
Abstract
Health-related quality of life (HRQOL) is an important clinical outcome parameter. Its analysis is particularly meaningful to patients with minor functional impairment. The main goal of this study was to assess long-term data of HRQOL and their variables for patients undergoing treatment for unruptured intracranial aneurysms (UIAs). Therefore, a cross-sectional study of HRQOL (SF-36 questionnaire) was conducted in patients treated for UIA using a telephone survey assessing numerous medical and sociodemographic variables. A total of 96 patients with a follow up longer than 36 months post-treatment were included. HRQOL results were compared with the German reference population. Uni- and multivariate analyses were performed to detect variables with an impact on outcome. After a mean follow up of 57.75 ± 13.56 months, patients with treated UIAs showed a significant decrease in the mental health domains ‘role emotional’ and ‘social functioning’ and the ‘mental health component score’ (MHCS) compared with the age- and sex-matched reference population. Overall, 47% of the patients showed a clinically and psychosocially relevant decrease compared with the mean MHCS of the reference population. Multivariate analysis suggests that mainly the treatment modality (coiling versus clipping) and additional remaining untreated UIAs negatively impacted mental HRQOL. In conclusion, the partly significant losses in HRQOL identify the necessity for less-wearing treatment strategies and a better prediction of risk of UIA rupture. Our results indicate that certain factors in the guidance and management of patients undergoing endovascular treatment may negatively affect their mental HRQOL. The relevance of additional UIAs remaining untreated on HRQOL is a new finding that should be considered in the counseling of patients with multiple UIAs.
Introduction
The World Health Organization defines quality of life (QOL) as an ‘individual’s perception of their position in life in the context of the culture and value system in which they live and in relation to their goals, expectations, standards and concerns’. 1 Health-related QOL (HRQOL) is the extent to which one’s usual or expected physical, emotional and social wellbeing is affected by a medical condition or its treatment. 2 Therefore, HRQOL is regarded as an important parameter in clinical outcomes research in addition to mere functional outcome measures, especially in patients with minor or no functional impairment.3–6 In patients with unruptured intracranial aneurysms (UIAs), HRQOL is thus of particular interest. On the one hand, functional impairment in these patients prior to treatment is negligible, 7 on the other hand, the prediction of the risk of rupture of UIAs and the necessity of a preventive treatment remain difficult to estimate.8–10 Thus, beyond the prevention of a potential subarachnoid haemorrhage (SAH), preservation of HRQOL after treatment is particularly crucial, and the main treatment goal should be to increase the patient’s number of life years with a good QOL.
Of note, a patient’s perception of HRQOL does not necessarily correlate with functional outcome, especially in patients with no or no significant post-treatment disability. 11 These patients, however, represent the vast majority. 12 HRQOL can thus not be deduced from functional outcome data (as performed in previous research 13 ), but has to be assessed independently. Available data on HRQOL after patients have been treated for UIAs are sparse and controversial. While a decline in HRQOL (to a lesser extent in patients undergoing endovascular treatment) in the short-term follow up after treatment is consistently reported by most authors,14–16 the extent of recovery of HRQOL and return to ‘baseline’ or reference population levels in the long term remains unclear. In addition, the potential impact of the treatment modality (surgical versus endovascular treatment) on long-term HRQOL remains unknown, as well as multiple additional factors, such as physical or psychological sequelae, retreatment, fear of rupture in incompletely treated lesions, further untreated aneurysms, repetitive follow up examinations/hospital visits, etc. 5
Although the first long-term (mean follow up of 6 years) outcome data on recovery, return to work, and life satisfaction after treatment of UIAs have recently been published, 17 data on HRQOL are lacking, particularly from comparative studies with long-term follow up (>36 months). 13 In this context, we studied long-term HRQOL in a series of consecutive patients who had undergone singular endovascular or microsurgical treatment in our centre.
Methods
Study design and population
We searched our prospectively managed hospital database for intracranial aneurysms to identify all consecutive patients who received a single treatment for a UIA by clipping or coiling (with or without stenting) between 2008 and 2012 and fulfilled further inclusion criteria (see below). Patients were contacted afterwards by telephone and a standardized survey was carried out to assess HRQOL using the 36-item short form (SF-36) questionnaire.
The study was conducted according to the principles expressed in the Declaration of Helsinki, and local ethics approval was obtained (Ethik Kommission Universitätsklinikum Essen, Review Board identification 15-6624-BO). Informed consent was obtained from all participants.
Inclusion criteria
We included patients aged 18–80 years with solitary treatment of an incidental UIA by coiling or clipping. All patients underwent a complete outcome assessment, both clinical [modified Rankin score (mRS) at discharge and at 12 months] and radiological [clipping: postoperative computed tomography (CT) scan within 24 hours and postoperative angiography within 7 days; coiling: post-interventional magnetic resonance imaging (MRI) within 3 days]. Further radiological and clinical follow up varied individually.
Exclusion criteria
Patients who underwent a second treatment for another ruptured or unruptured aneurysm before or after initial treatment and patients who underwent an invasive medical treatment necessitating hospitalization within 3 months prior to the telephone survey were excluded from the study.
Data collection and survey
Clinical baseline data of patients, aneurysms and procedures were obtained from the local clinical database and the picture archiving and communicating system. The degree of disability was assessed using the mRS. 18 Radiological data (location of aneurysm, size of aneurysm, degree of aneurysm occlusion, treatment-associated ischaemia) were independently assessed by an experienced neuroradiologist (I.W., C.M. or M.F.). HRQOL was assessed by standardized telephone interview (P.W.) using the German version of the SF-36. 19 This questionnaire addresses eight domains [physical functioning (PF), social functioning (SF), role physical (RP), role emotional (RE), mental health (MH), vitality (VT), bodily pain (BP) and general health perception (GH)] and two component scores [physical health (PHCS) and mental health (MHCS)]. 20 SF-36 data from a German population sample were used as a reference sample. 19 If incomplete, additional socioeconomic (employment status, marital status, education) and clinical baseline data were also obtained during the telephone interviews. Extra radiological follow up examinations (MRI, CT, angiography) beyond the baseline follow up were counted for each patient.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics version 22 (SPSS Inc., IBM Corp., North Castle, New York, USA). Interval-scaled data were expressed as mean and standard deviations, and nominal data were expressed as absolute numbers and valid percent. Data were tested for normal distribution by conducting a Shapiro–Wilk test, in addition to histograms and Q–Q plots. We used parametric statistics for between-group comparison and univariate analysis for normally distributed data and nonparametric statistics for non-normally distributed data. For categorical variables, Chi-squared or Fisher’s exact tests (expected frequencies <5) were applied. Based on the German reference sample, a sex- and age-matched 1–1 case-control sample was created. Comparison of mean values (SF-36 scores) was performed using the Student’s t test preceded by the Levene’s test. Effect size was reported using Cohen’s D. Internal consistency of the SF-36 results was tested by Cronbach’s α. To identify parameters with an impact on post-treatment HRQOL in the complete participating cohort (PC), univariate analysis was performed, whereupon significant parameters (p < 0.05) were included in a multivariate linear regression analysis. All tests were two tailed (α = 0.05).
Results
Of all the patients with UIAs treated in our institution between 2008 and 2012, 189 matched the inclusion criteria [overall cohort (OC)]. Of these, 96 (51%) participated in the study (PC) and 93 (49%) were not available or declined to participate [nonparticipating cohort (NPC)], 38 (41%) of these patients underwent clipping, 55 (59%) endovascular coiling. Of those who participated, 37 (39%) patients underwent surgical clipping [the clipping cohort (CLC)] and 59 (61%) underwent endovascular coiling with or without stenting [the coiling cohort (COC)]. The mean interval between aneurysm treatment and completion of the survey was 57.75 ± 13.56 months (Table 1). For the flow chart, see Figure 1.
Baseline characteristics of cohorts.

Values are given as n (%).
including arterial hypertension.
ACA, anterior cerebral artery; Acom, anterior communicating artery; CLC, clipping cohort; COC, coiling cohort; ICA, internal carotid artery; MCA, middle cerebral artery; MRI, magnetic resonance imaging; mRS, modified Rankin score; n/a, not available; NPC, nonparticipating cohort; OC, overall cohort; PC, participating cohort; Pcom, posterior communicating artery; VBS, vertebra-basilary system.
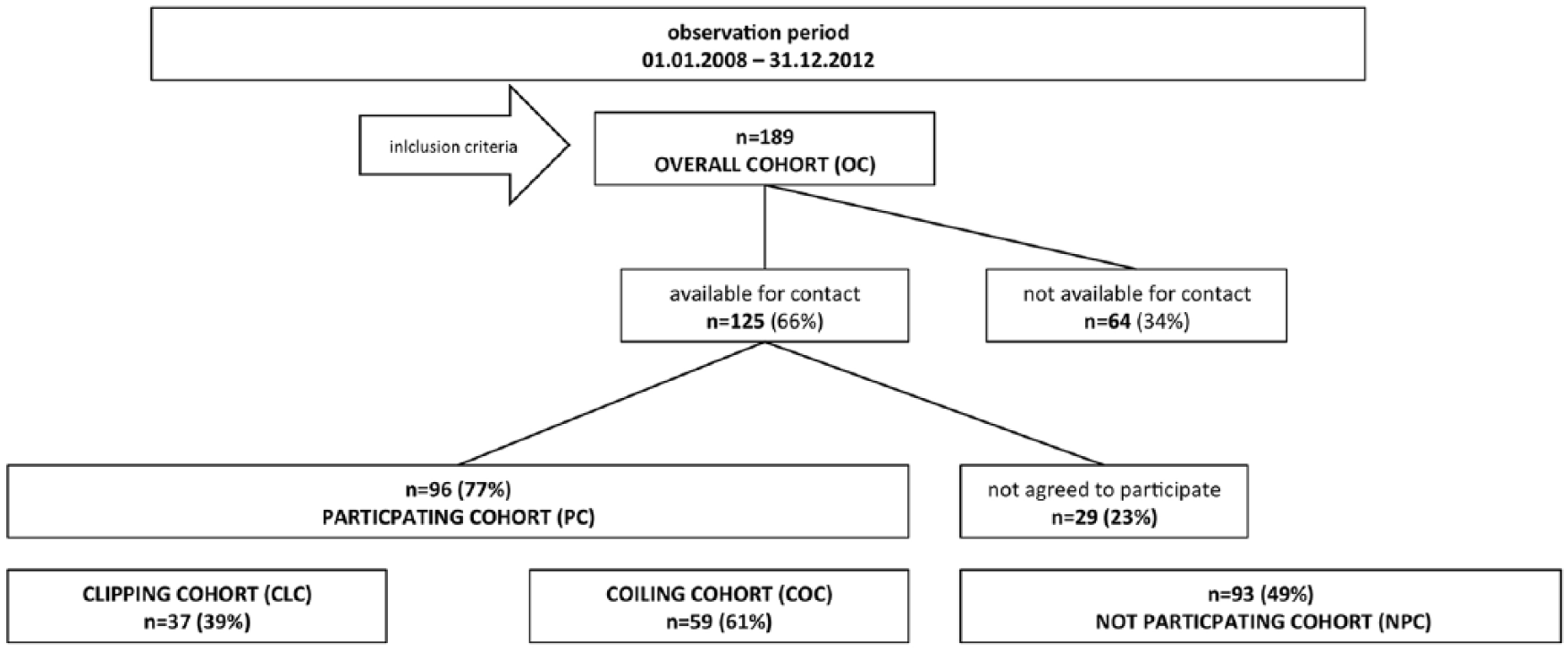
Study flow chart. Of 189 patients matched to the inclusion criteria in the observation period, 125 were available for contact. Finally, 96 of these (77%) agreed to participate.
Baseline clinical and radiological characteristics
Between-group analysis showed no significant differences in various baseline clinical and radiological parameters (see Table 1). Due to typical treatment allocation bias, 21 the COC included significantly more aneurysms of the posterior circulation and fewer middle cerebral artery aneurysms. Aneurysms of the CLC were larger when compared with the COC.
Clinical and radiological outcome
All groups showed no significant differences in various clinical and radiological outcome parameters (Table 2). The SF-36 results for all groups (PC, COC, CLC) and the age- and sex-matched German reference sample are shown in Table 3. Compared with the reference sample, the overall PC showed significantly decreased mental health domains (RE, SF) and MHCS. The COC showed similarly decreased scores, including the MH domain. In contradiction, the CLC showed no significantly decreased domains or component scores compared with the reference cohort. Effect sizes ranged between 0.32 and 0.59, reflecting minor (<0.40) and moderate (0.40–0.80) effects. 22 Cronbach’s α ranged between 0.893 and 0.907 for all SF-36 scores, reflecting good or excellent internal consistency/reliability. 23 In the PC, 47% (31, p = 0.006) of patients had an MHCS smaller than the mean score −2 points (clinically and psychosocially relevant difference24,25) of the reference sample. These were 53% (31, p = 0.001) and 38% (14, p = 0.15) for the COC and CLC, respectively (for details see Figure 2). In all, 10% of patients changed their work after aneurysm treatment: 3% retired from work completely and 7% reduced their work form full to part time. These numbers were similar in both treatment cohorts (see Table 2). The number of follow-up examinations beyond the postoperative baseline follow up was 0.7 ± 1.17 in CLC and 4.3 ± 2.3 in COC (p < 0.0001).
Clinical and radiological outcome of all cohorts.

Values are given as n (%).
As diagnosed on postoperative MRI (coiling) and catheter angiography (clipping).
As diagnosed on postoperative MRI or computed tomography scan (not including “spot-like” diffusion impairment).
Defined as medically or surgically treated procedure associated complications.
Defined as a decrease in mRS ⩾1 compared with preoperative condition.
Including patients who retired from work due to old age and those choosing to stay at home.
CLC, clipping cohort; COC, coiling cohort; MRI, magnetic resonance imaging; mRS, modified Rankin score; n/a, not available; NPC, nonparticipating cohort; OC, overall cohort; PC, participating cohort.
Results of the SF-36 questionnaire.

Age- and sex-matched sample from German reference cohort.
CLC, clipping cohort; COC, coiling cohort; PC, participating cohort; SF-36, 36-item short form.
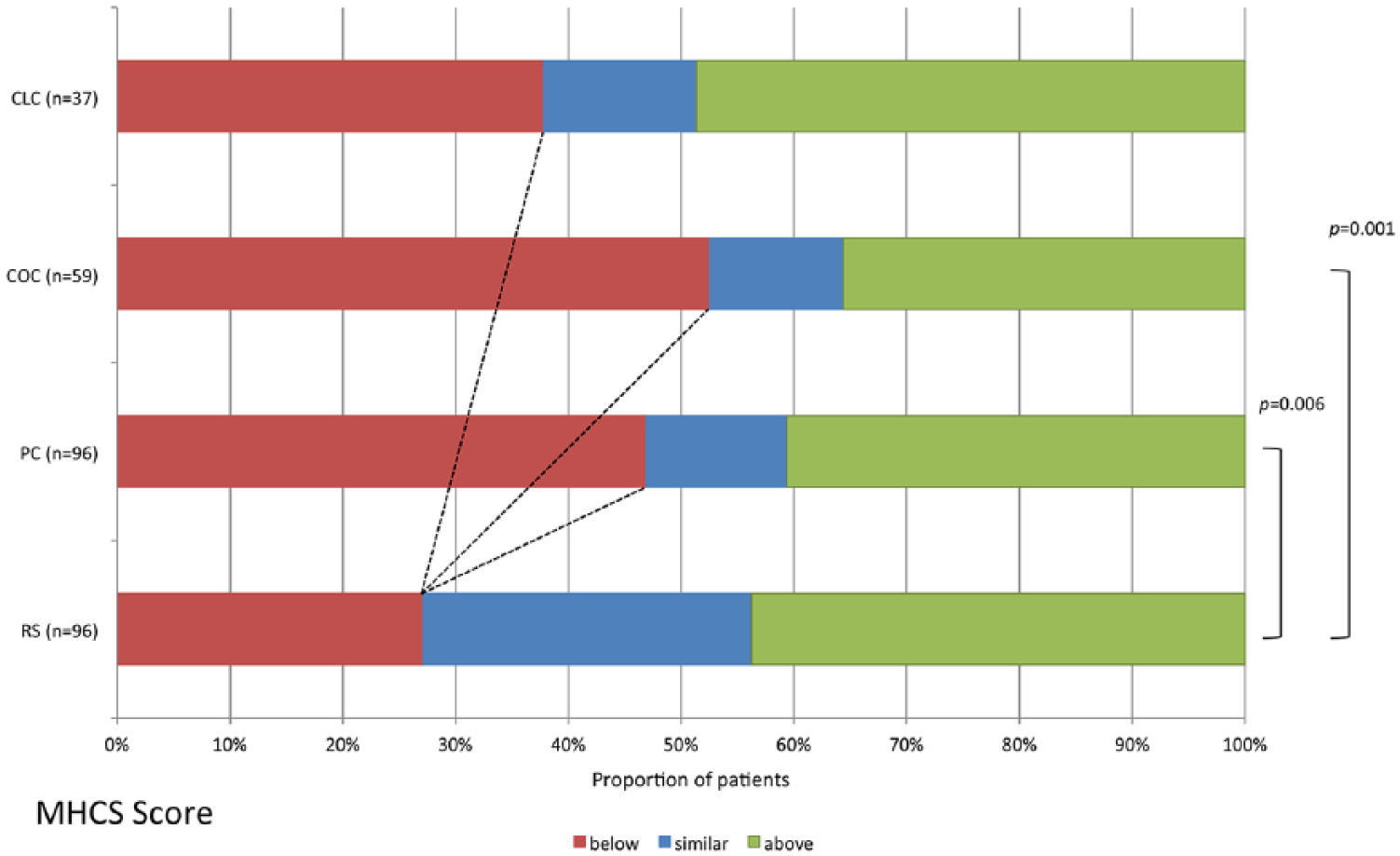
Proportion of patients with HRQOL (mental health component score) below, similar or above the mean value of the reference sample (RS) from the German population ±2 points (clinically and psychosocially relevant difference). Significant differences are marked. Both COC and PC showed a significantly higher proportion of patients below this clinically relevant cutoff point, thus a significantly higher proportion showed a decreased HRQOL compared with the normal population.
Univariate and multivariate analysis
Univariate analysis revealed several variables significantly correlating with the SF-36 subscore and sum score results (age, treatment modality, treatment survey completion time, additional remaining untreated aneurysms, aneurysm size). The following categorical or continuous (c) variables were tested and showed no significant correlation: sex, history of psychiatric disorder, history of chronic disease, number of follow-up examinations (c), degree of aneurysm occlusion, treatment-associated morbidity, treatment-associated ischaemia, marital status, employment status, and educational status. In the multivariate analysis, the following variables showed significant impact on SF-36 subscores and sum scores: age (MHCS, PHCS, MH, RE, SF and VT); treatment modality (MHCS, MH, SF, BP, PF and VT); additional remaining untreated aneurysms (MHCS, PHCS, MH, RE, RP, VT, BP and PF); treatment survey completion time (PHCS, RE, GH, BP, PF and RP); and aneurysm size (SF). Results of the multivariate analysis for the sum scores and three selected subscores are shown in Table 4 (complete multivariate analysis results are found in the online Supplementary Table e-1).
Multivariate analysis results of selected variables/factors.
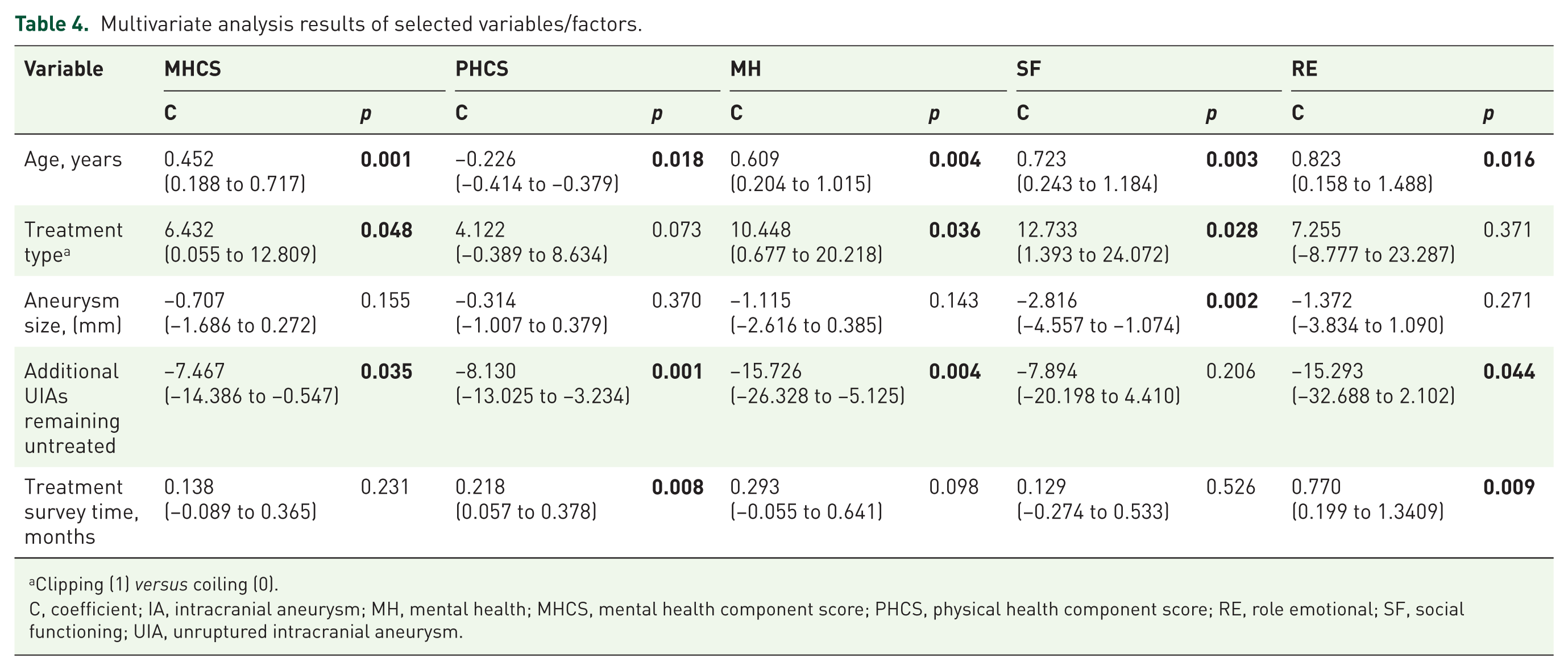
Clipping (1) versus coiling (0).
C, coefficient; IA, intracranial aneurysm; MH, mental health; MHCS, mental health component score; PHCS, physical health component score; RE, role emotional; SF, social functioning; UIA, unruptured intracranial aneurysm.
Discussion
In this study, patients treated for UIAs showed a significantly decreased HRQOL in the SF and RE domains and the MHCS in the long-term follow up (>36 months) compared with an age- and sex-matched normal population RS, as measured by the SF-36. A subgroup analysis revealed that this decrease in HRQOL compared with the normal population was only significant in the group that underwent endovascular treatment, while both subgroups showed no significant differences in between-group analysis (apart from aneurysm location and size) of multiple pre- and postoperative parameters.
How profound is this impairment of HRQOL?
The effect size of the difference in HRQOL of the PC and COC based on Cohen’s D was mainly ‘moderate’. This is in accordance with the effect size reported for the pre- and post-treatment results of various orthopaedic, cardiological and neurological chronic diseases. 26 In general, differences of 5 points in the domains and 2 points in the component scores in the SF-36 are regarded as clinically and psychosocially relevant.24,25 In this study, 47% of the PC showed a relevant decrease in the MHCS compared with the mean value of the RS. This was the case in 53% of the COC and only 38% of the CLC. For comparison, in the normal population RS, only 27% showed such a decrease, making the difference between the PC and COC significant. The fact that 10% of the patients reduced their working hours or stopped working due to treatment-related effects emphasizes the impact of treatment on the patients’ lives.
What factors are involved in the impairment of HRQOL?
In accordance with the subgroup results, our multivariate analysis of the complete cohort showed that the treatment modality had an impact on SF-36 results. Based on our data, we could not determine the underlying reasons for this interesting finding which had not been found in previous longer-term studies.26–28 Functional outcome, which has a major impact on HRQOL,5,6 did not differ between the two subgroups. Intervention-related morbidity was, as expected, relatively low in both groups. Univariate analysis accordingly revealed no impact of functional impairment on SF-36 results. Furthermore, physical SF-36 results, directly reflecting functional impairment,3,6 were unimpaired in both the complete cohort and subgroups compared with the RS. As already described in the Results section, various other sociomedical factors [including psychiatric diseases 29 and chronic diseases (based on SF-36 criteria 30 )], which could have affected HRQOL over the long follow-up period, also showed no significant impact on SF-36 results. A possible explanation for the significant discrepancy between coiled and clipped patients might be a difference in counseling and guidance/follow up of patients: mainly the more detailed information on higher potential reperfusion/retreatment rates in coiled aneurysms 31 and periodic controls of treatment results by imaging. The sheer number of follow-up examinations, which is naturally higher for patients undergoing endovascular treatment (as also shown in this study), on the other hand, showed no significant impact on HRQOL in this study. However, recent evidence about the low reperfusion rates of primarily adequately coiled intracranial aneurysms 32 has already led to the recommendation of a more restricted imaging follow up in German SAH guidelines. 33
In addition to treatment modality, multivariate analysis mainly revealed an impact of age (lower physical health scores, higher mental health scores with increasing age) and additional remaining untreated aneurysms. While the first is a well-known effect, 19 the latter is a new finding. In our opinion, the correlation of ‘untreated remainers’ with post-treatment HRQOL reflects the significant remaining fear of rupture of the untreated UIAs persisting over a long period of time. Accordingly, the effect size of this variable was especially profound in the domains, RE and MH. Our study may thus provide the first resilient argument 34 to include accessible additional aneurysms in a treatment via a chosen approach that otherwise would not provide critical criteria for a treatment (typically aneurysms <4 mm).
To date, no comparable studies on the long-term outcome of HRQOL exist. Only a few studies report on the short-term post-treatment course, mainly after microsurgical treatment. In summary, these studies report a decline of HRQOL within the first months and a marked but incomplete ‘recovery’ at 1-year post-treatment.14–16 There are three longer-term follow-up studies that analyzed patients who underwent both endovascular and microsurgical treatment. A cross-sectional study of patients who underwent either microsurgical/endovascular (n = 92) or no treatment (n = 81) of a UIA showed widely reduced physical SF-36 scores compared with a RS (individuals from the general normal population) in both groups. 26 However, the utilized RS was not matched for sex and age (the most significant impact factors of HRQOL 30 ), which is especially problematic considering the high mean age of this specific study population. Additionally, the study included patients with an extremely wide range of the intervention survey completion times (0.4–17.4 years), retrospectively recruiting from a 10-year period. Another study of 110 patients analyzed life satisfaction (LiSat-9) after treatment 17 and found that life satisfaction is reduced during recovery, and 20% of patients do not return to pretreatment baseline levels. A weak point of this study is its longitudinal retrospective approach. Consequently, the measurements may have been subjected to a response shift which may falsify results. 35 Additionally, comparison with the ‘baseline’ levels is problematic, as the diagnosis of a UIA itself is thought to reduce HRQOL for at least several months afterwards. 36 Hence, comparison with normal population samples may be more meaningful. Finally, a study of Pala and colleagues 28 reports on 77 patients after treatment of UIAs with 68% undergoing endovascular treatment. Also, in this study, the time interval between intervention and completion of the survey ranges widely (3–120 months) with a mean of roughly 24 months, which leads to a certain ‘mix-up’ of short-term and long-term outcomes. The authors found a decreased HRQOL in nearly all subscores and sumscores compared with normal population values, however it is unclear whether data were matched for age and sex. HRQOL in their cohort was even within the range of HRQOL in patients after SAH as reported earlier by the same group. 37 Overall, the relatively strong impairment of HRQOL in this study may be due to the above-mentioned study design aspects. Additionally, the authors themselves suggest that the results may be attributable to a high rate of chronic illnesses (54%) in the cohort.
Our study also has some limitations. First, although the sample size is relatively large, the detectable difference in the mean scores of the SF-36 of two cohorts is limited (5 points for component scores, 10 points for domains). 30 To detect more subtle differences, larger cohorts are necessary (approximately 200 participants for 2 points in component scores or 5 points in domains, respectively). Therefore, the effects on HRQOL may have been underestimated. Secondly, HRQOL has not been assessed prior to treatment to receive a ‘baseline’ score. However, due to the known acute impairment of HRQOL by the diagnosis of a UIA, 36 which seems to resolve over time, 27 a comparison with age- and sex-matched RSs may be preferable. Unfortunately, in this regard, our study lacks a control group with patients not undergoing treatment. Such a control group would help to more profoundly distinguish intervention-related effects from other influencing factors. Patients with UIAs may be prone to such factors. Buijs and colleagues reported that patients with untreated UIAs may show significantly decreased subscores compared with the normal population. 26 Finally, 51% of eligible patients participated in the study. Selection bias can thus not be excluded. The response rate of the patients that were available for contact (77%) is, however, within the typical range of comparable studies. Moreover, between-group analysis showed no differences between participating and nonparticipating patients.
Conclusion
Overall, our study provides new information on HRQOL and employment rates in the long-term follow up after treatment of a UIA. This will empower decision-making in and counseling of patients with a UIA, especially when the risk–benefit ratio of the treatment remains unclear. The partly significant losses in HRQOL indicate the necessity for less-wearing treatment strategies and better prediction methods for the risk of a rupture in UIAs in general. However, in this regard it should be kept in mind, that the event of an SAH leads to a massively decreased HRQOL in the majority of patients,38,39 even in the long-term follow up of those patients with initially good functional neurological outcome. 40
The significant difference in mental HRQOL outcome between ‘clipped’ and ‘coiled’ patients in our study is a new finding. Potentially, certain factors in the guidance and management of patients undergoing endovascular treatment may negatively affect their mental HRQOL. Finally, the relevance of additional UIAs remaining untreated, as presented in our study, is a new aspect that should be considered in the counseling of patients with multiple UIAs.
Supplemental Material
SDC_results_table1_ – Supplemental material for Relative health-related quality of life after treatment of unruptured intracranial aneurysms: long-term outcomes and influencing factors
Supplemental material, SDC_results_table1_ for Relative health-related quality of life after treatment of unruptured intracranial aneurysms: long-term outcomes and influencing factors by Philipp Dammann, Paula Wittek, Marvin Darkwah Oppong, Bernd-Otto Hütter, Ramazan Jabbarli, Karsten Wrede, Isabel Wanke, Christoph Mönninghoff, Klaus Kaier, Benedikt Frank, Oliver Müller, Christoph Kleinschnitz, Michael Forsting and Ulrich Sure in Therapeutic Advances in Neurological Disorders
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.