
Abstract
Chronic inflammatory demyelinating polyneuropathy (CIDP) is an immune mediated disorder of the peripheral nervous system with clinical features that include weakness, sensory loss, imbalance, pain and impaired ambulation which may lead to substantial disability. This review highlights current treatment strategies for CIDP, how best to utilize proven therapies such as intravenous immunoglobulin, oral prednisone, pulse dexamethasone, and plasma exchange, and when and how to use alternative immunosuppressive agents when first-line therapies are ineffective or poorly tolerated.
Introduction
Chronic inflammatory demyelinating polyneuropathy (CIDP) is a chronic, acquired, immune-mediated condition affecting the peripheral nervous system [Köller et al. 2005; Dalakas, 2011]. The pathogenesis of CIDP is incompletely understood and includes several humoral and cell-mediated mechanisms [Köller et al. 2005; Dalakas, 2011]. The classic form of the disorder is characterized by: (1) progressive limb weakness, usually with a predilection for proximal muscles, sensory loss, and areflexia with a relapsing or progressive course; (2) electrophysiological features of demyelination, including prolonged distal motor and F-wave latencies, reduced conduction velocities, and conduction block and temporal dispersion; (3) laboratory features of albumino-cytological dissociation in the cerebrospinal fluid; and (4) inflammation, demyelination, and remyelination on nerve biopsy [Dyck et al. 1993; Joint Task Force of the EFNS and PNS, 2010]. In most cases the diagnosis can be confidently established by clinical and electromyography (EMG) criteria, and nerve biopsy is less often required but can be helpful in selected cases. Numerous clinical trials have established the short-term efficacy of immune therapies such as corticosteroids, plasma exchange (PE), and intravenous immune globulin (IVIg) as the mainstay of treatment for CIDP, with several reports indicating the promise of novel immune therapies [Dalakas, 2011]. Although guidelines for the diagnosis and treatment of CIDP have been developed, the large variety of clinical and electrophysiological variants, associated systemic conditions, and lack of sustained improvement with standard treatments in up to one third of cases provide challenges to the clinician in practice. This review highlights the currently accepted therapies for CIDP and the role of potentially effective but unproven novel therapies.
Clinical features
CIDP is one in a spectrum of acquired immune-mediated demyelinating neuropathies that differ from each other mainly in their time course and clinical features. The two traditional categories of acute inflammatory demyelinating neuropathy (AIDP; Guillain–Barré syndrome) and CIDP have similar presentations except that the symptoms peak in less than 4 weeks in AIDP and are monophasic, and progress for 8 weeks or more in CIDP. For an illness that reaches its nadir between 4 and 8 weeks, the term subacute demyelinating neuropathy has been used [Oh et al. 2003]. The natural history of the latter group can follow the pattern of either AIDP (monophasic course with a plateau and then recovery) or CIDP (progressive or relapsing). In large series, CIDP represents approximately 20% of initially undiagnosed neuropathies and accounts for approximately 10% of all patients referred to neuromuscular clinics. The disorder most commonly occurs in adults between 40 and 60 years, but can affect the elderly and children. There is a slight predilection for men. The prevalence of CIDP is approximately two to five cases per 100,000 individuals, comparable to the frequency of AIDP [Rajabally et al. 2009]. Two-thirds of cases are progressive and the remainder relapsing, although in the modern era ‘relapses’ often reflect treatment withdrawal (e.g. IVIg, or rapid tapering of prednisone), but also may be triggered by infections or other systemic illnesses. Spontaneous relapses tend to affect younger individuals.
In its classic form, the initial symptoms of CIDP are progressive, symmetric limb weakness and sensory loss that usually begin in the legs (Table 1). Patients report difficulty walking, climbing stairs, arising from a chair, and may fall, or they may complain of reduced manual dexterity (trouble buttoning shirts, pulling up zippers, etc.) if hand weakness is present. A core clinical feature is proximal limb weakness, indicating a non-length-dependent neuropathy that implies proximal nerve demyelination and distinguishes such cases from the far more commonly encountered distal axonal polyneuropathies. The majority of patients also have sensory features, with complaints of numbness, tingling or buzzing of the acral extremities (paresthesias), and gait unsteadiness reflecting a sensory ataxia. Neuropathic pain is less common. The examination shows symmetric proximal and distal limb weakness, generalized hyporeflexia or areflexia, and distal sensory loss with large fiber modalities (joint position, vibration) disproportionately affected [Gorson et al. 1997; Köller et al. 2005; Dalakas, 2011].
Clinical features of chronic inflammatory demyelinating polyneuropathy [Joint Task Force of the EFNS and PNS, 2010].

Electrodiagnostic criteria
Nerve conduction studies establish the diagnosis of CIDP with confidence in the majority of cases. Several electrodiagnostic criteria have been proposed, all requiring some combination of:
reduced conduction velocities (CVs; e.g. <80% of the lower limit of normal [LLN] if the distal motor amplitude is normal, and <70% of LLN if the amplitude is substantially reduced);
prolonged distal motor latencies (DMLs);
prolonged F-wave latencies (FLs; e.g. >125% of the upper limit of normal [ULN] if the distal motor amplitude is normal, and >150% of ULN if the amplitude is reduced for distal latencies and F-waves); and
conduction block/temporal dispersion (CB/TD; e.g. conduction block is >50% reduction of proximal/distal [p/d] amplitude and abnormal temporal dispersion is >130% increase of p/d duration);
these criteria were initially established by expert consensus for research purposes through the American Academy of Neurology (AAN) [Report from an Ad Hoc Subcommittee of the American Academy of Neurology AIDS Task Force. (1991).] (Table 2).
American Academy of Neurology Ad Hoc Subcommittee Electrodiagnostic Criteria for chronic inflammatory demyelinating polyneuropathy [Report from an Ad Hoc Subcommittee of the American Academy of Neurology AIDS Task Force. (1991).].
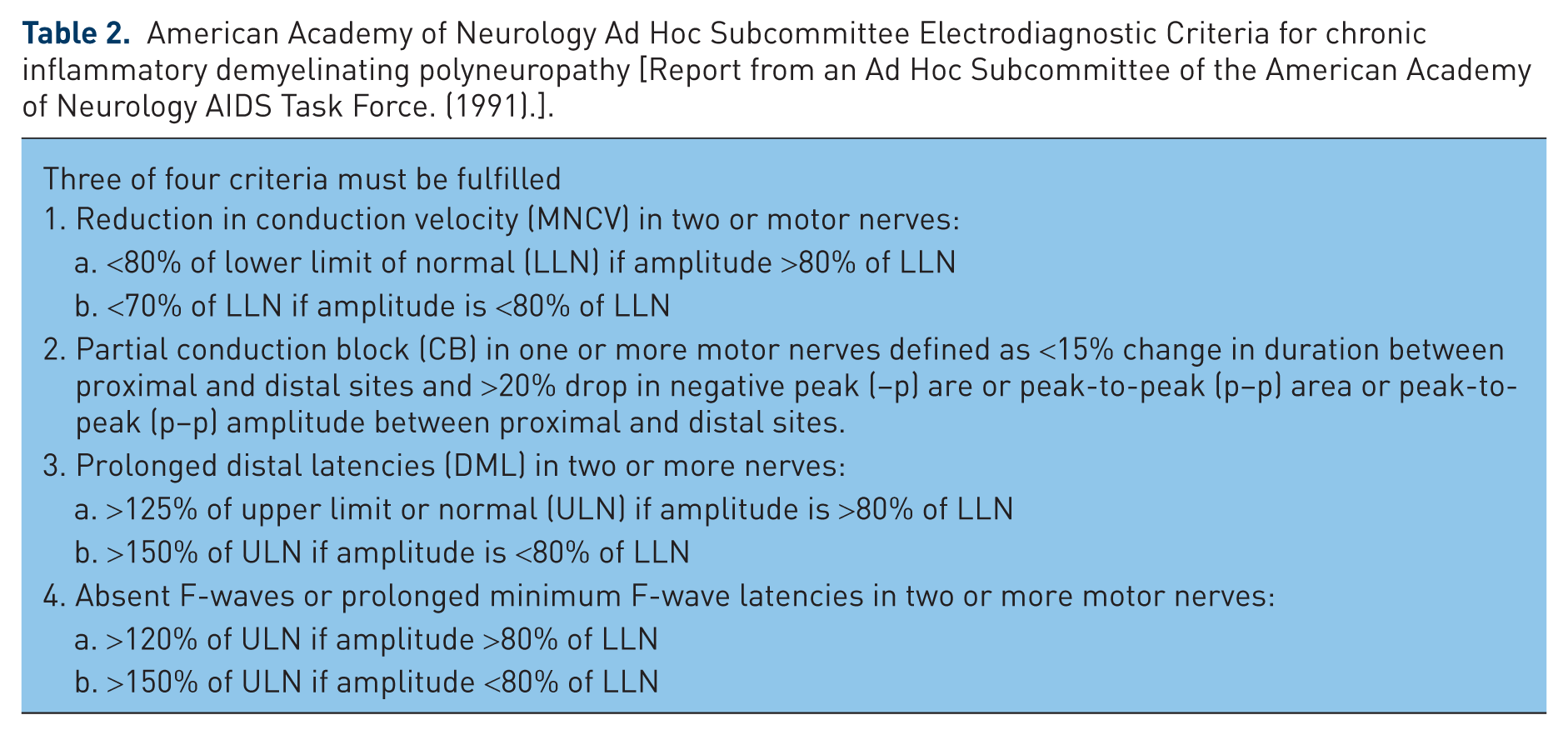
According to these AAN criteria, the presence of three of the four criteria, in two or more nerves, establishes the electrophysiological diagnosis of CIDP for research purposes. For the practicing clinician, these various schemes are contrived since only 50–60% of patients with typical clinical features of CIDP fulfill these strict electrodiagnostic criteria. Accordingly, over the last 20 years at least 15 alternative EMG criteria have been proposed with varying degrees of sensitivity and specificity [Bromberg, 2011], thus contributing to further controversy and confusion. Unfortunately, many of these criteria were established by way of circular reasoning or self-referential analysis (for example, investigators used certain EMG criteria to select CIDP cases to study, and then ‘validated’ the very same EMG criteria). Both the Koski and colleagues and EFNS diagnostic criteria (Tables 3 and 4) have high sensitivity (>80%) and specificity (>95%), and thus either can be recommended for use in clinical practice and for research purposes [Koski et al. 2009; Joint Task Force of the EFNS and PNS, 2010].
Koski and colleagues criteria for the classification of patients with chronic inflammatory demyelinating polyneuropathy (CIDP) [Koski et al. 2009].

According to American Academy of Neurology criteria
European Federation of Neurological Societies (EFNS)/Peripheral Nerve Society (PNS) Guideline Electrodiagnostic Criteria [Joint Task Force of the EFNS and PNS, 2010].

Electrodiagnostic studies have several important shortcomings in establishing the diagnosis of CIDP: (1) patients may accrue substantial axonal loss with absent or greatly reduced motor potentials, and therefore nerve conduction abnormalities may not fulfill criteria for demyelination; (2) those with a pure sensory variant may have absent sensory nerve action potential (SNAPs) and relatively normal motor potentials; (3) a few patients have electrodiagnostic abnormalities limited to proximal motor nerve segments that are detected only with motor root or Erb’s point stimulation [Menkes et al. 1998]; and (4) in clinical practice, there is a large group of patients, without axon loss, who do not fulfill any of the proposed EMG criteria and yet may still benefit from treatment [Magda et al. 2003]. In these patients, spinal fluid analysis and nerve biopsy may be especially helpful to confirm the diagnosis, and a therapeutic trial may be warranted in patients who do not fulfill strict electrodiagnostic criteria [Magda et al. 2003].
Treatment
The primary goals of treatment for CIDP are to reduce symptoms (weakness, sensory loss, imbalance, and pain), improve functional status (reduce disability and handicap), and if possible, maintain long-term remission. Conventional therapy for CIDP has included corticosteroids, PE, and IVIg (Table 5). Improvement can be expected in 50–80% of patients with one of the standard treatments (steroids, IVIg, PE) [Gorson et al. 1997; Köller et al. 2005; Dalakas, 2011]. Each of these treatments has been demonstrated to be superior to placebo in randomized, double-blind, placebo-controlled studies, and accordingly, insurance reimbursement in the United States should no longer be a problem. Furthermore, randomized, prospective clinical trials have shown that PE and IVIg, and IVIg and prednisolone, have similar short-term efficacy [Dyck et al. 1994; Hughes et al. 2002]. The practical issues associated with these agents are the lack of a durable response in many patients and the difficulties of using these therapies, ideally suited for short-term administration, for long-term management of a chronic disease. IVIg is expensive, time-consuming, and may have limited availability in some circumstances, PE can be invasive for those who require central venous catheters, and the therapy requires well-trained personnel at specialized centers. Corticosteroids have a large number of potentially serious side effects and often are tolerated poorly when used as a long-term therapy.
Therapy for chronic inflammatory demyelinating polyneuropathy.

Prednisone
Prednisone was first established as an effective therapy and superior to placebo in a 3-month, randomized, placebo-controlled trial of alternate-day, high-dose prednisone (120 mg) in 28 patients [Dyck et al. 1982]. The effect was similar between patients with a progressive and relapsing course. The average time to induce a response with prednisone (60 mg/day) has been reported to be approximately 2 months with maximal improvement not observed until after 6 months [Barohn et al. 1989]. One study showed improvement in disability scores within 2 weeks of starting 60 mg of daily prednisolone [Hughes et al. 2002]. A minority of patients remained in remission after tapering steroids, but most (up to 70%) have relapsed after discontinuing treatment and have required repeated courses of prednisone or alternative immunotherapy [Wertman et al. 1988]. In some patients the addition of azathioprine, or other so-called ‘steroid-sparing’ agents, may sustain a remission and reduce or eliminate the requirement for high-dose prednisone [Barohn et al. 1989; Dalakas, 2011], but this benefit has not been confirmed in a randomized, controlled trial [Dyck et al. 1985]. However, it should be noted that this study was limited in trial design due to the short duration of exposure to azathioprine, as the benefits of the drug typically require up to 12–18 months of therapy (see below). Young age at onset, duration of symptoms less than 6 months, slight neurologic impairment, and mild slowing of nerve conduction velocities have been associated with a favorable response to corticosteroids [Wertman et al. 1988]. Rapid tapering of prednisone also may increase the risk of relapse.
Owing to concern regarding long-term daily prednisone exposure, several alternative corticosteroid treatment regimens have been proposed. In a double-blind, placebo-controlled, randomized trial, high-dose oral dexamethasone (40 mg) was administered daily for 4 days sequentially, every month for 6 months, and was shown to be as effective as 60 mg of daily oral prednisone for 4 weeks followed by a tapering schedule over 6 months (approximately 40% response rate for both drugs) [van Schaik et al. 2010]. Adverse effects were similar between the groups, but one wonders whether side effects may have increased in the prednisone group with longer exposure [Gorson, 2010].
A retrospective study has suggested that intravenous, high-dose (1 g) methylprednisolone, administered daily for 3–5 days followed by a weekly regimen for 4–8 weeks, and then monthly as dictated by clinical course, was effective in 13 of 16 patients at 6-month follow up [Lopate et al. 2005]. If confirmed in larger, randomized, controlled trials, this approach may provide an effective alternative to daily oral prednisone with fewer adverse effects. In another retrospective study, 10 patients improved when treated in an open-label fashion with 500 mg of oral methylprednisolone weekly for 3 months, followed by a tapering dose that was dependent upon the patient’s clinical status. There was a sustained remission in six patients off therapy at last follow up [Muley et al. 2008].
Most patients observe improvement in strength and sensory symptoms after several weeks of steroid treatment. Maximal improvement occurs after 3–6 months of therapy, and only a minority of patients experience further recovery after 6 months [Wertman et al. 1988; Barohn et al. 1989]. The standard dosage of prednisone is 1.0–1.5 mg/kg/day, administered as a single morning dosage. Those who experience substantial clinical improvement with daily prednisone may reduce the dosage by switching to an alternate day regimen after 2 or 3 months and tapering by 5–10 mg on the alternate day, every 2–4 weeks, as gauged by the patient’s clinical state. If the patient deteriorates, the dosage should be increased to the minimum dose that induces sustained improvement. Anecdotal experience suggests that adding an alternative treatment (PE, IVIg, azathioprine, cyclophosphamide, or cyclosporine A) should be considered in patients who develop adverse effects, relapse repeatedly following reduction of the prednisone dosage, or require more than 35 mg of prednisone every other day.
Prednisone is best suited for younger patients with CIDP who have few other medical illnesses. Long-term prednisone therapy is generally poorly tolerated in the elderly and those who have concurrent medical conditions (e.g. hypertension, diabetes mellitus, obesity, peptic ulcer disease, and osteoporosis). Weight, blood pressure, blood glucose, electrolytes, ophthalmological evaluation, and stool guaiac require regular monitoring. In addition, periodic bone density measurements and a regimen to prevent steroid-induced osteoporosis should be instituted. This may include calcium and vitamin D, and biphosphonates. Contraindications to prednisone therapy include active peptic ulcer disease, poorly controlled diabetes mellitus or hypertension, severe osteoporosis, and systemic fungal infections. The major limitation of prednisone therapy is the large number of potentially serious adverse effects that develop after chronic (usually > 2 months) exposure. Some of the potential complications include: fluid retention, weight gain, insomnia, mood lability, psychosis, hyperglycemia, gastritis, osteoporosis, aseptic necrosis of the femoral or humeral heads, vertebral fractures, steroid myopathy, impaired wound healing, increased susceptibility to infections (herpes zoster, cutaneous fungal infection, reactivation of tuberculosis, recurrent pneumonia), cataracts, glaucoma, hirsutism, cushingoid state, and pseudotumor cerebri.
Plasma exchange
Two short-term randomized, placebo-controlled trials have demonstrated that PE is superior to placebo, with response rates ranging between 33% and 80% [Dyck et al. 1986; Hahn et al. 1996a]. The beneficial effects of plasma exchange in CIDP also have been supported by a Cochrane review [Mehndiratta et al. 2004]. Improvement was observed in the mean Neurologic Disability Score, grip strength, clinical disability grade, and summated mean motor potential amplitudes and conduction velocities that increased after treatment. Patients improved within 4 weeks after initiating therapy, and those with a chronic progressive course responded as well as patients with relapsing disease. Although the short-term efficacy of PE has been convincingly demonstrated, 50–67% of patients have deteriorated weeks to months after treatment and have required repeated exchanges or an alternative therapy to maintain improvement [Choudhary and Hughes, 1995]. Long-term outpatient plasma exchange can be used successfully in selected patients if peripheral access can be maintained or after placement of an arteriovenous fistula. Alternatively, combining prednisone or other immunosuppressive agents with PE may induce a prolonged remission [Hahn et al. 1996a]. Those with a short duration of disease and EMG or pathological features of a primary demyelinating neuropathy (without axonal loss) are more likely to respond to PE [Pollard et al. 1983; Hahn et al. 1996a]. Dyck and coworkers have established that the short-term (6 weeks) efficacy of plasma exchange is similar to IVIg [Dyck et al. 1994]. The beneficial effect of PE presumably results from the removal of pathogenic humoral factors, such as circulating immunoglobulins, auto-antibodies, pro-inflammatory cytokines or complement. A single exchange removes 3–5 liters of plasma and reduces intravascular IgG by approximately 45%, such that three to five exchanges are required to remove approximately 90% of circulating IgG. The exchanged plasma is replaced with 5% albumin and saline, sometimes supplemented with calcium, and with acid-citrate dextrose or heparin.
Although no specific guidelines have been established for the frequency or schedule of treatment, the frequency of PE can be guided by the duration of a clinical response. For example, those with severe disability (e.g. nonambulatory) generally are treated with five exchanges (each exchange 250 ml/kg) performed over a period of 7–10 days. Improvement usually occurs within several weeks followed by a stable phase of weeks to months; exchanges may be repeated periodically in a similar fashion as necessary to maintain improvement. The addition of prednisone or other immunosuppressive agents (azathioprine or cyclosporine A) may sustain longer periods of remission and reduce the frequency of exchanges. Those who have mild or moderate disability and remain ambulatory may benefit from two or three exchanges/week over a period of 2–3 weeks, followed by once or twice weekly exchanges for an additional 3 weeks. PE may be used safely as a long-term therapy (years) in patients with a chronic relapsing course who do not respond or develop adverse effects with other treatment modalities [Choudhary and Hughes, 1995]. PE may be an especially appealing therapy for patients who have contraindications to other treatments, such as prednisone for patients with diabetes mellitus and IVIg for those with pre-existing renal insufficiency.
Patients with poor peripheral venous access may require placement of a central venous catheter with the associated risk of pneumothorax, catheter site infection, and venous thrombosis. The placement of a permanent central venous catheter facilitates frequent exchanges in those patients who have poor peripheral venous access. Intravenous saline (0.5–1.0 liter) administered several hours before an exchange reduces the risk of hypotension and vasovagal symptoms. PE is generally well tolerated and safe, but it is invasive and time consuming and requires special equipment and well-trained personnel in medical facilities familiar with the procedure. There are relatively few contraindications to PE, and include coagulopathy, thrombocytopenia, and hypotension. Complications of PE are: hypotension, cardiac arrhythmia, vasovagal reaction, citrate toxicity with nausea and vomiting, electrolyte imbalance (citrate-induced hypocalcemia), allergic reactions to infused plasma or plasma substitutes, anemia, thrombocytopenia, muscle cramps, paresthesias, and infection, bleeding, venous thrombosis and pneumothorax as a complication of central catheters for venous access.
Intravenous IVIg
IVIg has been introduced as the main therapy for CIDP over the last two decades. Multiple well-controlled studies have demonstrated that approximately 50–70% of patients respond to IVIg [Hahn et al. 1996b; Mendell et al. 2001; Hughes et al. 2008]. Improvement occurs within a few weeks, and rarely recovery may be dramatic, appearing 1 or 2 days after completing the infusion. Usually the benefit is transient (1–6 weeks) with 50% of patients relapsing within weeks to months and subsequently requiring regular infusions to maintain maximum improvement. Patients with a progressive course or predominantly sensory deficits with tremor may be less likely to improve. Mendell and coworkers showed that 11 of 29 treatment-naïve patients with CIDP improved by one or more disability grades after receiving IVIg, 1.0 g/kg/day at baseline and after 3 weeks, compared with two of 21 patients who received placebo; 76% of IVIg-treated patients had improved strength [Mendell et al. 2001]. Improvement was noted as early as 10 days after therapy.
The recently published IVIg in CIDP Efficacy (ICE) trial was the largest and longest randomized, double-blind placebo-controlled trial demonstrating sustained efficacy of IVIg in CIDP utilizing a loading dose of 2 g/kg administered over 2–5 days, followed by repeated infusions of 1 g/kg administered every 3 weeks for 6 months [Hughes et al. 2008]. There were 117 CIDP patients enrolled in the trial who were randomized to IVIg or placebo and treated for 6 months, followed by re-randomization to an open phase of treatment for an additional 6 months follow up. This study showed 54% of treated patients responded with substantial improvement in measures of strength, functional disability, and quality of life compared with placebo-treated patients. Importantly, approximately half of those randomized to placebo in the open phase after having received IVIg in the blinded phase maintained their clinical response (i.e. approximately 50% of patients maintained their improvement off IVIg for 6 months), suggesting that some IVIg responders may be over treated with continued long-term therapy. IVIg responders were defined as having a two or more point improvement in the INCAT disability score, and the majority of such patients could be identified after 2 cycles of treatment [Latov et al. 2010]. Therefore, it seems reasonable to offer patients with CIDP three cycles of IVIg every 3 weeks, and if there is no meaningful clinical response, consider an alternative first line treatment (corticosteroids or plasma exchange). With the data from the ICE trial and other positive IVIg treatment trials, there is Level I evidence for the efficacy of IVIg in CIDP. Because it has a low frequency of adverse effects and is easy to administer, most experts believe IVIg has been established as the standard of care and should be the initial treatment of choice for patients with CIDP [Joint Task Force of the EFNS and PNS, 2010]. IVIg (Gamunex) has an FDA indication for this condition.
As with PE, anecdotal reports suggest that combining IVIg with prednisone or other immunosuppressive medications may further augment the duration of remission and reduce the frequency of IVIg infusions [Hahn et al. 1996b]. Most treatment trials in CIDP now incorporate IVIg therapy as standard of care treatment in the trial design when assessing the efficacy of other agents [RMC Trial Group 2009; Hughes et al. 2010].
The standard IVIg dosage is a loading dose of 2.0 gm/kg administered intravenously over 2–5 days, followed by 1 g/kg over 1 day every 3 weeks. Those who initially respond and then relapse after discontinuation of treatment likely will require long-term IVIg therapy. In practice, the addition of an oral immunosuppressant can be offered in an attempt to decrease the frequency of IVIg administration. Once the patient has stabilized, most tolerate IVIg dosage reduction or an increase of the treatment interval and still maintain clinical stability. Not surprisingly, the presence of axon loss (demonstrated clinically by prominent muscle atrophy or electrophysiologically by low or absent motor amplitudes) is the major prognostic factor for lack of response to IVIg therapy [Iijima et al. 2005].
A single infusion of IVIg is derived from plasma from approximately 5000 human blood donors. The mechanism of the beneficial effects of IVIg is not precisely known but is thought to be related to modulation of pathogenic autoantibodies [Dalakas, 2011]. Other considerations include suppression of pathogenic cytokines, Fc receptor blockade, reduced complement deposition, increased levels of macrophage stimulating factor and monocyte chemoattractant protein-1, and alteration in pathogenic T-cell function [Creange et al. 2003; Köller et al. 2005; Dalakas, 2011].
IVIg may be administered by rapid infusion (1.0 g/kg/day over 4–6 hours, for 2 days) in younger patients and is generally well tolerated [Grillo et al. 2001]. The drug should be given at a slower rate to the elderly or those with vascular disease, cardiac or renal insufficiency. Headache, fluid overload and flu-like symptoms are more likely to occur at higher infusion rates. Pretreatment with 60 mg of intravenous methylprednisolone may reduce the severity of headaches in headache-prone patients. The first treatment should be monitored in a supervised setting (hospital, office, or outpatient clinic), and if well tolerated, subsequent infusions may be provided safely in the home. An IgA level and renal function studies should be checked before the first IVIg administration. Elderly patients with borderline renal function are at especially high risk for renal failure.
There does not appear to be a significant difference regarding the efficacy of various brands of IVIg [Kuitwaard et al. 2010], however, in practice side effects may be more problematic with a particular brand of immunoglobulin in some patients; if a patient develops intolerable side effects from a specific formulation of IVIg (e.g. severe headache, rash, serum sickness reaction), it is advisable to change to an alternative brand and observe if efficacy can be maintained without adverse effects. For those patients who develop intolerable side effects to several brands of IVIg (usually headache), immunoglobulin may be administered subcutaneously (SCIg). Data are limited to open-label case reports but suggest this is a viable option to administer the drug with similar efficacy to IVIg and allowing greater patient autonomy with self-administered home infusion therapy [Cocito et al. 2011b]. A randomized, placebo-controlled trial to assess the efficacy of SCIg has been initiated in patients with CIDP who are dependent upon IVIg.
IVIg is contraindicated in patients with absolute IgA deficiency or a history of a previous allergic reaction following exposure to human immune globulin. Minor side effects are common and include headache, malaise, fatigue, and fever. Other adverse effects include: aseptic meningitis, rigors, myalgias, flushing, fluid overload with edema or congestive heart failure, renal insufficiency (presumably due to hyperosmolarity), hemolysis, transient neutropenia, back, chest, leg or abdominal pain, and eczematous rash. Rarely, IVIg induces a hyperviscosity syndrome with increased risk for deep venous thrombosis, myocardial ischemia, or stroke. Anaphylactic reactions may occur in IgA-deficient patients due to anti-IgA antibodies. Revised manufacturing processes have largely eliminated the risk of viral transmission.
Alternative immunosuppressive regimens
The indications for considering alternative immunosuppressive agents for patients with CIDP are: (1) the patient has not improved with sequential or combined trials of the above outlined conventional therapies that have demonstrated efficacy in randomized, controlled trials; (2) the patient has improved with these treatments but has frequent relapses, usually with attempts at weaning the medication, making continued therapy cumbersome, time-consuming, and costly; or (3) the patient has developed intolerable adverse effects with the proven therapies. The usual approach to using these medications would be in a situation where the patient has failed to remain in remission after discontinuing the proven therapies, and the goal is to stabilize the patient with an ‘add-on’ immunosuppressant, maximizing the appropriate dosage and duration of therapy before another attempt at weaning the first-line therapy; this has been classically used as a ‘steroid-sparing’ strategy but also can be used with attempts to wean IVIg or plasma exchange. It is critical to use these alternative drugs for long enough (for example, azathioprine for at least 12–18 months) before concluding the second-line drug has been ineffective and moving on to alternative second-line medication trials. Most of the agents reviewed below have been reported to be effective in some patients with CIDP in single case reports, open-label case series, and retrospective reviews, but few have been submitted to rigorous clinical trials that establish efficacy. In other cases, some of these agents (e.g. azathioprine, methotrexate, interferon B1a) have been carefully studied in larger controlled trials and were proven ineffective. There are several explanations why these drug trials were negative, including lack of appropriate duration of treatment (e.g. for azathioprine, the endpoint of the trial was only 9 months); complex trial design (e.g. in the methotrexate trial, patients were on varying tapering doses of IVIg or prednisone); lack of adequate power due to small sample size (azathioprine, interferon B1a trials) to detect a significant response; and a surprisingly high placebo response in patients assigned to the placebo arm of several studies (up to 44% in the methotrexate and interferon B1a trials), suggesting many patients randomized to placebo may have had inactive disease and therefore did not relapse as anticipated when IVIg was discontinued. The last, and perhaps most important conclusion, is that these agents simply may not be effective treatments for CIDP. Accordingly, it is prudent to advise the patient that these agents are not likely to be more effective than proven treatments and to maintain realistic expectations about recovery; this is particularly relevant for patients with a prolonged disease course and concomitant severe axon loss in whom the neurological deficit may be irreversible. In those individuals, a reasonable expectation would be to stabilize the condition and halt further progression.
Azathioprine
Although anecdotal reports have indicated that azathioprine is an effective therapy for CIDP [McCombe et al. 1987; Barohn et al. 1989], one randomized study of only 9 months duration showed that the degree of improvement with azathioprine combined with prednisone was similar to prednisone alone [Dyck et al. 1985]. However, the immunosuppressive effects of this agent may not occur for over 1 year, as previously noted, and therefore the duration of this trial was too short to exclude benefit. Others have found that azathioprine is helpful in some patients not only for stabilizing the disease course but, more importantly, for allowing reduction of prednisone dosage. Therefore, azathioprine is used ideally as adjunctive therapy for CIDP as a steroid-sparing agent. The usual dosage is 2.0–3.0 mg/kg/day administered orally as a single daily dose. A test dose of 50 mg/day may be given for the first week. If this is tolerated, the dose is gradually increased by 50 mg every few days. A compete blood count and liver enzymes should be monitored monthly for 6 months, and then every 3 months thereafter. An acute hypersensitivity reaction may occur in the first several days to weeks of therapy characterized by severe nausea and vomiting, diarrhea, fever, malaise and myalgias, rash, elevation in liver enzymes, and pancreatitis; these adverse effects are reversible upon discontinuation of the drug.
Cyclosporine A
Patients with treatment refractory CIDP may improve with cyclosporine A. Although published experience with cyclosporine A is restricted to several small case series, response rates ranged from 40–90%. Patients improved within 2–3 months of initiating treatment, and several discontinued prednisone without clinical deterioration [Barnett et al. 1998; Odaka et al. 2005]. The starting dosage is 5.0 mg/kg/day orally, in two divided dosages 12 hours apart; dose adjustments are made by following target blood levels. Once the patient has stabilized, the dosage should be titrated to the lowest dose required to maintain improvement. Cyclosporine A is contraindicated in patients with systemic infection, history of previous hypersensitivity reaction, abnormal renal function, uncontrolled hypertension, and malignancy. Blood pressure, renal and liver function (including creatinine clearance), serum lipids, magnesium and potassium require regular monitoring. Checking trough serum cyclosporine levels may minimize toxicity. A trough level should be maintained between 100 and 400 ng/ml. The main side effects of cyclosporine A are renal insufficiency, hypertension, hirsutism, tremor, gingival hyperplasia, increased risk of opportunistic infection, sepsis, nausea, vomiting, hepatotoxicity, seizures (possibly related to hypomagnesemia), headache, and cramps.
Cyclophosphamide
Oral cyclophosphamide also has been reported to be beneficial when administered for several months as monotherapy or in combination with prednisone [Good et al. 1998] Uncontrolled case series suggest monthly, pulse intravenous cyclophosphamide is effective when combined with prednisone or administered after cycles of PE [Fowler et al. 1979; Good et al. 1998; Dalakas, 2011]. Good and coworkers reported that 12 of 15 CIDP patients who were refractory to plasma exchange, IVIg or steroids improved with monthly intravenous pulse cyclophosphamide (1 g/m2); the average time to sustained improvement was 8.5 months [Good et al. 1998]. Complications included nausea, headache, rash, and anticipated leukopenia. No patient developed severe bone marrow suppression or malignancy with an average follow up of 3 years. Other reports have highlighted a treatment response following high-dose cyclophosphamide (200 mg/kg daily for 4 days) as myelo-ablative chemotherapy with or without autologous stem cell rescue [Brannagan et al. 2002]. The toxicity of these latter approaches requires that they be offered only within experimental study protocols.
Cyclophosphamide generally is reserved for patients with CIDP who fail conventional immunotherapy and is most often administered in conjunction with prednisone, IVIg or PE. The drug may be given orally as a single daily dose or as pulse intravenous therapy on a monthly basis. The response rate has been reported to be as high as 80%, however experience is restricted to retrospective case series. Leukopenia is a common adverse effect and a complete blood count with differential count, platelet count, and urinalysis should be checked 2 weeks after intravenous administration and every 2–4 weeks in patients taking oral cyclophosphamide. With intravenous therapy, the dosage should be adjusted by 25% increments to produce a transient reduction of the white blood cell count to 2.0–3.0 K/µl. Significant nausea can be avoided by administering ondansetron hydrochloride (8 mg p.o., b.i.d.) or other anti-emetics, and at least 3 liters of intravenous fluid should be given to reduce the risk or hemorrhagic cystitis. The standard oral dosage is 2.0 mg/kg/day; when administered intravenously, the typical dose is 1.0 g/m2 administered monthly for 6–12 months. The main side effects are dose-dependent bone marrow suppression, reduced resistance to infection, hemorrhagic cystitis, infertility, teratogenic effects, amenorrhea, nausea, vomiting, anorexia, alopecia, and malaise. Clinicians should be aware of the increased risk of malignancies, especially lymphoma and leukemia, in patients exposed to long-term or high-dose cyclophosphamide therapy. A history of previous bone marrow suppression or myelodysplastic syndrome is a contraindication to treatment with cyclophosphamide.
Interferons
Interferons have complex immunomodulating effects and may influence the levels of pro-inflammatory cytokines, especially tumor necrosis factor (TNF) alpha, interleukin-2, and interferon gamma, which have been demonstrated to have a role in the development of inflammatory demyelination. Several case reports and one prospective, pilot study indicated that interferon alpha 2a was effective in patients with CIDP who were refractory to conventional immunomodulating agents [Gorson et al. 1998]. No randomized, controlled trials with this agent have been conducted. Similarly, initial reports indicated that interferon beta-1a was effective in several patients with CIDP who did not improve after trials of prednisone, plasma exchange, cyclosporine A, IVIg, and azathioprine [Choudhary et al. 1995]. A prospective, multicenter, open-label trial of interferon B1a (30 µg IM weekly) for 6 months in 20 patients with CIDP showed significant improvement in the neurological disability score and clinical grading scale compared with baseline measures [Vallat et al. 2003]. However, a prospective, randomized, double-blind, placebo-controlled trial of interferon B1a (30 or 60 µg twice weekly for 4 months) in 67 IVIg-dependent CIDP patients did not show clinical improvement or reduced IVIg dosing in treated patients compared with placebo. Post hoc analysis indicated that a subset of more severely affected patients who required higher doses of IVIg at baseline did improve. Furthermore, the conclusions regarding lack of efficacy of interferon B1a cannot be considered definitive as the study was underpowered due to poor patient recruitment, and there was a surprisingly high rate (40%) of placebo responders [Hughes et al. 2010]. The usual dosage of interferon alpha 2a is 3 million IU, subcutaneously 3 times/week, and for interferon-beta 1a, 30 µg intramuscularly once per week. Common side effects include influenza-like symptoms (fever, chills, sweating, and myalgias), headache, fatigue, dizziness, nausea and vomiting, diarrhea, anorexia, abdominal pain, depression, irritability, and injection site reaction.
Mycophenolate mofetil
Mycophenolate mofetil (MM) is an immunosuppressant that has been used successfully for treatment of acute rejection after renal transplantation, and holds promise for the treatment of immune-mediated neuromuscular diseases [Sievers et al. 1997]. MM is an inhibitor of the de novo pathway of purine nucleotide synthesis, thereby blocking the proliferation of B- and T-cell lymphocytes [Sievers et al. 1997]. MM produces immunosuppression that is comparable to azathioprine without causing major bone marrow suppression. Several groups have reported improved strength and successful corticosteroid dosage reduction following therapy with MM [Gorson et al. 2004; Bedi et al. 2010]. The onset of improvement occurred within 3–4 months. Larger, randomized, controlled trials may further clarify the role of this agent in CIDP. The drug is appealing because it is easy to use, well tolerated, and has few long-term adverse effects.
MM has been administered in combination with cyclosporine A and prednisone. The efficacy and safety of MM in combination with other immunosuppressants has not been determined. This agent should not be used in pregnant women because of its teratogenic effect in animals. The standard dosage is 1.0 g administered twice per day, similar to the dosage that is recommended for renal transplant patients. Patients should be monitored for neutropenia with complete blood counts monthly for 6 months, then every 3 months thereafter. There are no contraindications to the use of MM. Potential side effects include nausea, headache, tremor, susceptibility to infection, leukopenia, and possibly an increased risk of developing lymphoma and other malignancies.
Methotrexate
Methotrexate has been a safe and effective agent for patients with inflammatory myopathies and other connective tissue disorders and has been used as a steroid-sparing drug for decades. Open label series have suggested a beneficial role in CIDP [Díaz-Manera et al. 2009]. However, a randomized, double-blind, placebo-controlled trial of escalating doses of methotrexate in steroid- or IVIg-treated CIDP patients showed no benefit over placebo [RMC Trial Group 2009]. However, the trial design was complicated, the placebo response was 44%, and the maximum dose of methotrexate (15 mg/week) was low. Therefore, the role of this agent as a steroid- or IVIg-sparing agent in patients with CIDP still remains uncertain.
Etanercept
Etanercept is a TNF alpha inhibitor approved for use in patients with rheumatoid arthritis. There is one report of three of 10 patients with CIDP who improved after 4–6 months of therapy [Chin et al. 2003]. The treatment was administered as a subcutaneous injection of 25 mg twice per week and was well tolerated. The authors suggested this novel therapy for CIDP warrants further study in a randomized, controlled trial. Conversely, several patients have been reported to develop a condition indistinguishable from CIDP after treatment with similar TNF inhibitors [Alshekhlee et al. 2010], and thus the role of this class of drugs in the treatment of CIDP remains unclear.
Rituximab
Rituximab is a chimeric monoclonal antibody that targets the CD20 antigen on B-lymphocytes. Depletion of B-lymphocytes may interfere with antibody-dependent, cell-mediated cytotoxicity involving peripheral nerve [Perosa et al. 2005]. Investigators reported that six of 13 treatment-refractory patients with CIDP responded to ritxuximab in an open-label, unblinded fashion [Benedetti et al. 2011]. Another retrospective open-label review from a nationwide CIDP patient registry suggested rituximab was beneficial in some patients [Cocito et al. 2011a]. The drug has also been reported to be effective in single cases of patients with CIDP and coexistent autoimmune diseases such as myasthenia gravis with Morvan syndrome [Sadnicka et al. 2011], CIDP with diabetes [Münch et al. 2007], Evans syndrome [Knecht et al. 2004], and idiopathic thrombocytopenic purpura [Benedetti et al. 2008]. Other investigators found rituximab was not helpful in weaning patients from IVIg in an open-label pilot study [Gorson et al. 2007]. The drug is generally well tolerated but currently is considered experimental pending confirmatory trials.
Alemtuzumab
Alemtuzumab is a humanized monoclonal antibody directed against the CD52 antigen, an epitope located on the surface membrane of all lymphocytes and monocytes. The drug causes significant, rapid and prolonged depletion of CD4 and CD8 T-cells and B-cells after a single infusion and has been shown to be effective in multiple sclerosis [Minagar et al. 2010]. There is one case series of seven treatment refractory, IVIg-dependent, CIDP patients treated with one or two infusions of alemtuzumab; two had a prolonged remission and two had a partial response allowing for reduction of IVIg dose and frequency of infusions [Marsh et al. 2010]. Three developed complications from acquired autoimmune diseases, one of whom died. Another prospective open-label pilot study is planned, but the use of the drug is limited by a higher risk of side effects, specifically autoimmune thyroiditis and idiopathic thrombocytopenic purpura. The drug should be considered an experimental therapy for CIDP.
Other immunosuppressant approaches
There was one report of efficacy of total lymphoid irradiation (TLI) in treatment refractory CIDP dating back over 25 years [Rosenberg et al. 1985]. This study has never been replicated and because of the potential toxicity and availability of safer and effective therapies, TLI has been discarded as a therapy by most experts in the field. There has been one case report of efficacy with tacrolimus [Ahlmen et al. 1998], and one case of clinical worsening after treatment with natalizumab [Wolf et al. 2010].
Hematopoietic stem cell transplantation, with or without pretreatment with cyclophosphamide, has been reported to induce sustained remission or even ‘cure’ in patients with treatment refractory CIDP [Axelson et al. 2008; Mahdi-Rogers et al. 2009]. This very aggressive intervention has been associated with significant complications related to immunosuppression, such as pneumonia and sepsis [Mahdi-Rogers et al. 2009]. Owing to the associated risks, this treatment only should be considered in patients who have severe disabling CIDP refractory to sequential trials of multiple less-toxic therapies listed above, performed at medical centers skilled in the procedure and management of potential complications, and ideally under the auspices of an institution approved study protocol.
Supportive therapies
Patients certainly may benefit from walking sticks, walkers, ankle–foot orthotics and other rehabilitation devices and strategies to assist ambulation and other activities of daily living. Physical and occupational therapy may be helpful to maintain range of motion, prevent joint contractures in paretic limbs, and assist in gait retraining. A moderate exercise regimen may help reduce physical fatigue and increase endurance. Psychological counseling can be helpful to manage symptoms of depression, anxiety, anger, and frustration associated with chronic disability. Symptomatic medications are available to offer relief of neuropathic and mechanical pain, fatigue, and alleviate depression and anxiety, but none have been studied in a rigorous fashion in patients with CIDP.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The author has received financial compensation for speaking engagements from Grifols Pharmaceuticals.