
Abstract
Background:
With recent developments in drug therapy for multiple sclerosis (MS), new treatment options have become available presenting patients with complex treatment decisions.
Objectives:
The objective of this study was to elicit patients’ preferences for different attributes of MS drug therapy.
Methods:
A representative sample of patients with MS across Canada (n=189) participated in a best–worst scaling study to quantify preferences for different attributes of MS drug therapy, including delaying progression, improving symptoms, preventing relapse, minor side effects, rare but serious adverse events (SAEs), and route of administration. Conditional logit models were fitted to estimate the relative importance of each attribute in influencing patients’ preferences.
Results:
A latent-class analysis revealed heterogeneity of preferences across respondents, with preferences differing across five classes. The most important attributes of drug therapy were the avoidance of SAEs for three classes and the improvement of symptoms for two other classes. Only a smaller group of patients demonstrated a specific preference for avoiding SAEs, and route of administration.
Conclusion:
This study shows that preferences for drug therapy among patients with MS are different, some of which can be explained by experiences with their disease and treatment. These findings can help to inform the focus of interactions that healthcare practitioners have with patients with MS, as well as further drug development.
Introduction
More than 2.3 million people globally and 93,535 in Canada have been diagnosed with multiple sclerosis (MS) [Canada, 2011; Multiple Sclerosis International Federation, 2013]. While there is no cure, currently available treatments help to manage flareups, reduce the frequency of relapses, control the symptoms, and potentially slow the progression of the disease [Minagar, 2013; Wingerchuk and Carter, 2014]. Until recently, most available MS treatments were injectable medications requiring frequent administration; however, recent developments in drug therapy for MS have produced new treatment options (e.g. oral, annual or semi-annual injections), presenting patients with complex treatment decisions [Thomas and Wakefield, 2015]. Given the differences in treatments with regard to route of administration, potential effectiveness, rates of adverse events, and frequency of administration, patient preferences for each of these therapy attributes may play a role in therapeutic selection. While it has been postulated that patients would prefer oral versus injectable therapies, there is a paucity of studies that have been undertaken to ascertain the relative importance of different routes of administration and other treatment attributes, and how different treatment characteristics might impact treatment choice.
The risk–benefit tradeoff is relevant for patients with MS. Medications for MS demonstrate significant levels of efficacy in terms of reducing relapse rates, disability progression, and brain lesions [Killestein et al. 2011]; however, some treatment alternatives also carry a risk of serious adverse events (SAEs), some of which can be fatal such as progressive multifocal leukoencephalopathy [Toussirot and Bereau, 2014]. Prior research suggests that both efficacy and side effects influence why patients choose to switch treatments (81% and 65%, respectively) [Calfee, 2006]. Specifically in MS, attributes such as reducing the frequency of relapse, slowing disease progression, reducing brain lesions, improving cognitive abilities, and reducing development of disabilities are all rated as important by roughly 90% or more of patients [Calfee, 2006]. In regards to side effects, many patients appear to be willing to tolerate the chance of severe (even deadly) side effects for the probability of greater efficacy [Calfee, 2006; Wilson et al. 2015]. Moreover, recent studies by Wilson and colleagues and Utz and colleagues suggest that route and frequency of administration (oral versus injectable) to be important attributes, with patients preferring oral to injectable treatments when side effects and efficacy are held constant [Utz et al. 2014; Wilson et al. 2015]. However, these studies have several limitations, including recruiting only patients with relapsing–remitting MS, and small, nonrepresentative samples.
Given the methodological limitations of previous studies, the objective of this study was to elicit patients’ preferences for different attributes of MS drug therapies in a representative sample of patients consisting of both progressive MS and RRMS, and with different treatment experiences. Given the heterogeneity of the sample, our secondary objective was to identify differences in preferences between different types of patients using latent-class modeling.
Methods
Recruitment and study sample
Study participants were recruited using CRC Research Inc. (Vancouver, Canada) in order to recruit a sample of patients with MS from across Canada. Potential participants were derived from CRC’s Canada-wide MS panel that consists of consenting patients with MS who were initially referred by MS associations, nurses, physicians, and caregivers. They were invited to participate in a best–worst scaling (BWS) survey if they were aged at least 19 years, were diagnosed with MS, were currently residing in Canada, and were fluent in speaking and writing in English. Recruitment was stratified by MS type to ensure a sufficient sample of progressive MS and RRMS, and treatment naïve and treatment experienced. The University of British Columbia Behavioural Ethics Board approved the study.
Study design
Initially, qualitative methods were used which included three focus groups and individual interviews with 23 patients (10 RRMS treatment naïve, eight RRMS treatment experienced, five progressive MS) to identify the attributes of MS treatment deemed most important to patients. A moderator briefly gave baseline information regarding MS treatment options and alternatives and their potential differences in effectiveness and side effects to ensure that all patients would have a similar baseline knowledge regarding the issues to be discussed. Given that treatment options are associated with both potential risks and benefits, issues for discussion raised by the moderator included the potential benefits and risks of MS treatment options, and potential alternative drug administration routes. The specific attributes that were identified in these interviews and discussions contributed to the design of the quantitative portion of the study. Six different attributes were deemed important from the focus groups and interviews, and each attribute was divided into appropriate levels (Table 1).
Attributes and levels included in the best-worst questionnaire.

MRI, magnetic resonance imaging; MS, multiple sclerosis.
Sawtooth Software Inc. (SSI, MaxDiff/Webv6.0) was used for survey design. SSI constructs near optimal plans [technical paper, 2005] using a system where the user inputs the total number of attribute levels, the number of attributes to show in each choice set, and the number of choice sets the respondent is to see in the questionnaire. SSI then generates a design based on four items, frequency balance, orthogonality, connectivity, and position balance, in that order.
Design by SSI is near optimal. It does not ensure that all levels are presented with exact equal frequency, nor does it ensure that all pairs are presented at the same frequency. However, across multiple versions, balance is obtained. Using 18 BWS questions per respondent across eight versions, one-way and two-way frequencies were balanced. Background information regarding the attributes of MS treatment options were provided to all participants completing the BWS questionnaire. The background information was developed to represent what a patient might receive if faced with making a treatment decision. Additional demographic and personal information regarding previous and current MS treatment characteristics of participants was also collected.
Sample size
The complexity of the analysis of a stated-choice experiment prohibits the use of generally applied sample size calculations based on hypothesis testing [De Bekker-Grob et al. 2015]. Therefore, the necessary sample size is based on the number of attributes included in the study and the fact that a random effects logit model will be used. This analytic approach requires that the minimum sample size should be more than the number of independent variables to retain sufficient degrees of freedom. The final regression model included the six treatment attributes plus six additional stratification variables. Therefore, given the general rule of a minimum of 10 observations for each independent variable in the model, a minimum of 120 participants was required for the study.
Statistical analysis
The study sample is described using descriptive statistics, with means and standard deviations (SDs) used for continuous data, and proportions for categorical data. BWS data were coded for analysis in Latent Gold Choice version 4.5.0 (Statistical Innovations, Belmont, MA) to facilitate a latent-class analysis (LCA) that distinguishes groups of individuals with similar preferences and effectively reveals heterogeneity of responders. To assess overall preferences of MS for different attributes of MS therapy, a one-class, random effects, conditional logit model was used. The reference level was chosen after running the model multiple times, and choosing the attribute level with the strongest negative preference (least preferred) as the reference level; the preferences for all other levels of all attributes are therefore compared with this level, and are therefore positive. The parameter estimate for each attribute level is interpreted as a relative utility (relative to the reference level), and p values indicate the significance of the estimates at the 0.05 level for their difference from the reference level.
In order to evaluate preference heterogeneity, a latent-class analysis was performed. To determine the preference estimates for different groups or classes of patients with MS, we fit LCA models with up to six latent classes. Model fit parameters including the log-likelihood function (LL), the Bayesian Information Criteria (BIC), and the Akaike Information Criteria (AIC) were used to assess the optimal model fit. Using both univariate analyses and backwards selection methods, demographic covariates were included in the models that were considered to be potentially explanatory variables across the different latent classes. Similar to the conditional logit model, the most preferred attribute level was chosen as the reference level such that all parameter coefficient estimates could be interpreted relative to the reference.
Given that the raw data provide the specific relative preference of each level of each attribute, the relative importance of each treatment attribute was also calculated. Relative importance was defined as the maximum effect an attribute makes on the utility of a given choice, considering all attributes. The relative importance ranges from 0 to 1, and is calculated based on the proportion of the difference between the maximum and minimum preference weights for each attribute relative to the sum of the total differences across all attributes [Vermunt and Magidson, 2005; Orme, 2010].
Results
Study sample characteristics
One hundred and ninety-three of the 875 eligible participants who were emailed an invitation completed the survey (response rate 22.1%). Of 193, four individuals had incomplete demographic data and were therefore excluded, leaving 189 respondents included in the final analysis (Table 2). The majority of respondents were women, reported having RRMS, had previously received an MS treatment which was subsequently stopped for a variety of reasons (Table 3), or had been diagnosed with MS over 10 years before the survey [mean 13.2 years (SD 3.6)]. Forty-five percent of individuals were currently on therapy for MS, while 40.7% and 46% reported that their MS had worsened or flared in the past 12 months, respectively.
Respondent characteristics.

MS, multiple sclerosis; SD, standard deviation.
Reason for discontinuation of previous treatment.
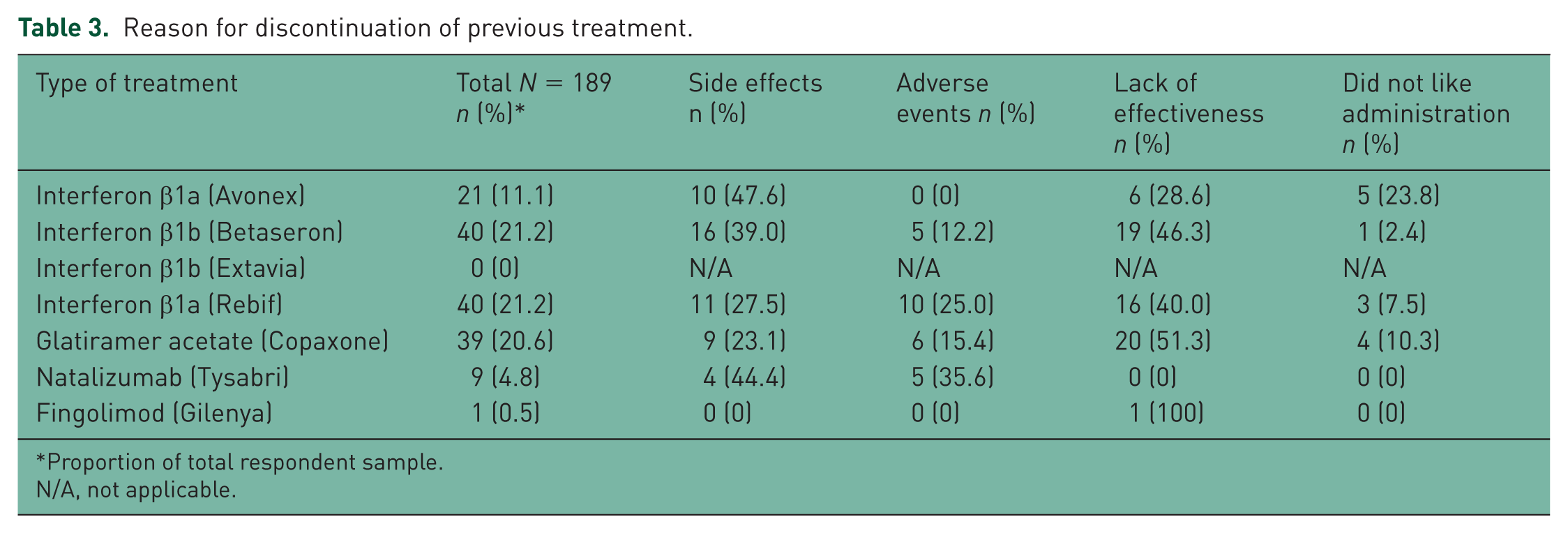
Proportion of total respondent sample.
N/A, not applicable.
Preferences for MS drug therapy
One-class model
A one-class model including all respondents revealed good face validity with an appropriate preference gradient across attribute levels as hypothesized a priori (Table 4). A SAE rate of 3% was the least desired attribute level and was therefore used as the reference level (i.e. relative preference = 0). Based on the one-class model, delaying progression by 8 years was the most desired characteristic (relative preference 5.61) and preventing relapse by 8 years was the second most preferred attribute (relative preference 5.06).
One-class model: preference weights.

MRI, magnetic resonance imaging; MS, multiple sclerosis.
Regarding route of administration, daily injections were the least desirable route (relative preference 1.06). While daily oral and yearly or biannual infusions were the most preferable administration strategies (3.49 and 2.41, respectively), respondents exhibited a stronger preference for any delayed progression (relative preferences ⩾ 3.73), any improvement in symptoms, and no risk of SAEs (3.68) than even daily oral administration. Looking at the relative importance of the overall attributes, in a one-class model (assuming preference homogeneity), the chance of experiencing a SAE and the effectiveness of improving symptoms were deemed the most important (relative importance 0.25 and 0.22, respectively).
Latent-class model: exploring preference heterogeneity
A latent-class model (Table 5) including demographic variables (Table 6) improved the model fit, suggesting preference heterogeneity across respondents. Specifically, the AIC, BIC, and LL all plateaued with the inclusion of five latent classes; therefore, a five-class model was deemed to best represent the preferences of this sample. A large proportion (40.4%) of participants fit in class 1, with 22.2% and 20.1% assigned to classes 2 and 3, respectively.
Preference weights across five latent classes.

Pref Wt, preference weight; SE, standard error.
Probability of having a specific characteristic within each latent class.

MS, multiple sclerosis.
Difference in preferences by latent class are illustrated in Figure 1. For respondents in class 1, the most important attribute was the avoidance of SAEs. Although the relative importance of the route and frequency of administration was similar to the other attributes for respondents in class 1, it was less important to those in class 1 relative to the other four classes. This might be explained by their experience with treatment and disease as class 1 members were predominantly treatment-experienced respondents (84.3%) with a relatively stable MS (66.8%). For respondents in class 2 who were most likely to be treatment naïve (54.8%) and to have had their symptoms worsen in the last year (58.3%), symptom control was the most important attribute, followed by avoiding SAEs. Of all classes, respondents in class 2 also had the strongest preference for daily oral administration.
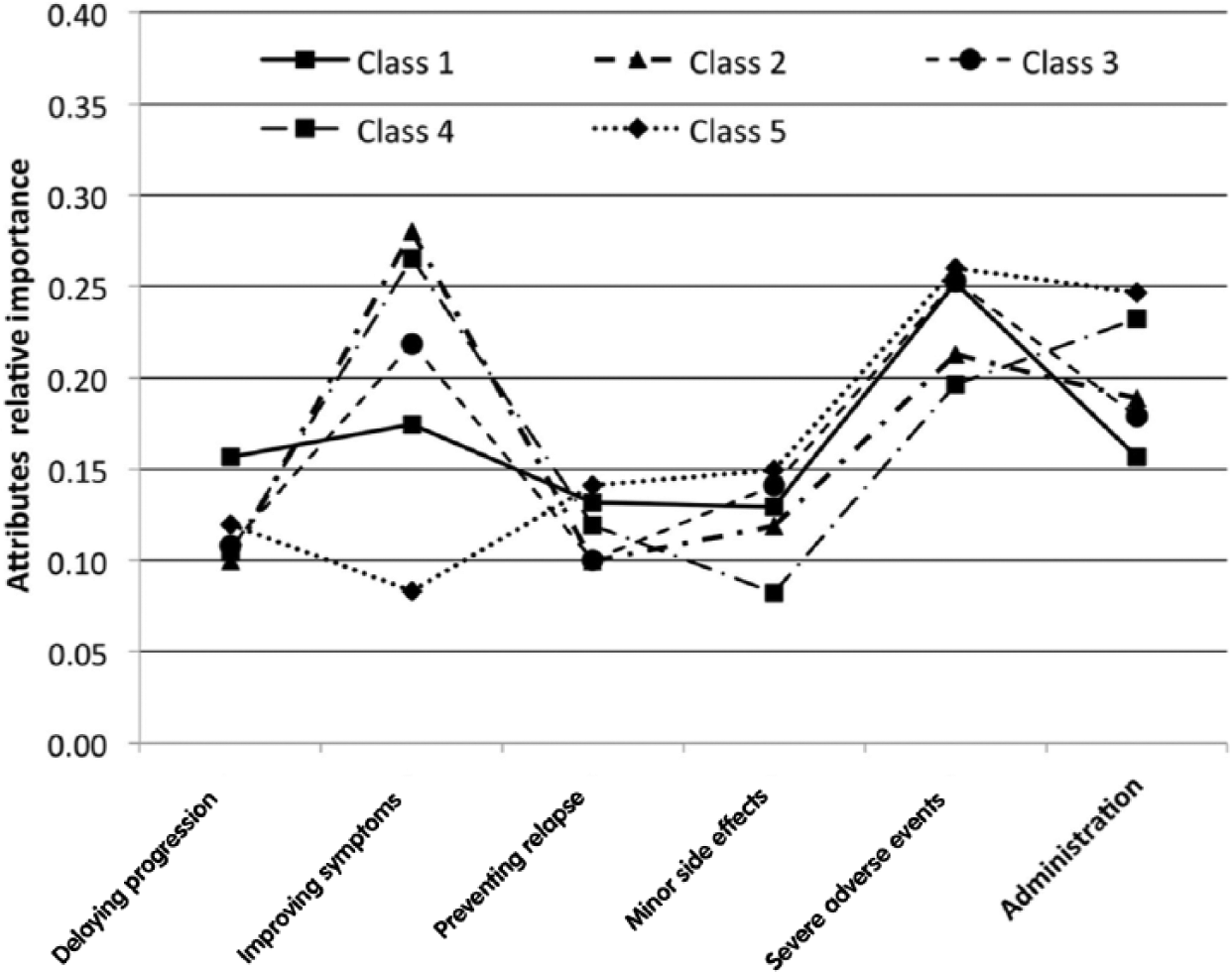
Relative importance of each attribute, but latent class.
Participants in class 3 were mostly concerned about avoiding SAEs followed closely by symptom improvement. This could be explained by their experience with treatment and disease given class 3 was composed of the highest proportion of treatment-experienced respondents (92%), and about half of them had stable MS with respect to progress or flare in the past 12 months. Symptom improvement was also the most important attribute for those in class 4, which was followed by route and frequency of administration. Interestingly, however, class 4 was dominated by individuals whose MS was relatively stable (with regards to progression or flare in the past 12 months). Of all groups, this group had the strongest positive preference for once yearly intravenous administration (5.44) and monthly intravenous infusions (4.78), which might be explained by the highest proportion of respondents with MS for greater than 15 years, and 84.5% were treatment experienced. Finally, while class 5 was only composed of approximately 7% of the sample, the mode of administration was the most important to this group, preferring the yearly intravenous (4.37) and daily oral administration (4.16), while being the least concerned about the improvement in their symptoms. This might be explained by the fact that over 90% of respondents in class 5 had MS that had not worsened in the 12 months preceding the study.
Discussion
This study shows that, overall, the most important treatment attributes of MS treatments for patients are the avoidance of SAEs and the improvement of symptoms. However, while previous studies have assumed preference homogeneity, our latent class analysis identified five distinct groups of patients with different preferences, and some specific factors that could explain this preference heterogeneity. It appears that of five potential groups of patients with different preferences, two (class 2 and 4) were most concerned about experiencing improvements in symptoms while those in the other three classes (class 1, 3, and 5) were most concerned about avoiding SAEs. While we had postulated that avoiding frequent injections would be an important factor for all patients, for only two classes of respondents was the route and frequency of administration the second most important attribute. Broadly, patients with MS who were treatment experienced had the strongest preference for ‘avoidance of SAEs’, and this might be explained by their treatment experience. While, for other patients, their experience with diseases might explain their preferences; for example, respondents whose MS worsened or progressed within the 12 months of the study had the strongest preference for ‘rare but substantial improvement of symptoms’.
These results are similar to prior studies of patient preferences for treatment of rheumatoid arthritis and diabetes whereby the majority of patients who were treatment experienced preferred their current route of administration [Guimaraes et al. 2011; Huynh et al. 2014; Harrison et al. 2015]. Like patients with MS in our study, drug safety, or SAEs, were of prime importance in choosing a specific drug. Likewise, recent studies of preferences of patients with MS suggest that route and frequency of administration were important treatment attributes, with oral treatments being preferred to injections when treatment frequency and frequency of side effects were held constant [Utz et al. 2014; Wilson et al. 2015]. Our findings concur with those of Wilson and colleagues, suggesting that prevention of relapse was not as important as improving symptoms and preventing SAEs [Wilson et al. 2015].
In contrast to our study, however, Wilson and colleagues found delaying disease progression to be the most important attribute. Another recent study by Johnson and colleagues used a choice-based conjoint analysis to evaluate the benefit–risk tradeoffs of treatment attributes associated with Tysabri (Biogen Idec, Inc. and Cambridge, MA) [Johnson et al. 2009]. In this study, delaying the time to disability was the most important factor for patients in choosing a hypothetical treatment, and they were willing to tolerate a nontrivial risk of death for a delay in disease progression. It is reasonable to believe that some patients might rather be dead than have their disease progress to the point of total dependence and the potential loss of dignity [Griebsch et al. 2005]. Nevertheless Wilson and colleagues and Utz and colleagues used small and nonrepresentative samples, only included patients with RRMS, only reported average preferences for the sample thus assuming preference homogeneity, and applied a DCE and choice-based conjoint analysis experiment, respectively [Utz et al. 2014; Wilson et al. 2015]. While a discrete choice experiment (DCE) approach could be used in our study to elicit preferences, it has been suggested that a better methodological approach to eliciting ‘relative’ preferences both between levels of a given attribute and across attributes is by using a BWS methodology [Marley and Louviere, 2005; Flynn et al. 2007, 2008; Marley et al. 2008; Potoglou et al. 2011]. This BWS methodology has facilitated the determination of the relative importance of each of the treatment attributes deemed to be most relevant to patients in making treatment decisions. The state of the art latent-class analysis also allowed for the evaluation of different preferences across patient groups, and for the exploration of the differences between groups.
Stated preference studies have inherent limitations. First and foremost, they are limited in that the preference weights elicited are specific to the attributes and levels that are presented. While it is not methodologically possible to include an exhaustive list of treatment characteristics for respondents to consider, it is important that those that are deemed to be most important to respondents be included. We went to great lengths to attempt to identify and include the treatment attributes most germane to patients’ treatment decisions, at least on average among patient with MS. It is possible that some attributes that are important to some patients were not included. For instance, the length of time a drug has been available (i.e. the uncertainty associated with potential benefit and potential harm), or whether or not a drug is recommended by their physician may be most important to some patients. However, through our focus groups, literature search, and consultation with experts, these were not included as it was felt that these attributes were less important than those included, on average, across all patients. Stated preference methods are also limited in that they are ‘stated’ preferences (respondents only tell you what they think) as opposed to ‘revealed’ preferences, which represent exactly how patients make choices. However, these techniques are being used increasingly more frequently to provide empiric quantitative evidence of what people’s choices ‘might’ be. Further, the response rate (~22%) was not surprising given the web survey method was used to recruit participants which generally yields a response rate lower than a mail- or paper-based approach [Shih and Fan, 2008]. Nevertheless, the low response rate might have introduced a nonresponse bias (selection bias) that could limit the generalizability of our findings.
The potential advantages of these stated choice techniques in this regard are that hypothetical treatment options can be offered and respondents’ preferences for treatments that may become available can be estimated. There are often arguments against these methods which suggest that respondents do not understand the problem, or the technique. However, the MS population tends to be a very well informed group of patients relative to other populations, so we are confident that most respondents were familiar with issues being presented. Additionally, a significant amount of background information was provided to respondents to help inform their preferences prior to them starting the choice task. Further to this, from the results, we can see that all preferences for all attributes where one can hypothesize what should be more and less preferred go in the a priori hypothesized direction, lending face validity to the results. Therefore, we feel it is likely that these results accurately represent the relative preferences of the respondents.
In conclusion, our findings from a sample of patients with all types of MS from across Canada show that these patients have very different treatment preferences, some of which can be explained by their experiences with their diseases, the type of MS they have, or their treatment experiences. These findings can help to inform the focus of interactions that healthcare providers have with patients with MS, as well as further drug development.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from Genzyme Canada.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Larry D Lynd: Consultancies = AstraZeneca, Sanofi Aventis, Boerrhinger Ingelheim, Pfizer Canada, BC Ministry of Health, BC Pharmacy Anthony Traboulsee received speaker fees and/or advisory board fees from Biogen, F. Hoffman-La Roche Genzyme, Serono and Carlo A Marra: Advisory Board fees: Boerrhinger Ingelheim, Glaxo, Pfizer Canada,; Working group: Canadian Agency for Drugs and Nicole Mittmann, Charity Evans, Kathy H. Li, Melanie Carter, and Celestin Hategekimana declare no conflict of interest.