
Abstract
Nonmotor symptoms are an integral part of Parkinson’s disease and cause significant morbidity. Pharmacological therapy helps alleviate the disease but produces nonmotor manifestations. While deep brain stimulation (DBS) has emerged as the treatment of choice for motor dysfunction, the effect on nonmotor symptoms is not well known. Compared with pharmacological therapy, bilateral subthalamic nucleus (STN)-DBS or globus pallidum interna (GPi)-DBS has significant beneficial effects on pain, sleep, gastrointestinal and urological symptoms. STN-DBS is associated with a mild worsening in verbal fluency while GPi-DBS has no effect on cognition. STN-DBS may improve cardiovascular autonomic disturbances by reducing the dose of dopaminergic drugs. Because the motor effects of STN-DBS and GPi-DBS appear to be similar, nonmotor symptoms may determine the target choice in surgery of future patients.
Keywords
Introduction
The pathology of Parkinson’s disease (PD) extends far beyond the nigrostriatal system and results in nonmotor symptoms coexisting with motor symptoms. Nonmotor symptoms can precede motor symptoms by years and are common in all stages of PD.They cause significant morbidity [Lim and Lang, 2010] and are often under recognized by health professionals [Parsons et al. 2006]. They can be divided into four domains: neuropsychiatric, autonomic, sleep and sensory dysfunction [Lim and Lang, 2010].
The effects of dopamine replacement therapy (DRT) and deep brain stimulation (DBS) on motor symptoms are well known. DBS has been shown to be more effective than the best medical therapy in improving ‘on’ time without troubling dyskinesias by 4.6 h/day, motor function in 71% versus 36% on medical therapy, and in quality of life 6 months after surgery [Weaver et al. 2009; Pahwa et al. 2006; Goetz et al. 2005]. This improvement was seen equally in bilateral DBS of the subthalamic nucleus (STN) and globus pallidum interna (GPi) [Follet et al. 2010].
The effect of various therapeutic modalities on nonmotor symptoms is still unclear. This review compares the effects of DBS and various dopaminergic drugs on nonmotor symptoms of PD.
Methodology
A literature search using PubMed databases was carried out for the effect of DBS and various antiparkinsonian medications on nonmotor symptoms using the following search words/phrases: deep brain stimulation, dopamine replacement, dopaminergic agonists, monoamine oxidase B (MAO-B) inhibitors, catechol-O-methyltransferase inhibitors, and cognition, behavioural abnormalities, autonomic involvement, autonomic disturbances, cardiovascular autonomic differences, gastrointestinal changes, micturition, sexual abnormalities, sleep disorders, pain, olfaction. The search yielded 2789 articles. Controlled studies that performed a head-to-head comparison of patients on DRT and after DBS are few and are listed in Table 1. These included 22 publications, 17 on neuropsychiatric symptoms, two on cardiovascular autonomic functions, one on sleep and two on quality of life. Subsequently, from PubMed indexed articles, additional reports were included after reference analysis if they evaluated the effect of DRT alone (Table 2) or DBS on various nonmotor symptoms, especially when there are no clear head-to-head comparison studies. Studies comparing the effect of DRT or DBS on overall nonmotor symptoms are given in Table 3.
Controlled studies comparing patients receiving dopamine replacement therapy (DRT) versus deep brain stimulation (DBS).
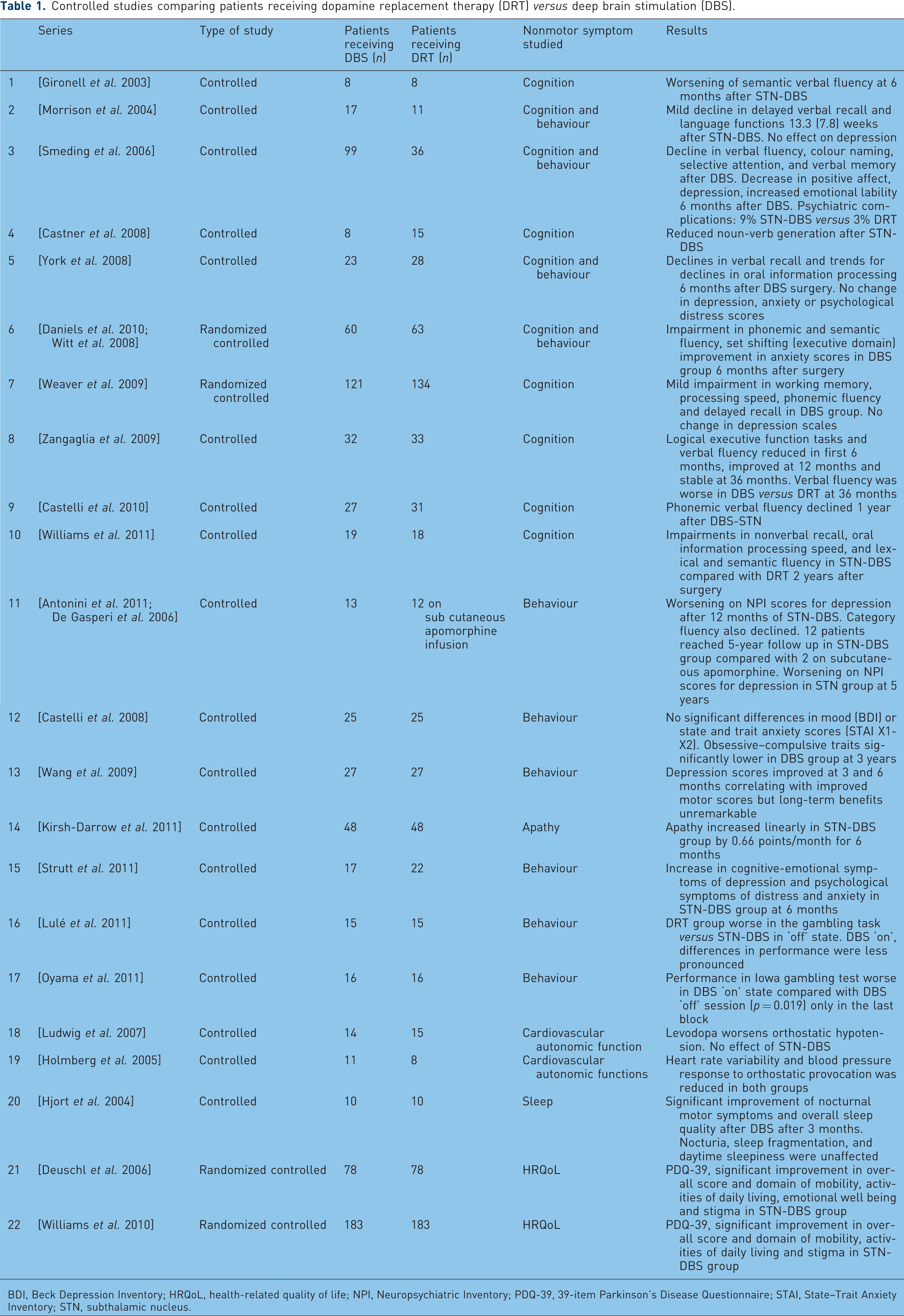
BDI, Beck Depression Inventory; HRQoL, health-related quality of life; NPI, Neuropsychiatric Inventory; PDQ-39, 39-item Parkinson’s Disease Questionnaire; STAI, State–Trait Anxiety Inventory; STN, subthalamic nucleus.
Effect of dopaminergic therapy on nonmotor symptoms of Parkinson’s disease (PD).

BDI, Beck Depression Inventory; ICD, impulse control disorder; PDQ-39, 39-item Parkinson’s Disease Questionnaire; PET, positron emission tomography; RIII, nociceptive flexion response; QL-GAT, quantitative lower-gastrointestinal autonomic test; UPDRS, Unified Parkinson’s Disease Rating Scale.
Studies comparing overall nonmotor symptoms in dopamine replacement therapy (DRT) and deep brain stimulation (DBS) groups individually.

NMS Quest, Nonmotor Symptoms Questionnaire; NMSS, Nonmotor Symptoms Assessment Scale; PDQ-39, 39-item Parkinson’s Disease Questionnaire; STN, subthalamic nucleus; UPDRS, Unified Parkinson’s Disease Rating Scale.
Review
The effects of DBS and DRT on each nonmotor domain are described below.
Neuropsychiatric dysfunction
Cognitive and behavioural changes are common nonmotor symptoms which can impair social and occupational functioning of patients. Cognitive abnormalities in PD are characterized by dysfunction in various domains of executive function, language, memory, vision and psychomotor speed [Lim and Lang, 2010].
Cognition
Studies on the effects of DBS on cognition have shown differing results. This is partly because of the inhomogeneity in neuropsychological tests and patient population characteristics in these studies. This is also evident in various meta-analyses and reviews. While recent meta-analyses have shown mild worsening of cognition, with cognitive problems in 41% of patients after STN-DBS [Temel et al. 2006] and a moderate decline in semantic and phonemic verbal fluency [Parsons et al. 2006], another review by Halpern and colleagues showed mixed results. Improvement in working memory, psychomotor speed and visuomotor sequencing was noted in some studies while worsening in tests of executive function – verbal fluency, memory and language functions – were noted in other studies [Halpern et al. 2009].
It is still unclear how the trajectory, stimulation parameters and position of DBS electrodes modify cognitive functions. A comparison of 299 patients with bilateral DBS, either STN or GPi, showed similar cognitive functions in both groups except for a decrease in visual processing speed in patients with STN-DBS [Follet et al. 2010]. Two other randomized, controlled studies, which compared the cognitive outcome of bilateral STN-DBS versus GPi-DBS [Rothlind et al. 2007] and unilateral STN-DBS versus GPi-DBS [Okun et al. 2009], found no significant difference in the cognitive outcomes, although there was a greater decline in letter verbal fluency in the STN-DBS group [Okun et al. 2009].
The exact location of the electrodes has an impact on cognitive outcome. In a study comparing unilateral STN versus GPi stimulation, there were no impairment in measures of mood and cognition when electrodes in the optimal locations of GPi or STN were stimulated, in contrast to adverse mood effects on stimulation of ventral locations in both targets [Okun et al. 2009].
There are very few studies on unilateral DBS. Cognition may be better preserved in these patients. In a recent study bilateral STN-DBS worsened cognitive and motor function in modest dual task conditions more than unilateral DBS [Alberts et al. 2008; Hershey et al. 2004]. This motor and cognitive worsening with bilateral STN-DBS was minimized with stimulation parameters that reduced current spread to nonmotor areas of the brain [Frankemolle et al. 2010].
Most dopaminergic agonists [Rektorová et al. 2005] showed no effect on cognition. While a few studies on dopaminergic agonists and MAO-B inhibitors have shown improvement in executive function and memory [Costa et al. 2009; Takahata et al. 2005; Speiser et al. 1998], others have demonstrated worsening of cognition by increased sedation, confusion or hallucinations [Jahanshahi et al.2010; Brusa et al. 2003].
Comparative studies of cognition of patients undergoing DBS with a control group on DRT are few and listed in Table 1. Most studies, including a large randomized, blinded assessment trial, have shown a mild but significant reduction in verbal fluency at the end of 6–12 months in patients who underwent STN-DBS compared with best medical treatment [Williams et al. 2011; Castelli et al. 2010; Daniels et al. 2010; Weaver et al. 2009; Zangaglia et al. 2009; Witt et al. 2008; York et al. 2008; Smeding et al. 2006; Morrison et al. 2004; Gironell et al. 2003]. A few studies have shown worsening in other tests of executive function [Weaver et al. 2009; Williams et al. 2011; Zangaglia et al. 2009; Witt et al. 2008; Smeding et al. 2006] and verbal memory [Williams et al. 2011; Weaver et al. 2009; York et al. 2008; Smeding et al. 2006; Morrison et al. 2004].
Controlled studies have looked at the short-term effects of DBS and DRT on cognition. Zangaglia and colleagues compared the effect of bilateral STN-DBS with standard medical therapy at 3-year follow up and found a reduction in verbal fluency scores in the surgical arm associated with a short-term transient worsening of frontal executive function [Zangaglia et al. 2009]. A recent study of 20 patients examined the effect of bilateral STN-DBS 8 years after surgery and showed slight but persistent reduction in verbal fluency, abstract reasoning, executive function and episodic memory [Fasano et al. 2010]. One patient developed dementia at 5 years and their condition continued to worsen at 8 years [Fasano et al. 2010].
While impairment in cognition after STN-DBS is mild in most patients [Halpern et al. 2009], patients with impaired attention, advanced age and a low levodopa response at baseline seem to be more vulnerable to cognitive decline after STN-DBS [Smeding et al. 2011]. Thus cognition is slightly impaired after STN-DBS and a strict selection of appropriate patients for surgery may be useful to prevent worsening of cognition.
Behaviour and mood
Various psychiatric disorders ranging from mood disorders – depression, mania, anxiety and apathy – to hallucinations and psychosis are seen in patients with PD on long-term medical management [Zgaljardic et al. 2003; Aarsland et al. 1999]. DRT, especially dopamine agonists, can cause or aggravate a variety of complex repetitive or reward-based behavioural disorders such as impulse control disorders, punding and dopamine dysregulation syndrome [Evans et al. 2009, 2004].
The neuropsychiatric outcome of bilateral STN-DBS is varied, with a broad range in reported rates of behavioural changes – depression 1.5–25%, attempted and completed suicide 0.5–2.9% and hypomania 4–15% [Voon et al. 2006]. Transient confusion and hypomania following bilateral STN-DBS has been reported, with improvement over 3–6 months [Voon et al. 2006; Takeshita et al. 2005]. Depressive symptoms have been shown to improve [Voon et al. 2006; Takeshita et al. 2005; Daniele et al. 2003], remain unchanged [Fasano et al. 2010; Porat et al. 2009; Witt et al. 2008] or worsen [Follet et al. 2010] after STN-DBS.
Suicide rates [Porat et al. 2009; Nazem et al. 2008; Soulas et al. 2008; Voon et al. 2008], anxiety, apathy [Porat et al. 2009; Drapier et al. 2006; Funkiewiez et al. 2004] and impulsivity [Bronstein et al. 2011] were found to worsen in most studies after STN-DBS. Few dopaminergic drugs are effective in improving mood in patients with PD. Pramipexole [Barone et al. 2010; Leentjens et al. 2009; Rectorová et al. 2003], ropinirole [Rektorová et al. 2008] and the newer MAO-B inhibitor safinamide [Borgohain et al. 2009] improve depression, while pergolide and other MAO-B inhibitors, for example selegiline, do not have significant antidepressant activity [Youdim and Bakhle, 2006].
Hallucinations, especially visual, and psychosis are a common complication in patients with PD. Older age, cognitive and visual disturbances can contribute to their emergence [Poewe, 2003]. Hallucinations and psychosis are aggravated by all dopaminergic and anticholinergic drugs [Poewe, 2003; Oertel et al. 2006; Parkinson Study Group, 2000; Rascol et al. 2000; Rinne et al. 1998]. Levodopa and dopamine agonists can cause many behavioural abnormalities such as impulse control disorders (ICDs), punding and dopamine dysregulation syndrome, which result in significant impairment in social function [Evans et al. 2009; Lawrence et al. 2007; Weintraub et al. 2010]. A recent review on the effect of bilateral STN-DBS showed that preoperative impulse control and related disorders may resolve or improve after STN-DBS, but these can also worsen or show no change at all. Moreover STN-DBS can also reveal or induce ICDs [Broen et al. 2011].
Studies comparing DBS and best medical treatment are shown in Table 1. Most studies have shown no significant change or improvement in scores of anxiety and depression [Wang et al. 2009; Weaver et al. 2009; Castelli et al. 2008; Witt et al. 2008; York et al. 2008; Smeding et al. 2006; Morrison et al. 2004]. Few studies have shown worsening of depression [Strutt et al. 2011; De Gasperi et al. 2006] and apathy [Kirsh-Darrow et al. 2011]. A controlled study showed increased overall psychiatric complaints (9%) in 99 patients who had STN-DBS compared with 3% in 36 patients on DRT [Smeding et al. 2006]. Two studies used gambling tasks to compare patients on dopaminergic agonists with patients who had STN-DBS [Lulé et al. 2011; Oyama et al. 2011]. In both studies, patients in the stimulator ‘on’ state were worse than in the ‘off’ state. Lulé and colleagues showed patients on medical treatment were worse compared with the STN-DBS group, while there was no significant difference in the study by Oyama and colleagues. This suggests that STN-DBS has a mild worsening of impulse control behaviour, but the concurrent decrease in dopaminergic medication may cause an overall reduction in impulse control abnormalities [Lulé et al. 2011].
In a direct comparison, bilateral STN-DBS was associated with worsening and bilateral GPi-DBS with improvement of depression [Follet et al. 2010]. This could be a manifestation of dopamine withdrawal syndrome and may be secondary to mesolimbic dopaminergic denervation or a direct effect of STN-DBS [Thobois et al. 2010]. In another head-to-head comparison trial, STN-DBS resulted in significant reduction in dopaminergic drug dosage compared with GPi-DBS, but was associated with more neuropsychiatric impairment [Moro et al. 2010].
Thus, overall, there may be a mild worsening of cognition and a risk of worsening of psychiatric disorders after STN-DBS. Reduction of behavioural disorders like ICDs by decreasing dopaminergic medication and other mechanisms [Ardouin et al. 2006] is also seen. GPi-DBS, however, seems to cause insignificant neuropsychiatric impairments.
Autonomic dysfunction
Autonomic dysfunction is common in patients with PD and can precede the onset of motor symptoms [Visser et al. 2004; Jost, 2003]. The association of autonomic disturbance has been recognized from the first description by James Parkinson (1817) and it increases with progression of disease, causing a major impact on quality of life [Jost, 2003].
Autonomic dysfunction in PD is thought to be predominantly due to central degeneration involving the ventrolateral medulla, dorsal motor vagal nucleus, nucleus tractus solitarius, periaqueductal gray matter in midbrain and descending sympathetic and parasympathetic pathways [Braak et al. 2004; Benarroch et al. 2000]. However, recent studies have demonstrated diffuse sympathetic denervation involving both central and peripheral neurons in patients with symptomatic autonomic disturbances [Goldstein et al. 2002; Orimo et al. 2002] and Lewy body pathology has also been found in peripheral autonomic neurons and ganglia [Minguez-Castellanos et al. 2007].
Cardiovascular
Cardiac autonomic disturbances are troublesome and especially orthostatic hypotension is a common problem. Levodopa and most antiparkinsonian medications can exacerbate orthostatic hypotension by varying levels [Bhattacharya et al. 2003; Lyytinen et al. 2001; Kujawa et al. 2000; Calne et al. 1960]. A recent Cochrane review on dopamine agonists demonstrated almost equal incidences of orthostatic hypotension with levodopa and dopamine agonists [Stowe et al. 2008].
Experimental studies in cats have shown that stimulation of the STN and globus pallidum externa produces tachycardia [Angyán, 1994] while stimulation of the GPi produces bradycardia [Angyán and Angyán, 1999]. Thornton and colleagues showed similar response in humans with an increase in heart rate and mean arterial pressure on STN stimulation while GPi stimulation showed no change in cardiovascular parameters [Thornton et al. 2002, Kaufmann et al, 2002]. Beneditti and colleagues showed that stimulation of the dorsal STN and/or the zona incerta resulted in constant autonomic changes, suggesting that they are involved in autonomic control, whereas the ventral STN and/or the substantia nigra reticulata are involved in associative/limbic-related autonomic activity and their stimulation resulted in varying autonomic changes [Beneditti et al. 2004].
The autonomic changes seen with STN-DBS may help in orthostatic hypotension by increasing heart rate, improving baroreceptor sensitivity and peripheral vasoconstriction, as noted by Stemper and colleagues [Stemper et al. 2006]. The effect may be secondary to an increased central sympathetic stimulation. Priori and colleagues also demonstrated an alteration in visual evoked potential, somatosensory evoked potential, sympathetic skin response and plasma renin level with DBS [Priori et al. 2001]. Other case series however did not find a similar change in heart rate, blood pressure and respiratory rate in patients with STN-DBS [Erola et al. 2006; Lipp et al. 2005].
Two controlled studies compared the effect of DRT and DBS on cardiovascular autonomic functions. Holmberg and colleagues compared 11 patients who had STN-DBS with eight patients on optimal medical therapy at baseline (preoperative) and at 1 year [Holmberg et al. 2005]. There was no difference in cardiovascular autonomic dysfunction in both groups in spite of a reduction in dose of dopaminergic medication in the STN-DBS group. The numbers in the study were small and the groups were heterogeneous with significantly shorter duration of disease in the pharmacotherapy group. Thus a small significant impact of STN-DBS may have been missed. Ludwig and colleagues compared the effect of levodopa with that of STN-DBS [Ludwig et al. 2007]. This was an immediate effect of a single dose of levodopa and the effect of STN-DBS compared with when it was switched off. While levodopa increased orthostatic hypotension, STN-DBS did not produce cardiovascular autonomic disturbances and only caused cutaneous vasoconstriction. The authors postulated that the effect of levodopa may have been secondary to a reduced sympathetic outflow caused by D2 receptor stimulation. The cardiovascular autonomic dysfunction in PD may be a combination of central and peripheral autonomic changes and the lack of effect of STN-DBS may stem from its inability to correct the peripheral component. An overall improvement in autonomic functions may be gained by the reduction of dopaminergic drugs after STN-DBS [Ludwig et al. 2007]. Larger randomized, controlled studies are needed to confirm the role of STN-DBS in orthostatic hypotension.
Genitourinary dysfunction
Urinary symptoms occur in 38–71% of patients with PD, the most common being nocturia, followed by urgency and frequency [Winge and Fowler, 2006]. The probable mechanism may be earlier perception of bladder sensation resulting in detrusor overactivity [Winge and Fowler, 2006]. This is improved by chronic DRT with a D1- and D2-receptor-mediated increase in volume at which patients recognize bladder filling [Brusa et al. 2007]. This effect of DRT is unclear and unpredictable in individual patients [Winge et al. 2004]. STN-DBS has been shown to have variable results. STN-DBS improves bladder symptoms with decreased detrusor hyperreflexia [Winge et al. 2007; Seif et al. 2004; Finazzi-Agrò et al. 2003] and increased bladder capacity [Shimizu et al. 2007; Herzog et al. 2006]. Herzog and colleagues postulated that this effect may be secondary to modulation of bladder afferents and central sensory processing.
There are very few studies on the effect of STN-DBS on other autonomic disorders. Sexual dysfunction is common in patients with PD. Both impaired function and excessive or distorted function have been described. Excessive or distorted function most frequently occurs in men as an adverse effect of DRT [Pfieffer, 2010]. Drugs have varied effects. Apomorphine, cabergoline, pergolide and levodopa have been shown to improve sexual impairment [Sakakibara et al. 2010]. Dopamine agonists can cause hypersexuality [Klos et al. 2005]. STN-DBS has been shown to improve sexual wellbeing in a cohort of 31 patients 9–12 months after surgery [Castelli et al. 2004] with a few reports of hypersexuality, especially in patients with mania [Roane et al. 2002; Romito et al. 2002].
Gastrointestinal dysfunction
Chronic constipation, nausea, dribbling of saliva, vomiting, dyspepsia, gastroparesis and dysphagia are very common, seen in 80% of patients with PD [Olanow et al. 2009]. A recent meta-analysis noted an increase in gastrointestinal symptoms of nausea, vomiting, dry mouth and constipation with adjuvant DRT compared with levodopa [Stowe et al. 2011]. Levodopa augmented rectal contraction, lessened paradoxical sphincter contraction and reduced constipation in a group of 19 patients [Tateno et al. 2011]. Improvement in constipation, excessive salivation and deglutition after STN-DBS has been noted in two studies [Ciucci et al. 2008; Zibetti et al. 2007].
Thermoregulation and sweating
Thermoregulation is impaired in patients with PD and sweating abnormalities can be troublesome. Abnormal sensations of heat or cold, impaired sweating responses, and hypothermia can all occur [Olanow et al. 2009]. In a study done by Swinn and colleagues, thermoregulatory abnormalities were found in 64% of patients with PD compared with only 12% of controls [Swinn et al. 2003]. Severe drenching sweats occur commonly as an end-of-dose ‘off’ phenomenon in patients with advanced disease and these may be satisfactorily controlled with adequate DRT [Pursiannen et al. 2007]. STN-DBS has been reported to ameliorate sweating during ‘off’ periods in patients with by 66%, 6 months after surgery [Trachani et al. 2010] and markedly reduce the fluctuations [Witjas et al. 2007]. The effect of DBS on sweating abnormalities occurring during the dopaminergic drug ‘on’ state has not been studied as yet.
Based on the current literature, STN-DBS may have a positive effect on cardiovascular autonomic disturbances and may improve orthostatic hypotension through reduction of DRT. There is some suggestion that STN-DBS may improve gastrointestinal, genitourinary and thermoregulatory symptoms more than medical therapy, but controlled studies are required.
Sleep
Sleep disturbances affect 74–98% of patients with PD [Amara et al. 2011]. These include insomnia, sleep fragmentation with early morning wakening, excessive daytime sleepiness, sleep attacks, rapid eye movement sleep behavioural disorder, nightmares and parasomnias, restless legs syndrome, periodic limb movements of sleep and akathisia [Amara et al. 2011]. Sleep disturbances in patients with PD are multifactorial. Degeneration of dopaminergic and nondopaminergic neurons in the brainstem causing specific sleep disorders, parkinsonian motor dysfunction, dyskinesias, pain, nocturia, dopaminergic and nondopaminergic medications, all contribute to sleep disturbances [Olanow et al. 2009]. In a recent study, the severity of sleep disturbance correlated positively with disease severity, UPDRS motor scores, levodopa dose, severity of rigidity, and severity of bradykinesia [Ziemssen and Reichmann, 2007].
Drugs have a complex effect on sleep disorders. They improve sleep disorders by improving nocturnal mobility and quality of sleep [Pahwa et al. 2007; Morgan and Sethi, 2006; Reuter et al. 1999; Askenasy and Yahr, 1985]. Dopaminergic agonists are also the treatment of choice for restless legs syndrome, and dramatic benefits have been observed with bedtime doses of numerous dopamine agonists, including pergolide, pramipexole, ropinirole, cabergoline and rotigotine [Vignatelli et al. 2006; Winkelman et al. 2006; Stiasny-Kolster et al. 2004; Walters et al. 2004]. However, at higher doses dopaminergic drugs, including levodopa and dopaminergic agonists, can cause sleep fragmentation and daytime somnolence, resulting in sleep attacks and injuries, and worsening restless legs syndrome by augmentation [Olanow et al. 2009; Micallef et al. 2009; Ferreira et al. 2000; Schapira, 2000; Frucht et al.1999; Allen and Earley, 1996].
Bilateral STN DBS-has been found to improve both objective polysomnographic measures of sleep and subjective sleep quality in several studies. Decreased awake state after sleep onset, improved nocturnal mobility, improvement in restless legs syndrome, increased continuous sleep time and sleep efficiency were seen after bilateral STN-DBS [Chahine et al. 2011; Zibetti et al. 2007; Cicolin et al. 2004; Arnulf et al. 2000]. The improvement in total sleep time, patient-reported sleep problems and early morning dystonia was seen even at 24 months after bilateral STN-DBS [Lyons and Pahwa, 2006]. However, excessive daytime somnolence did not improve with bilateral STN-DBS [Lyons and Pahwa, 2006]. The effect of GPi-DBS on sleep has not been well elucidated. In a recent comparative study, subjective improvement in sleep was noted in patients who underwent bilateral GPi-DBS at 36 months post surgery that was comparable to those who had bilateral STN-DBS [Volkmann et al. 2009].
Hjort and colleagues compared the effect on sleep of 3 months of STN-DBS in 10 patients with medical treatment in 10 patients using a visual analogue scale – Parkinson’s disease sleep scale [Hjort et al. 2004]. There was significant improvement in nocturnal motor symptoms and overall sleep quality while there was no effect on nocturia, sleep fragmentation and excessive daytime sleepiness. This suggests that STN-DBS probably acts only by reducing motor symptoms and does not have a significant central sleep modulation [Hjort et al. 2004].
Sensory changes
Olfactory loss is one of the first symptoms to appear in PD [Olanow et al.2009]. In a cohort of 15 patients, odour identification improved significantly at 6 and 12 months after STN-DBS [Guo et al. 2008]. This improvement was noted in the stimulator ‘on’ state only. STN-DBS improves neuronal activity in striatum and the orbitofrontal cortex and may result in olfactory recovery [Guo et al. 2008].
There is a change in sensory perception in patients with PD. Pain is a common complaint, detected in 70–80% of patients [Beiske et al. 2009] and is worse in the ‘off’ state [Nebe and Ebersbach, 2009]. Other sensory symptoms such as numbness, itching, tingling or thermal sensations are also seen, though less frequently than pain [Gierthmühlen et al. 2010].
Levodopa has been shown to improve sensory symptoms by the increasing pain threshold [Gerdelat-Mas et al. 2007; Slaoui et al. 2007; Brefel-Courbon et al. 2005]. Similarly, STN-DBS has been shown to reduce pain intensity and improve pain/sensory fluctuations and nonspecific sensory complaints compared with the preoperative state in various studies [Gierthmühlen et al. 2010; Kim et al. 2008; Witjas et al. 2007; Zibetti et al. 2007]. Improvement in thermal threshold has been demonstrated in a recent study after DBS [Maruo et al. 2011]. There are no head-to-head comparison trials of DBS and best medical treatment in sensory modulation. A recent trial compared the effect of levodopa with the stimulator in the ‘off’ state and the stimulator in the ‘on’ state in 15 patients, 6 months after STN-DBS [Gierthmühlen et al. 2010]. Patients subjectively felt that pain responded to levodopa and had reduced intensity of pain after STN-DBS compared with before STN-DBS. Both STN-DBS and levodopa had no effect on objective pain sensitivity. On evaluation of temperature, STN-DBS improved thermal detection thresholds while levodopa had no effect.
To summarize, both levodopa and STN-DBS improve pain perception and reduce pain intensity. STN-DBS also improves olfaction and thermal detection thresholds compared with medication. There is a need for large controlled trials to verify the actual effects.
Overall nonmotor symptoms
The literature is scant about the effect of medication or DBS on overall score of all nonmotor symptoms in patients with PD (Table 3). A small study did not find any significant effect of DRT on overall nonmotor symptom score [Kim et al. 2009]. But the study was done on de novo detected patients with PD and the effect of DRT on nonmotor symptoms may be more evident later in the course. Two recent studies assessed the effect of STN-DBS on nonmotor fluctuations using comprehensive scales, including cognitive, behavioural, dysautonomic and sensory symptoms before and a year after surgery [Nazarro et al. 2011; Witjas et al. 2007]. Nazarro and colleagues demonstrated an improvement in Nonmotor Symptoms Assessment Scale score, with the best improvement in autonomic functions. Witjas and colleagues studied the effect of DBS on nonmotor fluctuations. Pain and sensory fluctuations showed the best response to STN-DBS (84.2%). A good response was noted in dysautonomic and cognitive fluctuations (60%) along with a marked reduction in the incapacitating symptoms of drenching sweats and akathisia [Witjas et al. 2007].
Nonmotor symptoms affect patients’ quality of life. The final impact of treatment can be measured using health-related quality of life (HRQoL) scales. The scales take into account both motor and nonmotor improvements. Two randomized trials compared the effects of DRT and DBS on HRQoL using the 39-item Parkinson’s Disease Questionnaire as a primary endpoint [Williams et al. 2010; Deuschl et al. 2006]. There was a significantly better outcome in the DBS group at the end of 6 months [Deuschl et al. 2006] and 12 months [Williams et al. 2010]. There was significantly increased improvement in domains of mobility, activities of daily living, stigma and bodily discomfort in both studies, while improvement in emotional wellbeing was noted by Deuschl and colleagues. There was no difference in the domains of cognition, communication and social support between the two groups.
Further research on the effect of pharmacological therapy or DBS on nonmotor symptoms in patients with PD can help us to understand the pathophysiology of the disease and treat patients with a holistic approach.
Conclusions
Nonmotor symptoms occur throughout the course of PD. Bilateral STN-DBS or GPi-DBS as well as DRT have significant effects on nonmotor symptoms. On comparing DRT with DBS, the latter is more effective in reducing sensory, sleep, gastrointestinal and urological symptoms. Bilateral STN-DBS or GPi-DBS have varying effects on cognitive, behavioural and cardiovascular autonomic disturbances, with mild worsening in cognition noted with STN-DBS. STN-DBS may have a beneficial effect on cardiovascular autonomic and some behavioural disorders by decreasing the dopaminergic dose in patients. Considering the effect of DBS on both motor and nonmotor symptoms, surgery is a safe and highly effective therapy in selected patients. As the motor effects of STN-DBS and GPi-DBS are similar, nonmotor symptoms may determine the target choice in surgery of future patients.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors declare no conflicts of interest in preparing this article.