
Abstract
Health-related quality of life was studied in 35 episodic cluster headache (CH) patients during and after the cluster period, using a generic (SF-36) and a headache-specific (MSQ2.1) instrument. The results were compared with those of age-and sex-matched migraineurs (n = 53) and healthy persons (n = 62). During the cluster period patients had lower scores than controls in all SF-36 and MSQ2.1 domains. The difference was significant for most SF-36 and all MSQ2.1 domains. Although CH patients had lower scores than migraineurs on most scales, the difference was significant only on SF-36 scores measuring bodily pain and social functioning. There was a good correlation between the two instruments. After the termination of the cluster period the quality of life of patients was similar to that of headache-free controls. Generic and headache-specific QoL are severely impaired in CH and this impairment is at least as severe as in migraine.
Keywords
Introduction
Health-related quality of life (HRQoL) represents the overall effect of illness and its therapy, as reported and evaluated by the patient (1). In this respect, HRQoL is to be distinguished from functional status, which provides an objective assessment of a patient's physical and emotional capabilities by medical personnel (2). Overall HRQoL is a concept that includes physical and mental functioning and well-being, social and role disability, and general health perceptions of the individual (3).
The standardized evaluation of HRQoL makes it possible to quantify the burden of illness. Generic instruments (measuring overall HRQoL) also permit the comparison of the impact of one illness with that of others and also with values of those who are well. Such information may, among others, be useful for the allocation of healthcare resources. On the other hand, disease-specific HRQoL instruments let us appreciate the particular impact of a selected condition, allow the comparison of conditions which share the dominant symptom and can be helpful in selecting the most appropriate therapy for the patients. They may also better reflect the specific concerns of patients with these disorders (4).
Cluster headache (CH) is characterized by recurrent unilateral attacks of severe headache, accompanied by local signs and symptoms of cranial autonomic dysfunction (5). It is reasonable to suppose that CH has a substantial impact on patients’ quality of life. CH attacks may occur several times throughout the day over periods of several weeks. The stabbing, often excruciating pain can disrupt the daytime activity both at the workplace and in the family setting. Leisure and social activities may also be affected. The night-time occurrence of attacks can lead to sleep deprivation, which further degrades performance (6). Personal accounts of patients underline these considerations (7).
While HRQoL in migraine and chronic headaches was widely studied, the effects of CH received much less attention. We therefore set out to assess overall and disease-specific HRQoL in episodic CH patients, using a generic and a headache-specific instrument.
Patients and methods
Patients
Thirty-five consecutive out-patients of the headache service of the Department of Neurology, Semmelweis University were involved. All fulfilled the International Headache Society criteria for episodic CH (5). Patients also having other significant headaches (migraine, chronic or frequent episodic tension-type headache, chronic daily headache) were not included. While most patients had no other medical problems, we did not exclude CH sufferers with concomitant illness, provided that they had CH as the main complaint at the time of the study. We excluded patients with severe or untreated disorders.
The patients filled in the questionnaires during their first visit due to the new CH period.
At least 3 months after the termination of the CH period telephone interviews were used to clarify the health status of the patients and then follow-up questionnaires were sent to them by mail. The results were compared with those of a group of migraineurs (n = 53) and a control group from the general population (n = 62) who did not have migraine, cluster or daily headaches. Both comparator groups were matched for sex and age. A detailed description of the control groups is to be found in Results.
Methods
We used the Hungarian versions of the generic HRQoL instrument SF-36 (8, 9), and MSQ version 2.1 (10, 11), a headache-sensitive instrument originally devised for the assessment of HRQoL in migraine. Both tests had been developed by the Medical Outcomes Trust. The domains measured by the respective instruments are listed in Table 1.
Quality of life domains as measured by the SF-36 and MSQ 2.1 instruments
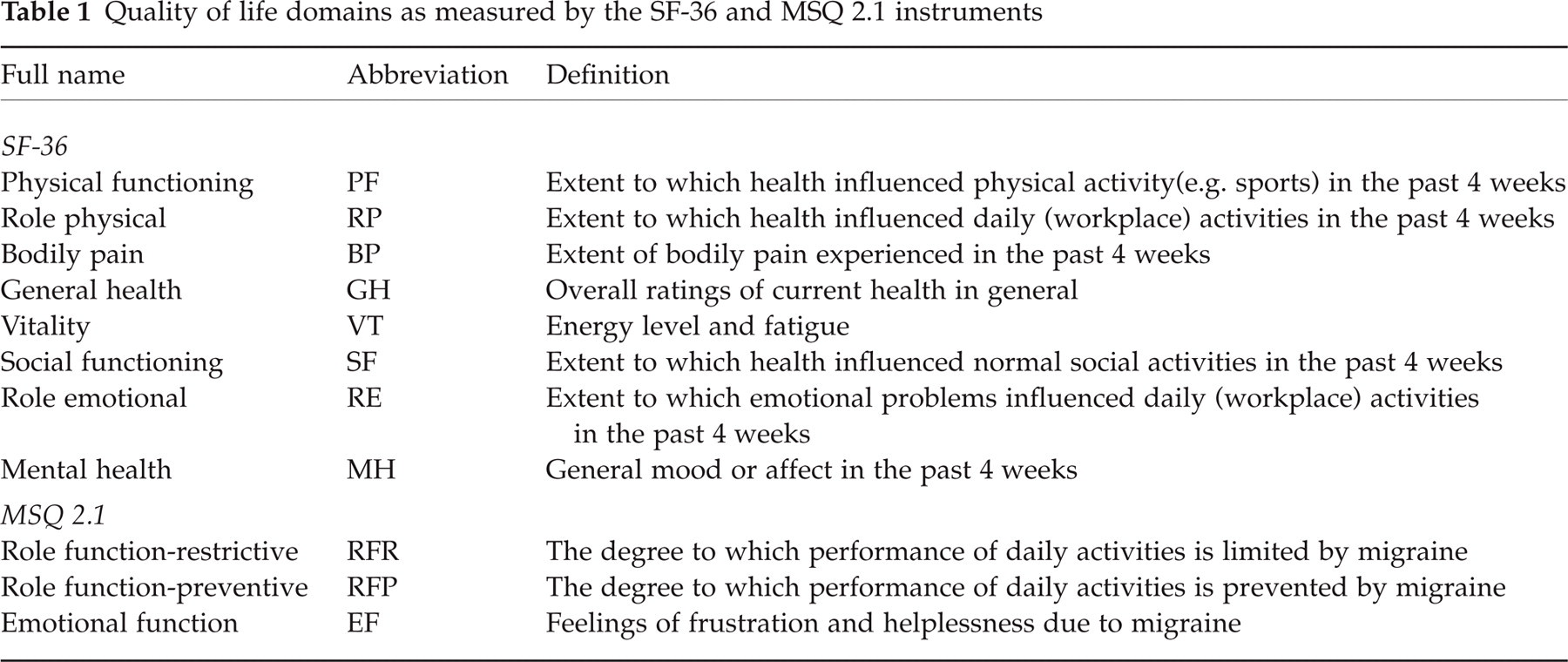
The SF-36 is a multipurpose, short-form generic health survey that yields an eight-scale profile of functional health and well-being by asking only 36 questions. The eight health concepts measured by SF-36 were selected from 40 included in the Medical Outcomes Study (MOS) that used a 149-item Functioning and Well-Being Profile (12). The 36 items of SF-36 are aggregated in eight scores, each representing 2–10 items. Table 1 lists the names and definitions of these scores. Four items [physical functioning (PF), role physical functioning (RP), bodily pain (BP) and general health (GH)] represent physical health and four [vitality (VT), social functioning (SF), role emotional functioning (RE), mental health (MH)] are related to mental health; accordingly, physical and mental composite scores can also be calculated (13). Extensive statistical testing proved that all items in each score met strict predefined criteria of convergent validity (i.e. each item was substantially related to the total score of that scale) and of discriminant validity (i.e. each item correlated significantly higher with its scale than with other scales) (14). While SF-36 includes eight of the most frequently measured health concepts, it does not address all important ones. Among the content areas not included in it are sleep adequacy, cognitive functioning, sexual functioning, health distress, family functioning, self-esteem, eating, recreation/hobbies and communication (13). As it is a generic measure, SF-36 does not gather data about symptoms or problems that are specific to one condition. Nevertheless, SF-36 was found to be a reliable and useful means of studying the functioning and well-being of patients, as testified by nearly 4000 publications to date and by translations used in more than 50 countries (13).
The recognition that generic HRQoL tools may not fully capture all aspects that are relevant to migraineurs led to the development of several migraine-specific instruments. The MSQ was developed for the assessment of long-term impact of migraine. The currently used version, MSQ2.1, contains 14 questions measuring three dimensions that were found to represent the effect of migraine on the sufferer. Seven items measure the degree to which performance of normal activities (work and leisure activities, interaction with family members, but also concentration, energy and tiredness) is limited by migraine (role-restrictive dimension). Four items gather information about the extent of migraine interrupting these activities (role-preventing dimension). Three items measure the emotional effects of migraine (feeling frustrated, feeling like a burden to others, and being afraid of letting others down). MSQ2.1 was found to be a reliable instrument for assessing HRQoL in migraine, and showed modest to moderate correlation with migraine symptoms (15).
The wording of MSQ2.1 contains no explicit distinction as to what aspect of migraine is responsible for the limitation (i.e. whether it was caused by the pain, the accompanying symptoms, the aura, if any, or a combination of these). In order to make data comparable we had to change the wording of MSQ2.1 by substituting ’migraine’ with ’headache attacks’ in all three study groups. As in non-medical Hungarian usage ’migraine’ is used interchangeably with ’(severe) headache attack’, we felt that this change would not compromise the study. Moreover, head pain is probably the most important source of migraineurs’ limitations, as suggested by a recent study where rapid, complete, and sustained pain relief were shown to be the main determinants of HRQoL (16). The high frequency of ’migrainous’ headache accompaniments (nausea, vomiting, photo- or phonophobia) in our CH sample (see Table 2), similar to those observed by Bahra et al. (17), further decreases the possibility that the different accompanying symptoms of CH and migraine would cause large-scale differences in HRQoL. Although we are not aware of MSQ2.1 being used in conditions other than migraine, we think that its application in this CH sample is justified and MSQ2.1 scores of CH patients and migraineurs can be compared.
Demographic data of patients and controls
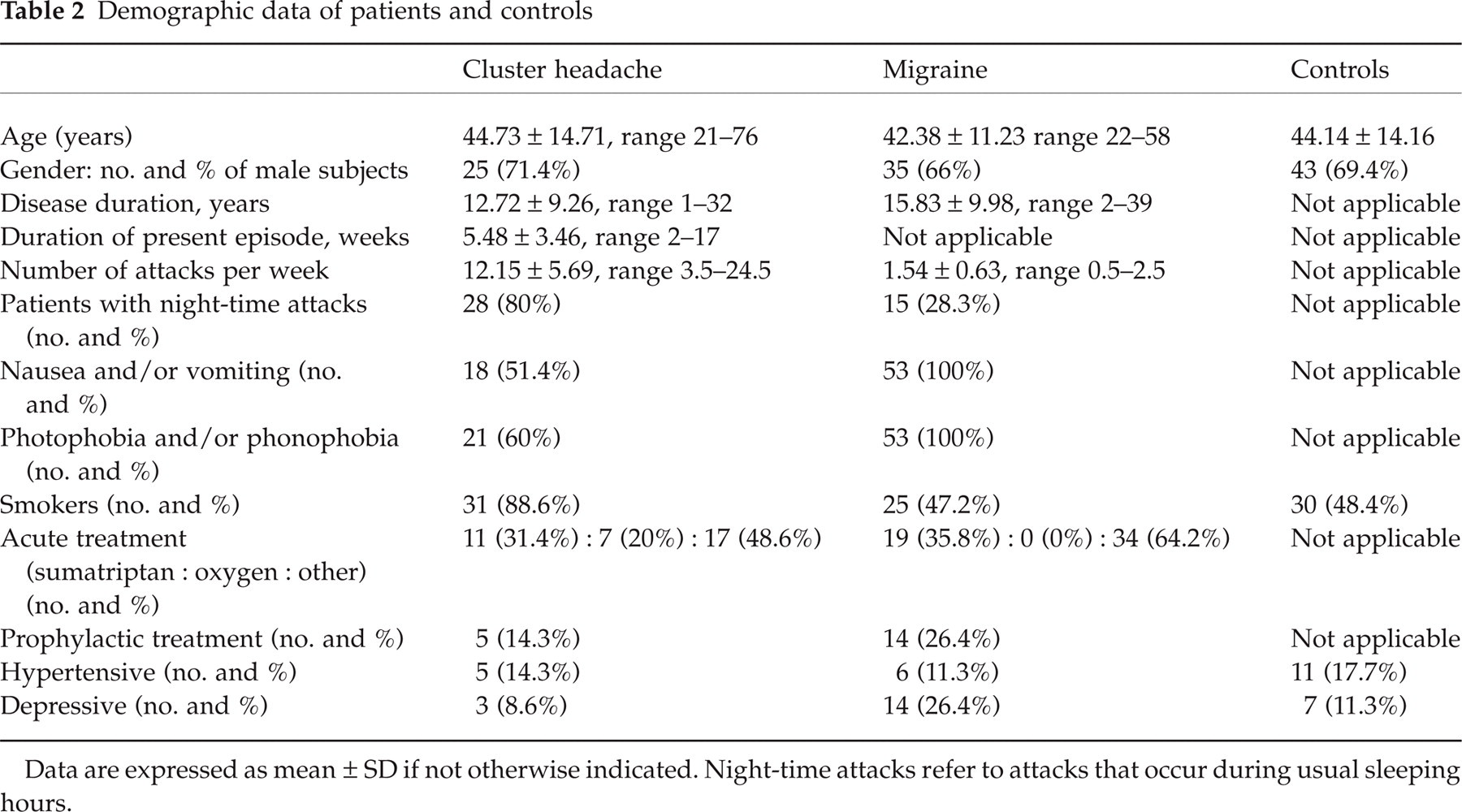
Data are expressed as mean ± SD if not otherwise indicated. Night-time attacks refer to attacks that occur during usual sleeping hours.
For both questionnaires, scores were calculated according to the respective guidelines (18–20) and then transformed to scales from 0 to 100 (0 meaning the worst possible condition).
Statistics were calculated using SPSS and Graph Pad software. Kolmogorov–Smirnov tests with Lilliefors’ correction method were used to test for normality of data. As the data distribution of most HRQoL domains was not Gaussian, Wilcoxon signed rank tests were used to check differences within the CH group (during vs. after the episode), and Kruskal–Wallis ANOVA with Dunn's multiple comparisons tests for differences between groups. Spearman's non-parametric tests were used to check for correlation between the two instruments and between HRQoL scores and patient characteristics.
Results
Patient characteristics
A total of 35 CH patients were studied. Twenty-four (69%) did not have any relevant medical condition other than CH. Eleven patients (31%) also had other health problems, including five cases with medically treated hypertension, three with mild depression, one with low back pain and one with essential tremor. One patient had Type 2 diabetes mellitus, while one of the hypertensive patients had a mild degree of leukoaraiosis confirmed by magnetic resonance imaging. The majority of CH patients did not receive prophylactic treatment at the time of the study. In five, prophylactic verapamil treatment had already been started, but they were still experiencing daily attacks. Only 11 (31/%) of the 35 used subcutaneous sumatriptan as abortive agent; other options were oxygen, indomethacin or soluble non-steroidal anti-inflammatory drugs. The infrequent use of sumatriptan was due to financial issues (the local health system covers only 50% of its price).
The demographic data of the patient groups is presented in Table 2.
The two comparator groups were matched to the CH group for sex and age. There was no significant difference in disease duration and percentage of sumatriptan users in the CH and migraine groups. The percentage of depressed patients was significantly greater and that of hypertensive patients somewhat smaller in migraineurs; the concomitant disease profile in the headache-free control group was similar to the CH group.
Generic HRQoL
During the cluster period, CH patients had lower scores in all SF-36 domains than non-migrainous controls. The difference was statistically significant in six domains (role physical, bodily pain, general health, vitality, social functioning and mental health). CH patients scored significantly lower than migraineurs in the bodily pain and social functioning domains. Table 3 summarizes SF-36 scores and P-values.
Generic HRQoL: SF-36 scores of cluster headache (CH) patients: comparison with migraineurs and controls

Kruskal–Wallis ANOVA and Dunn's multiple comparisons tests. ns, Not significant (P > 0.05); PF, physical functioning; RP, role physical functioning; BP, bodily pain; GH, general health, VT, vitality; SF, social functioning; RE, role emotional functioning, MH, mental health.
After the termination of the cluster period, CH patients’ scores significantly improved in the role-physical, bodily pain and social functioning domains (P < 0.002). Vitality and mental health scores also tended to improve (P = 0.063 and P = 0.074, respectively). There was no statistical difference between CH patients outside the bout and headache-free controls. There was no correlation between SF-36 scores and the characteristics (age, disease duration, length of the present CH period and number of attacks) of CH patients, with the exception of a correlation between VT scores and age (r = 0.402, P = 0.0275) and MH with disease duration (r = 0.621, P = 0.0103). There was no significant difference between the scores of sumatriptan users and non-users.
Migraineurs scored lower than controls in all SF-36 domains; the differences were statistically significant for physical functioning, role-physical, bodily pain, general health and social functioning scores.
Headache-specific HRQoL
Patients during the CH period scored the lowest on all three MSQ 2.1 subscores. There was a significant difference between CH patients and controls as well as between migraineurs and controls (P < 0.001 on all subscores for both patient groups vs. controls). The difference between CH patients’ scores and those of migraineurs was not significant. After the bout, CH patients’ subscores improved dramatically and were similar to the headache-free control values. There was no correlation between MSQ2.1 scores and the characteristics (age, disease duration, length of the CH period, number of attacks, type of abortive drug) of CH patients. MSQ2.1 scores and P-values are presented in Table 4.
Headache-specific HRQoL in cluster headache (CH) patients, migraineurs and controls: MSQ2.1 scores and P-values (Kruskal–Wallis ANOVA and Dunn's multiple comparisons tests)
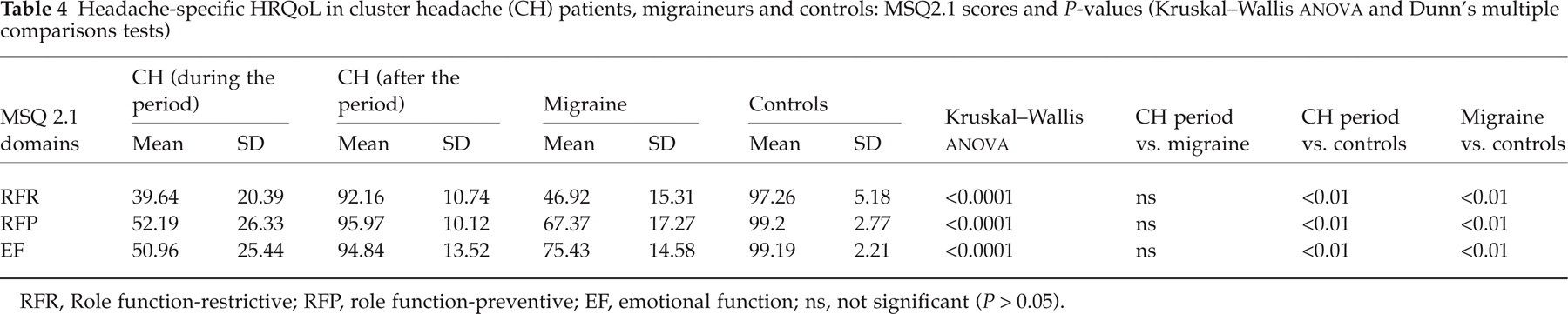
RFR, Role function-restrictive; RFP, role function-preventive; EF, emotional function; ns, not significant (P > 0.05).
Correlation between the SF-36 and MSQ2.1 questionnaires
As expected, the bodily pain subscore of SF-36 correlated with all MSQ2.1 subscores: more severe pain was associated with more pronounced limitations in role and emotional functioning. Limitations in the role-physical domain also correlated with loss of functioning in all MSQ2.1 subscores. Of the four SF-36 subscores reflecting physical health (13), role-physical and bodily pain scores correlated with both the role [role function-restrictive (RFR), role function-preventative (RFP)] and emotional (EF) components of MSQ2.1, while SF-36's physical functioning score correlated with emotional functioning on MSQ2.1. The fourth, i.e. the general health score, showed no correlation. Of the four SF-36 subscores related to mental health (vitality, social functioning, role emotional and mental health) three (VT, SF and MH) positively correlated with emotional functioning, and two (VT and RE) with the role-function preventing aspect of CH. Surprisingly, there was no correlation between physical functioning and the role functioning items of MSQ2.1 or between the emotional functioning subscores of the two instruments (RE and EF). The correlation between the SF-36 and MSQ2.1 subscores is presented in Table 5.
Correlation between SF-36 and MSQ2.1 subscores

SF-36 domains: PF, physical functioning; RP, role physical functioning; BP, bodily pain; GH, general health, VT, vitality; SF, social functioning; RE, role emotional functioning, MH, mental health. MSQ2.1 domains: RFR, role function-restrictive; RFP, role function-preventative; EF, emotional function.
Discussion
In this study, generic and headache-specific HRQoL were found to be seriously impaired during the cluster period. This impairment was at least as severe as in migraineurs for most HRQoL domains; bodily pain and social functioning were significantly worse in CH.
Using generic HRQoL measures for the comparison of different groups suffers from the inherent disadvantage of not clarifying whether the results are caused by the index condition (at present, headache) or by concomitant illness. We tried to correct the possible bias by selecting control populations with a similar concomitant disease profile. Other possibilities would be either the careful elimination of all patients with any concomitant illness, or the study of large numbers of patients selected from the general population. Due to the small prevalence of CH none of these seemed feasible.
In the past decade, various studies have addressed the impact of migraine, tension-type headache and chronic daily headache on HRQoL. Studies with generic HRQoL instruments have established that the impact of migraine on patients’ health status and quality of life may be similar to, or even greater than, that of other chronic disorders such as osteoarthritis (21), diabetes (21), low back pain (22), depression (22, 23), or congestive heart failure (22).
By contrast, there is only a limited amount of data concerning overall quality of life in CH. One study used the MOS Short Form Health Survey (SF-20) to assess the QoL and well-being of 208 consecutive patients in a headache clinic (24). SF-20 measures physical, role and social functioning, mental health, pain and health perceptions; many of its questions are included in SF-36 but the latter also studies emotional role functioning and vitality and collects more information about physical functioning, physical role functioning and pain. Thirteen CH sufferers were included; other diagnoses were migraine, tension-type headache and ‘mixed headache’. CH patients had significantly worse pain scores and greater limitation in social functioning than controls or migraine patients. Physical functions and general health perception of CH patients, however, were generally well preserved. The latter finding is in contrast with our present observations of impaired general health during the cluster period. The difference between the two generic HRQoL instruments, the small number of CH patients in the SF-20 study and the fact that a part of them were examined outside the bout (25), makes the interpretation of data somewhat difficult.
Recently D’Amico et al. administered the SF-36 to 56 Italian CH patients (34 episodic and 22 chronic) during the active periods and compared the results with Italian normative data (25). Cluster headache was associated with a significant decrease (P < 0.0001) in six of the eight scales (role physical, bodily pain, general health, social functioning, role emotional and mental health). It is of interest that in the present study five of these scales (role physical, bodily pain, general health, social functioning and mental health) were also significantly worse. There was no significant difference between the HRQoL of episodic and chronic CH patients. Surprisingly, the comparison of sumatriptan users and those using a different abortive drug did not show any significant difference. Episodic patients were studied only in the active phase and mention was not made of any concomitant disease the patients may have had. Notwithstanding these limitations, there is a striking similarity between the SF-36 profiles of Italian and Hungarian CH patients during the episode: five of the eight scales decreased in both populations, while physical functioning was not statistically different from controls. Italian CH patients had worse emotional role functioning than controls whereas Hungarian patients scored lower on the vitality subscore. On the whole, these data indicate that the HRQoL impairment in CH is quite uniform in different cultural and linguistic contexts.
The generic instrument SF-36 makes it possible to compare HRQoL in different medical conditions. Based on literature searches, CH patients seem to have a very unfavourable profile. All SF-36 subscores of the present CH population were significantly lower than those of patients with previous myocardial infarction (26). CH patients had significantly worse scores in all SF-36 dimensions except physical functioning than patients who had survived peritonitis (27). CH patients had more severe bodily pain, lower vitality, worse social functioning and mental health than patients with surgically treated hip arthrosis (28), peripheral artery disease (29), or coronary artery disease (29). The comparison of SF-36 scores obtained in different languages and cultures is to be made with caution (30, 31). Nevertheless, as the similar profiles of Italian (25) and Hungarian CH sufferers indicate that the consequences of CH may be similar in other countries, too, we think that comparisons between the effects of CH and other medical conditions on HRQoL are not entirely unjustified.
MSQ2.1 has been widely used to study migraine-specific quality of life (15, 31–33). Results of a multinational investigation of HRQoL in migraineurs suggest that while migraine does interfere with quality of life, MSQ2.1 scores are also dependent on the socio-cultural setting (31). In the present study, migraineurs’ role-function restrictive (RFR) scores were comparable to values obtained in Australia and Canada, while role-function preventive (RFP) and emotional functioning (EF) scores resembled Italian and Swedish values (31). MSQ2.1 was found to be more sensitive in detecting HRQoL changes of migraineurs than SF-36 (33). The same was observed when comparing scores of the present CH population during and after the bout. Due to its sensitivity, relative brevity and simplicity, MSQ2.1 may be useful as a measure of therapeutic efficacy in CH drug trials.
Most of the items of SF-36 and all items of MSQ 2.1 concern the limitations in the 4 weeks preceding the completion of the instrument. The similar time window allows for a comparison between the two instruments and also lets us appreciate the impact of the condition in a more precise way. In the present CH population the two instruments showed good correlation. It was surprising that limitations caused by CH were not significantly more severe than those of migraineurs, as would have been expected from personal accounts of patients (not included in the present study) who suffer from both headache types. Being a generic HRQoL measure, SF-36 may not be sensitive enough to certain effects of CH on the patients’ functionality and well-being. The relative insensitivity of MSQ to the consequences of CH may be explained by the item selection process during the development of MSQ, which aimed at achieving a highly migraine-specific measure (15). We feel that these two instruments may not capture some essential aspects of CH. A simple example for the different effects of CH and migraine on QOL, not measured by SF-36 or MSQ, would be the way these headaches influence the quality of sleep. Differences in item selection and concept definition may also explain why subscales measuring seemingly related concepts (e.g. SF-36's role-emotional subscale and the emotional functioning subscale of MSQ2.1) do not correlate. That the partial lack of correlation between the two instruments is not caused solely by the difference between CH and migraine is underlined by the finding of only low to modest correlation (r < 0.4) between MSQ2.1 and SF-36's physical and mental composite scores in a large sample of migraineurs (15).
The present study, as well as the previous ones, may be criticised for the method of patient selection. Although CH is a severe condition that prompts medical consultation in most cases (34), patients with more severe limitations may be more motivated to seek medical advice in a specialized headache centre. It is therefore possible that the self-perceived health limitations of the present CH sample are more severe than those of an ‘average’ CH sufferer. A population-based approach, as recently carried out on a Dutch sample of migraineurs (35), may yield more precise results. In spite of these limitations, this study further demonstrates that CH severely affects the sufferer's functioning and well-being during the active period. The limitations are at least as severe as those caused by migraine and are probably more severe than in a number of important conditions. An early diagnosis as well as adequate acute and preventive treatment measures are essential to reduce this burden.
Copyright information
SF-36 Health Survey Copyright © 1992, Medical Outcomes Trust. All rights reserved. MSQ vs. 2.1 Copyright © 1992, 1996, 1998, Glaxo Wellcome Inc. All rights reserved.