
Abstract
Introduction:
Information on use of palliative care services among individuals with Duchenne and Becker muscular dystrophy is scant despite the clearly documented need.
Methods:
We examined associations between uptake of palliative care services by 233 males with Duchenne and Becker muscular dystrophy aged 12 and older for both caregiver and affected male characteristics using the Muscular Dystrophy Surveillance Tracking and Research Network baseline interview.
Results:
Ninety-one percent of caregivers (213/233) used at least one palliative care service. Case management had the highest frequency of use (59%). Use of palliative care was more frequently associated with the characteristics of affected males, as were some individual palliative care services. Utilization of six individual services differed among Muscular Dystrophy Surveillance Tracking and Research Network sites. While research suggests that pain is a frequent problem in Duchenne and Becker muscular dystrophy, only 12.5% reported use of pain management services.
Discussion:
Although palliative care use among families of males with Duchenne and Becker muscular dystrophy is high overall, there is much variability in use of individual services. Use of palliative care is driven by disease experience in the affected male. Many of the care recommendations for these individuals highlight the importance for early involvement of palliative care professionals.
Keywords
Background
Duchenne muscular dystrophy (DMD) is a genetic neuromuscular disorder resulting in progressive muscle weakness and loss of skills, orthopedic abnormalities, and cardiac and respiratory insufficiencies. With improved medical interventions and intensive health supports, individuals with DMD now live into their third decade, but disease progression is variable and difficult to predict.1–3 As a result, there is an increasing need for palliative care services that are today viewed as complementary to medical interventions.3–5
The current definitions of palliative care address much more than end-of-life care and include the early stages of a condition.4–7 Services typically considered as palliative include respiratory care to improve functioning and maintain quality of life, case management, counseling about decision-making as the disease progresses, legal planning like advanced directives, and other supportive services, all of which are critical in DMD.3,5,8–10 Despite the documented importance of palliative care overall, there has been some debate about its role in the care of individuals with neuromuscular disorders. 11
The study described herein extends our earlier research to quantify utilization of palliative care among families of individuals with DMD. 11 Our current research includes families of individuals with DMD and Becker muscular dystrophy (BMD), a generally milder form of muscular dystrophy. The aims are to (1) describe palliative care services that families of a large cohort of males with DMD and BMD, hereafter DBMD, had ever received and (2) evaluate factors associated with utilization of services.
Methods
We utilized information collected through the Muscular Dystrophy Surveillance and Research Network (MD STARnet) baseline interview dataset. MD STARnet is a network of six sites funded by the Centers for Disease Control and Prevention to conduct population-based surveillance and research for DBMD.12,13 Activities began in 2002 with four geographic regions of the United States (Arizona, Colorado, Iowa, and western New York). Two additional sites were subsequently added to the network: Georgia (2005) and Hawaii (2008). The surveillance methodology has been described elsewhere. 13 Individuals with DBMD were included in the network if they were born on or after January 1, 1982 and resided in one of the sites. Data were collected on individuals through death, out migration from the catchment area, or the end of the surveillance project. Sites collected data under a public health authority or Institutional Review Board (IRB) approvals.
The MD STARnet conducted a series of interviews, the first of which were baseline interviews of primary caregivers of 364 living or deceased males identified during the first two surveillance years (April 2004–August 2006) from Arizona, Colorado, Georgia, Iowa, and western New York. Hawaii did not participate in the interview component. Local IRB approval to conduct interview data collection with primary caregivers was obtained at each site separately from any surveillance approvals obtained. Written informed consent was waived as all participants were contacted by mail and participated by phone. Interviews with primary caregivers were conducted during 2007–2012 and collected data on familial and socioeconomic characteristics, healthcare and other services received, including palliative care. 12 Regarding palliative care, primary caregivers were asked to indicate if services had ever been received for the male with DBMD under their care. Sample size included parents of all individuals identified, abstracted, and classified as having DBMD, which was considered a population-based cohort. There were a total of 464 identified index males, of which 419 were considered eligible for the survey.
Settings/subjects
Details of the MD STARnet survey sample and baseline interview have been reported previously. 12 Data for the younger affected siblings were not included in the analyses to eliminate duplicate primary caregiver responses. We excluded one male who moved out of the United States and another who was determined not to have DBMD, resulting in a sample of 362 affected individuals and their primary caregivers. We excluded those affected males who were under the age of 12 years at the time of the interview, resulting in a total of 233 primary caregivers and affected individual pairs analyzed. The age exclusion allowed us to make our data comparable to those reported previously by our group 11 and assess data for families whose children were likely at the stage of requiring supportive services, interventions, and other planning relevant to palliative care.
Measurements
The use of palliative care was measured as receipt of at least one palliative care service (hereafter palliative care use) and uptake of 14 individual services as reported by the affected males and their primary caregivers. The individual services included attendant care, case management, homemaker services, mental health services, pastoral care, respite care, social work, transportation, dietary services, home meals, hospice care, pain management, respiratory care, and skilled nursing.
Palliative care use and individual palliative services were evaluated in relation to selected characteristics of the affected males and primary caregivers in the families. Characteristics of the latter included age at interview (25–39/40–49/50–64), race/ethnicity as reported by the primary caregiver (white non-Hispanic/Hispanic/other), education (⩽high school/some college or vocational/college graduate), household size, the MD STARnet site (Arizona/Colorado/Iowa/western New York), whether family had healthcare insurance (yes/no), whether family had insurance denied (yes/no), current marital status if primary caregiver was the biological parent (single/married), whether primary caregiver works or goes to school (yes/no), and the number of hours the primary caregiver spends at work or school.
Characteristics of the affected males are variables describing their disease experience. They included person-years affected with disease (i.e. duration of disease), disease phenotype, use of a wheel chair, age when wheel chair was first used, use of noninvasive positive pressure ventilation (NIPPV) devices, age when NIPPV was first used, age when first had trouble walking or running, and age when first noted speech delay. Person-years with disease was calculated as the difference between age at interview and age at diagnosis. Disease phenotype was based on age of onset of signs and symptoms. Affected males who had signs and symptoms before their sixth birthday were classified as early onset. If the signs and symptoms started after the sixth birthday, then onset was classified as late.
Statistical analyses were conducted to examine associations between each characteristic and palliative care use, following the descriptive approach in previous MD STARnet reports of services utilization.12,14 For palliative care use and individual service uptake, the comparison group included primary caregivers who reported no use of palliative care and those who reported no use of the individual service, respectively. T-tests and chi-square tests were used to test for differences in means and proportions, respectively. In all statistical tests, p-value <.05 was considered to be statistically significant.
Results
As reported previously, the response rate for the MD STARnet baseline interview was 53.8%, with respondents more frequently being mothers (87.5%), who were older, white non-Hispanic with at least a high school education. 12 The median age of the primary caregivers at interview in our sample was 45.8 years, and 45% reported family incomes greater than US$50,000. Among the 233 affected males in the analysis, 185 (79%) had early onset of signs and symptoms and the median ages at interview and at DBMD diagnosis were 17.8 and 5.0 years, respectively. The mean for person-years of disease was 12.9. Comparing the younger cases that were excluded from the analysis with the analytic dataset, we found that that primary caregiver’s median age at interview, affected male’s median age at interview, and person-years of disease were all predictably lower in the excluded cases. Families of excluded cases also had a higher proportion of incomes greater than US$50,000 (53.9% vs 45.0%). The analytic dataset included a higher proportion of individuals with the late-onset phenotype, which was also reflected in an older median age at diagnosis (5.0 vs 4.0 years).
Palliative care use
Among the 233 primary caregivers with valid data, 91% (213/233) reported palliative care use (Table 1). Of the primary caregivers reporting receipt of palliative care, more than half reported receipt of five or more individual services. Figure 1 presents the frequency of use for each service compared to the previous study. 11 Case manager services were the only services received by more than half of families. All remaining individual services were received by less than 48% of families.
Associations between selected affected male and caregiver characteristics and use of at least one palliative care services, MD STARnet baseline interview.

DBMD: Duchenne and Becker muscular dystrophy; MD STARnet: Muscular Dystrophy Surveillance, Tracking, and Research Network; NIPPV: noninvasive positive pressure ventilation.
Chi-square test computed with new categories for caregiver’s age (20–49 vs 50 years or above); caregiver’s race/ethnicity (non-Hispanic White vs others); caregiver’s education (high school or lower vs some college or more); family income (US$50,000 or less vs >US$50,000).
Chi-square p-value <.01.
Chi-square p-value <.05.
t-Test p-value <.05.
One case only, so data not shown.
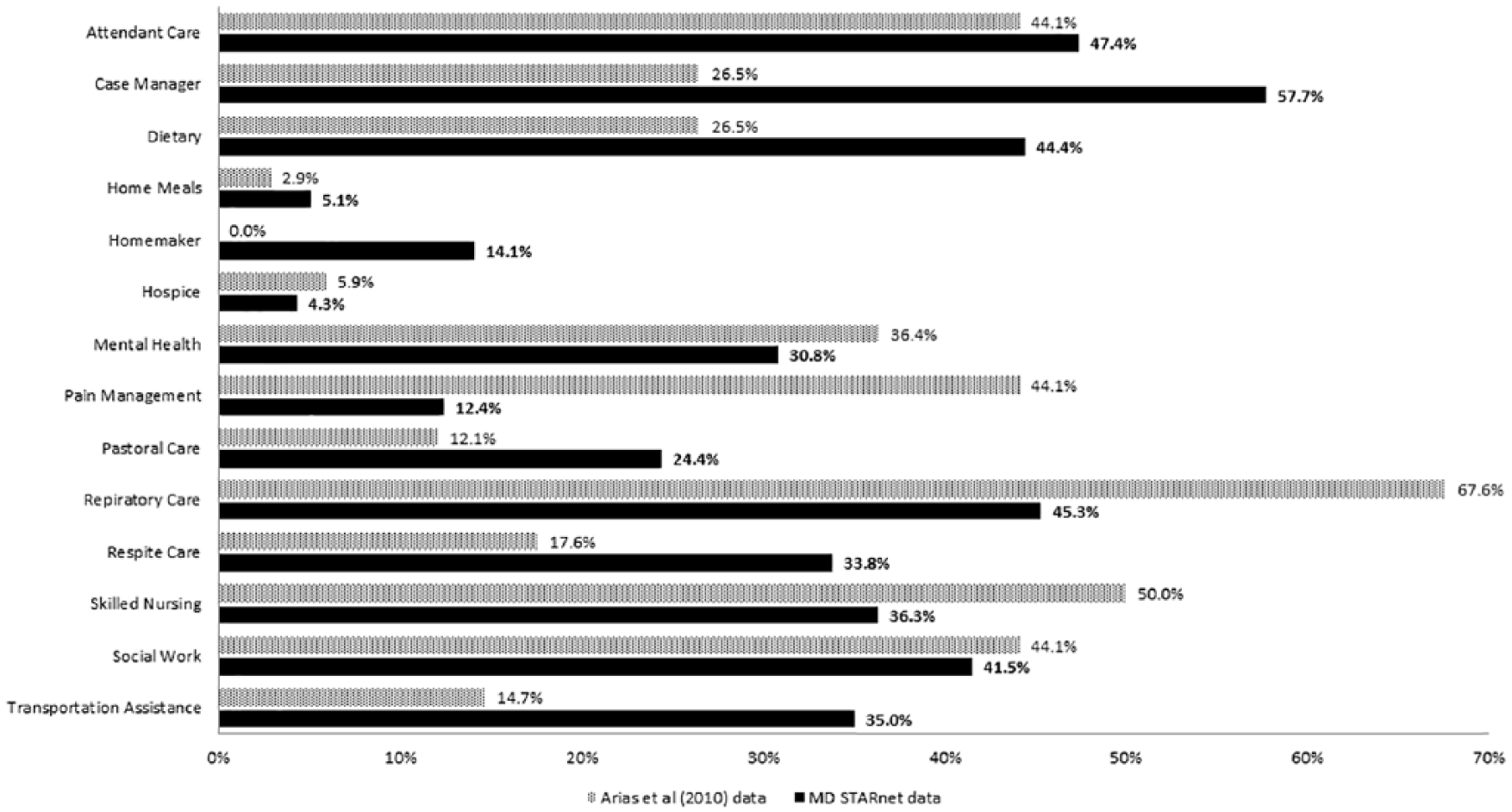
Palliative care services ever received from the Arias et al. 11 pilot and the MD STARnet interview data.
Associations between palliative care use and characteristics of respondents
Use of palliative care in relationship to the caregiver and affected male characteristics is shown in Table 1. No associations were found between palliative care use and specific caregiver characteristics or MD STARnet site. However, users of palliative care were more likely to have lower family income. Use of palliative care was not associated with the age when NIPPV devices were first used or age when speech delay was first noted. Affected males who used palliative care had significantly longer duration of disease and were significantly younger when they first used a wheel chair and when they first experienced trouble walking/running than nonusers (Table 1). Those who used palliative care also were more likely to have the early-onset disease phenotype, use a wheel chair, and use NIPPV devices.
We assessed the relationship of the use of individual behavioral/social-related palliative care services with primary caregiver and affected male characteristics (Table 2). No significant associations were found between the use of individual services and primary caregiver’s age at interview, marital status, and household size, so these characteristics are not shown. Use of certain behavioral/social-related services was significantly associated with indicators of socioeconomic status. Users of respite and transportation services were more likely to have lower education and for transportation less likely to be non-Hispanic white. Use of social work was more likely among lower-income families. Significant variation among sites for use of case management, homemaker, respite care, and transportation was observed. With respect to characteristics of affected males, those who used mental health services had longer duration of the disease and were more likely to be using a wheel chair. Males who used pastoral care were those with longer disease duration. Families that used respite care were more likely to have a male using a wheel chair and NIPPV devices. Males who used attendant care and transportation services had longer disease duration and were more likely to use a wheel chair. Users of attendant care were also younger when they first used a wheel chair and were more likely to be using NIPPV devices. Those who used homemaker services were more likely to be using NIPPV devices and were younger when they first experienced trouble walking or running. Use of case management was more likely in families of males who had longer disease duration, had the early-onset phenotype, were using a wheel chair and were younger when they first did so, were using NIPPV devices, and were younger when they first had trouble walking or running. Usage of social work was more likely when males had the early-onset phenotype, were using a wheel chair and were younger when they did so, and were using NIPPV devices.
Associations between selected affected male and caregiver characteristics and use of behavioral and social-related palliative care services.

MD STARnet: Muscular Dystrophy Surveillance, Tracking, and Research Network; NIPPV: noninvasive positive pressure ventilation.
Numbers reported may not add to the total number of respondents as questions may have been left blank by a respondent but the data still included in the overall analysis.
Chi-square test computed with new categories for caregiver’s race/ethnicity (non-Hispanic White vs others); caregiver’s education (high school or lower vs some college or more); family income (US$50,000 or less vs >US$50,000).
Significant association between caregiver’s race/ethnicity and use of transportation (p < .01).
Significant associations between caregiver’s education and use of respite care (p < .05) and transportation (p < .01).
Significant associations between MD STARnet site and use of case management (p < .01), homemaker services (p < .01), respite care (p < .01), and transportation (p < .05).
Significant association between family income and use of social work (p < .05). Association between family income and use of transportation trended close to significance (p = .08).
Significant association between family having insurance denied and use of mental health services (p < .05).
Significantly more person-years of disease among those who use attendant care (p < .01), case management (p < .01), mental health services (p < .05), pastoral care (p < .05), and transportation (p < .01).
Significant associations between disease phenotype and use of case management (p < .01) and social work (p < .05).
Significant associations between wheel chair use and use of attendant care (p < .01), case management (p < .01), mental health services (p < .05), respite care (p < .01), social work (p < .01), and transportation (p < .01).
Significantly younger age when they first used a wheel chair among those who used attendant care (p < .05), case management (p < .05), and social work (p < .05).
Significant associations between use of noninvasive positive pressure ventilation and use of attendant care (p < .01), case management (p < .01), homemaker services (p < .05), respite care (p < .01), and social work (p < .05).
Significantly younger age when they first had trouble walking or running among those who used case management (p < .01) and homemaker services (p < .01).
Associations between health- and medical-related palliative services and primary caregiver and affected male characteristics are shown in Table 3. Significant variation among MD STARnet sites was found for use of dietary and skilled nursing services. Use of both respiratory and skilled nursing services was more likely in lower-income families. Affected males who used dietary services were more likely to be using a wheel chair and NIPPV devices and were younger when they first experienced trouble walking or running. Users of pain management had a longer duration of the disease and were more likely to be using NIPPV devices. Finally, males who used both respiratory and skilled nursing services had experienced more years with the disease, were more likely to be using a wheel chair and were younger when this was first done, and were more likely to be using NIPPV devices.
Associations between selected caregiver and affected male characteristics and use of health- and medical-related palliative care services.

MD STARnet: Muscular Dystrophy Surveillance, Tracking, and Research Network; NIPPV: noninvasive positive pressure ventilation.
Numbers reported may not add to the total number of respondents as questions may have been left blank by a respondent but the data still included in the overall analysis.
Chi-square test computed with new categories for caregiver’s race/ethnicity (non-Hispanic White vs others); caregiver’s education (high school or lower vs some college or more); family income (US$50,000 or less vs >US$50,000).
Significant associations between MD STARnet site and use of dietary services (p < .05) and skilled nursing (p < .01).
Significant associations between family income and use of respiratory care (p < .05) and skilled nursing (p < .01). Association between family income and use of pain management trended close to significance (p = .09).
Significant association between family having insurance declined and use of dietary services (p < .01).
Significant associations between caregiver working or going to school and use of pain management (p < .01) and skilled nursing (p < .05).
Significantly more person-years of disease among those who used pain management (p < .05), respiratory care (p < .01), and skilled nursing (p < .01).
Significant associations between wheel chair use and use of dietary services (p < .01), respiratory care (p < .01), and skilled nursing (p < .01). Association between wheel chair use and use of pain management trended close to significance (p = .07).
Significantly younger age when they first used a wheel chair among those who used respiratory care (p < .01) and skilled nursing (p < .05).
Significant associations between use of noninvasive positive pressure ventilation and use of dietary services (p < .05), pain management (p < .01), respiratory care (p < .01), and skilled nursing (p < .01).
Significantly younger age when they first had trouble walking or running among those who used dietary services (p < .05).
Discussion
The sparse literature on palliative care use among individuals with DMD suggests that services are not recommended or utilized as much as they could be. Previous reports indicate variable use of palliative care by individuals with DMD and their families as well as variation in the individual palliative care services used.10,11
We have described palliative care use as reported by 233 primary caregivers of males with DBMD. Although use of any palliative care in our study was quite high (91%), there was considerable variability in usage of individual services. The number of services received ranged from 1 to 12 with a median of 4 out of 14 services listed (data not shown). Only one service, case management, was received by the majority of males with DBMD (59%); all others were received by less than half. Of note, the use of pain management services (12.6%) was the same as previously reported. 11 This result remains of interest, as a comprehensive review of pain research in DMD concludes that it is a common problem in this population. 15 The data suggest that pain may be treated by providers not associated with formal pain management services. Ironically, respiratory care and skilled nursing were reported less frequently than in our previous study despite the release of guidelines on respiratory care and monitoring in 2004. 16
In our study, we found a significant association between the use of at least one palliative care service with lower income, which may be an artifact of the receipt of Medicaid versus private insurance coverage and costs. Similarly, use of respiratory care, skilled nursing, and social work were associated with lower income. Some other services had more frequent use among those who were Hispanic or other or had a high school education or less. These findings contrast with those of a previous MD STARnet study of complementary and alternative medicine (CAM), which found CAM services were used more frequently in families where the primary caregiver was college educated and income was higher. 12
One finding in need of further study is the variation among sites in the use of individual palliative care services. The current research extends that of Pandya et al. 17 who found differences among MD STARnet sites in receipt of dietary and case management services in families of affected males across all ages. In our restricted range of affected males aged 12 and older, we found site differences for these same two services, as well as four additional palliative care services. Research has also identified MD STARnet site differences in use of rehabilitative devices by affected males and the age when use of these devices was initiated. 18
In our previous report, 11 for all of the palliative care services we examined, we found that service utilization is associated with the predisposing variable current age of the individual with DMD, irrespective of other factors we evaluated. In this new investigation, we have identified specific characteristics of affected males associated with use of palliative care in general and for specific services. Across all characteristics we examined, there were significant associations of service usage with characteristics of affected males that reflect disease progression and severity, as would be expected in this population. Males with DBMD who used palliative care were those who had early onset of disease, were younger when they first had trouble walking or running, and had experienced more years with the disease. In addition, they were using a wheel chair and were younger when they first did so, and were using NIPPV devices. A similar pattern was found with individual palliative care services.
To our knowledge, our study is the first that utilizes a population-based sample of males with DBMD and their families to examine the palliative care use and factors associated with their use. Thus, these findings may be indicative of the utilization of palliative care in this population. Most of the previous studies have been based on small surveys. 11
There are a number of limitations of the MD STARnet baseline survey including the response rate of just 53.8% and the possible influence of participation bias given that the respondents were older, non-Hispanic whites with more education. 12 There was potential recall bias given that information was self-reported by primary caregivers who might not have remembered all of the palliative care services received. Another limitation is that we did not account for availability of palliative care services among MD STARnet sites. Also, we did not inquire in the questionnaire whether palliative care services were offered to families by their care providers or whether they were offered but not available. Our sample selection could introduce some sampling bias due to the inclusion of a larger proportion of late-onset affected males who might demonstrate a milder phenotype, thereby reducing the need for some palliative care services. Understanding the reasons behind the lack of palliative care service uptake is a critical question to address in future research.
The earliest research on palliative and hospice care in individuals with advanced end-stage muscular dystrophy used qualitative methods to investigate commonalities in the need for palliative care. 11 The early studies concluded that palliative care services for individuals with muscular dystrophy had not been sufficiently developed to be considered part of existing healthcare for these disorders. Our previous pilot of 34 families of young men with DMD demonstrated that families are not using palliative care and a need to improve awareness of these services. 11 The current study provides population-based data on the largest sample to date of individuals with DBMD and their use of palliative care.
The use of palliative care in rapidly progressing conditions like DBMD provides families with numerous advantages. These include empowering a family to make decisions proactively about how to handle specific disease progression limitations (i.e. scoliosis surgery; tracheostomy); engaging the family in focusing on a long life rather than avoiding the discussion of future functional decline as a means for avoiding discussion of a child’s death; and assisting with care coordination, management, and informed decision-making.3,9,19
Conclusion
Our study presents data from a population-based sample of young men with DBMD and their families regarding their use of palliative care services. The data support the following conclusions:
Although overall use of palliative care is high among families of males with DBMD, use of individual palliative care services is extremely variable.
All but one of the individual palliative care services were used by less than 50% of families and 9 of the 14 services were used by 37% or less families.
Use of palliative care services is associated with fewer predisposing and enabling characteristics such as primary caregiver’s education and family income than it is with the needs of affected males.
Palliative care services improve the quality of life for both caregiver and individuals with progressive conditions like DBMD. Our data suggest these services are underutilized among families of individuals with DBMD. Furthermore, our study points to a continuing need to educate healthcare providers and the public about palliative care and its capabilities for improving the quality of life among individuals with conditions like DBMD and their families. Redefining the role of palliative care for life-limiting pediatric conditions and incorporating these services early on in the disease process within specialty clinics would be an important next step in the process and would improve the understanding and awareness of available services. It would also foster proactive decision-making for families who are taught to deal with their child’s disease progression as living with a progressive disease rather than reaching various phases of decline toward death.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was either obtained from or waived by the Institutional Review Board at each individual site (AZ, CO, GA, IA, and wNY). Each site received Institutional Review Boardapproval for the caregiver survey (University of Arizona IRB-1, protocol 05-0426-01; Colorado Department of Public Health and Environment IRB, protocol 2006001; Georgia Department of Public Health IRB, protocol 090805; Centers for Disease Control and Prevention IRB-A, protocol 4792; University of Iowa IRB-1, protocol 200509724; New York State Department of Health, protocol 03-062).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the Cooperative Agreement numbers, DD000187, DD000189, DD000190, and DD000191 funded by the Centers for Disease Control and Prevention.
Informed consent
Verbal informed consent was obtained from all subjects before the study. Written informed consent was waived by IRBs as participants would not have face-to-face contact with any interviewers.