fluctuations or therapy refractory tremors exist. While costs have been shown to increase by 32% in the first year after DBS surgery, they decrease by 54% by the second year and hence were concluded to be economically more efficient than medical treatment alone by the second year after surgery. 29
Disease duration may be regarded as an indicator for the stage of the disease. While the risk of a potential floor effect for patients with early motor fluctuations has been discussed, the results of the EARLYSTIM trial indicate that the relative rate of improvement in such patients is similar to DBS results in advanced stages of the disease, and even though the absolute improvement may be less (given the lower baseline severity), QOL still may dramatically improve by the treatment. 30 In line with these results, STN DBS with long and short disease duration was shown to improve QOL in patients with an age of more than 60 years in a small single-center study, 27 which indicates that early motor fluctuations can also be reliably improved by STN DBS in patients, which do not fulfill the demanding inclusion criteria of the EARLYSTIM trial, where patients older than 60 years were excluded. As opposed to STN DBS data on GPI DBS in PD patients with early motor fluctuations are lacking so far.
However, concerns about early DBS have been expressed in several regards: patients with early motor fluctuations have been claimed to have a lower benefit–risk ratio due to a lower absolute motor improvement, but similar risks of relevant adverse events compared with patients with advanced stages of the disease. 31 As such, the question has been raised whether it is possible to be ‘too early’ for DBS surgery. Early surgery bears the risk that patients with atypical Parkinsonian syndromes with some (but attenuating) response to dopaminergic treatment may accidentally be misdiagnosed as PD patients with early motor fluctuations. DBS surgery offered to those patients would lead to frustrating results. Additionally, any dramatic complications during surgery such as cerebral bleeding may have more relevant on quality-adjusted life years in younger patients. This especially applies for PD patients in the ‘honeymoon’ phase of treatment, when relevant refractory tremor or motor fluctuations as approved indications for DBS are not present. Studies of DBS in this particular patient population have been criticized because of ethical issues given the low but existent risks of DBS surgery, while there is no evidence for the disease-modifying effects of DBS, and hence no additional benefit towards best medical treatment. 32 In line with these considerations, a questionnaire-based study on a small population of PD patients suggests that there is a remarkable reluctance to undergo DBS surgery, assuming that there is more to lose than to gain from this treatment. 33 Additionally, the validity of the results obtained from the EARLYSTIM study has been questioned, particularly assuming that patients who participated in the study were motivated to undergo DBS surgery and hence might be exposed to placebo and ‘lessebo-like’ effects. 31
However, most of these concerns could be dispelled by Schüpbach and colleagues, so the authors concluded that patients with early motor fluctuations should be considered as candidates for DBS surgery as long as it can be justified from the signs and symptoms which considerably impact patients’ QOL and which can be expected to respond to DBS. 30
Surgical procedure and intraoperative management
DBS surgery is preferentially performed in a relative medication-off state. To facilitate the rapid adaption of therapy, the authors recommend withdrawal of long-acting dopaminergic agents and temporary replacement by levodopa and continuous administration of apomorphine prior to surgery. 34 At our center, levodopa is discontinued at least 12 h prior to surgery, similar to assessments of motor symptoms in the off state. Apomorphine in turn is continued until initiation of surgery. To prevent nausea and vomiting, domperidone (10 mg three times a day) should be considered one day before and during the first 2 days of using apomorphine. Any medication associated with an increased risk for cerebral hemorrhage must be discontinued appropriately.
As a prerequisite to define the target point and the trajectory for DBS electrode placement, the patient’s individual anatomy as provided by MRI of the brain has to be illustrated in stereotactic space. Such a scenario can be directly realized either by using frameless devices for DBS, or stereotactic frames which allow for the acquisition of MRI. Another option is the assessment of cranial computed tomography with attached stereotactic frame and its co-registration to previously performed cranial MRI. Up-to-date imaging techniques allow for the direct identification of STN or GPI as the main targets for DBS. The first estimation of the target point is generally based on stereotactic coordinates of well-established atlases. Indirect anatomical characteristics like the size of the third ventricle may be utilized for further refinement of the target point. Direct identification of target nuclei may be used for further refinement, despite heterogeneous data on its accuracy. 35
Following a skin incision and the drilling of a burr hole allowing the entrance to the planned trajectory, microelectrodes are inserted and either step-wise (steps 0.5–1 mm) or continuously forwarded along the planned pathway. Utilization of microelectrode recording (MER) may help identify target areas by distinct activity patterns, determined by spontaneous background firing, spike discharges, and changes of activity due to movement or sensory stimuli and therefore may increase the accuracy of the final electrode placement. 36 The same applies to intraoperative test stimulation. As such, relatively low thresholds for characteristic side effects, like tetanic contraction due to stimulation of the internal capsule, may help in estimating the proximity to adjacent anatomical areas, which mediate the side effects of DBS. In turn, low thresholds for beneficial effects without the development of side effects suggest a favorable position. Once the optimal target has been specified, the DBS electrode is eventually inserted. If the electrodes provide directional leads, an orientation marker positioned slightly proximal to the uppermost contact helps predefine the anatomical arrangement of the segmented contacts. In our experience, torsion effects may lead to a twist of the electrode within the first day after surgery, which may counteract any precise planning in advance. Following electrode implantation, the final DBS electrode location is confirmed by postoperative computed tomography (CT) or MRI scans.
The pros and cons of microelectrode recording for precise neuro navigation
It is an old debate whether (semi) MER increases the accuracy of the DBS lead placement. 37 MER may help identify anatomical targets via the detection of characteristic cellular firing patterns. 38 Experienced centers on MER report that an alternative trajectory is preferred over the initially predefined target in about 25% of cases, leading to more preferable motor outcomes. 39 Also, intraoperative test stimulation via microelectrodes may predict the risk of early capsular side effects at a given target and therefore may also enhance decision-making on the DBS electrode placement. 40 Consequently, MER is a useful technique to optimize placement of the final DBS electrode and routinely utilized in most DBS centers, including our own.
The hallmarks of MER are increased costs and duration of DBS surgery, 32 as well as an increased risk of cerebral hemorrhage, 41 or sustained neurological deterioration. 42 Consequently, the utility of MER may be questioned, especially since the availability of imaging technology like interventional MRI may nowadays facilitate a highly accurate placement of the DBS. 43 Similar to the described complication rates of DBS surgery in general, there is a distinct variability of described hemorrhage rates following MER, which may be dependent on the type of electrode used for recording, 44 and presumably the experience in its application. Indeed, well-applied MER can serve as a well-tolerated method, which does not lead to permanent histologically detectable lesions. 45 A recent study published by Bjerknes and colleagues suggests that MER utilizing multiple simultaneous microelectrodes leads to better outcomes, compared with the single sequential MER technique. 46 If MER is intended to be utilized during surgery, all trajectories have to be planned accurately in order to avoid penetration of structures which are associated with an increased risk of complications, such as the caudate nucleus (cognitive impairment), 47 or local blood vessels (cerebral hemorrhage). If these safety requirements are kept, the authors conclude that MER is a valuable method, especially if cutting-edge imaging techniques as alternatives to ensure optimal placement of the DBS lead cannot be easily implemented in the routine DBS surgery.
Perioperative protocols of anesthesia
Anesthetic management during surgery can either be performed as conscious analgo-sedation, or general anesthesia using either inhalative or intravenous sedative agents. Generally, awake techniques are preferred, since it allows for interaction with the patient during surgery and good accuracy of neuro navigation-based MER and intraoperative test stimulation. However, awake surgery of the brain may be considered as terrifying or exhausting for the patients. Therefore, general anesthesia may be regarded as an alternative option, even though GABAergic anesthetic agents affect the neural activity pattern of target structures and hence impede the quality of MER. 48 Additionally, intraoperative test stimulation will only provide limited insights in such cases, that is, tetanic contraction due to the current spread into the internal capsule. The implantation of the IPG is performed under general anesthesia, which may follow immediately after electrode implantation or in a second session.
As outlined in the previous section, up-to-date imaging techniques allow for well-tolerated and accurate DBS lead placement without the application of MER. Therefore, it is not surprising that recent publications on clinical safety and efficacy of DBS surgery under general anesthesia lead to results equivalent to awake surgery. 49 However, patients undergoing awake surgery may improve faster and have better results on axial symptoms like dysarthria, potentially since DBS-induced worsening of such symptoms can easily be detected during intraoperative testing stimulation in awake surgery, allowing for better decision-making on the final electrode placement. 50 In summary, awake surgery still seems advantageous for STN DBS in PD, although asleep surgery may be considered with lower threshold in patients not suitable for awake surgery. 50
Targets for DBS
Despite the success of dopaminergic treatment for bradykinesia and rigidity, PD tremor may not respond as satisfactorily to dopaminergic treatment or other tremor-depressant drugs. Hence, it is not surprising that the suppression of a medication-refractory disabling tremor was a primary aim of the first DBS procedures, targeting the ventral intermedius thalamic nucleus (VIM) based on lesioning experiences. 5 VIM DBS indeed alleviates tremor, but not bradykinesia or rigidity. 51 Following these experiences, DBS of the VIM or slightly inferior structures, namely the posterior subthalamic area (PSA), 52 may be considered in PD patients who suffer from disabling tremor only or do not apply for STN or GPI DBS.
Growing insights into basal ganglia involvement in the pathophysiology of cardinal motor symptoms of PD and experiences with lesioning techniques led to the consideration of the STN and GPI as targets for DBS in PD. So far, STN DBS is the more commonly used, but both targets allow for improvement of PD-associated appendicular symptoms (brady/akinesia, rigidity, and tremor). Initial data on STN DBS showed an impressive improvement of the Unified Parkinson’s Disease Rating Scale motor subscore (UPDRS-III), by 49–71%,53,54 and a marked reduction of the levodopa equivalent daily dosage (LEDD) by 56%. 53 The following analyses (mainly class IV studies with a follow up period of 6–24 months in most cases) revealed similar results, indicating an average improvement of 52% in the UPDRS-III and of 35% in QOL assessments, as well as an improvement of dyskinesia, daily off-periods, and LEDD by 69%, 68%, and 56%, respectively. 55
While the motor symptoms of PD are the primary targets of STN DBS, there are also indicators for nonmotor improvements. Present studies indicate that STN DBS may alleviate hyperdopaminergic behaviors and neuropsychiatric fluctuations, most likely because of associated reduction of dopaminergic medication.56,57 The presence of hyperdopaminergic behaviors and neuropsychiatric fluctuations may therefore be judged as additional arguments in favor of STN DBS in patients with disabling motor fluctuations. Additionally, STN DBS may improve the subjectively rated quality of sleep, pain, autonomic function, 58 including weight gain, presumably due to the modulation of central metabolic control. 59
Compared with STN DBS, fewer studies are available evaluating the efficacy of GPI DBS in PD. But comparative studies suggest that differences of the effects gained from STN and GPI DBS are just slight, heterogeneous, and without any convincing advantage of one target towards the other.60–68 GPI DBS may be associated with fewer side effects such as reduced verbal fluency, dysphagia, gait disturbances, or psychiatric symptoms. Some authors claim better antidyskinetic effects of GPI DBS than STN DBS. However, GPI DBS has a lower potential to reduce LEDD and a higher demand on battery consumption to achieve beneficial results. In addition, the present data do not allow us to draw any reliable conclusions about the effects of GPI DBS on hyperdopaminergic symptoms and neuropsychiatric fluctuations. Several publications on STN DBS demonstrated a sustained efficacy for more than a decade;69–71 while similar profound long-term results on GPI DBS efficacy in PD have yet to be provided. Indeed, several publications reported a loss of efficacy in GPI DBS, which could be compensated by subsequent STN DBS.72–75 However, GPI DBS has also been introduced as a successful strategy to manage the unsatisfactory long-term results of STN DBS. 76
To date, the question of whether STN or GPI DBS is superior has not been resolved and is still a matter of controversial debate. With respect to the available data, STN DBS may be preferred in patients with high demand on dopaminergic medication or hyperdopaminergic behaviors and neuropsychiatric fluctuations, while GPI DBS can be considered as primary target in cases of mild cognitive decline, predominant axial symptoms, or severe hyperkinesia, even on low medication. 77
For axial symptoms of PD, DBS of the mesencephalic locomotor region has been suggested as an alternative target, given very heterogeneous results from STN and GPI DBS. 78 As such, DBS of the pedunculopontine area has been chosen as the target for electrode placement. 79 However, the results of a recent meta-analysis of long-term efficacy were disappointing. 80 Recently, DBS of the substantia nigra pars reticularis was described to improve gait and posture. Combined with STN DBS, Weiss and colleagues revealed additional beneficial effects on the freezing of gait. 81 To date, the impact of DBS of the mesencephalic locomotor region is still unknown and further studies are needed for validation before consideration in the clinical standard of care.
Postoperative management
Current technical advances such as current steering along the longitudinal axis of the stimulation electrode as well as utilization of segmented leads allow for a more precise definition of the volume of neural activation (VNA). However, these opportunities also increase the degrees of freedom in the complex scenario of DBS programming. As such, the procedure to identify optimal stimulation settings become more challenging in terms of time management and potential risks for confounding results due to the patients’ exhaustion during the assessment. The clinical assessment of optimal stimulation parameters at our center are strongly influenced by programming algorithms provided by Volkmann and colleagues, 82 and recommendations by Cheeran and colleagues. 83
A reliable assessment of PD-related symptoms is mandatory to reliably rate the degree of clinical response to DBS. Care should be taken, if the patient is assessed shortly after DBS surgery, since microlesion effects from MER or the DBS electrode as well as acute foreign body reactions may alter hemostasis of neural activity and therefore may have a direct impact on motor and nonmotor function. As such, the microlesion effect may dramatically improve cardinal symptoms even without the application of chronic stimulation. 84 Additionally, the mental stage may change and lead to hypomania, depression, or apathy. In such scenario, extensive testing would not provide valid results. Therefore, clinical assessment for optimal stimulation parameters should ideally be performed after complete remission of microlesion effects. Based on the authors’ experience, it is reasonable to perform such clinical assessment not earlier than 1 week after electrode implantation. In that case, postoperative baseline motor function is obtained after withdrawal of dopaminergic medication for at least 12 h. Bradykinesia, rigidity, and rest tremor are evaluated based on standardized scores, like the UPDRS-III. Likewise, axial symptoms like dysarthria, postural stability and gait performance are evaluated. The rater should be aware that tremor, rigidity and bradykinesia may have a different time course of response to DBS. DBS is applied in a sequence of monopolar stimulations (‘monopolar review’), that is, the IPG case serves as an anode, while each contact of the DBS electrode is individually selected as a cathode. We recommend a step-wise evaluation of stimulation at a certain height, starting with the lowermost contact. In the presence of segmented leads, we recommend to first coactivate all segments of a given height and to also apply omnidirectional stimulation. Afterwards, all segmented leads should be individually tested for beneficial and side effects, as done for omnidirectional stimulation.
Traditionally, a stimulation frequency of 130 Hz and a pulse width of 60 µs is applied for this procedure and for chronic stimulation after the contact providing the best stimulation results have been identified. If applicable, the stimulation amplitude should be specified as current (constant current mode), given its low variability of clinical efficacy due to impedance changes in the long-term treatment.85,86 For a reasonable relationship between clinical accuracy and time consumption, we recommend a step-wise increase of the stimulation amplitude by 0.5 mA for evaluation of cylindrical contacts. For segmented leads, a given current amplitude leads to a higher charge density on the contact and therefore a larger VNA, compared with omnidirectional stimulation. Hence, lower thresholds for clinical improvement and occurrence of side effects can be expected. Therefore, we suggest further specification by increase of the stimulation amplitude by 0.1–0.2 mA, until the relevant clinical improvement is observed again. The lowest amplitudes leading to (1) such improvement and (2) complete alleviation of symptoms should be noted. Similarly, the lowermost amplitude causing sustained transient and sustained side effects (e.g. negative impact on gait, balance, and speech) should be precisely documented as well.
The contact providing optimal prerequisites for chronic DBS is eventually identified by low amplitude thresholds for beneficial effects and a large therapeutic window, that is, a large difference between threshold amplitudes for sustained side effects and symptom improvement. For the application of chronic stimulation, a careful increase of the stimulation amplitude and simultaneous careful adaption of dopaminergic medication should be preferred over directly choosing the stimulation intensity which led to optimal results during a monopolar review and a rapid decrease of the LEDD, since slow adaptions may reduce the risk of postoperative apathy. 87
Rarely, any monopolar setup leads to sustained side effects at low stimulation amplitudes and therefore prevents satisfactory improvement. In that case, the therapeutic window can be increased by lowering the pulse width to 30 or 40 µs, as shown in a recent study. 88 Alternatively, a bipolar setup may help narrowing the spread of current and hence prevent modulation of anatomical structures which mediate adverse effects. Conversely, a combined selection of several contacts as cathodes may further shape and extend the VNA and therefore may be applied if monopolar cathodic stimulation via a single contact does not provide optimal symptom control. 89 In the case of relevant axial symptoms, like freezing of gait or dysphagia, which may be refractory or even caused by standard DBS settings, we suggest reducing stimulation frequency to 60–80 Hz if the abovementioned procedures turn out to be ineffective.90,91 In turn, increase of stimulation frequency may provide additional clinical effect especially if tremor cannot sufficiently be suppressed with standard stimulation frequency of 130 Hz. 89
Chronic DBS is ideally applied with settings providing the best suppression of clinical symptoms without any adverse effects. However, this situation cannot always be achieved. In such cases, patient and healthcare providers should make a shared decision for further procedures. One potential solution is to provide different stimulation programs, which can be switched by the patient at any time. For example, if complete tremor suppression is accompanied by impairment of speech, a second stimulation program may provide incomplete tremor control but no negative effects on speech. Dependent on the patient’s needs, either program would provide optimal support (e.g. optimal tremor control while eating, optimal speech during conversation). Healthcare providers should also be aware that side effects may evolve over time and not immediately manifest. Similarly, as recently revealed for DBS of the VIM, a prolonged deactivation (‘stimulation holiday’) for several days may be needed to reveal DBS-associated adverse effects such as gait ataxia, which may be mediated by a maladaptive neural response. 92 Therefore, such a procedure is advised to be performed in cases of unusual worsening of symptoms several weeks to months after the application or adaption of chronic DBS.
Complications and side effects
DBS surgery is generally regarded as well tolerated. 12 However, the nature of this techniques implies that there are potential risks during the surgical procedure, and interestingly, considerable differences can be found among different publications. 93 Intracranial hemorrhage has been reported to occur in about 1–10% of cases. However, only one study reported bleeding rates of 10%, and expert consensus declared that the risk of symptomatic intracranial hemorrhage can be estimated to be less than 2%. 12 Further surgery-related complications and associated risk estimations were stroke (0–2%), infection (0–15%), lead erosion without infection (1–2.5%), lead fracture (0–15%), lead migration (0–19%), and death (0–4.4%). 12 Additionally, intra- or postoperative seizures may occur in about 1–5%.94,95 Despite the precision and accuracy of functional neurosurgery, the inaccurate placement of the DBS is not uncommon and may be responsible for the lack of therapeutic effects or disabling side effects impeding the patients’ QOL. Indeed, a recent study evaluating two North American databases indicated a rate of 15.2–34% for revision and removal of DBS electrodes. 96 In about 50% of available data, re-surgery was performed because of hardware-related complications or infections, which is comparable to the findings of other studies, where hardware-related complications were found in 11.3-–25% of cases.95,97 The remaining 7–17% of electrode revisions or removals were assumed to originate from electrode misplacement. The risk for patients with bilateral DBS was approximated to be about twice as high as for patients with unilateral DBS, 98 indicating a fixed risk for each electrode, which was estimated to be 4.3-–8.4% per electrode year.97,99 The effects of brain penetrations due to microelectrodes or the DBS leads may lead to microlesion effects or foreign body reaction, resulting in a transient improvement of motor function. 84 In addition to the alteration of motor function, microlesion effects may also impair cognitive states and verbal fluency,45,82 or development of transient psychiatric conditions. 100 Additionally, persistent deterioration of neurological function has been described (gait and speech disturbances, cognitive decline, and depression). 101 In particular, passage of electrodes through the caudate nuclei is associated with increased risk of cognitive decline and therefore should be avoided. 47
Adverse effects from DBS itself depend on the stimulation parameters and the geometric relationship between the electric field generated and critical anatomical structures. As such, STN, GPI, and VIM DBS may lead to the spread of current to the corticospinal tract and cortico-brainstem fibers (corticomesencephalic, corticopontine, and corticobulbar tract) and hence to tonic muscle cramps or forced deviation of gaze. In such cases, stimulation at low frequencies (4 Hz) may mediate repetitive contractions (‘tremor drive’) of the affected body part. Time-locked electromyography allows the confirmation of motor-evoked potentials. 102
The most common adverse effect of STN DBS are impairment of axial motor performance, such as disturbances of speech, postural stability and gait. Less often, eyelid apraxia, dysphagia, vegetative symptoms like ipsilateral sweating and mydriasis, or hypersalivation are observed. Diplopia may occur as the result of co-stimulating the oculomotor nerve. Overstimulation of the sensorimotor part of the STN may lead to dystonia or dyskinesia, whereas co-stimulation of the substantia nigra may induce akinesia despite loss of rigidity. Cognition, including verbal fluency, may worsen due to STN DBS itself (mediated by spread of curent into nonmotor areas of the STN), or because of lesion effects following microelectrode recording or final electrode placement.42,62,103,104 While generally considered not to be clinically significant, 58 cognitive impairment is common and may be observed in about 41% of STN DBS patients, especially in patients with advanced stages of the disease. 105 Apathy is another common phenomenon after STN DBS surgery, which may counteract improvements of QOL, despite the relevant improvements in motor function. 106 Since STN DBS may allow for the dramatic reduction of dopaminergic medication, the secondary effects due to levodopa withdrawal have to be carefully distinguished from the effects associated with DBS or DBS surgery. 107 In fact, a slow and careful adaption of dopaminergic medication after DBS surgery as opposed to aggressive reduction may reduce the risk of post-surgery apathy. 87 Impairment of depressive symptoms and anxiety is another potential risk of STN DBS and has been estimated to be 8% and 2%, respectively. 105 An increased risk of committing suicide has also been described, 108 even though an increased risk for suicidal ideations could not be confirmed in a recent randomized, controlled trial. 109 Hence, the present data do not allow for robust statements on whether and to what degree STN DBS increases the risk of suicidal behavior. Additionally, (hypo)manic states can be found in about 4% of patients following STN DBS surgery, 105 which is associated with a ventromedial placement of the DBS electrode. 110 Given this considerable percentage of patients who develop depression, anxiety or (hypo)mania, regular clinical evaluations after surgery are essential for early detection and optimal treatment of such patients, including the ones at risk of committing suicide.
For GPI DBS, psychiatric disturbances such as depression and suicide have also been reported. 109 In some studies, a lower frequency was observed than in STN DBS, 111 while other studies did not find significant differences among the two targets. 112 GPI DBS via more ventrally located contacts may lead to phosphenes due to co-stimulation of the optic tract, which is usually transient. Additionally, ventral stimulation provides great antidyskinetic effects but may worsen bradykinesia, whereas the spread of stimulation into the external pallidum may induce dyskinesia. 113
The side effects of stimulation of the VIM or PSA may be especially observed in the long-term treatment either due to effects of plasticity or the need to increase stimulation amplitudes to maintain satisfactory clinical results due to adaptive processes. Hence, the discontinuation of stimulation is suggested during the night time, if applicable, to reduce such effects. While modulation of the dentato-thalamic tract is considered relevant for tremor control, stimulation of other cerebellar tracts such as the ascending limb of the uncinate tract may cause dysarthria and gait ataxia. Similar to STN DBS, transient paresthesia due to stimulation of sensory fibers are common and unproblematic, but overstimulation or stimulation via a too dorsally placed contact may also lead to persistent and unpleasant sensory symptoms.
Mechanisms of action
Early theories primarily pointed out the clinical similarities of lesioning and DBS in a given anatomical target and hence high frequency DBS was assumed to mediate its effects by functionally lesioning adjacent neural structures. In fact, neighboring neuronal activity was found to be suppressed by high frequency STN and GPI DBS.114,115 Theoretical and electrophysiological studies however provided evidence that mechanisms underlying DBS are rather mediated by activation of axonal fibers, while neural somas are less likely to be excited because of higher activation thresholds. 116 The cumulative effect of orthodromic (synaptic) transmission to efferent cells depends on the relation of excitatory and inhibitory fibers activated by DBS, 117 leading to neural inhibition in regions with predominant GABAergic afferents, like STN and GPI. 118 Similarly, high frequency STN DBS leads to activation of excitatory efferent fibers to the GPI and substantia nigra pars reticulate,119,120 while GPI DBS at high frequencies reduces thalamic activity via inhibitory efferents. Additionally, antidromic modulation of cortical activity via the hyperdirect pathway has been shown to be crucial for clinical efficacy in animal models of STN DBS, 121 and human studies also revealed DBS-evoked cortical potential compatible with such antidromic activation in PD patients. 122 These observations describe the immediate neurophysiological reaction to DBS pulses, but they do not account for the observation that high but not low frequency DBS is crucial to mediate clinical effects.
This finding however, can be well explained by the impact of DBS on pathological oscillatory activity: oscillatory activity in the beta of sensorimotor cortex, basal ganglia, thalamus and the cerebellum, which is most prominent during static motor control, (rest or tonic muscle contraction) and thought to preserve this state. Increased oscillatory activity in the low beta band is a characteristic finding in PD, which is correlated to bradykinesia and rigidity. 123 In turn, motor improvement after administration of levodopa is accompanied by suppression of such excessive beta activity. 124 Since reduction of motor velocity can also be induced by entrained beta activity in the motor network of healthy probands, 125 increased beta activity in PD is considered to play a causal role in PD an not to be just an epiphenomenon. Besides pathological beta activity, PD tremor is associated with increased synchronized activity in the basal ganglia, the thalamus, and motor regions of the cerebral cortex. 126 High DBS may disrupt such oscillatory activity, since antidromic propagation of DBS-evoked action potentials collision block endogenously generated action potentials. 127
Finally, non-neural tissue may play a crucial role, especially in the chronic efficacy of DBS. Gliotransmitters have been showed to be released by high frequency DBS in an amplitude and frequency-dependency manner, which may maintain neural hemostasis and also contribute to changes of blood perfusion and synaptic plasticity in an environment of chronic high frequency stimulation. 127 More extensive information about current understanding of the mechanisms underlying DBS is provided elsewhere.127,128
New developments
Recent advances of pulse generators and electrodes allow for a more focused, selective modulation of neuronal targets of interest. This is achieved either via the precise shaping of the electric field created by DBS and via preferred activation of myelinated fibers as realized by appropriate pulse width selection. Simultaneously, these advances also increase the degrees of freedom to adapt DBS and therefore represent a new challenge to perform a systematic and valid clinical assessment.
Current steering via multiple independent current control
Initial hardware improvements for Medtronic DBS systems (Medtronic, Dublin, Ireland) were rechargeable IPGs and the applicability of an alternating stimulation pattern to provide current via two different contacts of the same electrode, 129 which may allow to further suppress dyskinesia or side effects in (STN) DBS by shaping the electric field along the longitudinal axis of the DBS electrode (interleaving DBS).130,131 Further options for longitudinal shaping of the VNA were introduced in hardware devices from Boston Scientific, (Boston Scientific Corporation, Marlborough, Massachusetts, USA) which provide the currently unique feature of multiple independent current control (MICC) for each contact of the electrode. This technique allows, besides even more complex shaping of the electric field, the seamless transition of a given electric field between two adjacent contacts (current steering).132,133 MICC also warrants constancy of the electric field generated from DBS even if the impedances of simultaneously activated contacts asymmetrically vary over time. In contrast, such scenarios of varying impedances would lead to a predominant current flow via the contact with lower impedances and hence to a change of the applied electrical field in IPGs with a just a single current source.
Spectrum of applicable pulse widths
Many studies suggest that activation of neural fibers but not cell bodies is crucial to gain therapeutic effects of DBS.116,121 It is well known that myelinated axons have a much lower chronaxie, compared with less or unmyelinated fibers or cell bodies. 134 Up-to-date IPGs account for these insights and offer even shorter pulse widths than traditional IPGs, which were restricted to a minimum value of 60 µs. Indeed, pulse width reduction increases the therapeutic window for DBS and hence is particularly useful in patients who experience side effects even with low stimulation amplitudes.88,135 Table 1 summarizes the features of IPGs currently available in clinical standard of care.
Capabilities of the latest generation implantable generators currently approved in clinical standard of care.

IPG, implantable pulse generator; M, approved adapters for deep brain stimulation electrodes by Medtronic can be provided; MICC, multiple independent current control; MRI, magnetic resonance imaging.
Medtronic SC offers current supply for one single electrode only.
Segmented DBS electrodes for directional DBS
The most cutting-edge technology currently available for DBS in clinical standard of care is the advancement of electrode design directional stimulation. Here, current is applied via single or multiple segmented leads, which, to a certain degree, allows the steering of the current along a vector perpendicular to the electrode and therefore provides a more focused stimulation to reach preferred anatomical areas, while simultaneously avoiding areas which mediate side effects. 136 Theoretical studies suggest that a directional DBS via segmented contacts may shift the center of the VNA up to 1–1.3 mm compared with omnidirectional DBS. 137 As a consequence, directional DBS will not be able to compensate unsatisfactory results in the case of gross lead misplacement but rather help optimize results in well-placed or just slightly (1–1.3 mm) misplaced electrodes. 137 This especially applies for STN DBS, given the proximity to brain areas which may mediate side effects, like the internal capsule. As with the longitudinal modulation of the electric field, MICC offers a more gradual approach to modulate the main direction of applied current, which has a higher impact on the accuracy of radial VNA shaping than uniform current distribution in multi-cathodic DBS. 137 Furthermore, the distinct selection of segmented contacts, especially when using MICC, allows for orientation-selective pathway activation and hence may help increase the therapeutic window. 138
Since the surface of the segmented contacts is considerably smaller than the one of classical cylindrical contacts, a given stimulation amplitude providing constant current dramatically increases the local current density on the contact, especially close to its edges, 139 and thus the size of the electric field generated by DBS. In fact, while usage of a segmented contact is associated with higher impedance values for the same reason, the overall smaller amount of applied current to generate a given VNA may eventually lead to less battery consumption and hence a more efficient stimulation. Currently, all approved DBS electrodes offering directional stimulation consist of a classical contact at the most distal position, followed by two segmented contacts, which are separated into three equal surfaces, respectively. Each segment covers 25% of the electrode circumference, since the central angle of the arc-shaped segment is 90°. The most proximal contact has a cylindrical shape without segmentation again.
Special features of different electrode models
Among the last generation DBS electrodes, the Boston Scientific DB-2201-45 is the only one offering eight different heights for classical cylindrical contacts. Hence, this electrode offers the distribution of current via a broad longitudinal range. Another method to modulate the range for stimulation along the electrode’s longitude, Medtronic and Abbott (Abbott Laboratories, Abbott Park, Illinois, USA) electrodes can be ordered with a contact spacing of 1.5 mm and 0.5 mm. For a more precise adaption of the electric field to the patient’s anatomy, a small spacing of 0.5 mm is preferred for STN DBS. For DBS of the much larger GPI, a spacing of 1.5 mm is predominantly selected. Medtronic’s 3391 electrode, offering a contact length of 3 mm and a spacing of 4 mm, is generally not used for DBS in PD but rather reserved for DBS in psychiatric diseases. The Boston Scientific DB-2202-45 electrode is also characterized by a special configuration of the lowermost contact, which does not have a cylindrical shape but also comprises the electrode’s tip, similar to the lead 6148, which was second last electrode model of St. Jude Medical (Abbott). If stimulation is applied by such a contact, the resulting electric field is slightly different from cylindrical electrodes and covers a larger volume beneath the tip. 140 This special contact has a larger surface, compared with cylindrical contacts. Hence, a given stimulation amplitude will lead to a lower charge density and consecutively to a smaller VNA. Therefore, higher stimulation intensities may be needed to gain a satisfactory clinical effect, despite the advantage of a more pronounced stimulation field beneath the electrode. 140 Table 2 provides an overview on the characteristics of different DBS electrode models.
Capabilities of latest generation deep brain stimulation electrodes which are currently approved in clinical standard of care.
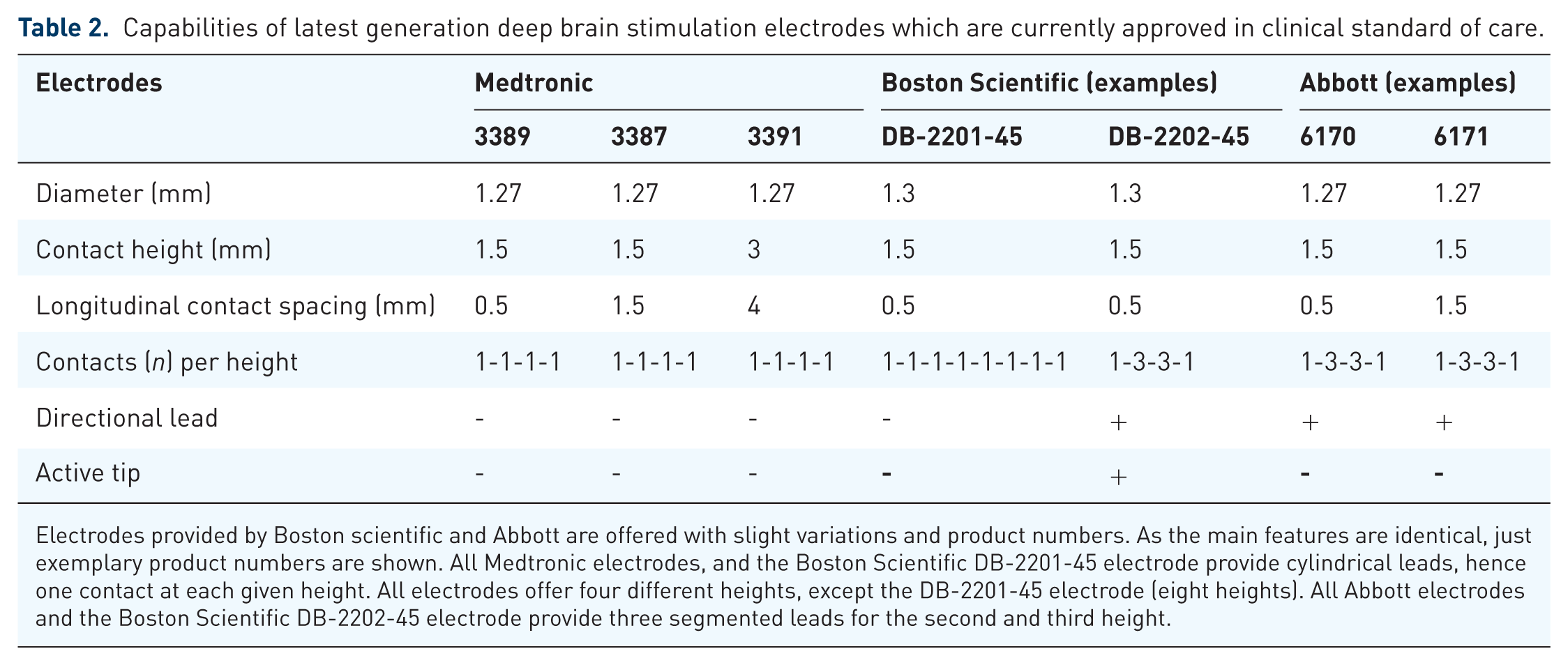
Electrodes provided by Boston scientific and Abbott are offered with slight variations and product numbers. As the main features are identical, just exemplary product numbers are shown. All Medtronic electrodes, and the Boston Scientific DB-2201-45 electrode provide cylindrical leads, hence one contact at each given height. All electrodes offer four different heights, except the DB-2201-45 electrode (eight heights). All Abbott electrodes and the Boston Scientific DB-2202-45 electrode provide three segmented leads for the second and third height.
Future directions
Adaptive neuromodulation
Recent advances in DBS for PD just emerged and their therapeutic power and potential superiority towards former generation DBS devices and electrodes, the implementation of further advances in DBS technique may be expected shortly. Hardware-related innovation include adaptive closed-loop techniques. Given the characteristic increase of basal ganglia oscillatory activity in the beta frequency band in PD and its correlation with PD-related symptoms, adaptive stimulation has been suggested to suppress this beta activity if it exceeds a certain threshold level. 141 This technique additionally allows the avoidance of a short beta burst, which may be associated with healthy motor processing and suppression of long beta bursts, which are correlated with motor impairment in PD. 142 Phase-specific DBS, restricted to a distinct phase of tremor has also been introduced as an effective and energy-efficient technique in a case series of essential and dystonic tremor patients, 143 which may also be applied for DBS in PD tremor. Complementary strategies have suggested neurochemical analysis, that is, dopamine release, to adapt DBS intensity in a closed-loop framework. 144 Further hardware-related improvements may be provided by new stimulation waveforms, which have been suggested as more efficient than standard rectangular waves. 145
Optimization of electrode placement and programming
High-field MRI (7T) may facilitate the identification of anatomical targets for DBS, 146 and the growing availability of such imaging data is likely to enhance the precision of DBS placement. The same applies to imaging sequences such as diffusion imaging and consecutive tractography to delineate cortical connections of subcortical DBS targets, which may be associated with clinical efficacy.85, 147 With the availability of highly precise imaging data for surgery planning, MER may become less relevant in the future, especially as there is evidence that MER may increase the risk of microlesions during surgery and hence negatively impact the outcome of surgery.41,43 Once the DBS electrode is implanted, software tools may aid the programmer to gain a better understanding of the spatial relationship between the DBS electrode, the anatomical target, and the VNA, and also help identify electrophysiological markers for ideal targets. 147 Since the degrees of freedom for DBS programming constantly increase with new features like directional stimulation, MICC, or broader ranges of applicable pulse widths, it is virtually impossible to assess all settings which may be advantageous for an individual patient. Hence, predictors for DBS efficacy are strongly needed to allow for preselection of a limited number of setups, which are likely to provide optimal results in chronic DBS. Computational models of DBS were not only used as tools to provide a better understanding of DBS, but also to identify optimal targets and stimulation parameters. 148 So far, the application has been predominantly used for research purposes. Nevertheless, CE-certified software solutions are commercially available, the validity of their application to improve DBS programming however, has yet to be shown on robust clinical studies.
The role of DBS in an era of novel treatment options for PD
Novel treatment options for PD have been introduced, which may not only address motor symptoms but rather reduce progression of the disease. Such treatment strategies include for example monoclonal antibodies, small molecules, or chelating agents. 149 So far, it is unclear, if and to what degree such treatment methods are able to act as disease-modifying agents. In the case of successful applications, deceleration of disease progression may delay the occurrence of motor fluctuations, the classical indication for DBS. While the gradual decrease of DBS surgery may be expected from such development, patients who are treated with DBS may also benefit from such treatments combined with DBS due to delayed manifestation of DBS-refractive symptoms like cognitive decline or frequent falls.
Conclusions
DBS is an effective and generally well-tolerated treatment for motor symptoms in PD. Cutting-edge technology in combination with novel medical treatment options may dramatically reduce the burden associated with the disease.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
CJH received a travel grant from Abbott; SF declares no conflicts of interest; SJG received honoraria and travel expenses from Medtronic, Abbott, and Boston Scientific; LW received honoraria from Medtronic and Abbott/St. Jude Medical; AS received honoraria from Abbott, Boston Scientific, Medtronic and Abbvie.