
Abstract
Background:
The enthusiasm for natalizumab, a highly efficacious agent in the treatment of multiple sclerosis (MS), has been tempered by the risks of progressive multifocal leukoencephalopathy associated with its use, and strategies to minimize those risks are of great interest. Extended interval dosing (EID) has been proposed as a way to maintain the efficacy of natalizumab while reducing exposure to it. We reviewed a cohort of patients who received natalizumab at 6–8-week intervals instead of the typical infusions every 4 weeks with the goal to assess if patients on EID had an increase in clinical relapses.
Methods:
This is a retrospective review of all patients with MS treated with natalizumab at two MS centers where patients were offered the opportunity to switch to an EID every 6 or 8 weeks.
Results:
A total of 361 patients received natalizumab for 22 ± 13 months (minimum duration 6 months). Of these, 96 patients received EID natalizumab at some point for 20 ± 11 months (minimum duration 6 months). Over the study period, there was no significant difference between the relapse rate in the monthly dosing (13%) and the EID (13%) groups of patients.
Conclusion:
Natalizumab is effective in controlling MS as very few clinical relapses were observed in our dataset. We found that EID did not compromise the treatment effect as measured by relapse rate and no significant breakthrough disease activity was observed. EID is an optional regimen for maintenance natalizumab therapy, but prospective studies are warranted to determine its efficacy.
Introduction
Natalizumab, a monoclonal antibody directed against α4 integrin, limits the entry of mononuclear cells into the central nervous system. It is typically administered every 4 weeks and its efficacy for treatment of multiple sclerosis (MS) was established in randomized clinical trials with both clinical and radiological outcome measures [Miller et al. 2003; O’Connor et al. 2005; Polman et al. 2006; Havrdova et al. 2009]. Natalizumab reduced clinical relapses and new lesions on magnetic resonance imaging (MRI) at levels exceeding the reductions obtained by injection therapies [Holmen et al. 2011] and a growing number of postmarketing studies have lent support to the superiority of natalizumab over interferon β and glatiramer acetate [Fernandez et al. 2012; Putzki et al. 2009, 2010a, 2010b; Castillo-Trivino et al. 2011; Oturai et al. 2009; Prosperini et al. 2011; Outteryck et al. 2010]. However, safety concerns, almost exclusively related to the association with progressive multifocal leukoencephalopathy (PML) [Linda et al. 2009], a potentially fatal infection caused by the John Cunningham (JC) virus, have led to instituting surveillance programs (Tysabri, the TOUCH Prescribing Program; http://www.tysabri.com/tysbProject/tysb.portal/) and the Tysabri Observational Program [Kappos et al. 2012], and have spurred the search for strategies that could minimize the risks of PML. This complication from natalizumab therapy is higher in patients that are positive for anti-JC virus serology, receive infusions for more than 24 months, or were subjected to prior immunosuppression [Kappos et al. 2011; Bloomgren et al. 2012].
A ‘drug holiday’, interruption of natalizumab for 3 months or longer, after 12–24 months of monthly infusions, has been proposed as a means to reduce the chance of PML and was found to be poorly tolerated, with increased numbers of MS relapses, typically occurring after 3 months of suspension [Killestein et al. 2010; Borriello et al. 2011]. We hypothesized that therapeutic effects could be maintained with extending the dosing by periods of 6–8 weeks [extended interval dosing (EID)] and performed a chart review for all consecutive patients who were followed at the Vanderbilt University Medical Center, Nashville, TN, USA and Barrows Neurological institute, Phoenix, AZ, USA and received natalizumab therapy for 6 months or longer over a 7-year period. We also looked at patients who discontinued or interrupted natalizumab therapy (‘drug holiday’).
Methods
As the study was retrospective and used existing data without collection of personal identifiers for patients, the Institution Review Boards at Vanderbilt University Medical Center and Barrow Neurological institute approved the study and waived the need for informed consent.
Natalizumab (http://www.tysabri.com/tysbProject/tysb.portal/) was reintroduced to the market in 2006. We retrospectively reviewed demographics, duration of therapy with natalizumab, disease severity by Expanded Disability Status Scale (EDSS), disease activity in terms of clinical relapses and MRI data of all consecutive patients who were followed at our institutions and received natalizumab for 6 months or longer in the period between September 2006 and April 2013.
After monthly infusions for 12–24 months, patients were offered the possibility of changing the monthly administrations to an EID of 6 or 8 weeks. Patients who were on EID for less than 6 months and elected to revert to monthly doses were counted as monthly dosing in our dataset.
MRI scans were obtained as part of the routine management and occurrence of new T2, fluid-attenuated inversion recovery or contrast enhancing lesions were counted as changes from the baseline scan done before the initiation of natalizumab, or the switch to EID regimen.
Statistical analysis was performed to test whether the EID regimen was as effective as standard monthly dosing using the Equivalence Test Based on the Generalized Linear Mixed Effects Model [Blackwelder, 1982]. The following assumptions were made: the baseline relapse rate (for monthly dosing patient/control) is 0.13, which is an empirical estimate from the data; the margin of error is 0.2, which means we would think the two groups have equivalent relapse rate if the difference in rate falls between -0.2 and 0.2.
Results
A total of 462 patients were identified in our database as having received natalizumab at least once. One hundred and one of them were removed from the statistical analysis as they discontinued natalizumab due to intolerance or had received the infusions for less than 6 months as of April 2013. Of the remaining 361 patients on natalizumab for 6 months or longer during the study period, 96 patients were on EID at some point. The demographic characteristics of the patients are shown in Table 1.
Baseline characteristics of patients in the study.
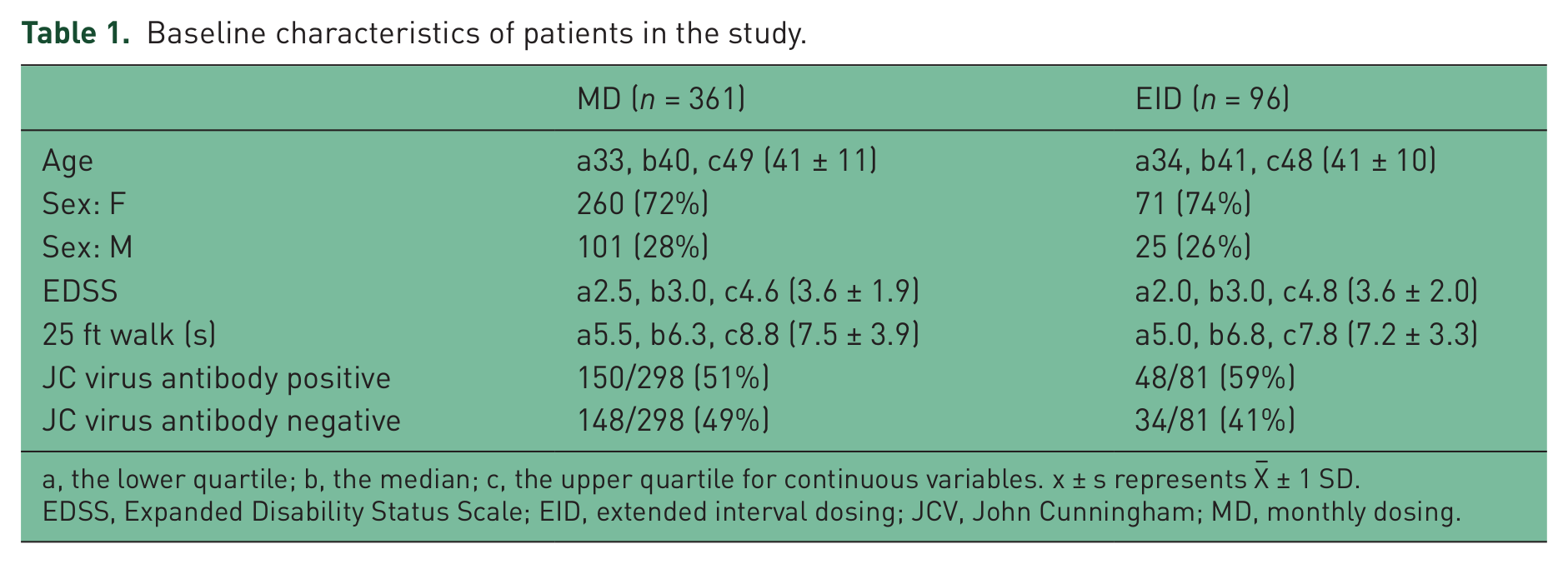
a, the lower quartile; b, the median; c, the upper quartile for continuous variables. x ± s represents X– ± 1 SD.
EDSS, Expanded Disability Status Scale; EID, extended interval dosing; JCV, John Cunningham; MD, monthly dosing.
The majority of patients were switched from a first-line therapy to natalizumab because of breakthrough disease activity, either by clinical relapses or evidence of new lesions by MRI. Forty-one patients were switched to natalizumab as they could not tolerate the first-line therapies, while in 17 patients natalizumab was the initial treatment of choice due to high disease activity at presentation.
There were no significant differences in the overall patient population and those who received EID, with regards to age, sex distribution, EDSS and 25 ft walk times.
We looked at the differences between clinical and radiological activities between patients on monthly dosing and EID (Table 2). Clinical events occurred at variable intervals after starting natalizumab, ranging from 1 to 27 months. The patients who had relapses within the first 6 months on therapy and elected to discontinue natalizumab were removed from the statistical analysis. There were a total of 46 relapses among the 361 patients during monthly dosing (13%). There were 13 relapses in the 96 patients during EID (13%). Using the Equivalence Test Based on the Generalized Linear Mixed Effects Model there was no difference in the relapse rate between monthly dosing and EID. The number of new MRI lesions was 36/340 (11%) in monthly dosing and 8/87 (9%) in EID.
Clinical relapses and MRI activity during the study period.

a, the lower quartile; b, the median; c, the upper quartile for continuous variables. x ± s represents X– ± 1 SD.
EID, extended interval dosing; MD, monthly dosing; MRI, magnetic resonance imaging.
A total of 75 patients discontinued natalizumab or went on a ‘drug holiday’ of 6 months or longer. Of the 75 patients, 22 had clinical relapses or MRI activity. The time to relapse during the drug holiday was 5.95 ± 2.27 months.
Of note, eight patients were tested for anti-natalizumab antibodies, prompted by the occurrence of new disease activity and five had positive results. Having all discontinued treatment within 6 months, they did not contribute to the data analysis.
Discussion
The conclusions that can be drawn from a retrospective study are necessarily limited. However, the following observations may be made. First, natalizumab is confirmed to be an effective agent for the treatment of MS, with levels of efficacy greater than those observed in the randomized clinical trials. We report a relapse rate for patients treated with natalizumab of 0.13 over the study period. This is in line with many other studies based on real world use of the medication [Fernandez et al. 2012; Putzki et al. 2009, 2010a, 2010b; Castillo-Trivino et al. 2011; Oturai et al. 2009; Prosperini et al. 2011].
Second, our results show that prolonged interruption of natalizumab is poorly tolerated, thus confirming the observations of other investigators [Killestein et al. 2010; Borriello et al. 2011; Kaufman et al. 2010]. The mean time to relapse during the drug holiday in our patient cohort was 5.95 months. The use of pulse doses of steroids was also found to be ineffective to control recurrence of disease activity [Borriello et al. 2012; Fox et al. 2014].
Third, we report our experience with the EID of natalizumab. The relapse rate in patients on EID was no different than the one in patients on monthly dosing. It is conceivable that the non-randomized nature of our study, where patients with less active disease may be more likely to be switched to the EID, predisposes to skewed results. However, given the overall low relapse rate, it is doubtful that this had an impact on our data. Moreover, strategies to personalize treatment choices are increasingly required and guidelines for the selection of patients who could be the best candidates for the treatment have been proposed [Bloomgren et al. 2012; Coyle et al. 2009]. In fact, the incidence of PML cases associated with natalizumab has paralleled the ever-increasing use of the medication (https://medinfo.biogenidec.com/). With the rationale of minimizing the risks of PML, other authors have explored dose-suspension strategies whose theoretical benefits are outweighed by recurrences of disease activity [Fox et al. 2014; West and Cree, 2010; O’Connor et al. 2011].
Although it is not clear if EID reduces the risk of PML any more than monthly dosing, α4 integrin saturation by natalizumab at the end of 4 weeks has been reported to range from 80% [Miller et al. 2003] to less than 40% [Hyams et al. 2007], and allowing recirculation of mononuclear cells via reduced receptor saturation during the second month could in theory preserve some degree of immune surveillance. A recent study aimed at monitoring the serum levels of natalizumab in patients with MS on monthly dosing of natalizumab has demonstrated that variations exist between individuals. Over time, in some patients who do not clear the medication within a 4-week period, it tends to accumulate in their serum [Foley, 2011].
EID has been adopted by other authors with consistency in safety and better tolerability over the suspension strategies [Tornatore and Erwin, 2012], and the data presented here suggest that EID of natalizumab is reasonable and does not compromise the treatment effects. EID is currently under investigation in a controlled clinical trial (Eudra CT Number: 2010-024000-10; https://www.clinicaltrialsregister.eu). Its potential for favorably impacting the incidence of PML could only be detected in the context of programs that monitor large numbers of treated patients [Bomprezzi et al. 2012].
Footnotes
Acknowledgements
The authors are thankful to Susan Couch, Iris Pena and Tabitha Medrano for their invaluable support with coordination of patients’ care, Dr Lily Wang and Yaping Shi for assistance with statistics, and the patients for their trust and cooperation with the treatment regimen.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Dr Bomprezzi and Dr Pawate have no disclosures to report.