
Abstract
Duchenne muscular dystrophy is a genetically determined X-linked disease and the most common, progressive pediatric muscle disorder. For decades, research has been conducted to find an effective therapy. This review presents current therapeutic methods for Duchenne muscular dystrophy, based on scientific articles in English published mainly in the period 2000 to 2014. We used the PubMed database to identify and review the most important studies. An analysis of contemporary studies of stem cell therapy and the use of granulocyte colony-stimulating factor (G-CSF) in muscular dystrophy was performed.
Introduction
Duchenne muscular dystrophy (DMD) is the most commonly inherited pediatric muscle disorder. It is an X-linked genetic progressive and degenerative myopathy characterized by muscle wasting and weakness, which can lead to loss of motor functions in puberty, cardiac and respiratory involvement, and premature death [Mercuri and Muntoni, 2013]. The disease is one of a number of types of myopathies that differ depending on the degree of severity and the affected muscle types [Emery, 2002]. DMD occurs at a rate of approximately 1:3500 male births and arises due to spontaneous mutations in the dystrophin gene (locus Xp21.2); 65% of causative mutations are intragenic deletions, 6–10% are intragenic duplications and 30–35% are point mutations (along with other sequence variations) [Nallamilli et al. 2014]. The disease is caused by a deficiency of dystrophin or the synthesis of functionally impotent dystrophin, a critical protein component of the dystrophin glycoprotein complex (DGC) acting as a link between the cytoskeleton and the extracellular matrix in skeletal and cardiac muscles [Braun et al. 2014].
A consequence of DGC inefficiency is muscle fragility, contraction-induced damage, necrosis and inflammation [Lapidos et al. 2004]. As a result, fibrous and fatty connective tissue overtakes the functional myofibers. A majority of patients are restricted to a wheelchair in their early teens, succumbing to cardiac/respiratory failure in their twenties [Bach and Martinez, 2011].
Another problem seen in children with DMD is neurodevelopmental delay, which is observed from the first months or years of life. Cognitive and behavioral difficulties have been identified in approximately a third of DMD patients and are more frequent in patients with mutations after exon 44, affecting Dp140 (the short isoforms of distrophin expressed in the brain) and are compounded further in boys with mutations after exon 63 affecting the shortest Dp71 (the isoform of distrophin expressed at high levels in the brain) [Pune et al. 2012; Cyrulnik and Hinton, 2008; Hinton et al. 2007; Pane et al. 2013]. These isoforms are structural components of neurons, glial cells and Schwann cells.
Diagnosis and appropriate therapy consisting of pharmacotherapy, rehabilitation, and surgical management can preserve the child’s ambulation and prolong their functional independence, and should be started as early as possible, ideally before clinical signs, muscle pathology and motor delay have progressed more severely [Pane et al. 2013; Muntoni, 2010]. This management strategy aims at reducing the early inflammatory process and slowing muscle necrosis.
In searching for an effective therapy for DMD, only steroids have been shown to produce a slowing in the declining course of the disease [Ricotti et al. 2013].
Medical research has been searching for alternative therapeutic approaches for patients with muscular dystrophies. New advances in the management of DMD use exon skipping, gene therapy and cellular therapy to alter the disease process and slow its progression [Sharma et al. 2014]. Exon skipping refers to skipping the genetic abnormality that leads to an incomplete but potentially better functioning protein sequence [Arechavala-Gomeza et al. 2012]. Gene therapy aims at introducing the absent dystrophin gene using various vectors and adeno-associated virus vectors are used; they do not cause human disease and are able to persist for years [Braun et al. 2014]. However, several practical difficulties have so far prevented gene therapy from being a clinically feasible and viable option [Konieczny et al. 2013].
The aim of this review is to present current therapeutic methods used to treat DMD based on scientific articles published in English mainly in the period between 2000 and 2014. We focused on stem cell therapies, in particular, which have the potential to treat muscular dystrophies. We also used the PubMed database to review the most important clinical studies related to muscular dystrophies. The search period covered 1 January 2010 to 31 December 2014; all articles were published in English. We used the following Medical Subject Headings (MeSH): muscular dystrophy, children, stem cell, hematopoietic stem cells, satellite cells, embryonic stem cells, epidermal stem cells, autologous stem cells, pluripotent cells, and muscle stem cells.
Stem cell based therapies
Stem cell based therapy is considered to be one of the most promising methods for treating muscular dystrophies. Stem cells are defined by certain features and, foremost, an ability for long-term self-renewal and the capacity to differentiate into multiple cell lineages. ‘Self-renewal’ refers to the ability to undergo cycles of mitotic division while maintaining the same undifferentiated state as the parent cell [Huan-Tng et al. 2012]. Stem cells are responsible for the development and maintenance of tissues and organs [Price et al. 2007]. A stem cell may be: (i) pluripotent (totipotent), that is, able to give rise to endodermal, ectodermal, and mesodermal lineages of cells, e.g. embryonic stem cells (ESCs); (ii) multipotent, that is, able to give rise to all cells in a particular lineage, e.g. hematopoietic stem cells (HSCs), neural stem cells (NSCs) and epidermal stem cells (EpSCs); and (iii) unipotent and thus able to give rise to only one cell type, e.g. keratinocytes [Parkinson, 1992].
Isolation of stem cells can be from embryonic or adult tissues. In regard to anatomical location, small quantities of adult stem cells exist in most tissues throughout the body, where they remain quiescent for long periods prior to being activated in response to disease or tissue injury. They can be found in hematopoietic [Osawa et al. 1996], neural (dentate gyrus of the hippocampus and the lateral ventricle wall of the olfactory bulb [Goritz and Friesen, 2012; Galli, 2000], dermal [Toma et al. 2001], muscle [Qu-Petersen et al. 2002; Young, 2001] and hepatic [Shafritz et al. 2006] systems. These locations are often loosely referred to as ‘niches’ but, strictly speaking, the name has a much stronger emphasis on the surrounding micro-environment and its constituent supporting and regulatory cells, from which extrinsic signals are derived that can strongly influence the functions of the residing stem cells [Huan-Tng et al. 2012]. Adult stem cells give rise to cell types of the tissue from which they originated [Price, 2007], but according to scientific reports, they can differentiate into lineages other than their tissue of origin, e.g. transplanted bone marrow or enriched HSCs were reported to give rise to cells of the mesoderm [Orlic et al. 2001; Jackson et al. 2001], endoderm [Theise et al. 2000] and ectoderm [Mezey et al. 2000].
Based on these scientific discoveries, the terms ‘stem cell medicine’ and ‘regenerative medicine’ have been created. The use of stem cells has been reported in therapies related to Parkinson’s disease [Ourednik et al. 2002], spinal cord injury [Teng et al. 2002], multiple sclerosis [Pluchino et al. 2003], amyotrophic lateral sclerosis [Clement et al. 2003], stroke [Liu et al. 2009], retinal degeneration [Li et al. 2006], Alzheimer’s disease [Barnham et al. 2004] and myocardial infarction [Jackson et al. 2001] among others. The protective stem cell property is mediated mostly through the release of specific trophic factors that modulate the survival capabilities of the surrounding neurons [Carletti et al. 2011]. Nevertheless, the goal is to achieve the development of safe and effective stem cell therapies [Huan-Tng et al. 2012].
Muscle stem cells
The formation of skeletal muscle begins during the fourth week of embryonic development, as specialized mesodermal cells called myoblasts begin rapid mitotic division [McLean et al. 2012]. By month 5, the muscle fibers are accumulating protein filaments important in muscle contraction. As the growth of muscle fibers continues, aggregation into bundles occurs and, by birth, myoblast activity has ceased. Muscle contraction on a subcellular level is a complex process in the sarcomere involving an influx of calcium ions into the muscle fiber and an interaction between myosin, actin, and the proteins troponin and tropomyosin.
Stem cell based therapies for the treatment of DMD can proceed via two strategies. The first is autologous stem cell transfer involving cells from a patient with DMD that are genetically altered in vitro to restore dystrophin expression and are subsequently re-implanted [Mendell and Clarke, 2006]. The second is allogenic stem cell transfer, containing cells from an individual with functional dystrophin, which are transplanted into a dystrophic patient [Partridge, 2004].
Skeletal muscle damaged by injury or by degenerative disease, such as muscular dystrophy, is able to regenerate new muscle fibers. Regeneration depends mainly on satellite cells (SCs), myogenic progenitors localized between the basal lamina and the muscle fiber membrane, but other cell types outside the basal lamina, such as pericytes, also have myogenic potency [Tedesco et al. 2010]. Because of the proprieties of SCs, there have been several clinical trials since the early 1980s involving the transplant of SCs by intramuscular injections of these cells into several locations of a single muscle or at most a few muscles [Miller et al. 1997; Skuk et al. 2006]. Although results in treating DMD patients have been encouraging, this method has been limited by: (i) the necessity of a huge number of injections; (ii) immune responses toward injected SCs; and (iii) the rapid death of most of the SCs in the first 72 hours following injection [Fan et al. 1996; Guerette et al. 2007]. Other studies indicate that 90% of donor cells are cleared within the first hour following transplantation by cell-mediated immune response [Maffioletti et al. 2014; Sku and Tremblay, 2013], resulting in the impossibility of delivering myoblasts systematically via circulation.
Bone marrow cells
Two main types of stem cells usually derived from adult bone marrow are HSCs and mesenchymal stem cells (MSCs). They can sometimes be obtained from fat, skin, periosteum, synovial membrane and muscle as well. MSCs are multipotent and capable of differentiating into several connective tissue types including osteocytes, chondrocytes, adipocytes, tenocytes and myoblasts [Bongs and Lee, 2005]. They can also impose an additional anti-inflammatory and paracrine effect on differentiation and tissue regeneration via cytokine pathways, have anti-apoptotic features [Meirelles and Nardi, 2009; Keating, 2012; Uccelli et al. 2011] and can produce extracellular matrix molecules [Meng et al. 2010]. These genetically determined pluripotent cells may be easily isolated from bone marrow because they have membrane proteins (marker CD34+ and specific marker STRO-I). Compared with pluripotent ESCs or induced pluripotent stem cells (iPSCs), MSCs have a greater biosafety profile and lower risk of tumorigenicity, and perhaps that is why numerous MSC-based therapies have made it to the clinical trial stage [Huan-Tng et al. 2012; Ra et al. 2011].
Granulocyte colony-stimulating factor
Granulocyte colony-stimulating factor (G-CSF) – glycoprotein – was initially identified as a hematopoietic cytokine and has been used in research and clinical studies for the mobilization of HSCs from the bone marrow into the peripheral blood [Demetri and Griffin, 1999; Metcalf, 2008]. It is used to treat neutropenia after cytostatic therapy. Recent studies have suggested that G-CSF also plays a role in cell differentiation, proliferation and survival [Harada et al. 2005; Zaruba et al. 2009]. It has a wide variety of actions including reducing apoptosis, driving neurogenesis and angiogenesis, and attenuating inflammation [Schneider et al. 2005; Kawada et al. 2006] and acts positively on the process of peripheral nerve regeneration during the course of muscular dystrophy [Simões et al. 2014]. As recently demonstrated, alterations exist in the muscle interface with the nervous system, caused by the chronic muscular degeneration process that retrogradely affects the spinal cord micro-environment, specifically the alpha motor-neurons [Simões and Oliveira, 2010], and that also causes deficits in peripheral nerve regeneration in the course of DMD [Simões and Oliveira, 2012]. It was also demonstrated that G-CSF can potentially re-establish homeostasis in the spinal cord micro-environment of MDX mice (mouse strain for DMD research). It was observed that G-CSF, as well as stem cells, induces the production of growth factors such as insulin-like growth factor 1, hepatocyte growth factor, epidermal growth factor, transforming growth factors, platelet-derived growth factors, and cytokines. The effect of its activity is the proliferation of satellite cells, with subsequent transformation into myotubes and muscle fibers, regulation of myoblast proliferation and differentiation, and promotion of muscle regeneration and repair [Ruozi et al. 2012]. Positive effects of muscle regeneration were observed in several studies, including the above mentioned experiments on mice [Simões et al. 2014], following muscle injuries [Stratos et al. 2007; Hara et al. 2011] and after acute myocardial infarction [Harada et al. 2005; Okada et al. 2008].
A clinical trial was performed on a 15-year-old boy with facioscapulohumeral dystrophy (FSHD). G-CSF 5 μg/kg was given subcutaneously daily for 5 days in the same month, four times in one year. The patient reported increased muscle strength in the upper and lower limbs after 2 months of G-CSF treatment. We confirmed the increase in muscle force of the upper and lower extremities in an objective assessment using a dynamometer for upper limbs and in leg tensor apparatus for lower limbs. Before the study, the patient was able to walk 380 meters within 6 minutes, 420 meters after 3 months, 450 meters after 6 months, and 480 after 12 months. The patient did not report any side effects following G-CSF administration [Sienkiewicz et al. (In press)]. All clinical reports published to date agree on the long-term safety of G-CSF, in that an increased risk for any of the observed outcome parameters was never observed [Mueller et al. 2012].
Clinical and case reports
There have been different attempts to repair muscle damage in DMD and there are different ways to transplant bone marrow cells in a patient’s body. Previous trials have concentrated on the delivery of myogenic stem cells to the sites of muscle lesions via systemic circulation [Farini et al. 2009; Jin et al. 2005]. However, intravenously injected cells may become trapped in other organs (e.g. liver, spleen, lungs), resulting in only a small portion entering the muscle microvasculature and migrating into dystrophic muscles [Chen et al. 2001].
Another method was established to develop cellular therapy for muscle tissues. The authors used arterial route delivery and observed widespread distribution of donor stem cells throughout the muscle capillary network. The cells entered the circulatory system and migrated within dystrophic muscles after serial passages within the capillaries of the injected area. The environment of the dystrophic muscle made it possible to recruit the transplanted cells from the vessels following the secretion of specific cytokines and other inflammatory molecules [Farini et al. 2012].
To date, in the years from 2010 to 2014, no controlled or randomized clinical trial on cell therapy in patients with DMD has been published (Table 1). In an open study, Sharma and colleagues demonstrated the efficacy of autologous bone marrow mononuclear transplantation by intrathecally intramuscularly to patients with DMD, BMD and lower gird dystrophy [Sharma et al. 2013]. However, they did not provide the molecular diagnosis of these dystrophies. No significant adverse events were noted. An increase in trunk muscle strength was seen in 53% of the cases, 48% showed an increase in upper limb strength, 59% showed an increase in lower limb strength and approximately 10% showed improved gait. Of 150 patients, almost 87% had functional improvement upon physical examination and electromyogram (EMG) studies after 12 months.
Clinical trials of cell therapies in muscular dystrophies.
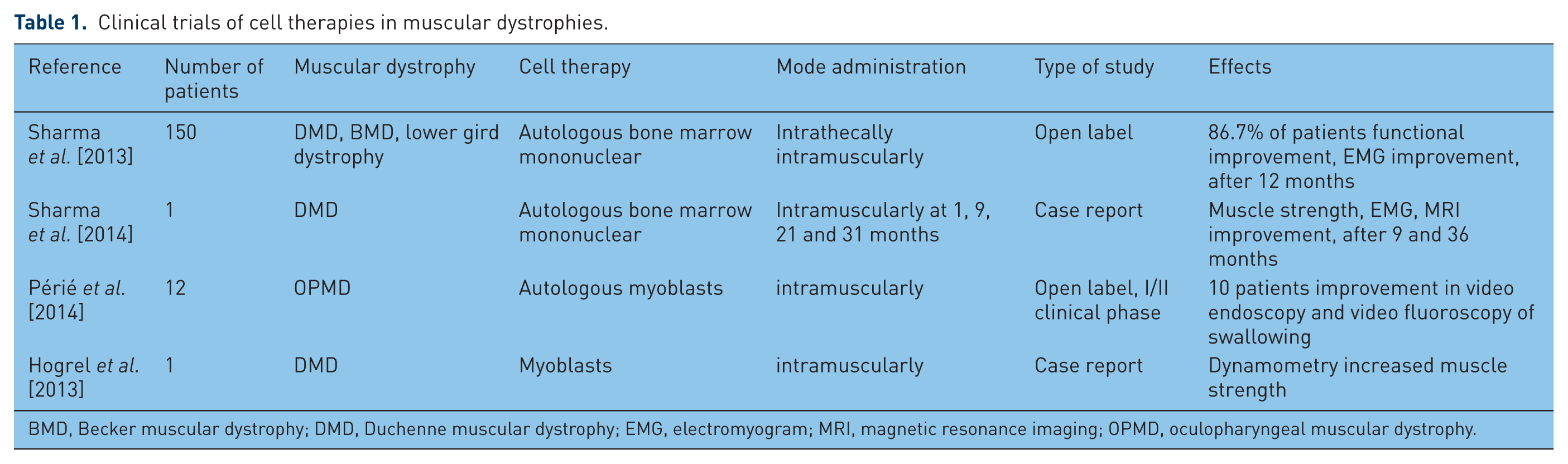
BMD, Becker muscular dystrophy; DMD, Duchenne muscular dystrophy; EMG, electromyogram; MRI, magnetic resonance imaging; OPMD, oculopharyngeal muscular dystrophy.
Périé and colleagues conducted an open phase I/IIa clinical study using autologous myoblast transplantation in 12 adult patients with oculopharyngeal muscular dystrophy (OPMD) [Périé et al. 2014]. OPMD can be an autosomal dominant neuromuscular disease or autosomal recessive which appears in early middle age (fifth decade). Progressive ptosis and weakness of the extraocular muscles is the initial clinical finding. Dysphagia (swallowing difficulties) begins with food but, as the condition worsens, liquids become difficult to swallow as well. Proximal limb weakness develops later on in the disease and usually occurs near the center of the body, particularly muscles in the upper legs and hips. This condition progresses slowly over time and individuals may need assistance of a cane or walker, but rarely will they need a wheelchair [Chien, 2012].
The feasibility and safety endpoints of autologous myoblast (178 million) transplantation in the pharyngeal muscles were assessed by video endoscopy in addition to physical examinations. Therapeutic benefits were also assessed through video endoscopy and video fluoroscopy of swallowing, quality-of-life score, dysphagia grade and a drink test. Short- and long-term (2 years) safety and tolerability were observed in all patients, with no adverse effects. There was an improvement in the quality-of-life score for all patients and no functional degradation in swallowing was observed for 10 patients.
In case reports, Sharma and colleagues and Hogrel and colleagues demonstrated beneficial effects of autologous bone marrow mononuclear and myoblast transplantation in patients with DMD [Sharma et al. 2014; Hogrel et al. 2013]. Sharma and colleagues demonstrated increased muscle strength in clinical examination [Sharma et al. 2014]. Furthermore, magnetic resonance imaging (MRI) showed no increase in fatty infiltration until the end of the follow-up period. An EMG study showed improvement in the vastus medialis muscles 9 months after the first transplantation, which was maintained after 3 years. Hogrel and colleagues reported the unique situation of a symptomatic female DMD patient who was transplanted with myoblasts received from her asymptomatic monozygotic twin sister 20 years ago [Hogrel et al. 2013]. Dynamometry was performed to detect the long-term effects of this cell therapy, and the long-term safety of myoblast transplantation was established by this exceptional case.
In theory, ideal stem cells used to treat DMD should fulfil several criteria, including: (i) be expandable in vitro without losing stem cell proprieties; (ii) be immuno-privileged; (iii) differentiate into muscle fibers either to repair damaged fibers or to replace fibers that have already been lost; (iv) reconstitute the satellite cell pool with functional stem cells, so that when a fiber or part of a fiber undergoes necrosis in the future, satellite cells capable of producing dystrophin are present to repair and maintain the fiber; and (v) lead to improvement in muscle strength so that the treated patient experiences an improved quality of life [Meng et al. 2011].
Gene therapy
Gene therapy for DMD requires the delivery of a new dystrophin gene to all muscles of the body, which make up greater than 40% of the body mass. The gene therapy approach is directed at restoring the contractile capacity of the skeletal muscle by introducing a functional copy of DMD in muscle fibers. The main challenge is the large size of dystrophin cDNA (13 kb of sequence) [Mendell et al. 2012]. However, the presence of very mild cases of DMD characterized by a conserved reading frame and loss of a major portion of the central ‘rod domain’ led to the design of mini and micro dystrophins that can fit in viral vectors (retroviruses and lentiviruses). The best results were observed in younger animals: muscle biopsy detected increased trans gene expression in 65% of the fibers. Furthermore, the muscle was more resistant to contraction and able to generate greater strength [Kobinger et al. 2003].
A clinical trial was recently carried out in six patients with DMD. Low and high doses of a recombinant adeno-associated virus serotype 2 carrying a mini-dystrophin were injected into the biceps muscle [Mendel et al. 2010]. Muscle biopsies were performed 42 days after administration in four patients and after 90 days in two patients, and compared with a sample of contralateral untreated muscle. All the samples contained the DNA vector. Lymphocyte infiltration suggested an unpredictable T-cell immune response against the viral vector.
According to Konieczny and colleagues, the immunogenicity of lenti and adenoviruses as vectors precludes them from use in systemic administration due to the danger of producing a life-threatening systemic immune response [Konieczny et al. 2013].
In addition to viral gene therapy, several nonviral replacement and repair approaches have been studied for treatment of DMD, for example, delivery of unencapsidated plasmids, changing the mRNA splicing, and ribosomal read through of premature stop codons.
Exon skipping and suppression of stop codons are promising approaches in increasing dystrophin expression in patients with DMD.
Exon skipping
Most mutations in the dystrophin gene of patients with DMD are deletions that disrupt the open reading frame. The length and structural characteristics of dystrophin, which contains repetitive domains, suggest the possibility of excluding disruptive exons from mRNA during splicing, partially preserving protein function. It is suggested that dystrophin levels of 30–60% may preserve muscle function and have been hypothesized to ensure the preservation of muscle strength [Muntoni and Wells, 2007].
Based on this evidence, exon skipping is being heavily researched for the treatment of DMD where the muscular protein dystrophin is prematurely truncated, which leads to a nonfunctioning protein. In molecular biology, exon skipping is a form of RNA splicing used to cause cells to ‘skip’ over faulty or misaligned sections of genetic code, leading to a truncated but still functional protein despite the genetic mutation. Exon skipping is used to restore the reading frame within a gene [Touznik et al. 2014].
Currently, clinical trials are designed to promote exon 51 skipping in DMD patients, expecting an improvement in their clinical phenotype to at least a BMD-like phenotype. The choice of exon 51 was based on two considerations: (i) in-frame deletions of this portion of the gene are generally associated with mild BMD phenotypes; and (ii) out-of-frame mutations that could benefit from exon 51 skipping account for at least 20% of DMD mutations [Helderman-van den Enden et al. 2010].
Modulation of splicing is achieved with antisense oligonucleotides (AONs), DNA molecules capable of binding intronic and exonic mRNA sites, and modifying splicing events.
Patients with genotypes suitable for applying this multiple skipping approach represent 63% of DMD patients. Skipping exons 45–55 is also suggested, considering that individuals with this deletion present with an exceptionally mild BMD phenotype [Aoki et al. 2012].
Exon skipping recently gained interest because of optimistic results in clinical trials. Systemic administration of the antisense oligonucleotide PRO051showed dose-dependent molecular efficacy in patients with DMD, with a modest improvement in the 6-minute walking test after 12 weeks of extended treatment [Goemans et al. 2011].
Ambulation improvements in a population of patients with early stage DMD are encouraging, but need to be confirmed in larger studies. Exon skipping provides a mutation-specific, and thus potentially personalized, therapeutic approach for patients with DMD.
Suppression of stop codons
Ataluren (formerly known as PTC124) is a novel, orally administered small molecule compound for the treatment of patients with genetic disorders due to a nonsense mutation; it is in clinical development for the treatment of DMD caused by a nonsense mutation. The safety and tolerability of ataluren were confirmed in a phase IIa study, which recruited 38 ambulant and non-ambulant boys older than 5 years of age. Muscle biopsy samples taken after 28 days of treatment revealed a mean 11.1% increase in dystrophin expression. A significant reduction in creatine kinase (CK) levels was also recorded. A phase IIb double-blind, placebo-controlled clinical trial with ataluren valuated the safety and efficacy of administering the drug for 48 weeks in 174 patients with DMD/BMD patients [ClinicalTrials.gov identifier: NCT00592553. Patients older than 5 years of age who were able to walk unassisted for at least 75 meters during the 6-minute walking test. The primary outcome was improved ambulation as assessed by the 6-minute walking test (the aim was an increase of 30 meters in the final distance compared with placebo). However, the study was stopped because the primary outcome was apparently not reached. However, a more detailed analysis of the data revealed that patients receiving low-dose ataluren exhibited better performances in the walking test than patients receiving placebo (29.7 meters more than placebo at the end of the study period) and less of a decline in timed function tests [Finket et al. 2010].
Corticosteroids in DMD
Daily corticosteroids are the gold standard treatment for ambulant patients with DMD. The use of corticosteroids leads to an improvement in the muscle strength of patients affected with DMD [Bushby et al. 2004].
Long-term therapy delays the loss of ambulation (by several years), reduces the need for vertebral surgery, improves cardiopulmonary function, postpones non-invasive ventilation and generally improves life expectancy and quality [Shapiro et al. 2014]. Starting treatment before the plateau in motor skills (4–6 years of age) is strongly recommended, whereas therapy is not indicated in patients younger than 2 years of age [Bushby et al. 2010].
Introducing treatment after the loss of ambulation appears to preserve upper limb strength, reduce the progression of scoliosis, and delay pulmonary and cardiac decline [Moxley et al. 2010].
The key mechanisms of action of corticosteroids are still poorly defined, but are probably related to the modulation of cellular events, including apoptosis, inflammation, regulation of calcium concentration and myogenesis.
Conclusion
Treating DMD has been palliative in nature for decades. With discoveries involving stem cells and their features, along with the possibility of obtaining therapeutic applications as well as factors of their release, new treatment methods for the most common progressive pediatric myopathy and other diseases have emerged. However, such discoveries are still in the very early stages and this method of therapy requires further careful, in-depth studies and observations (Table 2).
Pros and cons of cell therapy in patients with Duchenne muscular dystrophy.

In our opinion, gene therapy including exon skipping and suppression of stop codons offers promising approaches for increasing dystrophin expression in patients with DMD. As a genetic disorder, logically DMD must be cured by the correction of an invalid gene. However, there are different mutations, so such therapies must be individualized. Because DMD is a progressive disease, it would be logical to introduce gene therapy during the first year of the lives of these patients.
Footnotes
Acknowledgements
We wish to thank Urszula Humieniak-Dworakowska and EditMyEnglish, an affiliate of Grammar Labs LLC (USA), for correcting our manuscript.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.