
Abstract
Background:
‘Thromboinflammation’ describes a novel concept in stroke pathophysiology that has opened up the possibility of immunotherapeutic approaches which could become promising strategies for targeted stroke therapies in the future.
Methods:
We reviewed current evidence for agents approved for multiple sclerosis in preclinical and clinical stroke studies. A systematic review was performed in accordance with the PRISMA statement, searching MEDLINE, the Cochrane Central Register of Controlled Trials, and reference lists of articles published until 16 October 2017.
Results:
The review included 52 of 629 identified studies, consisting of 5 clinical and 47 preclinical trials. Most of the studies showed beneficial effects of the evaluated immunotherapeutic drugs in terms of reduction in morphological lesion size and improvement in functional outcome. Nevertheless, the significance of these findings is limited due to the high degree of heterogeneity.
Conclusions:
Immunotherapy of stroke might be effective and could become a promising treatment strategy, but larger clinical trials with standardized interventions and outcome measures are needed.
Keywords
Introduction
The concept of ‘thromboinflammation’ describes the pathophysiological link between thrombus formation, that is, mechanisms related to platelet aggregation and plasmatic coagulation, and inflammation in the development of ischaemic stroke (IS). 1
With the help of murine stroke models and transgenic mouse strains, it has been demonstrated by independent groups that immunological processes involving the innate or adaptive immune system modulate IS pathophysiology. Histopathological findings demonstrating immune cell infiltration in the ischaemic brain were reported as early as the 1990s, but the pathophysiological relevance remained unclear. 2 Yilmaz and coworkers were the first to show that Rag1−/− mice, that is, mice lacking lymphocytes, develop smaller cerebral infarctions compared with wild-type animals. 3 This observation paved the way for rodent stroke studies analysing immunomodulating therapies with agents that have already been approved for the treatment of patients with multiple sclerosis. As the majority of rodent studies had positive outcomes, in the next step, the first clinical trials in stroke patients were started.
The aim of our study was to systematically assess the published preclinical and clinical studies that analysed an immunotherapeutic compound approved for multiple sclerosis in stroke.
Methods
We conducted a systematic review and followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 4
Prior to systematically reviewing the literature, the following eligibility criteria were defined: (a) clinical studies: randomized controlled trials (RCTs) or prospective studies with or without a control group if they analysed a compound approved for multiple sclerosis in patients aged 18 years or older with stroke [cerebral ischaemia or spontaneous intracranial haemorrhage (ICH)] or transient ischaemic attack; (b) animal studies that analysed a compound approved for multiple sclerosis in an experimental stroke model. Publications about spinal cord ischaemia and subarachnoid haemorrhages have been excluded due to particular pathophysiological mechanisms.
The main outcome measures that have been considered were mainly stroke volume and functional deficits. In part, additional outcomes, such as brain oedema, local brain inflammation or systemic cytokine levels, have been assessed. Due to space restrictions, it has been necessary to limit Tables 1–6 to principal content. Because of the pronounced heterogeneity of the study design, stroke model, intervention and outcome variables, it was not possible to calculate a meaningful meta-analysis for any of the outcome variables.
Characteristics of preclinical studies analysing glatiramer acetate.
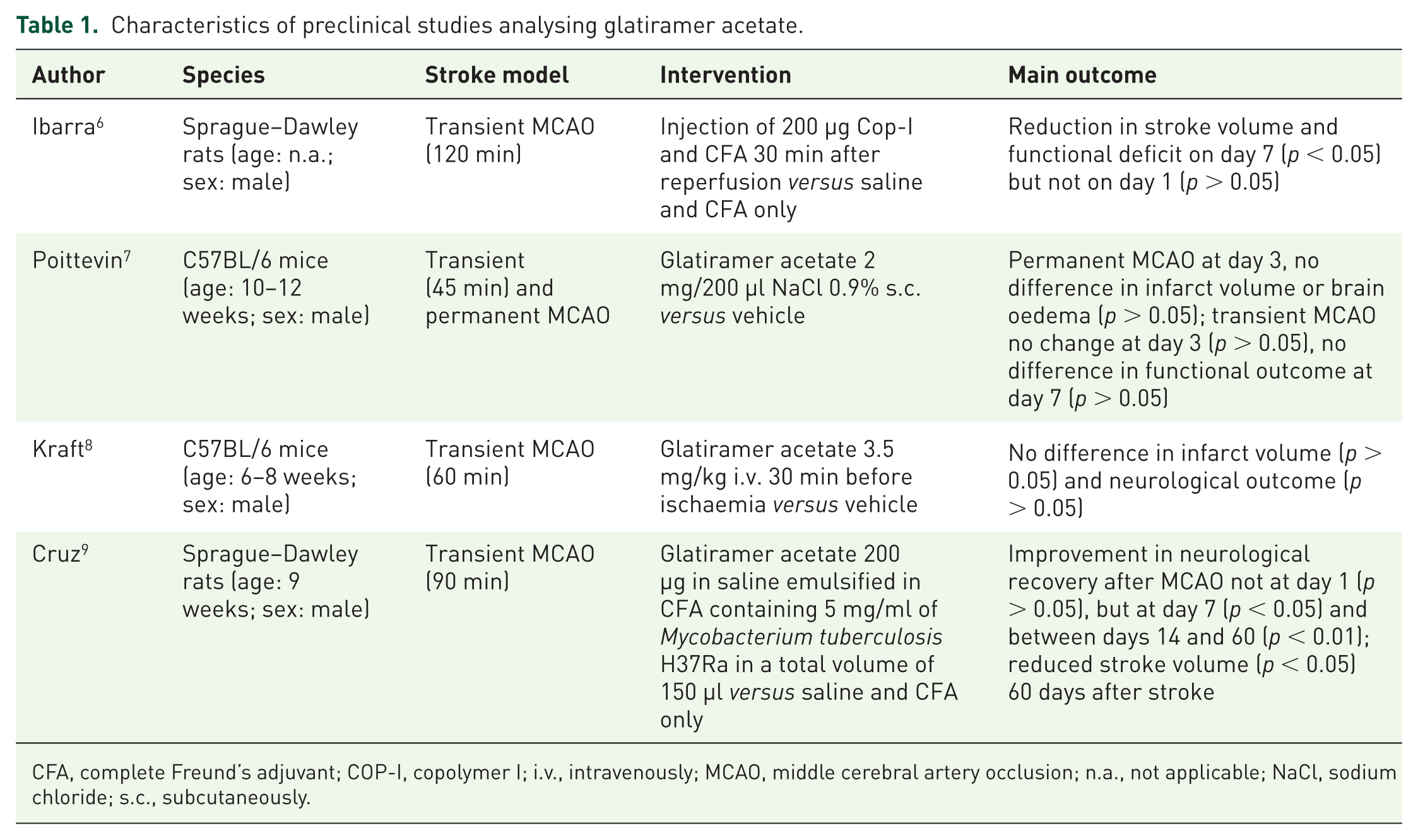
CFA, complete Freund’s adjuvant; COP-I, copolymer I; i.v., intravenously; MCAO, middle cerebral artery occlusion; n.a., not applicable; NaCl, sodium chloride; s.c., subcutaneously.
Characteristics of preclinical studies analysing interferon β.
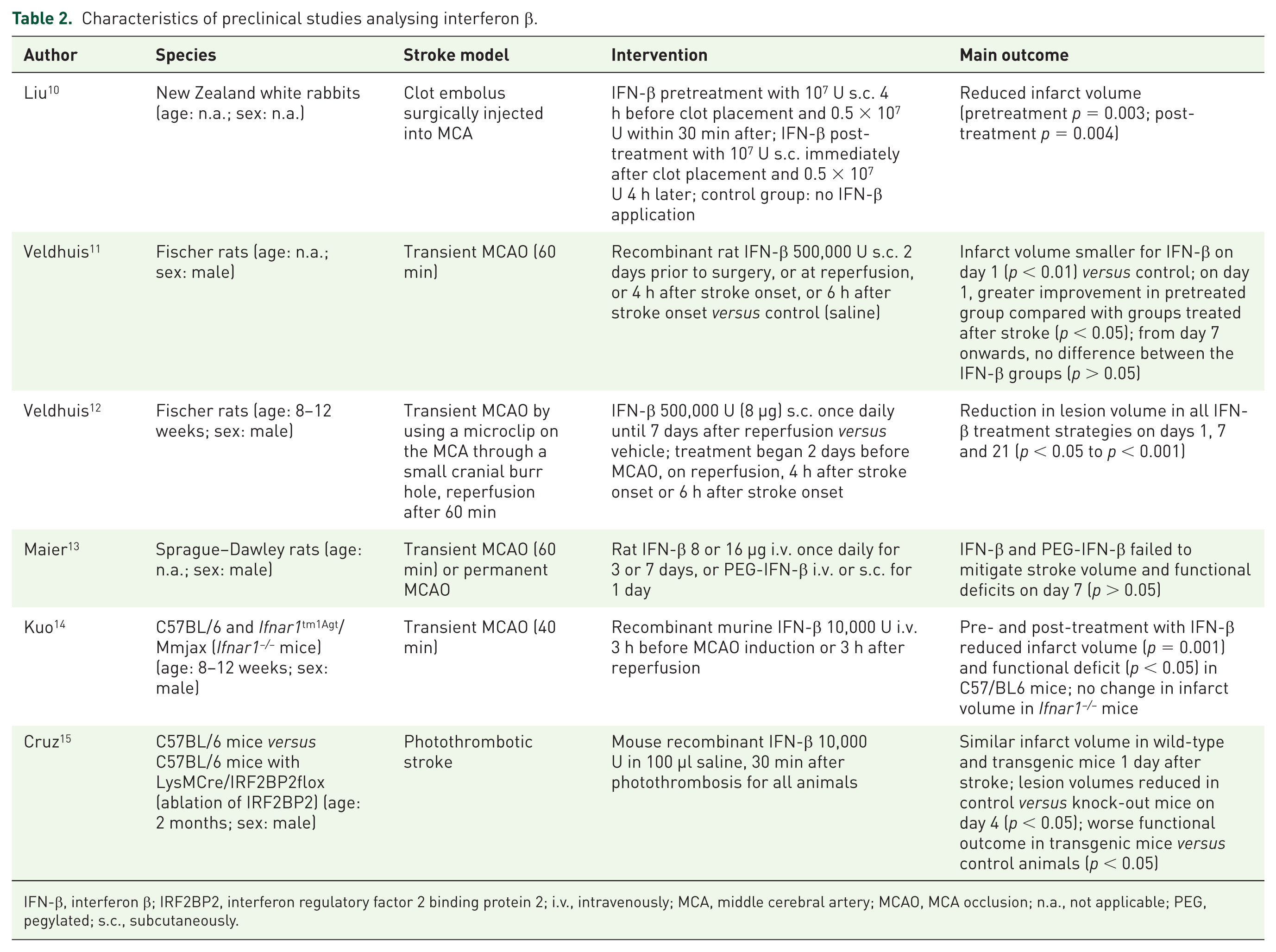
IFN-β, interferon β; IRF2BP2, interferon regulatory factor 2 binding protein 2; i.v., intravenously; MCA, middle cerebral artery; MCAO, MCA occlusion; n.a., not applicable; PEG, pegylated; s.c., subcutaneously.
Characteristics of preclinical studies analysing fingolimod.

BBB, blood–brain barrier; DMSO, dimethyl sulphoxide; FTY720, fingolimod; HPC, hypoxic preconditioning; ICH, intracerebral haemorrhage; i.p., intraperitoneally; i.v., intravenously; MCAO, middle cerebral artery occlusion; n.a., not applicable; PBS, phosphate-buffered saline; p.o., per os; rt-PA, recombinant-tissue plasminogen activator.
Characteristics of preclinical studies analysing natalizumab.

ICH, intracranial haemorrhage; i.p., intraperitoneally; i.v., intravenously; MCAO, middle cerebral artery occlusion; n.a., not applicable; SHR, spontaneously hypertensive rat.
Characteristics of preclinical studies analysing dimethyl fumarate.
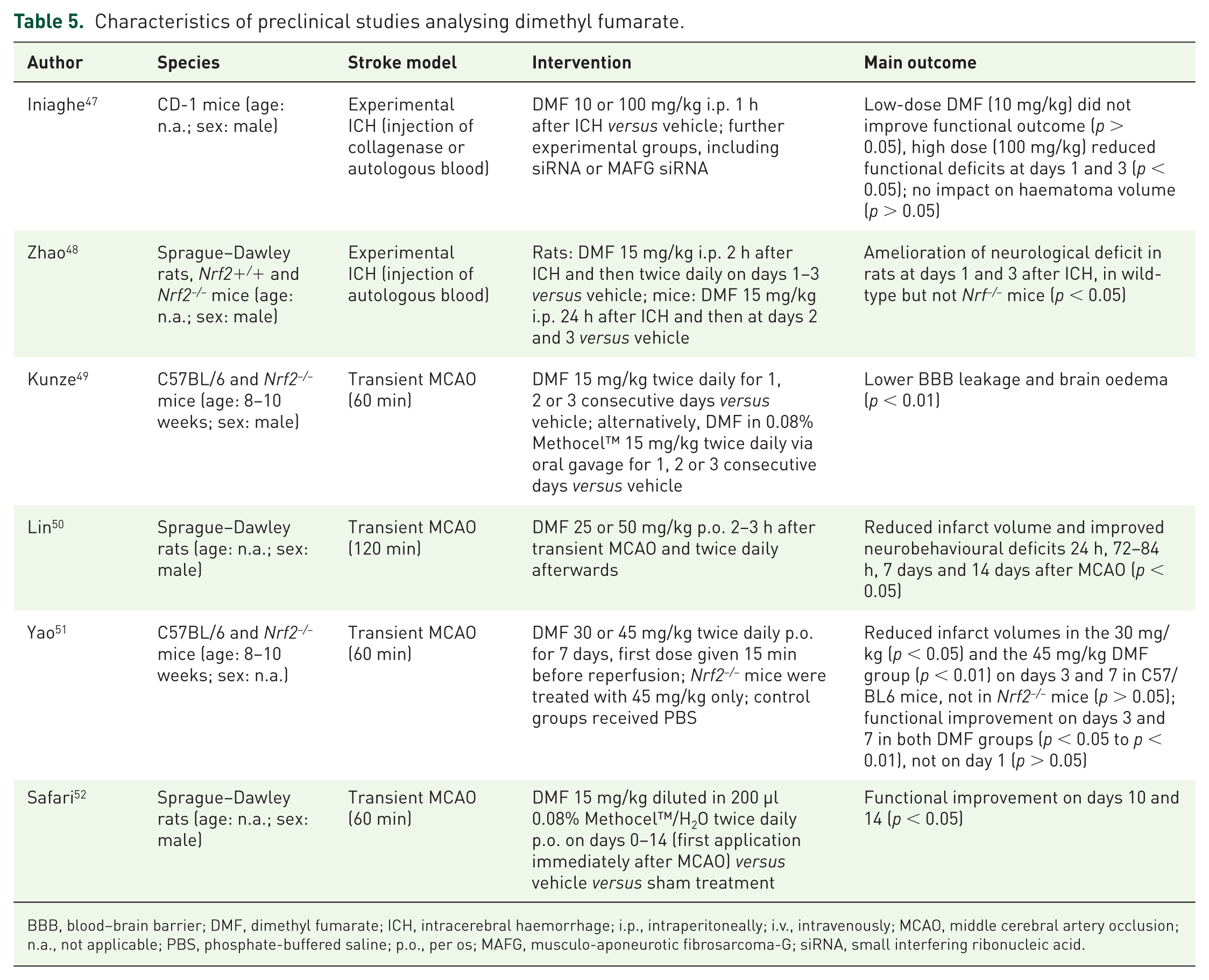
BBB, blood–brain barrier; DMF, dimethyl fumarate; ICH, intracerebral haemorrhage; i.p., intraperitoneally; i.v., intravenously; MCAO, middle cerebral artery occlusion; n.a., not applicable; PBS, phosphate-buffered saline; p.o., per os; MAFG, musculo-aponeurotic fibrosarcoma-G; siRNA, small interfering ribonucleic acid.
Characteristics of clinical studies.

AHA, American Heart Association; CT, computed tomography; DWI, diffusion-weighted imaging; FLAIR, fluid-attenuated inversion recovery; GCS, Glasgow Coma Scale; GRE, gradient echo sequences; ICH, intracerebral haemorrhage; i.v., intravenously; max., maximum; mBI, modified Barthel Index; MRI, magnetic resonance imaging; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; p.o., per os; RCT, randomized controlled trial.
Literature search and data extraction
A literature search was conducted on 16 October 2017 including MEDLINE (via PubMed) and the Cochrane Central Register of Controlled Trials. In addition, the reference lists of the included studies were reviewed to identify further studies. We continued the literature search until no further publications were identified. Four reviewers (ZM, MD, VP and PK) independently screened each title and abstract. Studies published until 16 October 12017 were considered. In the case of disagreement regarding study eligibility, a consensus meeting was arranged.
The databases were searched combining extensive search strings with the following Boolean operators: (mitoxantrone OR azathioprine OR ‘glatiramer acetate’ OR glatiramer OR ‘interferon beta’ OR ‘Peginterferon beta-1a’ OR ‘pegylated interferon’ OR FTY720 OR fingolimod OR natalizumab OR ‘α4 integrin’ OR daclizumab OR ocrelizumab OR cladribine OR teriflunomide OR ‘dimethyl fumarate’ OR fumarate OR alemtuzumab) AND (stroke OR ‘ischemic stroke’ OR ‘hemorrhagic stroke’ OR ‘experimental stroke’ OR ‘cerebral ischemia’ OR ICH OR ‘brain hemorrhage’ OR ‘cerebral hemorrhage’ OR ‘cerebral infarction’ OR ‘ischemia-reperfusion’). The compounds [mitoxantrone, azathioprine, glatiramer acetate, interferon β (IFN-β), fingolimod, natalizumab, daclizumab, ocrelizumab, alemtuzumab, cladribine, teriflunomide, dimethyl fumarate (DMF)] were chosen based on their approval for treatment of patients with multiple sclerosis in the European Union. FTY720 is used as a synonym for fingolimod. Mouse CD49d-specific antibodies and selective anti-α4-antibodies equate to natalizumab in humans. Monomethyl fumarate, as the main metabolite of DMF, has been evaluated in preclinical stroke studies, 5 but is not approved for multiple sclerosis and, therefore, not part of this review. At the time of the literature search, ocrelizumab has not been approved in the European Union (EU). As approval was expected in the EU soon, we decided to include ocrelizumab in the literature search.
Extracted data included species, stroke model, intervention and major outcome in the rodent studies (Tables 1–5), as well as study design, population, stroke type, intervention, major end points and major results in the clinical trials (Table 6).6–57
Results
The database literature search identified 624 papers. Five additional publications were found after screening of the reference lists. Of these 629 publications, 552 papers were excluded after abstract review with regard to inappropriate content. The 77 remaining articles were reviewed on a full-text basis. Further, 25 of them were excluded due to the study design or other violation of inclusion criteria. Finally, 52 studies met our eligibility criteria and were included in the review (Figure 1, Tables 1–6).

Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram.
Description of included studies
Of the 52 included studies, 47 were animal studies (Tables 1–5)6–52 and 5 were clinical trials (Table 6).53–57 Study characteristics and interventions are summarized in Tables 1–6.
Description of preclinical studies analysing glatiramer acetate
We identified four studies that met our inclusion criteria.6–9 In all of them, a transient middle cerebral artery occlusion (MCAO) was performed and in one, an additional permanent MCAO 7 was performed. Two studies used mice,7,8 the other, two rats.6,9 Glatiramer acetate application (dose, route, time point), read-out times, as well as outcomes differed between the studies. Two of the studies showed stroke volume reduction;6,9 the other two did not.7,8 A more detailed synopsis can be found in Table 1.
Description of preclinical studies analysing interferon β
Six studies met our inclusion criteria.10–15 Different stroke models have been used including transient MCAO,11–14 permanent MCAO, 13 photothrombotic stroke 15 and a clot embolus model. 10 Two studies used mice,14,15 three used rats,11–13 and one used rabbits. 10 IFN-β (dose, route, time point), read-out times, as well as outcomes differed between the studies, with four studies showing a reduction in stroke volume10–12,14 and one not. 13 Cruz and colleagues provide evidence that the anti-inflammatory and stroke-protective effect of IFN-β is lost in mice lacking interferon regulatory factor 2 binding protein 2 (IRF2BP2). 15 A more detailed synopsis can be found in Table 2.
Description of preclinical studies analysing fingolimod
We identified 23 studies that met our inclusion criteria.16–38 Sixteen studies analysed ischaemic stroke using transient16–23,26,28,30,32–34 or permanent MCAO,22,23 a thromboembolic stroke model 27 or photothrombotic stroke. 29 Seven studies investigated ICH.24,25,31,35–38 A broad spectrum of mice, as well as Sprague–Dawley rats have been used throughout the studies. Fingolimod (FTY720) treatment varied between the studies regarding dose (0.24–3 mg/kg),17,23,32 application route and time. The majority of studies evaluating IS described FTY720-related reduction in stroke volumes.16–21,23,26,27,30,32,33 A more detailed synopsis can be found in Table 3.
Description of preclinical studies analysing natalizumab
We identified eight studies that used different MCAO models39–43,45,46 or an ICH model 44 and analysed different rat strains39–41 or mice.42–46 Five of the IS studies described a reduction in stroke volume associated with antibody-mediated α4 integrin blockade,39–41,42,46 Langhauser and colleagues did not. 43 Llovera and colleagues found the type of MCAO model used (transient versus permanent) to be crucial for stroke volume reduction. 45 Hammond and coworkers evaluated α4 integrin blockade in an ICH model and presented evidence of improvement in functional outcome. 44 A more detailed synopsis can be found in Table 4.
Description of preclinical studies analysing dimethyl fumarate
We detected six studies that performed an experimental ICH by injection of collagenase 47 or autologous blood,47,48 or used transient MCAO as a model of IS.49–52 The intervention (dose, timing and route of administration of DMF) differed between the studies. All studies were positive in at least one outcome variable, including function,47,48,50–52 stroke volume50,51 and brain oedema. 49 A more detailed synopsis can be found in Table 5.
Description of clinical studies
In total, five clinical trials have been identified that met our inclusion criteria.53–57 Of these, only the study of Elkins and colleagues is a double-blinded RCT; 53 the others are single-blinded studies.54–57 Elkins and coworkers evaluated natalizumab 300 mg intravenously in patients with acute and first IS (n = 161). Despite promising data in most of the preclinical studies (see above), the primary end point remained negative. 53 In contrast, all of the studies that analysed fingolimod in IS55,57 or ICH54,56 (n = 23–47) reached their end points, including functional outcome54,55,57 and reduced infarct volume increase.55,57 A more detailed synopsis can be found in Table 6.
Discussion
In this systematic review, we found that immunotherapy in preclinical IS and ICH improved clinical and paraclinical outcome variables in most of the studies. As a limitation, the preclinical trials are very heterogeneous in design and used different stroke models, different occlusion times of the MCAO model, different doses of the immunotherapeutic drug, distinct time points of treatment and different application routes. Therefore, the comparability of the studies is very low and calculation of a meta-analysis regarding major outcome variables is not possible. The heterogeneity of the studies can also contribute to discrepant results in preclinical trials, which can be paradigmatically seen in studies regarding the role of regulatory T cells in IS. 58 Very often, the methodological quality of preclinical studies is low compared with clinical trials, and blinding and randomization procedures are not common in every laboratory, potentially leading to biased results. Moreover, only one preclinical study identified in our review analysed female animals that definitely does not represent the typical stroke population. 37 Methodological limitations might be one of the reasons for translational roadblocks, that is, difficulties in confirming positive preclinical results in clinical trials. Standardization of animal studies, 59 adherence to the Animal Research: Reporting of In Vivo Experiments guidelines (available at: https://www.nc3rs.org.uk/arrive-guidelines) and multicentre animal RCTs can improve data quality. 45
Encouraged by positive preclinical trials, the first clinical trials evaluating natalizumab and fingolimod in stroke patients have been conducted. From a methodological perspective, the RCT by Elkins and coworkers is the best of these studies, but remained negative regarding the primary end point, with slight treatment-associated benefits on functional outcomes (ACTION trial). 53 In contrast, the trials analysing fingolimod were not double blinded and much smaller, but positive regarding major outcome variables.54–57 The latter trials included mainly Asian patients; therefore, generalizability of data might be limited. In summary, the main limitation of the clinical trials is the heterogeneity of the included studies, the restricted data quality and generalizability, as well as the, in part, very low numbers of patients per study. Study heterogeneity comprises mainly population (IS versus ICH) and outcome variables.
The identified studies analysed immunomodulatory treatment with INF-β, glatiramer acetate, fingolimod, natalizumab and DMF. Until now, it is only incompletely understood what the stroke-specific mechanisms of these agents are. Therefore, the following aspects known from multiple sclerosis treatment might be the most relevant effects, but also other mechanisms might play an important role. INF-β inhibits IFN-γ, induces interleukin 10 expression and reduces the transmigration of lymphocytes and monocytes into the central nervous system (CNS). Glatiramer acetate (among other mechanisms) induces protective TH2 cells that secrete immunomodulating cytokines like interleukin-4, -6 and -10. Fingolimod is a sphingosine-1-phosphate-analogon that inhibits the efflux of lymphocytes out of lymph nodes leading to a profound lymphopenia and thus reduced CNS infiltration. Moreover, fingolimod seems to reduce thromboinflammation and improves cerebral blood flow. 26 The monoclonal antibody natalizumab blocks the adhesion molecule α4-integrin that is relevant for the infiltration of immune cells over the blood–brain barrier into the CNS. Finally, DMF has an antioxidant effect and activates the nuclear factor (erythroid-derived 2)-related factor 2 (Nrf2) pathway.
In conclusion, immunotherapy in stroke instrumentalizes the concept of thromboinflammation and could become a novel treatment option in the future. Despite translational limitations, the available clinical data are promising. Nevertheless, given the heterogeneity and low number of clinical studies, it is too early to reliably judge the novel strategy of immunotherapy in general. Therefore, further well-designed trials are urgently needed and are on the way (e.g. ACTION 2 and FAMTAIS 60 ) [ClinicalTrials.gov identifiers: NCT02730455 and NCT02956200].
Footnotes
Acknowledgements
Mirjam Dreikorn, Zeljko Milacic and Vladimir Pavlovic contributed equally to this work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
PK has received travel support and honoraria for medical advisory boards from Bayer, Boehringer Ingelheim, Daiichi Sankyo and Bristol-Myers Squibb, outside the submitted work. The other authors declare that there are no conflicts of interest.