
Abstract
Background:
The aim of this work was to report a case of an acute motor and sensory axonal neuropathy (AMSAN) treated with propionate to evaluate its therapeutic potential in AMSAN.
Materials and methods:
The patient was investigated by clinical examination, electroneurography, high-resolution nerve ultrasound and confocal corneal microscopy at baseline and the 2 month follow up. We compared the outcome with those of five other patients with acute motor axonal neuropathy (AMAN) and AMSAN of who were referred to our neurology department in the past 5 years.
Results:
Considering the poor prognosis of patients with acute axonal neuropathies and in comparison with the previously treated patients with AMAN or AMSAN in our clinic, the regression of our patient’s symptoms and the improvement in the additional examinations under propionate seemed exceptionally good.
Conclusion:
Propionate may have an additional therapeutic effect in autoimmune inflammatory neuropathies.
Introduction
Acute motor/motor-sensory axonal neuropathy (AMAN/AMSAN) is an axonal subtype of Guillain-Barré syndrome (GBS) and was first described 1986 by Feasby and colleagues. 1 Clinical symptoms of AMAN are characterized by an acute weakness of the limbs, often accompanied with respiratory failure, at times with cranial nerve disorders and vegetative involvement. In AMSAN sensory disturbances additionally occur. The course of disease is similar to the classical GBS, but more severe and prolonged with frequent ventilator dependency, slow recovery and significant residues.2–8 The therapy of AMAN and AMSAN is based on that of the acute inflammatory demyelinating polyradiculoneuropathy (AIDP), 9 that is, plasma exchange (PLEX) and intravenous immunoglobulin (IVIG), while the benefit of corticosteroids remains ambiguous. 2
In the past 5 years five patients with AMAN and AMSAN were referred to our neurology department. Of these, four had a severe tetraparesis with a modified Rankin scale (mRS) of 4 or 5 at admission. Therapy response was poor to moderate, and residues after therapy were evident in all five patients. A total of four patients were still severely disabled (mRS 4 or 5) at discharge (Table 1).
Patients with AMAN or AMSAN treated in our department between 2012 and 2017. Patient no. 6 was additionally treated with propionate.
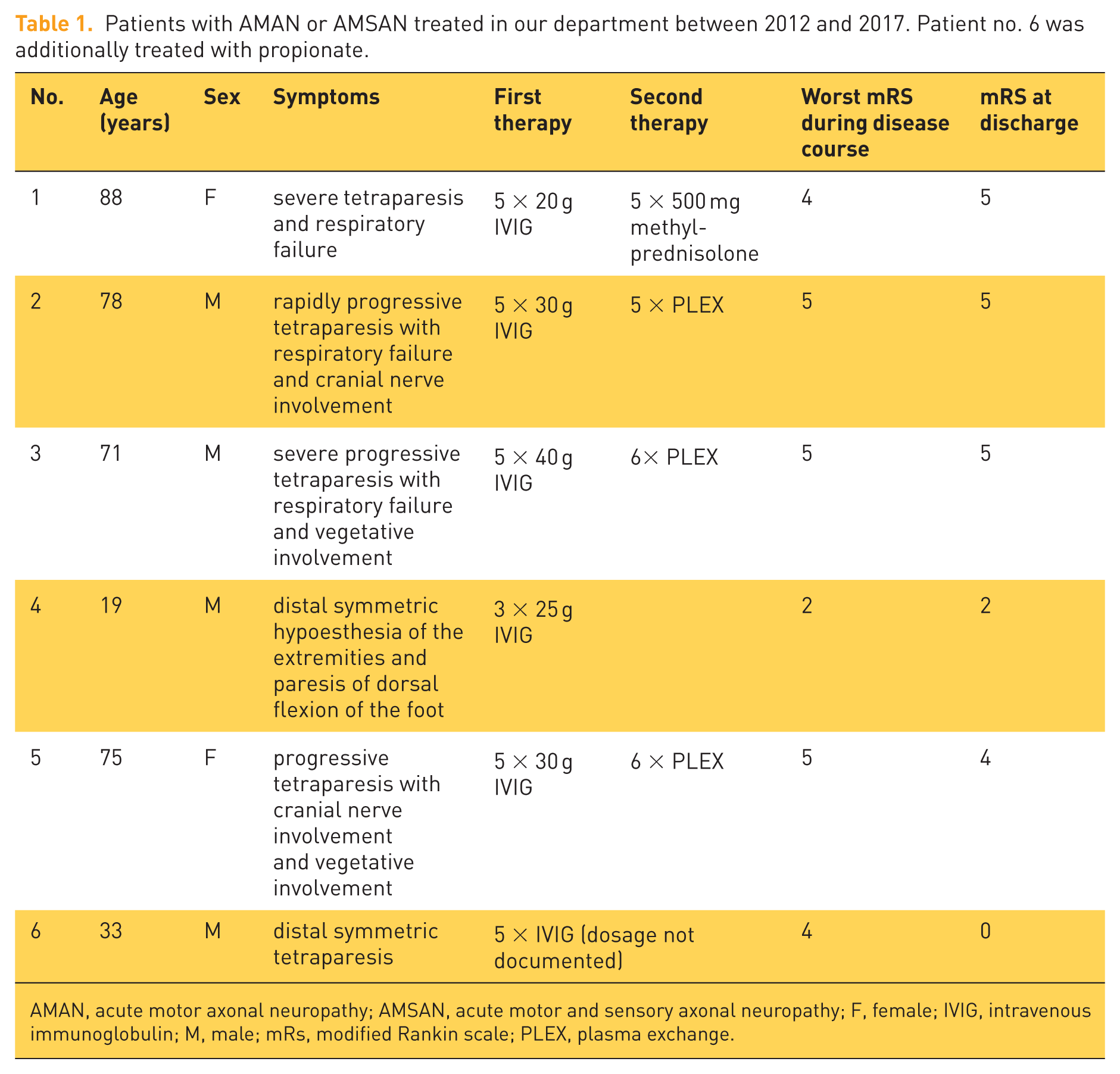
AMAN, acute motor axonal neuropathy; AMSAN, acute motor and sensory axonal neuropathy; F, female; IVIG, intravenous immunoglobulin; M, male; mRs, modified Rankin scale; PLEX, plasma exchange.
Based on data highlighting the beneficial effect of the dietary short chain fatty acid propionate on the gut associated immune regulation via regulatory T-cells in multiple sclerosis, 10 we set out to evaluate its therapeutic potential in AMSAN.
Hence, when a patient with AMSAN was referred to our clinic recently we added propionate in the recovery phase of the disease.
Materials and methods
The propionate-treated patient was investigated by clinical examination, electroneurography, high-resolution nerve ultrasound and confocal corneal microscopy (CCM) at baseline and at the 2 month follow up. CCM, a non-invasive technique to visualize the corneal sub-basal nerve plexus, has been used in the diagnostic of various neuropathies in the last years. 11 Stettner and colleagues (2015) showed that CCM identifies axonal loss in immune-mediated neuropathies and reveals alterations of distinct cells around the corneal nerve plexus. 12 CCM was performed with a Heidelberg Retina Tomograph III with a Rostock cornea module, ACC-Metrics software, version 2.0 (Xin Chen and Mohammad Dabbah, Manchester, UK), and the average of five high-quality images was calculated.
We compared the clinical course and the outcome of patients with AMAN/AMSAN that were treated with the established therapies in our department in the past 5 years with one patient with AMSAN, whom we additionally treated with propionate in the recovery phase of the disease. Written informed consent was obtained from the patient treated with propionate for publication as a case report. The data about the other AMAN/AMSAN patients were obtained during a previous study about inflammatory polyneuropathies, which had recruited since 2010 and was approved by the ethics committee of the Ruhr University Bochum, Germany (reg. no. 4382-12). This ethics approval and informed consent for the previous study covered the individual patient information included in the current case report.
Case history and results
A 33-year-old man presented in our department 18 days after diagnosis of AMAN during a vacation in Bali. After feverish diarrhea, he reported fasciculation of the limb muscles, followed by a weakness in the arms and legs. The mRS at this time point was 4. In a hospital in Bali, the diagnosis of an AMAN was established based on the clinical course and electrophysiological findings. A lumbar puncture was rejected by the patient. He was treated with immunoglobulins over 5 days (dosage not documented), which led to an improvement of the symptoms. At admission to our clinic 18 days after diagnosis in Bali, a distal symmetric tetraparesis with muscle strength grade 4 (of 5; MRC) of the hands, 4+ of arm flexion and 4 of foot elevation was observed and the patellar and Achilles tendon reflexes were diminished. Electroneurography (ENG) showed an axonal sensorimotor polyneuropathy with motor emphasis. Electromyography revealed distinct abnormal spontaneous activity in the tibialis anterior muscle. Cerebrospinal fluid (CSF) analysis showed a normal cell count with mildly elevated protein of 583 mg/l. High-resolution nerve ultrasound (HRUS) showed an enlargement of the tibial nerve, the ulnar nerve and the radial nerve, as may be seen in immune neuropathy.13,14 CCM revealed a significant reduction in nerve fiber length, density and branching density, compatible with small-fiber neuropathy. A therapy with propionate at a daily dosage of 2 × 500 mg was started to potentially accelerate the recovery phase. It was taken for the entire follow-up period of 2 months without any breaks. No side effects were reported by the patient. The formulation was sodium propionate in a capsule of gelatin, manufactured by Flexopharm Brain GmbH & Co. KG, Herne, Germany. In the follow-up examination 2 months later, the patient reported a good condition of health with only slight fatigue. Muscle strength was completely normalized in all limbs that had previously revealed a paresis, and the clinical examination was normal. Electrophysiological exams also showed a considerable improvement (Table 2). Abnormal spontaneous activity in electromyography was no longer detectable. Consistently, CCM showed normalized results, while nerve ultrasound slightly improved (Table 2).
Results of ENG, HRUS and CCM of the propionate-treated AMSAN patient at baseline and follow-up visit. Values outside the normal range are highlighted.

AMSAN, acute motor and sensory axonal neuropathy; CCM, confocal corneal microscopy; ENG, electroneurography; HRUS, high-resolution nerve ultrasound.
Discussion
AMAN and AMSAN as axonal subtypes of GBS are reported to have a more severe course than classical GBS, and patients regularly suffer from disabling residues.2,3 Propionate was previously described as an immune-regulating drug in multiple sclerosis. 10 We treated one patient with AMSAN with propionate with a daily dosage of 2 × 500 mg. Residual disabilities after classical GBS were previously described to persist in over 60% of patients 10 years after disease onset 7 and fatigue persists in almost half of patients more than 20 years after the acute disease. 8 Considering the poor prognosis of patients with acute axonal neuropathies, the regression of our patient’s symptoms under propionate seemed extraordinary. In regard to the applied diagnostics and published CCM normative values, 15 CCM in particular showed an extensive recovery in short-term follow up. Nevertheless, to our knowledge, an investigation with CCM in acute immune-mediated neuropathy has never been reported before. In our case, HRUS showed some abnormalities of peripheral nerves, with regression at the 2 month follow up. HRUS in GBS was reported to show abnormalities of the peripheral nerves; 16 however, this was also described to be relatively uncommon or to show no correlation with clinical evolution.17–19
Compared with the other patients with AMAN or AMSAN treated in our clinic, the patient treated with propionate had an excellent outcome with an mRS of 0. Regarding age and sex, the current propionate-treated patient can best be compared with patient no. 4 (Table 1). Though patient no. 4 had less severe paresis at admission, the outcome of patient no. 4 was worse than the outcome of the propionate-treated patient (mRS of 2 versus 0). The other patients mentioned in Table 1 had more severe symptoms, and hence, a worse outcome than the propionate-treated patient. The recovery of the patient treated with propionate therefore seemed extraordinary. This result may suggest a therapeutic effect of propionate in acute inflammatory axonal neuropathies. However, AMSAN and AMAN patients may also show prompt recovery because of distal reversible conduction failure 20 or reversible very distal motor nerve terminal degeneration. 21 Furthermore, no investigations directly showing the evidence of the immunological effect of propionate were performed in this case report.
Further studies are warranted to explore the effect of propionate and to show whether propionate treatment in acute inflammatory neuropathies in a broader range may be useful. To prove the therapeutic efficacy of propionate in autoimmune inflammatory neuropathies, controlled study data are needed.
Conclusion
With regard to the worse prognosis of patients with acute axonal neuropathies, and in comparison with the previously treated patients with AMAN or AMSAN in our clinic, the outcome of the patient with AMSAN treated with propionate seemed extraordinary. This supports the suggestion that recruitment of regulatory T-lymphocytes through propionate may have an additional therapeutic effect in autoimmune inflammatory neuropathies.
Footnotes
Author contributions
The following author contributions are acknowledged in the preparation of this manuscript. Min-Suk Yoon: study planning, data collection, drafting and revising the manuscript, critical comments during data collection and manuscript revision.
Kalliopi Pitarokoili: critical comments during data collection and manuscript revision.
Dietrich Sturm: data collection, critical comments during data collection and manuscript revision.
Aiden Haghikia: study planning, critical comments during data collection and manuscript revision.
Ralf Gold: Critical comments during data collection and manuscript revision.
Anna Lena Fisse: study planning, data collection, drafting and revising the manuscript, critical comments during data collection and manuscript revision.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Min-Suk Yoon: received speakers’ honoraria from CSL Behring, Grifols and a scientific grant from CSL Behring, not related to the manuscript.
Kalliopi Pitarokoili: received travel grants and speakers’ honoraria from Novartis, Biogen idec, Teva, Bayer and Grifols, all not related to the manuscript.
Dietrich Sturm: received funding from the Ruhr University, Bochum (FORUM-Program), not related to the manuscript.
Aiden Haghikia: received speaker’s honoraria from Bayer Healthcare, Biogen Idec, Merck Serono, Novartis and Teva.
Ralf Gold: received consultation fees and speaker honoraria from Bayer Schering, Biogen idec, Merck Serono, Novartis, Sanofi-Aventis and Teva. He also acknowledges grant support from Bayer Schering, Biogen idec, Merck Serono, Sanofi-Aventis and Teva, none related to this manuscript.
Anna Lena Fisse: none.