
Abstract
In recent years, there has been a paradigm shift in the treatment of multiple sclerosis (MS) owing to the approval of a number of new drugs with very distinct mechanisms of action. All approved disease-modifying drugs primarily work directly on the immune system. However, the identification of an ‘optimal choice’ for individual patients with regard to treatment efficacy, treatment adherence and side-effect profile has become increasingly complex including conceptual as well as practical considerations. Similarly, there are peculiarities and specific requirements with regard to treatment monitoring, especially in relation to immunosuppression, the development of secondary immune-related complications, as well as the existence of drug-specific on- and off-target effects. Both classical immunosuppression and selective immune interventions generate a spectrum of potential therapy-related complications. This article provides a comprehensive overview of available immunotherapeutics for MS and their risks, detailing individual mechanisms of action and side-effect profiles. Furthermore, practical recommendations for patients treated with modern MS immunotherapeutics are provided.
Introduction
Change of treatment paradigms in multiple sclerosis
Multiple sclerosis (MS) is a chronic immune-mediated inflammatory demyelinating disease of the central nervous system (CNS) that primarily affects young adults with a mean age of onset between 20 and 40 years of age. Although there is still no cure available and no clearly accepted disease pathogenesis, the long-term prognosis of patients with relapsing forms of the disease has improved considerably over the last decade. This is largely due to the regulatory approval of a range of highly active immunotherapeutic drugs, commencing with the first monoclonal antibody natalizumab in 2006.
As a consequence of improved treatment options and, in particular, the availability of highly effective therapies, the scope for patient- and disease-activity-centred treatment decisions has broadened. In parallel, there has been a change in the perception of what constitutes treatment success. Whereas 15 years ago, successful treatment was defined by a reduction in relapse rate and limited increase in inflammatory magnetic resonance imaging (MRI) lesions, treatment now targets ‘no evidence of disease activity’ (NEDA; Box 1). Furthermore, long-term data from clinical trials underscore the relevance of early immune therapy for reduction of and impact on disease progression and prevention of disability accrual. Therefore, MS should be treated as early as possible, and treatment efficacy should be monitored continuously.
NEDA-3 concept.

MRI, magnetic resonance imaging; NEDA, no evidence of disease activity.
However, the emergence of highly effective treatment options for MS has been accompanied by an increasingly complex array of adverse effects, the management of which requires extensive knowledge of each individual treatment’s mechanism of action and potential side effects, especially with regard to immune compromise following chronic immune therapy. Here, we review the risks and side-effect profiles associated with modern MS immunotherapies and provide practical monitoring recommendations for their use.
General principles and considerations for MS immunotherapies
Inductive reasoning would suggest that the therapies found to be effective in MS are good at regulating or inhibiting immunological responses to unknown disease target(s) in the CNS. The ideal MS therapy would selectively restore failed immune tolerance without impeding other parts of the immune system. However, we have at best a limited understanding of how current therapies alter MS pathophysiology, and none of the existing therapeutic approaches has this degree of selectivity for MS. Prevailing treatment strategies modulate the immunological response using general or more selective immunosuppressive approaches, specific regional strategies that target the CNS, or by altering immune cell regulation (Table 1).
Categories of immune therapies in MS.

Ab, antibody; APC, antigen-presenting cells; BDNF, brain-derived neurotrophic factor; CSF, cerebrospinal fluid; DHODH, dihydroorotate dehydrogenase; GA, glatiramer acetate; IFN, interferon; IL, interleukin; mAb, monoclonal antibody; MHC, major histocompatibility complex; NK, natural killer; VLA4, very late antigen 4/ VCAM, vascular cell adhesion molecule 1.
Most immune therapies for MS are associated with immunosuppression, which is typically defined as an inhibition of the adaptive immune system. 1 This definition refers to both short-term/intermittent (pulsed, induction) and long-term persistent immunosuppression (chronic, maintenance). A practical way for a drug to be considered an immunosuppressant is whether the observed effects include one or more of: (1) lymphopenia or functional lymphocyte impediment; (2) opportunistic or increased infections; (3) association with secondary malignancies known to be driven by underlying infections; and (4) reduced antibody response to vaccines. Importantly, many genetic and some acquired immunodeficiency states are also associated with increased autoimmunity, simplistically this may be a suppression of regulatory effects.2,3 The practical dangers of this were illustrated in the increase in inflammatory skin and brain disease with daclizumab.
Although it may seem unnecessary to state, it is important that the disease being treated is indeed MS. One fatal case of a patient with progressive multifocal leukoencephalopathy (PML) that arose as a consequence of natalizumab treatment showed no evidence of MS after post mortem examination. 4 Less egregiously, there are situations where MS may be difficult to distinguish from other CNS inflammatory disorders such as neuromyelitis optica spectrum disease (NMOSD), myelin oligodendrocyte glycoprotein (MOG) spectrum disorders, sarcoidosis or CNS affection within systemic immune disorders [e.g. systemic lupus erythematosus (SLE)].
The ideal time to consider risk mitigation for MS immunotherapies is right from the beginning of diagnosis. This can include practical measures such as fulfilment of local vaccination recommendation and selective vaccination for infections including varicella zoster virus (VZV) and hepatitis B. Checking for other relevant infections that might require treatment such as latent tuberculosis (TB), avoidance of osteopenia with vitamin D and appropriate sun exposure and ensuring cervical cancer screening is up to date are also suggested. Use of a quick, standardized screening checklist (e.g. www.immunosuppressionscreen.net) may assist in the initial assessment of patients. 5
Time is also the source of uncertainty for long- and very long-term risks of immunotherapies. In particular, the two-year time course of most randomized controlled trials (RCTs) may be enough time to determine the risk of common bacterial infections. However, it is not sufficient to determine the critical risks of indolent infections, PML with natalizumab being a salient example.6,7 The long-term fear is the possibility of an increased risk of malignancy, which has been shown clearly with very long-term follow up of iatrogenic immunosuppression associated with solid organ transplant or infectious immunosuppression due to HIV/AIDS. 8 The data is less clear than in fields such as rheumatoid arthritis (RA), but the studies are constrained by generally short follow-up and exposure to multiple medications. The systemic effects on cardiovascular risk are less well appreciated but are substantial, particularly with diseases such as SLE or RA. 9 Even in MS, corticosteroid use and relative immobility may contribute to cardiovascular disease, although infection appears to be the prevalent cause of death in MS. 9
Thus, derisking MS immune therapy is a critical aspect and includes considerations for assessments at (1) baseline, (2) during infusion/immune reconstitution and (3) monitoring (Table 2).
Derisking immune therapy.

ASI, antibody-specificity Index; CSF, cerebrospinal fluid; DMT, disease-modifying treatment;
DNA, deoxyribonucleic acid; FBC, full blood count; HIV, human immunodeficiency virus; IRTS, immune reconstitution therapies; LFT, liver function test; LP, lumbar puncture; MRI, magnetic resonance tomography; PJP, Pneumocystis jiroveci pneumonia; PML, progressive multifocal leukoencephalopathy; TB, tuberculosis; TFT, thyroid function test; U&E, urea & electrolytes; VZV, varicella zoster virus.
Finally, the risks to a foetus are another important consideration in MS, which has a disproportionate effect on women of childbearing age (Table 3). The risks to the mother from un(der)treated MS should also not be ignored. Education about different treatments and the timing of planned fertility is important in many modern treatment paths. Breast-feeding, loss of fertility and male fertility are also considerations with some MS drugs.
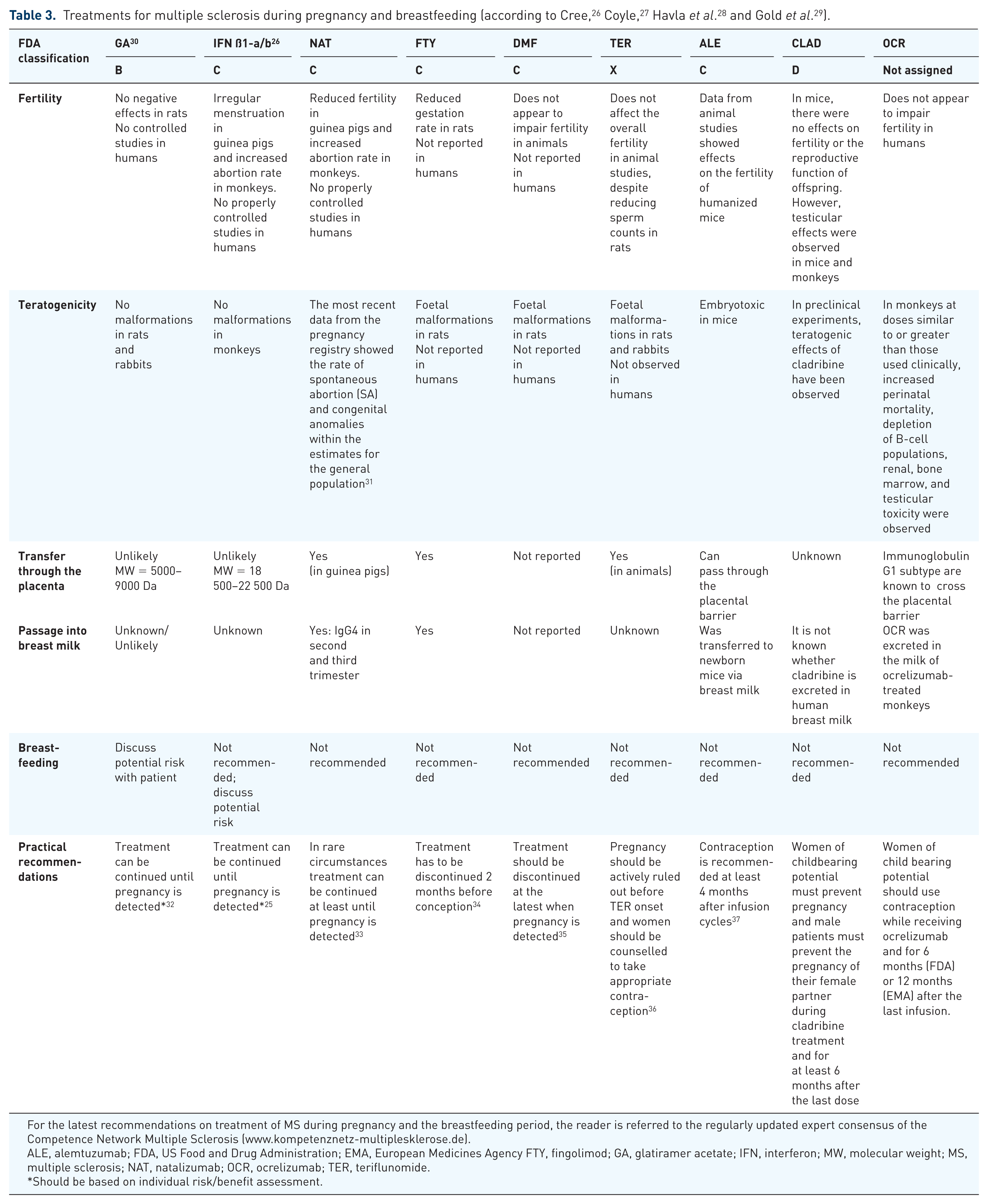
For the latest recommendations on treatment of MS during pregnancy and the breastfeeding period, the reader is referred to the regularly updated expert consensus of the Competence Network Multiple Sclerosis (www.kompetenznetz-multiplesklerose.de).
ALE, alemtuzumab; FDA, US Food and Drug Administration; EMA, European Medicines Agency FTY, fingolimod; GA, glatiramer acetate; IFN, interferon; MW, molecular weight; MS, multiple sclerosis; NAT, natalizumab; OCR, ocrelizumab; TER, teriflunomide.
Should be based on individual risk/benefit assessment.
Risks and risk management for specific MS therapies
Interferon beta 1a, Interferon beta 1b (Betaferon®/Betaseron®; Extavia®; Avonex®; Rebif®; Plegridy®)
Interferon beta (IFNβ) influences immune functions such as increased production of anti-inflammatory cytokines that shift the cytokine network, 10 altered immune cell trafficking across the blood–brain barrier,11,12 modulation of the antigen-presenting function of dendritic cells, and promotion of anti-inflammatory B-cell functions.13,14 There is no increased risk of infections and neoplasia during IFNβ treatment and efficacy of vaccinations is not impaired. 15 Some patients experience changes in immune cell composition in the peripheral blood (mainly mild leukopenia or lymphopenia). Interestingly, the risk for these changes decreases with treatment duration. 16 A severe but rare complication of IFNβ treatment is the development of thrombotic microangiopathy, which is associated with thrombocytopenia, haemolytic anaemia and microvascular occlusions.17,18 It has been suggested that this is dose and time dependent (high dose, >5 years). Furthermore, liver enzyme elevations can be observed and toxic or autoimmune hepatitis with acute liver failure has occurred very rarely. 19 An increased prevalence of autoimmune thyroid disease has been noticed, particularly in the first year of IFNβ therapy. 20 Owing to its immunogenic nature as a modified protein, application of IFNs can induce development of neutralizing antibodies, which might impair drug efficacy.21,22 Observational studies have not shown an increased risk for foetal malformation, although birth weight was reduced in animals.23,24
Practical monitoring recommendations
A summary of practical monitoring recommendations is given in Table 4. Particular caution is advised in patients with preexisting suicidal depression and epilepsy. Before and during treatment, differential blood and platelet count and liver enzymes should be obtained. During treatment, liver enzymes and creatinine should be monitored periodically. Monitoring of possible nephropathy, liver disease and myelosuppression can be necessary during treatment. In patients with thyroid dysfunction, regular thyroid function tests are recommended. Monitoring of blood pressure and other signs and symptoms of nephrotic syndrome, thrombotic microangiopathy, haemolytic–uremic syndrome (HUS) and, especially in patients with preexisting cardiac disease, possible clinical worsening must be considered. Vaccination is possible during therapy with IFNβ. During pregnancy, therapy with IFNβ has to be terminated; however, it can be continued until pregnancy is detected (Table 3). 25
Risks and monitoring of MS immune therapies.

APC, antigen-presenting cells; BDNF, brain-derived neurotrophic factor; CIS, clinically isolated syndrome; CRP, C-reactive protein; CSF, cerebrospinal fluid; DHODH, dihydroorotate dehydrogenase; ECG, electrocardiogram; GFR, glomerular filtration rate; HPV, human papillomavirus; ITP, idiopathic thrombocytopenic purpura; JCV, John Cunningham virus; PML, progressive multifocal leukoencephalopathy; PPMS, primary progressive multiple sclerosis; RRMS, relapsing–remitting multiple sclerosis; TSH, thyroid-stimulating hormone; TTE, transthoracic echocardiogram; ULN, upper limit of normal; VLA4, very late antigen 4/ VCAM, vascular cell adhesion molecule 1; VZV, varicella zoster virus.
Glatiramer acetate (Copaxone®) and generic compounds (Clift®, Perscleran®, Glatopa®)
Glatiramer acetate (GA) and its generic compounds are a mixture of synthetic polymers consisting of glutamate, lysine, alanine, and tyrosine that competes with myelin antigens for presentation to T cells. From the point of immune surveillance, this mechanism of action does not involve nonspecific downmodulation of pathogen-specific effector T-cell responses. There is no increased risk of infections and neoplasias observed in GA-treated patients. Occasionally patients develop swelling of the lymph nodes, potentially owing to transient activation of antigen-specific immune responses elicited by the antigenic peptide mixture. 38 In some cases, changes in peripheral blood cell composition can be observed encompassing both leukocytosis or leucopenia; additionally, thrombocytopenia can occur. 39 Furthermore, liver enzyme elevations can occur occasionally. 40 Patients have to be informed that lipoatrophy may occur with long-term administration of GA. 41 With respect to pregnancies, no increased risk for malformations was seen in preclinical experiments or in humans.30,42
Practical monitoring recommendations
See Table 4 for a summary of practical monitoring recommendations. Before treatment, differential blood count, liver enzymes and creatinine should be obtained. 32 During treatment, kidney function should be monitored in patients with chronic kidney disease. 43 Vaccinations are possible during immune therapy with GA. Treatment can be continued until pregnancy is detected, however, during pregnancy, GA therapy should be terminated 44 (Table 3). It should be noted that in some countries including Australia, GA treatment can be continued during pregnancy.
Dimethyl fumarate (Tecfidera®)
The mode of action of dimethyl fumarate (DMF) has not been fully elucidated, but may include anti-inflammatory and cytoprotective aspects reported to be mediated via the nuclear factor (erythroid-derived2)-like transcriptional pathway, which is involved in the cellular response to oxidative stress. 45 However, a recent study showed that the anti-inflammatory activity of DMF may occur through alternative pathways, independent of Nrf2. 46 DMF causes pronounced lymphopenia below 500/µl in 4–6% of patients that may persist for several weeks or months.47,48 DMF use is associated with gastrointestinal (GI) side effects, such as abdominal pain, nausea, diarrhoea and dyspepsia in approximately 15% of patients. 49 One patient was observed with eosinophilic gastroenteritis 2 months after DMF initiation. 50 Therefore, careful clinical evaluation of protracted and severe GI symptoms should be considered. 50
Initial reports suggested that overall infection rates are not increased and vaccination responses are not impaired. However, since approval, several cases of fumaric acid-associated PML have been described (see Table 5). Cases of PML in MS patients receiving DMF might be differentiated from cases associated with other fumaric acid formulations.51–54 Whereas most DMF-associated PML cases exhibited prolonged lymphopenia, one patient showed only slightly reduced lymphocyte counts. 55 In the ENDORSE study (ClinicalTrials.gov identifier: NCT00835770), an ongoing 12-year extension study of the pivotal phase III studies (DEFINE/CONFIRM), patients new to DMF had decreases in lymphocyte counts (6–9% below 500/µl) and this remained stable in those continuing DMF treatment (7–8% below 500/µl). 56 However, in a another cohort, a substantial proportion of DMF-treated MS patients (28%) displayed lymphocyte counts below 500/µl after more than 1 year of treatment, 57 indicating that for unknown reasons, the risk of lymphopenia might increase over time. One important common denominator of PML associated with DMF is age (likely related with factors associated to immune senescence): all patients were ⩾50 years. Of note, the potential PML risk in patients who have switched from natalizumab to DMF cannot be estimated at present. In the ENDORSE study, excepting one fatal case of PML, the interim results of the ENDORSE extension study did not show an increased incidence of opportunistic infections. 58
PML risk under immunomodulatory therapies.

EMA, European Medicines Agency; MS, multiple sclerosis; PML, progressive multifocal leukoencephalopathy.
Although no clinically significant DMF-associated hepatotoxicity was reported in clinical trials, cases of liver injury associated with DMF treatment have been described recently.62,63 Therefore, the prescribing label for DMF (Tecfidera®) has been updated to include a warning of potential liver injury that could require hospitalization.
Practical monitoring recommendations
See Table 4 for a summary of practical monitoring recommendations. DMF should not be used in patients suffering from severe active or chronic infections, severe GI infections, hepatic or kidney diseases. Furthermore, the substance should not be used in patients with active cancer.
Lab testing of differential blood count, liver enzymes, kidney function and brain MRI should be obtained before treatment initiation. Kidney function should be monitored after 3 and 6 months, and every 6 months afterwards. Differential blood counts should be performed every 8–12 weeks during treatment duration. In the case of a 6-month persistent lymphopenia below 500/µl, DMF treatment should be reconsidered. In the case of persisting leukopenia, we recommend increased vigilance for opportunistic infections. However, the management of lymphopenia (above 500/μl, but below 800–1000/μl, and especially in older patients) is less certain, particularly in light of the recently published PML case with lasting persistent low-grade lymphopenia. 55 It may be advisable to closely monitor blood counts in those patients every 4 weeks and remain clinically vigilant for potential signs of opportunistic infections. Based on recent publications illustrating distinct effects of DMF treatment on different lymphocyte subpopulations, 64 flow cytometric quantification of lymphocyte subsets might help detect significant, early reductions in relevant T-cell subsets, especially in those patients exhibiting low-grade lymphopenia on routine blood counts. Of note, no data exist with regard to DMF and John Cunningham virus (JCV) antibody status and antibody titer; hence, routine testing of JCV titer cannot be recommended at this time. Vaccinations are possible during immune therapy with dimethyl fumarate. Treatment should be discontinued at the latest when pregnancy is detected 29 (Table 3).
Teriflunomide (Aubagio®)
Teriflunomide acts as a selective and reversible inhibitor of the mitochondrial enzyme dihydroorotate dehydrogenase (DHODH), which is expressed in lymphocytes. 65 TEMSO and TOWER phase III clinical studies revealed a slight but notable decrease in peripheral lymphocyte counts of approximately 15%.66,67 The incidence of infections was comparable between placebo- and teriflunomide-treated patients in both studies. However, there were several cases of unusual or opportunistic infections such as Klebsiella-induced sepsis, intestinal TB and Gram-negative sepsis.66,68 Interestingly, rare cases of significant neutropenia (below 900/μl) were also reported. 69 It is hence conceivable that individuals with an enhanced vulnerability towards teriflunomide-induced neutropenia might be at risk for severe infections. However, in the described cases, pre-infection levels of neutrophils were not monitored unfortunately. So far, two cases of PML 70 were reported in patients treated with leflunomide, the precursor of teriflunomide used for treatment of RA, and there was a very recent report of PML in an MS patient treated with teriflunomide for 2.5 months, which occurred however approximately 8 months after natalizumab treatment cessation. 61 The recently presented data from the Teri-PRO study showed a real-world safety profile consistent with that seen in the clinical development program. 71
Teriflunomide is metabolized in the liver and can cause relevant elevations of liver enzymes in the first months following teriflunomide initiation.66,67 For unknown reasons, there have been some cases that exhibited elevated pancreatic enzymes. Moreover, a slight but notable blood pressure elevation has also been described. There was a single case of toxic epidermal necrolysis 72 and interstitial lung disease (ILD) has been described during postmarketing surveillance. In preclinical experiments, teriflunomide was embryotoxic in two different species. In humans, so far there has been no reported increase in malformations or abortions (Table 3).73,74
Teriflunomide and leflunomide have effects on a range of enzymes important for drug metabolism, including several CYP enzymes, OAT3 and BCRP. 75 The practical importance of this in most cases is uncertain, but particular caution is recommended in combination with methotrexate, the effect of which may be increased and may contribute to the risk of ILD seen independently with both drugs; 76 with statins, in particular rosuvastatin, in which dose limitation to 10 mg daily is recommended; and with warfarin, in which dose adjustment may be needed.
Practical monitoring recommendations
See Table 4 for a summary of practical monitoring recommendations. Teriflunomide should not be used in patients suffering from severe active or chronic infections (HIV, hepatitis B and C, TB) as well as in case of severe hepatic and kidney disease. 36 Before treatment onset, severe active or chronic infections such as TB, virus hepatitis or HIV infection should be ruled out. Lab testing of differential blood, platelet count and liver enzymes should be obtained and blood pressure should be documented.
During treatment, liver enzymes, differential blood (in case of infections) and blood pressure should be periodically monitored. In case of reproducible liver enzyme elevations [2–3× upper limit of normal (ULN)], liver enzymes should be monitored weekly. If liver enzymes are repeatedly above 3× ULN, treatment should be discontinued and further diagnostic procedures applied (e.g. liver sonography and differential diagnostics). Teriflunomide should be actively eliminated by forced interruption of enterohepatic circulation. New onset or worsening pulmonary symptoms suggesting ILD, such as persistent cough and dyspnea, may be a reason for discontinuation.
Signs and symptoms of myelosuppression, Stevens Johnson syndrome, toxic epidermal necrolysis, DRESS (drug reaction with eosinophilia and systemic symptoms syndrome) and peripheral neuropathy should be considered given the reported cases of these problems with leflunomide in RA. Under therapy with teriflunomide, live-attenuated vaccines should be avoided. However, administration of inactivated vaccines is possible. 77 Pregnancy has to be actively ruled out before teriflunomide onset and women need to be counselled to take appropriate contraception. In case a pregnancy is planned, teriflunomide has to be discontinued, followed by forced interruption of enterohepatic circulation (via cholestyramine or activated charcoal) and subsequent confirmation of low teriflunomide plasma levels (Table 3).
Natalizumab (Tysabri®)
Natalizumab is a monoclonal antibody directed against the α4 chain of the α4β1 integrin (VLA-4).78,79 Binding of the antibody to the VLA-4 molecule interferes with immune cell adhesion to endothelial cells, for example, at the blood–brain barrier, thus limiting immune cell invasion into the CNS. 80 The most important adverse event in the treatment with natalizumab is the occurrence of PML. Whereas the event is comparatively rare (Table 5), 7 it is fatal in up to 20% of cases and results in permanent neurological residua in many or most others. There is currently no established treatment available other than drug withdrawal, which is frequently combined with plasma exchange.
In keeping with the mechanism of action, a mild increase in peripheral leukocyte/lymphocyte counts and a left-shift have been described.81,82 Occasionally, a rise in CD34-positive stem cells, nucleated red blood cells and B cells occurs. These rather mild changes indicate that PML risk monitoring cannot rely on testing of blood counts, and even detailed immune phenotyping using flow cytometry is not yet able to reveal any changes that predispose PML development.
Owing to its immunogenic potential, development of persisting neutralizing antibodies against natalizumab has been observed in about 6% of patients and can be associated with persistent infusion-related adverse events as well as reduced clinical efficacy. 83
Acute retinal necrosis (ARN), a fulminant viral infection of the retina has been observed in natalizumab-treated patients. 84 There is no generally increased risk for developing malignancies under natalizumab, suggesting that immune surveillance is not generally compromised, but there has been a number of CNS and GI lymphomas, which are areas in which natalizumab impairs immune surveillance. 85 In case of mild classical infections, natalizumab treatment can be continued. However, in case of moderate or severe infection, treatment should be postponed and appropriate treatment of infections should be initiated. Recently, recurrent natalizumab infusion-associated aseptic meningitis was reported. 86
Practical monitoring recommendations
See Table 4 for a summary of practical monitoring recommendations. Natalizumab should not be used in patients suffering from severe active or chronic infections or those who have a history of malignancy. During the first 6 months of therapy, control of liver enzymes should be performed periodically. In case of severe liver damage, natalizumab should be permanently ceased. Prior to every infusion, infections have to be clinically excluded, eventually supported by blood counts. Infusion-related adverse drug reactions must be considered and might prompt testing for presence of neutralizing antibodies. Under therapy with natalizumab, life-attenuated vaccines have to be avoided, and the efficacy of inactivated vaccines may be compromised.
There is an increasing PML risk with continued treatment duration of natalizumab.7,87,88 Therefore, all patients should be reevaluated and reconsented to continue natalizumab treatment every 6 months. JCV antibody positive patients treated for more than 18 months need to be closely monitored both clinically (every 3 months) and by MRI (every 3–6 months) with a special focus on PML-related signs and symptoms (e.g. aphasia, apraxia, cognitive impairment). JCV antibody positive patients who remain on therapy with natalizumab should be reassessed every 6 months to facilitate the most accurate PML risk assessment. A neuroradiologist experienced in PML diagnostics should perform MRI evaluation and include diffusion weighted imaging (DWI) and post-contrast sequences. 89 In very rare instances, the transmission of natalizumab-associated PML has been suggested as a possibility90–92 and ‘high-risk’ patients should therefore avoid direct contact with active PML patients. 91 Furthermore, signs and symptoms of herpes simplex, VZV encephalitis, virus-related retinal necrosis, cryptococcal meningitis and other opportunistic infections must also be considered during natalizumab treatment. The inclusion of the JCV-antibody index can provide additional stratification of PML risk, because patients with index values <0.9 appear to be in the same risk category as patients with negative JCV antibody status. 6 JCV antibody negative patients should be assessed for JCV seroconversion every 6 months. The risk of seroconversion under natalizumab treatment is higher than in the average population and in MS patients. 93 Most seroconversions give a rise in JCV antibody index values above 0.9, which can be considered “true” seroconversion as a result of JC infection. 94 Other biomarkers for risk assessment under natalizumab have been suggested, especially the expression of L-selectin on CD4+ T lymphocytes. 95 Whereas its association with PML risk and JCV serology has been shown by several groups,96–99 its use in clinical routine practice is limited by the availability of the assay but also by lack of regulatory approval. CD62L was first published as a potential risk biomarker in 2013 95 and the biological connections between natalizumab-treatment, JCV serology and CD62L in its cellular 98 and soluble/shedded form 96 have repeatedly been shown. However, retrospective reproduction as a PML risk biomarker was successful in some cohorts, 97 but not in others, 100 depending on assay conditions. Therefore, the biomarker is considered exploratory and currently measured prospectively in studies101,102 to assess its validity, sensitivity and specificity.
In general, natalizumab is contraindicated during pregnancy but in rare circumstances treatment can be continued at least until pregnancy is detected 33 (Table 3).
Fingolimod (Gilenya®)
Fingolimod is a functional antagonist of the sphingosine-1-phosphate receptor that sequesters lymphocytes in the lymph nodes. In general, the risk of infections with fingolimod is slightly increased. In the phase III TRANSFORMS study, two fatal cases of VZV and HSV infections occurred in subjects taking a higher dose of fingolimod. 103 Furthermore, in post-marketing analysis of 54,000 patient years, there was an increased incidence of VZV reactivations. However, the risk for severe, unusual or even fatal VZV manifestations was not increased. 104 It is conceivable that due to interference with lymphocyte trafficking, local immune surveillance of neural cells harbouring VZV viruses is compromised, resulting in VZV reactivation.105–109 Several cases of PML have also been described in fingolimod-treated patients without previous treatment with natalizumab (Table 5). In addition, there were isolated cases of opportunistic fungal cryptococcosis110,111 and a single case of leprosy. 112
Licensing studies showed an increased rate of local skin tumours, especially basal cell carcinomas (13 cases) and melanomas (6 cases). Further isolated cases of skin tumours (seven cases of melanoma)113–116 and lymphomatous disease (B- and T-cell lymphomas, lymphomatoid papulosis) have been described since approval.117,118 Recently, two cases of Merkel cell carcinoma have also been reported. 119 The PANGAEA study described 21 cases of basal cell carcinoma, 6 of melanoma and 4 of other carcinomas of the skin. 120
In addition, isolated cases of haemophagocytic syndrome (HPS) have been described in the context of fingolimod treatment. 121 The aetiology of this syndrome in association with fingolimod still remains enigmatic. However, its proposed association with Epstein–Barr virus (EBV) infection might suggest a connection between fingolimod, dysregulated herpes virus responses and HPS. 122
Owing to the high expression of S1P receptors on cardiomyocytes, fingolimod dosing may cause negative chronotropic and dromotropic effects.123,124 Importantly, this effect is very transient due to rapid receptor downmodulation on cardiomyocytes, which means cardiac monitoring is only required during first dose application. 125 Some patients develop liver enzyme elevations after treatment cessation.
Practical monitoring recommendations
See Table 4 for a summary of practical monitoring recommendations. Fingolimod should not be used in patients suffering from severe active or chronic infections, as well as cardiac arrhythmias (such as sick sinus syndrome, relevant bradycardia, higher degree AV block) and severe liver disease. Sufficient immunity against VZV needs to be documented, and in case of negative VZV antibodies, appropriate vaccination must be performed. In addition, lab testing of differential blood count, liver enzymes and kidney function should be obtained before treatment initiation. Owing to cardiac-related side effects, a first-dose observation procedure is recommended. Patients should be examined hourly for bradycardia by measuring pulse and blood pressure for at least six hours. Prior to dosing and at the end of the observation period, an electrocardiogram (ECG) must be performed. After fingolimod treatment onset, liver enzymes should be analysed after 4 weeks and followed by testing every 3 months in the first treatment year. Differential blood counts should be tested after 3 months. Afterwards, testing should be performed periodically as necessary. In the case of confirmed liver enzyme [alanine transaminase (ALT), aspartate transaminase (AST)] elevations above 5× ULN, weekly testing of liver enzymes should be performed. In case of persistent elevations, fingolimod treatment should be discontinued permanently. Blood counts should be tested periodically, and fingolimod treatment should be stopped in case of a confirmed and persistent lymphopenia below 100–200/µl. Of note, recommended cut-off values vary, as the EU recommends a cut-off of 200/µl, whereas in Switzerland a cut-off of 100/µl is recommended.
Fingolimod treatment also modestly compromises immune responses against vaccines, and use of live attenuated vaccines should be avoided.
Blood pressure should be periodically monitored during treatment. Signs and symptoms of posterior reversible encephalopathy syndrome (PRES), respiratory diseases, cryptococcal meningitis, PML and cardiac disease should be considered during treatment. In patients with history of macular oedema, ophthalmological examination during the first year of treatment should be performed.
Furthermore, regular dermatologic examinations should be performed as part of the recommended routine check-up for skin cancer. It is recommended to discontinue therapy with fingolimod at least 2 months before planned conception in female patients (Table 3). However, the risk of recurrence of disease activity during pregnancy after stopping fingolimod may be substantial. 126
Alemtuzumab (Lemtrada®)
Alemtuzumab is a monoclonal IgG1 antibody binding to the human CD52 protein. It is a humanized antibody with a mouse-derived antigen-specific, highly variable Fab region and an Fc region of human origin. CD52 is a glycosylphosphatidylinositol (GPI)-anchored protein consisting of 12 amino acids expressed at high levels on T and B lymphocytes and to a lesser extent on monocytes and macrophages and eosinophilic granulocytes. Mature natural killer (NK) cells, plasma cells, neutrophil granulocytes and most importantly haematological stem cells show little or no expression. Antibody infusion thus leads to a selective depletion of lymphocytes, associated with a cytokine release syndrome causing flu-like symptoms such as fever, headache, muscle soreness, nausea, fever, rash and changes in blood pressure.
Pronounced long-term lymphopenia and, rarely, neutropenia 127 occurs after administration of alemtuzumab. Tissue-resident lymphocytes, however, including those located in secondary lymphoid organs such as lymph nodes, spleen and bone marrow, are less affected than circulating lymphocytes.128,129 Long-term immune reconstitution was examined after treatment with alemtuzumab in a RA cohort. Results showed differences in immune cell composition some 20 years after the last alemtuzumab infusion (e.g. significantly reduced CD4+ and CD8+ memory cells). 130 The pronounced depletion of circulating immune cells explains the temporally increased susceptibility towards infections, especially classical infections of the upper respiratory tract, urinary tract infections, oral herpes manifestations as well as flu-like infections. Severe VZV-(re-)infections have also been observed. There have been some atypical infections, 131 such as reactivation of latent TB,103,132 spirochete infections, Pasteurella infections, oesophageal candidiasis, 132 several cases of Listeria meningitis 133 and cerebral nocardiosis. 134 Infusion-related pulmonary and systemic cytomegalovirus (CMV) reactivation was also described recently.135,136 Furthermore, cases of acalculous cholecystitis and atypical pneumonitis during infusions have been noted in the post-approval phase. 137 Despite the increased incidence of mild infections and rare atypical or opportunistic infections, the overall rate of severe bacterial infections is not significantly increased over the longer term (it may be in the first month), most likely due to the mild and very transient effects on the innate immune cell compartment. To date, only one definite case of PML has been described in the context of alemtuzumab therapy, although evidence of PML prior to commencement of alemtuzumab and after cessation of natalizumab was noted. Several PML cases have been described in lymphoma patients receiving polychemotherapy including alemtuzumab, but lymphoma itself is a PML risk factor.
Acute infusion-related reactions due to cytokine release syndrome and an increased risk of infections are expected and are consistent with the mechanism of action of the drug. It should be noted that this cytokine release syndrome might result in transient deterioration of neurologic symptoms. 138 In a single case, acute pneumonitis and pericarditis, presumably related to rapid cytokine release has been reported and should be considered in patients with severe immune-mediated reactions during and/or after alemtuzumab infusion. 139 Further, a cohort study showed a transient moderate drop in platelet counts, but not below the lower limit of normal (LLN) in the majority of patients. 140 However, thrombocytopenia was symptomatic (ecchymoses and purpura) in a single fatal case. 141 Leukocytoclastic vasculitis has been reported as an additional infusion-related reaction. Therefore, this (benign) cutaneous vasculitis should be considered in patients with infusion-related cutaneous changes.142,143
The third and most important group of side effects is the occurrence of secondary autoimmune diseases.144,145 Secondary autoimmunity affects the thyroid gland in at least 35% of treated patients; approximately 2% develop autoantibodies against platelets [idiopathic thrombocytopenic purpura (ITP)]. Moreover, there are rare cases of autoimmune neutropenia, haemolytic anaemia and autoimmune kidney diseases (incidence 0.3%).146,147 The reason for the profound increase of autoimmune diseases after alemtuzumab therapy and particularly in thyroid autoimmune disorders remains unclear, and so far there are no prognostic and predictive markers available. An increase in the same autoimmune diseases albeit with a lower rate of thyroid autoimmunity than alemtuzumab occurs following autologous haema-topoietic stem cell transplantation. 148
Recently, cases of paradoxical disease exacerbation shortly after alemtuzumab treatment initiation have been reported.149–152 One hypothesis suggests that a dysregulated B-cell autoimmunity exacerbates MS.
There is no observed increased risk for developing malignancies per se. However, an increased incidence of human papillomavirus (HPV)-related cervical dysplasia has been observed, as have several thyroid malignancies, skin cancers and one case of Burkitt lymphoma. It is possible that the periodic immunodepletion followed by recovery will mean that the increase in malignancy risk is less with alemtuzumab over the long-term compared with chronic suppressive strategies.
Practical monitoring recommendations
See Table 4 for a summary of practical monitoring recommendations. Alemtuzumab should not be used in patients suffering from active malignancies, severe liver or kidney insufficiency, or known coagulation disorders. Before treatment, active chronic infections, especially TB, syphilis, HIV, hepatitis B virus (HBV) and hepatitis C virus (HCV) must be excluded. Sufficient immunity against VZV should be documented, and in case of negative VZV antibodies, appropriate vaccination must be performed. With regard to lab diagnostics, differential blood count, liver enzymes, kidney renal parameters and urine analysis (including microscopy) should be obtained monthly. Every 3 months, thyroid-stimulating hormone (TSH) should be assessed to screen for potential thyroid pathology. When switching from natalizumab, especially in high-risk patients (longer treatment duration, JCV antibody positive, high JCV antibody index, prior immune suppression) we recommend excluding subclinical PML with cMRI and, optimally, including cerebrospinal fluid (CSF) examination with JCV DNA testing [and potentially antibody-specificity index (ASI) for anti-JC antibodies].
Monthly differential blood counts including platelets must be performed for at least 48 months after the last infusion to monitor for treatment-associated cytopenia and the development of secondary autoimmune disease. Moreover, monthly tests of renal function [creatinine, glomerular filtration rate (GFR), urine status and sediment to search for infections as well as proteinuria as indicator for nephropathy or glomerulonephritis] and 3 monthly testing of thyroid function via TSH should be performed.
The efficacy of vaccinations can be impaired after alemtuzumab administration; hence, the schedule of vaccinations according to local guidelines should be completed 6 weeks prior to alemtuzumab treatment. Administration of live attenuated vaccines should be avoided in patients who are treated with alemtuzumab. Influenza vaccinations can be performed 6 months after alemtuzumab infusions.
Symptoms of cytokine release syndrome as a consequence of alemtuzumab infusion should be mitigated by pre-administration of intravenous steroids, paracetamol and H2 blockers. Oral prophylaxis with acyclovir (2×200 mg) should be administered from the first day of alemtuzumab infusion for a total of 1 month to reduce risk of local herpes virus reactivations. To reduce the risk of Listeria infection, we further recommend avoiding consumption of nonpasteurized milk products and raw meat, fish or seafood for a month before and 2 months after the infusion cycle. In light of potential inhalation of nocardia or legionella from soil, intensive gardening should be avoided or done with a mask during the month before and the first 3 months after alemtuzumab infusion. Clinical vigilance and education of patients for the signs and symptoms of ITP, Goodpasture syndrome and any kind of opportunistic infection is mandatory.
In female patients, regular cervical screening for HPV infection or cervical dysplasia/neoplasia should be performed.
Pregnancy is a contraindication for alemtuzumab and contraception is recommended at least 4 months after the last infusion cycles 37 (Table 3).
Daclizumab (Zinbryta®)
Daclizumab is a humanized monoclonal antibody that binds to the Tac epitope of the alpha-subunit (CD25) of the high-affinity interleukin-2 receptor, which is mainly expressed on T cells. 153 Integrated analysis of all clinical daclizumab studies showed a cumulative incidence of any opportunistic infection of 2%, primarily due to noninvasive Candida infections and pulmonary TB. 154 Interestingly, although the clinical study program revealed only minimal changes in the overall infection rate, there was an unexpected doubling of severe bacterial infections, most commonly standard infections such as pneumonia or urinary sepsis.155–157 The seven- to eight-fold increase in NK cells seems to elicit variable skin reactions including rashes, contact dermatitis, urticaria, folliculitis and others.158,159 Moreover, the complex effects of daclizumab on the immune-regulatory network seem to predispose to the development of other immune-mediated disorders, including lymphadenopathy, noninfectious colitis, autoimmune thyroiditis and Grave’s disease, glomerulonephritis and autoimmune hepatitis. 160 Very recently in the post-approval setting 12 cases of severe inflammatory brain disorders occurred under daclizumab treatment,161–163 which initiated both urgent review by the European Medicines Agency (EMA) and resulted in global voluntary withdrawal of the drug by the company. Owing to the fact that some of these disorders occurred several months after daclizumab treatment cessation, patients should be clinically monitored for at least 12 months. 164 Other cases of suspected autoimmunity (e.g. fatal autoimmune hepatitis, autoimmune haemolytic anaemia) under daclizumab have been reported. 165 This recent example impressively shows that the safety profile of drugs can change in the post-marketing setting despite performance of a rigorous clinical study programme and should therefore highlight the necessity of increased vigilance especially in newly approved drugs.
Ocrelizumab (Ocrevus®)
Ocrelizumab is a humanized recombinant anti-CD20 antibody that targets an epitope distinct from, but overlapping with, the epitope bound by rituximab, causing rapid elimination of circulating CD20+ B cells.166,167 The safety profile of ocrelizumab is so far based on data from phase III clinical studies OPERA I, OPERA 2 and ORATORIO.168,169 Here, the most frequent adverse events were infusion-related reactions, most of them mild or moderate. Moreover, there was a slight increase in typical infections such as pharyngitis, upper respiratory tract infection, headache and urinary tract infection.168,169 Although no cases of PML or other opportunistic infections on monotherapy have been described in the study program, the relatively small sample size and limited duration of follow up prevents definitive evaluation. However, PML occurred in one primary progressive multiple sclerosis (PPMS) patient under ocrelizumab in the context of a compassionate use program. 60 Since then, five more carry-over cases have been described (four additional natalizumab carry-over cases, one fingolimod-associated PML case; Table 5). There was only a slight increase in the incidence of herpes virus associated infections in ocrelizumab-treated patients.
In the rituximab experience, cases of hypogammaglobulinemia as well as reductions in the number of T cells over time have been observed.170,171 Furthermore, rare cases of neutropenia have been described.172,173 With regard to infections, some specific infections have been documented such as Pneumocystis pneumonia or Pasteurella infections.174,175
Four neoplasms occurred in the OPERA I and II trials: two cases of invasive ductal breast carcinoma, one case of renal cell carcinoma and one case of malignant melanoma. In the ORATORIO trial, 11 patients developed neoplasms: breast cancer in four patients, basal cell carcinoma in three patients and endometrial adrenal carcinoma, anaplastic lymphoma, malignant fibrous histiocytoma and pancreatic carcinoma in single cases. The relevance of this imbalance in neoplasms in the ocrelizumab group compared with either the placebo group or the active comparator group currently is unclear. However, the possibility that ocrelizumab might enhance the risk of carcinoma cannot be excluded to date. The overall incidence rate of first neoplasm among patients treated with ocrelizumab across all studies was 0.449 per 100 patient-years of exposure as compared with 0.216 per 100 patient-years of exposure in the pooled comparator groups. To date, however, there is no clear risk for specific tumour entities in patients receiving ocrelizumab.
Practical monitoring recommendations
See Table 4 for a summary of practical monitoring recommendations. Ocrelizumab should not be used in patients suffering from active malignancies. Before initiating treatment, severe active or chronic HBV infection must be excluded. Owing to the increased risk of HBV-associated hepatitis and liver failure in B-cell-depleted patients, patients with positive hepatitis B core antibodies should be continuously monitored for HBsAg and HBV DNA every 12 weeks.176,177 Lab testing including differential blood count should be assessed. We also recommend documenting CD19+ B-cell counts and total IgG in the serum at baseline. Fulfilment of local vaccination recommendations at least 6 weeks prior to initiation of ocrelizumab, including pneumococcal and VZV vaccinations in seronegative patients, should be documented. To decrease the risk of infusion-related reactions, administration of methylprednisolone and antihistaminic as well as an antipyretic treatment is recommended.
After treatment onset, control visits are recommended after 4 weeks and then every 3 months. Differential blood count including CD19+ B-cell counts needs to be performed every 3 months. In addition, every 6 months, we recommend quantification of total IgG in the serum and CD4+ T-cell counts. Owing to large variations in B-cell repopulation kinetics, monitoring of B-cell repopulation might be warranted especially in patients exhibiting clinical or radiological signs of new MS disease activity to potentially adjust the treatment interval accordingly. Efficacy of vaccinations under ocrelizumab treatment might be impaired and the administration of live attenuated vaccines should be avoided. As there are no valid long-term data on the prevalence of cancer under ocrelizumab, it is recommended that regular cancer check-ups are performed in treated patients. 178 Pregnancy is a contraindication for ocrelizumab. Women of child bearing potential should use contraception while receiving ocrelizumab and for 6 months (FDA) or 12 months (EMA) after the last infusion. (Table 3).
Cladribine (Mavenclad®)
Cladribine, a synthetic purine analogue that is resistant to adenosine deaminase (ADA), is able to disrupt DNA synthesis and repair specifically in lymphocytes. The resulting lymphopenia experienced with cladribine can explain the temporally increased susceptibility towards infections, especially herpes virus infections and reactivations.179,180 Furthermore, there have been reports of TB reactivations in cladribine-treated patients.180,181 As already observed for alemtuzumab, the overall rate of infections as well as the rate of severe bacterial infections was not increased substantially in cladribine-treated compared with placebo-treated patients, most likely due to the rather mild effects on the innate immune compartment.182,180 Until now, a few PML cases have been described in patients treated intravenously with cladribine in the context of hairy cell leukaemia, and in one case of cladribine monotherapy for systemic mastocytosis. 183 However, so far, there have been no cases of PML in the MS clinical study programs with oral cladribine.59,184
In preclinical experiments, teratogenic effects of cladribine have been observed.185,186 Within the clinical study program, there was a slightly increased rate of malignancies in cladribine-treated versus placebo-treated MS patients (10 events in 3414 patient years, that is, 0.29 events per 100 patient years; versus 0.15 events per 100 patient years in the placebo group).
Practical monitoring recommendations
See Table 4 for a summary of practical monitoring recommendations. Cladribine should not be applied in patients suffering from severe active or chronic infections (TB, HIV, VZV, HBV and HCV), severe liver or kidney damage or active cancer. Owing to preferential renal excretion, cladribine should not be applied in patients with moderate to severe renal dysfunction. Sufficient immunity against VZV should be documented, and in case of negative VZV antibodies, appropriate vaccination must be performed. In general, all local vaccination recommendations should be fulfilled at least 4–6 weeks before treatment onset.
With regard to lab diagnostics, differential blood count should be obtained before treatment. Blood lymphocyte counts need to be assessed prior to each individual treatment cycle. Before treatment in year 1, counts need to be within normal limits, and before year two, they need to exceed 800/μl. After treatment onset, lymphocyte counts need to be retested at 2 and 6 months after each cycle, and in case of lymphopenia below 500/μl, follow up needs to be performed until recovery. Furthermore, these patients should be actively monitored for infections, especially herpes virus infections. In case of severe lymphopenia below 200/μl, oral prophylaxis for herpes virus reactivations should be administered.
Application of live attenuated vaccines should be avoided and application needs to be completed at least 4–6 weeks before cladribine treatment onset. Of note, blood transfusions into cladribine-treated patients should be irradiated before use to avoid graft-versus-host disease. Cladribine is contraindicated in patients with active malignancies. All patients should be advised to follow guidelines for routine check-ups for early cancer diagnosis. Cladribine is contraindicated during pregnancy and effective contraception is warranted until at least 6 months after last cladribine intake. Furthermore, owing to its potential gametotoxic effects, male patients also need to apply effective contraceptive methods until at least 6 months after the final application.
Immunosuppressive drugs approved for treatment of MS
Mitoxantrone (Ralenova®)
Mitoxantrone is a topoisomerase-II-inhibitor, which interferes with DNA synthesis, preferentially in rapidly dividing cells including immune cell populations. 187 It is primarily used for treatment of certain types of cancer, however, it has been approved for treatment-refractory MS as well as treatment of secondary progressive MS. 188 Owing to its potent antiproliferative effects, it suppresses both T and B cells, but also macrophages, and reduces proinflammatory cytokine production by these cells.
As an antiproliferative agent, mitoxantrone displays the typical side effects of chemotherapeutic drugs including nausea, vomiting, hair loss and increased risk of infections.189,190
Furthermore, like other members of the anthracycline family, it is cardiotoxic in a dose-dependent fashion, which limits its use to a cumulative dose of 100 mg/m2; in individual cases treatment might be continued under close cardiologic monitoring up to a maximum dose of 140 mg/m2. Furthermore, there is an increased risk of leukaemia in mitoxantrone-treated patients with a frequency between 0.25% and 6% in different patient cohorts. 49 Owing to potential gametotoxic effects in humans, both male and female patients need to take appropriate precautions to prevent pregnancies. Male patients have to be informed about the potential risk of irreversible infertility and the possibility of sperm cryopreservation.
In summary, owing to its unfavourable side-effect profile and the change in treatment landscape in MS in the last few years, use of mitoxantrone in MS patients has declined rapidly. Therefore, practical monitoring recommendations will not be discussed here but are provided in Table 4.
Azathioprine (Imurek®)
Azathioprine is an antimetabolite interfering with purine nucleotide synthesis needed for DNA and RNA replication. 191 It has been used in MS for more than three decades and received approval in the EU for this indication in 2000. Owing to its antiproliferative effects it primarily affects rapidly dividing cells of the body including immune cells. Accordingly, treatment-associated lymphopenia is expected but is in most cases rather mild. 192 According to a meta-analysis overall infection rates are not significantly elevated, however, single cases of TB or sepsis under azathioprine treatment have been described. 192
Long-term treatment with azathioprine has been associated with an overall 4.4 times elevated rate of malignancies after 10 years of treatment. 193 It is hence not recommended to pursue treatment after 10 years. Allopurinol interacts with azathioprine to significantly increase effect and potential toxicity; the combination should only be used with caution, initial dose reduction and close monitoring.
In light of the lack of data on azathioprine in MS from clinical trials meeting current quality standards and the increasing treatment options in this indication, use of azathioprine in MS is decreasing and is currently only rarely used in this indication and will therefore not be discussed here in detail; however, practical monitoring recommendations are provided in Table 4.
Concluding remarks
The availability of a broad spectrum of immune therapies with distinct modes of action, risk and side-effect profiles poses new challenges to this field, especially with regard to the common clinical scenario of long-term mono-immune therapy; and various sequential treatment possibilities that may be associated with additive immunosuppression. Management decisions to minimize treatment-related risk require comprehensive clinical, laboratory and, where appropriate, MRI assessment (derisking MS treatment at any time point, starting from diagnosis). For each treatment decision, individual risk stratification is required and consequent pharmacovigilance needs to be maintained (Table 4).
We believe that an understanding of the individual mechanism of action of each drug is essential for appropriately contextualizing laboratory abnormalities and their association with risk. One example is monitoring of peripheral lymphocyte counts and lymphopenia (commonly considered a measure of immune suppression): in the context of fingolimod treatment, lymphocyte numbers are decreased in the periphery owing to entrapment, although these cells remain functionally intact within the secondary lymphoid organs. This explains tolerance of profoundly decreased lymphocyte numbers (e.g. 200/μl in the EU). In the context of DMF treatment, however, a decrease of lymphocyte counts below 500/μl should result in treatment discontinuation. In the context of alemtuzumab and cladribine, lymphopenia is due to the specific mode of action, but does not directly correlate to individual safety (nor efficacy of treatment)
Another important facet of sequential treatment in MS is the currently evolving concept of pulsed immune reconstitution therapy with long-lasting consequences on the immune system (alternatively named induction therapy). One important example of this category is alemtuzumab, where sustained stability can be achieved in the majority of patients after only two treatment cycles. However, alemtuzumab is sometimes ineffective or results in paradoxical worsening,150,194 and sequential treatment after alemtuzumab administration is necessary. This scenario might also be applicable to cladribine, another drug causing lasting depletion of lymphocyte populations followed by lymphocyte reconstitution and a sustained treatment response in a proportion of patients.
MS treatment associated risks are influenced by (i) drug-related factors (mode of action, on-/off-target effects, chronic versus pulsed therapy) and (ii) patient-related factors (sequential treatment, comorbidities, age, genetic predisposition, lifestyle/environments factors), which have to be considered in a comprehensive risk assessment and monitoring approach.
The increasing complexity of MS therapies, especially with regard to treatment sequencing and potential additive immune compromise, heightens the need for standardized pharmacovigilance/safety data collection in disease-specific patient registries. Such databases provide a platform for systematic and independent analysis of safety data after drug approval; and facilitate the provision of these data to the community.
Finally, the development of novel therapeutics for MS should not only target maximizing drug efficacy, but also minimizing drug risk, especially in the context of long-term use, treatment sequences and, potentially, combination therapy. Ideally, therapeutic strategies that promote immune reconstitution very early in the disease without impairing natural defence mechanisms or endogenous control of incipient autoimmunity should be developed.
Footnotes
Funding
JH is (partially) funded by the German Federal Ministry of Education and Research (Grant Numbers 01ZZ1603[A-D] and 01ZZ1804[A-H] (DIFUTURE)).
HW is funded by the German Federal Ministry of Education and Research (Grant Numbers BD604561 and BD604573) (Competence Network Multiple Sclerosis) and by the German Research Fundation (DFG) ( Grant Numbers SFB-TR 128A09, SFB-TR 128A10, SFB-TR 128V and SFB-TR 128Z02) (Collaborative Research Centre 128 “Multiple Sclerosis”).
Conflict of interest statement
LK reports personal fees and non-financial support from Genzyme, Novartis and Roche, personal fees from Merck Serono, Teva, and CSL Behring, as well as grants from Novartis and Biogen outside the submitted work. JH reports grants from Friedrich-Baur-Stiftung, personal fees and non-financial support from Merck, Novartis, Roche, Bayer Healthcare, Santhera, Biogen, Sanofi-Genzyme, and non-financial support from Guthy-Jackson Charitable Foundation, all outside the submitted work. NS reports non-financial support from Sanofi-Genzyme and Novartis outside the submitted work.
RH reports personal fees from Novartis, Actelion, Roche, Sanofi-Genzyme, Merck, and Teva outside the submitted work.
SR reports funds including but not limited to travel support, honoraria, trial payments, research and clinical support to the neurology department of which he is a member, from NHMRC, MGANSW, MGAQLD, MAA, Lambert Initiative, Beeren foundation and from Baxter, Bayer Schering, Biogen Idec, CSL, Genzyme, Grifols, Octapharma, Merck, Novartis, Roche, Sanofi Aventis Genzyme, Servier, TEVA outside the submitted work. This includes participating in the CARE MS1 and 2 RCTs and the long term Lemtrada PASS study. He is Co-founder / shareholder of Medical Safety Systems trading as RxMx (grant and contracts with Genzyme > $25000 AUD with Novartis, Roche, Janssen, potential application to multiple drugs). National IVIG Governance Advisory Council & Specialist Working Group Australia (Neurology) (paid), Australian Medical Services Advisory Committee ad-hoc sub-committee on IVIG (paid), Australian Technical Advisory Group on Immunisation Varicella Zoster working party (unpaid), Nerve Research Foundation board member (unpaid). Furthermore he is public Salary as a staff specialist neurologist from Concord Hospital Sydney Local Health District (paid), private billings from patients and medicare Australia reimbursement as a private practice neurologist (paid), medical advisor (unpaid) to various patient and advocacy groups. MB reports grants from Biogen, Novartis Pharmaceuticals, Sanofi-Genzyme, and Merck outside the submitted work. Dr Barnett is a Consultant to Medical Safety Systems and Research Director at the Sydney Neuroimaging Analysis Centre.