
Abstract
Background:
The rapid evolution of endoscopic resection techniques for colorectal polyps has created a diverse but fragmented evidence base, making it challenging to determine the technique that optimally balances efficacy and safety.
Objectives:
To comprehensively compare the efficacy and safety of all mainstream colorectal polypectomy techniques.
Design:
A systematic review and Bayesian network meta-analysis (NMA), conducted in accordance with PRISMA-NMA guidelines.
Data sources and methods:
Databases searched included PubMed, Web of Science, Embase, Scopus, Cochrane Library, CNKI, Wanfang Database, and SinoMed. Model convergence was assured (Brooks-Gelman-Rubin diagnostic), and consistency was evaluated via node-splitting analysis. Treatment hierarchies for primary efficacy outcomes (R0 resection, En bloc resection, complete resection) and secondary safety outcomes (bleeding, perforation) were established using surface under the cumulative ranking curve (SUCRA) probabilities.
Results:
100 RCTs (24,786 patients; 34,244 polyps) comparing 13 techniques were included. Underwater endoscopic mucosal resection (U-EMR) and EMR ranked highest for R0 resection (SUCRA: U-EMR 49%, EMR 30%) and En bloc resection. For complete resection, endoscopic submucosal dissection (ESD) ranked highest (SUCRA: ESD 49%). Cold forceps polypectomy (CFP) and cold snare polypectomy with submucosal injection (CSP-SI) were consistently the least effective across efficacy outcomes. Hot snare EMR (HS-EMR) was associated with the highest risk of bleeding, while cold snare polypectomy (CSP)-based techniques were generally safer for perforation. ESD demonstrated a favorable safety profile for bleeding. The evidence certainty was generally low to moderate.
Conclusion:
This NMA provides a comprehensive hierarchy of polypectomy techniques. U-EMR and EMR are among the most effective for R0 and En bloc resection, while CSP-based techniques are among the safest. HS-EMR carries a higher bleeding risk. These findings provide crucial evidence to guide clinical decision-making and future guideline development, while also highlighting key evidence gaps requiring further research.
Trial registration:
PROSPERO (CRD420251139746).
Keywords
Introduction
Colorectal cancer (CRC) ranks as the third most prevalent malignancy globally. 1 Endoscopic polypectomy is the cornerstone for its primary prevention, where the efficacy of resection techniques-measured by complete resection, low recurrence, and minimal complications-directly influences preventive outcomes and long-term patient prognosis. 2 With the widespread implementation of screening programs, polyp detection rates continue to rise. Consequently, efficient, safe, and standardized resection techniques are essential for achieving the ultimate goal of cancer prevention. 3
Endoscopic technology has undergone substantial development in recent years, available techniques now include basic modalities (cold/hot biopsy forceps, cold/hot snare polypectomy), conventional endoscopic mucosal resection (EMR), and emerging approaches such as underwater EMR (U-EMR), cold EMR (cEMR), and endoscopic full-thickness resection (EFTR). 4 This rapid evolution has significantly expanded therapeutic options, however, has not simplified clinical decision-making but instead introduced considerable complexity due to a fragmented and inconsistent evidence base. Critical questions remain unresolved: what is the comparative efficacy and safety profile of cold (CSP) versus hot snare polypectomy (HSP)? When should resection escalate to EMR or endoscopic submucosal dissection (ESD)? These uncertainties are compounded by three interrelated deficiencies in the current evidence: (1) a lack of direct head-to-head trials for most clinically relevant technique pairings (e.g., a notable gap exists between EMR and ESD5,6); (2) existing comparative studies are often limited in scope—for instance, comparisons between cold and hot EMR are frequently restricted to specific lesions like large serrated polyps,7,8 and analyses of CSP versus EMR often focus only on technical variations;9–11 and (3) inconsistent nomenclature across studies, which hinders reliable synthesis. Conventional meta-analytic methods, dependent solely on direct pairwise evidence, remain insufficient to address these cross-modal evidence gaps.
To address these limitations, this study employed a systematic review and network meta-analysis (NMA) methodology to compare the efficacy and safety of all mainstream colorectal polypectomy techniques. 12 The research strictly adhered to PRISMA-NMA guidelines and was registered on PROSPERO (ID: CRD420251139746). Primary efficacy outcomes are complete resection rate, En bloc resection rate and R0 rate; secondary safety outcomes include bleeding rate and perforation rate. The interventions compared across the studies encompassed 13 techniques: CSP, Underwater Cold Snare Polypectomy (U-CSP), HSP, Cold Forceps Polypectomy (CFP), CSP with Submucosal Injection (CSP-SI), EMR, U-EMR, Hot Snare EMR (HS-EMR), ESD, Trans-anal ESD (T-ESD), Trans-anal Endoscopic Microsurgery (TEM), jumbo forceps polypectomy (JFP) and Hybrid ESD (HFP). This study provides three principal contributions: First, it delivers the first comprehensive, high-level evidence comparing all mainstream techniques, clarifying their relative efficacy-safety profiles to inform individualized clinical practice. Second, it offers pivotal evidence to guide updates of international guidelines. Third, it identifies key deficiencies in the current evidence landscape-such as technique pairings lacking direct comparisons or yielding low-certainty evidence-to prioritize future research. By synthesizing fragmented data, this analysis aims to establish a robust evidence base for optimizing polypectomy practice and ultimately, CRC prevention.
Methods
This systematic review and NMA is registered (CRD420251139746) on the International Prospective Register of Systematic Review (PROSPERO). We followed the PRISMA-NMA checklist statement for NMA (Supplemental Appendix A).
Data sources and search strategy
A systematic literature search was conducted across multiple electronic bibliographic databases from inception until 13 June, 2025 to identify all relevant randomized controlled trials (RCTs). Databases searched included PubMed, Web of Science, Embase, Scopus, Cochrane Library, CNKI, Wanfang Database, and SinoMed. The search strategy employed a comprehensive set of terms structured around three core concepts: (1) colorectal polyps, (2) polypectomy techniques, and (3) study design. Database-specific filters for excluding animal studies were all applied in the search strategy. Language restrictions were applied to English and Chinese during the initial search. The complete search strategies for all databases are provided in Supplemental Appendix B.
Study selection
Records were imported into EndNote Web v.20 for deduplication. Two independent reviewers (Li and Lei) screened titles/abstracts via Rayyan, a systematic review management platform, with full-text review for ambiguous cases. 13 Discrepancies were resolved by a third reviewer (Deng).
Inclusion criteria
Population: Adult patients with endoscopically or histologically confirmed colorectal polyps; Interventions & Comparisons: Direct comparison of two or more endoscopic resection techniques (e.g., cold vs. hot snare, conventional vs. underwater EMR, EMR vs ESD); Outcomes: Reported at least one of the pre-specified efficacy or safety outcomes; Study Design: RCTs.
Exclusion criteria
Studies were excluded if they: (1) focused solely on polyposis syndromes or invasive carcinoma; (2) had a non-comparative design (e.g., case series); (3) were abstracts without available full text; or (4) lacked essential data on polyp characteristics or outcomes.
Primary and secondary outcomes
Primary (Efficacy) Outcomes: R0 resection rate, En bloc resection rate, and complete resection rate.
Secondary (Safety) Outcomes: Major bleeding rate (intraprocedural or delayed requiring intervention) and perforation rate.
Detailed eligibility criteria, including specific definitions of techniques and outcomes, are provided in Supplemental Appendix C.
Data extraction
Extracted information was categorized into: study characteristics (e.g., author, year, country); population and polyp details (e.g., sample size, demographics, polyp features); the specific interventions compared; outcome data for all pre-specified efficacy and safety metrics; and other relevant parameters such as procedure time and recurrence. The complete data extraction schema with all itemized variables is available in Supplemental Appendix E.
Evaluating the quality of the studies
Two independent reviewers (Li and Lei) assessed the risk of bias for each study using the revised Cochrane Risk of Bias Tool (RoB 2.0). 14 This evaluation systematically examined five critical domains: (1) bias arising from the randomization process, (2) bias due to deviations from intended interventions, (3) bias due to missing outcome data, (4) bias in outcome measurement, and (5) bias in selective reporting. Each domain was judged as “low risk,” “some concerns,” or “high risk,” with disagreements resolved through consensus discussion or adjudication by a third reviewer (Deng). Plots visualizing the judgments were applied using the robvis tool. Subsequently, the overall confidence in evidence for NMA outcomes was appraised using the GRADE framework. This assessment evaluated key domains including risk of bias, inconsistency, indirectness, imprecision, and publication bias. 15 The evidence quality for each outcome was categorized into four hierarchical levels (high, moderate, low, or very low confidence), with findings synthesized in evidence profile tables to facilitate transparent interpretation of results.
Statistical analysis methods
Data synthesis was performed at two levels: direct pairwise meta-analysis and Bayesian NMA. All models adopted a random-effects framework. First, for each direct comparison between two techniques, we calculated pooled risk ratios (RRs) with 95% confidence intervals (CIs). Heterogeneity was assessed using the I² statistic. Where substantial heterogeneity (I² > 50%) was observed in a comparison with sufficient data (typically ⩾6 studies), meta-regression was performed to explore predefined covariates. We performed a NMA within a Bayesian framework to evaluate the relative efficacy and safety of different polypectomy techniques, which integrates direct and indirect evidence to estimate relative effects across all 13 interventions simultaneously. 16 The parameters of the model were estimated using Markov Chain Monte Carlo (MCMC) simulation. A consistency model was fitted to integrate direct and indirect evidence, using a binomial likelihood and a logit link function for binary outcomes. Treatments were ranked for each outcome using the surface under the cumulative ranking curve (SUCRA), where a higher value indicates a more favorable rank.17,18 We assessed model convergence and the statistical assumption of evidence consistency. Pre-specified sensitivity analyses examined the robustness of findings, particularly regarding sparsely connected interventions. For outcomes with an adequate number of studies, potential publication bias was evaluated. Detailed specifications of the Bayesian model, including all computational parameters, diagnostic criteria, and software code, are provided in the Supplemental Appendix D.
Results
Study selection
The initial literature search identified 1756 records. After removing duplicates and screening titles and abstracts, 151 full-text articles were assessed for eligibility. Finally, 100 studies comprising 24, 786 patients were included in this NMA. The study selection process is detailed in the PRISMA flow diagram (Figure 1).

PRISMA flow diagram.
Study characteristics
100 RCTs published between 2011 and 2025 were included (total N = 24,786 patients; total polyps resected = 34,244). Studies originated from 21 different countries, predominantly China (n = 29), Japan (n = 22), the United States (n = 12) and South Korea (n = 12). The sample-size weighted mean age was 63.0 years, with a male predominance (median proportion 60%). Polyp sizes ranged from diminutive (⩽1 mm) to large (⩾20 mm), and 58 studies focused on sub-centimeter (⩽10 mm) lesions. The interventions compared encompassed all 13 predefined techniques. The NMA was conducted for five endpoints: R0 resection, En bloc resection, complete resection (efficacy), and pooled major bleeding and perforation (safety). Detailed study characteristics are summarized in Supplemental Appendix E.
Primary outcomes: Efficacy of resection
R0 resection
Seven treatment options (CSP, HSP, U-CSP, EMR, U-EMR, CFP, and CSP-SI.) were analyzed for R0 resection (Figure 2(a)). The SUCRA and cumulative probability plots showed a clear hierarchy among the evaluated interventions. U-EMR demonstrated the highest SUCRA value (0.858), followed by U-CSP (0.730) and EMR (0.655), suggesting that these three modalities had the greatest likelihood of yielding optimal R0 resection outcomes. HSP was associated with the lowest SUCRA value (0.188) and displayed minimal cumulative probability of achieving a favorable rank (Figure 3(a), Supplemental Appendix H).

Network plots of eligible comparisons. (a) R0 Resection; (b) En Bloc Resection; (c) Complete Resection; (d) Bleeding; (e) Perforation.
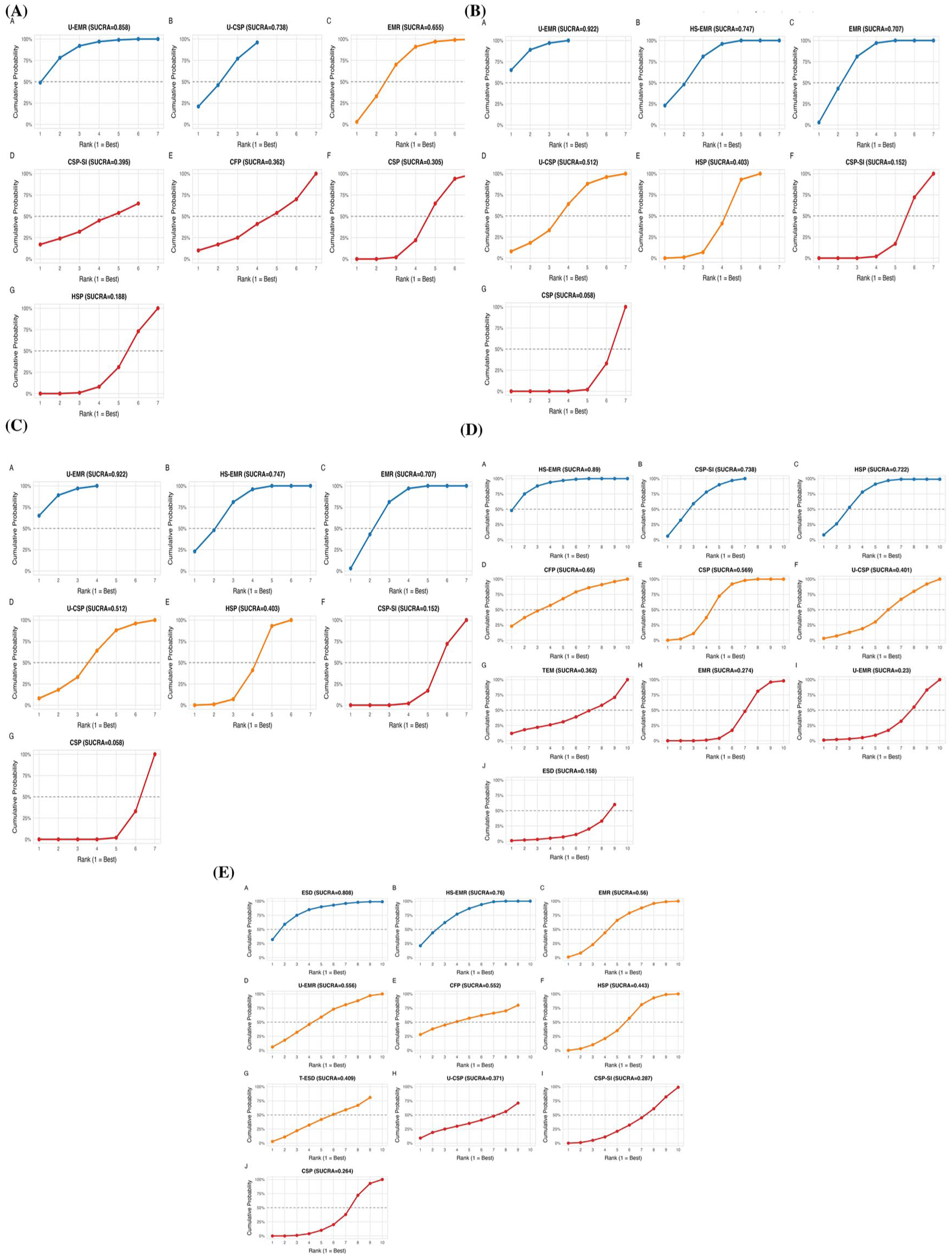
Ranking of endoscopic resection techniques based on the SUCRA for all efficacy and safety outcomes. (a) R0 resection, (b) En bloc resection, (c) Complete resection, (d) Major bleeding, and (e) Perforation. The SUCRA value (ranging from 0 to 1.0) represents the percentage of efficacy a treatment achieves relative to an imaginary ideal treatment. A higher SUCRA value indicates a better ranking. Blue curve (SUCRA >0.7) indicates a high likelihood of being among the best treatments; orange curve (SUCRA 0.4–0.7) indicates a moderate ranking; red curve (SUCRA <0.4) indicates a low likelihood of being superior.
Key comparisons supporting this hierarchy showed U-CSP was superior to both conventional CSP (RR = 3.15, 95% CI: 1.18–8.70) and HSP (RR = 4.01, 95% CI: 1.19–13.42). EMR was also more effective than HSP (RR = 3.59, 95% CI: 1.06–13.60). No significant difference was observed between the top-ranked U-EMR and EMR (RR = 1.61, 95% CI: 0.69–3.79) (Figure 4). The network showed good consistency (all node-splitting p > 0.05) and convergence (all parameters were close to 1).

Net league table presenting comparative effects for R0 resection.
The most frequent direct comparison, CSP versus HSP, showed no significant difference in R0 resection (RR = 0.97, 95% CI: 0.92–1.03), but with moderate heterogeneity (I² = 63.1%). A meta-regression exploring polyp size, patient sex, and study region did not identify significant sources for this heterogeneity (all p > 0.05), indicating the observed moderate heterogeneity may be due to the limited number of studies or other unmeasured study-level characteristics (Table 1). Complete results are in Supplemental Appendix H.
Meta-regression and subgroup analyses of the log risk ratio (CSP vs HSP).

CSP, cold snare polypectomy; HSP, hot snare polypectomy
En bloc resection
The network of interventions for R0 resection comprised 7 treatments (Figure 2(b), Supplemental Appendix I). SUCRA and cumulative probability analyses identified U-EMR as the most favorable approach (SUCRA = 0.922), followed by HS-EMR (0.747) and EMR (0.707). The corresponding cumulative probability curves for these three techniques displayed pronounced increases at rank 1. Conversely, CSP ranked lowest across all treatments, with a SUCRA value of only 0.058 and negligible cumulative probability of occupying a high rank (Figure 3(b)).
Compared to conventional CSP, both EMR, U-EMR, HS-EMR and HSP demonstrated significantly higher En bloc resection rates. Notably, U-EMR demonstrated superior performance compared to conventional techniques. Specifically, U-EMR showed significantly higher En bloc resection rates versus CSP (RR = 7.18, 95% CI: 2.41–20.95) and HSP (RR = 3.23, 95% CI: 1.02–10.15; Figure 5). Node-splitting analysis indicated good overall consistency (Supplemental Appendix I).

Net league table presenting comparative effects for En bloc resection.
The direct comparison between CSP and HSP showed considerable heterogeneity (I² = 87.8%) and a point estimate favoring HSP, though not statistically significant (RR = 1.97, 95% CI: 0.77–5.03). The meta-regression indicated that the observed moderate heterogeneity was not explained by any of the tested covariates. Node-splitting analysis indicated good overall consistency in the network. Full results are in Supplemental Appendix I.
Complete resection
The network of interventions for R0 resection comprised 7 treatments (CSP, HSP, EMR, JFP, ESD, CFP, and HFP) (Figure 2(c), Supplemental Appendix J). ESD and EMR as the leading strategies, with SUCRA values of 0.842 and 0.848, respectively. While CFP demonstrated the poorest performance, yielding the lowest SUCRA (0.212) (Figure 3(c)).
Supporting the efficacy of EMR, it was significantly superior to CSP (RR = 2.32, 95% CI: 1.19–5.34), CFP (RR = 2.92, 95% CI: 1.19–8.13), and HSP (RR = 2.44, 95% CI: 1.27–5.27). No statistically significant difference was observed between the top-ranked ESD and EMR (RR = 1.09, 95% CI: 0.38–3.32) (Figure 6). The direct comparison of CSP versus HSP for complete resection showed no significant difference (RR = 0.99, 95% CI: 0.97–1.01) and low heterogeneity (Supplemental Appendix J).

Net league table presenting comparative effects for complete resection. Net league table: head-to-head comparisons. Risk ratios (RRs) and 95% confidence intervals (CIs) are reported.
Sensitivity analysis
Sensitivity analysis underscored the extreme instability of TEM ranking. In accordance with our pre-specified plan, TEM was excluded from the primary analysis due to being connected by only one study. When included in a post-hoc sensitivity analysis, it markedly altered the ranking probabilities: TEM was ranked first with a high probability (81%), while the probabilities of ESD and EMR being ranked first dropped substantially from 49% to 11% and from 32% to 2%, respectively. This dramatic shift is based solely on a single direct comparison study (Barendse et al., 2018) connecting TEM to the network. Consequently, the comparative efficacy estimate for TEM is highly uncertain, and the results of this sensitivity analysis should be considered unreliable (Supplemental Appendix J).
Secondary outcomes: Safety profiles
Bleeding
Evidence from 36 RCTs contributed to 15 direct comparisons (Figure 2(d), Supplemental Appendix K). HS-EMR emerged as the worst intervention, with the highest SUCRA value (0.89), indicating a high probability of being ranked first in terms of bleeding events. Conversely, ESD demonstrated the highest safety profile, with a SUCRA value of 0.158 and a nearly flat cumulative curve (Figure 3(d)).
The network league table indicated that HS-EMR carried a significantly higher risk of bleeding compared to conventional EMR (RR = 3.71, 95% CI: 1.25–11.98). Conversely, ESD appeared to have a lower risk than HS-EMR, though with a wide confidence interval (RR = 0.16, 95% CI: 0.03–0.90). Complete safety comparisons are in Supplemental Appendix K.
Perforation
The network of interventions included 11 treatments (CSP, HSP, U-CSP, EMR, U-EMR, CSP-SI, HS-EMR, ESD, TEM, T-ESD, and CFP) (Figure 2(e), Supplemental Appendix L). ESD (SUCRA = 0.808) and HS-EMR (SUCRA = 0.76) had the highest probabilities of being ranked as the worst interventions. In contrast, CSP, CSP-SI, and U-CSP occupied the safest ranks, with SUCRA values of 0.264, 0.287, and 0.371, respectively, indicating minimal likelihood of achieving perforation outcomes (Figure 3(e)).
Comparative analysis showed that HS-EMR carried a significantly higher risk of perforation compared to CSP (RR = 2.67, 95% CI: 1.14–6.44). The point estimate for ESD versus HS-EMR was not statistically significant (RR = 1.18, 95% CI: 0.19–6.89). Similar to the bleeding outcome, the effect estimates for several techniques, notably U-CSP, were accompanied by extremely wide credible intervals, indicating substantial uncertainty. Full results are in Supplemental Appendix L.
Assessment of heterogeneity, convergence, and publication bias
Heterogeneity was high in several direct comparisons, such as CSP versus HSP for En bloc resection (I² = 87.8%). The convergence of all NMA models was confirmed, with all PSRF being close to 1.0. Publication bias was assessed using comparison-adjusted funnel plots and Egger’s linear regression test for all five outcomes. For complete resection outcome, Egger’s test revealed significant small-study effects (p < 0.001). The accompanying funnel plot showed visual asymmetry, with a paucity of studies in the left-bottom quadrant, suggesting the possibility of unpublished small studies with null or negative findings. The funnel plots for other outcomes were visually symmetrical, indicating a low likelihood of substantial publication bias (Figure 7).

Funnel plots for the assessment of potential publication bias.
Risk of bias
The risk of bias for the included studies was assessed using the RoB2 tool. Among the 100 studies, 60 were rated as “Low risk,” 33 raised “Some concerns” primarily related to deviations from missing outcome data, and 7 were judged as “High risk” of bias due to issues such as randomization process, missing outcome data, or deviations from the intended interventions. The overall assessment indicates that the majority of studies were of satisfactory methodological quality, though a notable proportion warranted cautious interpretation (Supplemental Appendix G).
Certainty of evidence (GRADE)
The GRADE assessment across the three networks indicated that the overall certainty of evidence was predominantly low, primarily due to concerns of imprecision and indirectness. For many comparisons, the CIs showed no obvious difference between interventions, leading to downgrading for imprecision. Furthermore, a substantial number of comparisons were based solely on indirect evidence from the network, resulting in downgrading for indirectness. Inconsistency was not a major concern in several direct comparisons where node-splitting analyses confirmed consistency. Study limitations and publication bias were generally not considered robust reasons for downgrading in any of the networks.
Discussion
This NMA provides the first comprehensive, simultaneous ranking of the efficacy and safety of 13 polypectomy techniques, translating fragmented data into a practical evidence hierarchy. The key findings are threefold. First, regarding efficacy, U-EMR consistently emerged as a top-ranking technique for achieving R0 resection and En bloc resection. For the outcome of complete resection, ESD and EMR demonstrated the highest probabilities of success. Second, the safety profile of techniques varied considerably; HS-EMR was associated with the greatest risk of bleeding, while CSP-based techniques were generally ranked among the safest for perforation. These actionable insights are tempered by the predominantly low certainty of evidence, underscoring the need for more robust comparisons. Collectively, this synthesis translates fragmented data into a practical evidence hierarchy to inform clinical practice and prioritize research.
The superior ranking of water-assisted techniques (U-EMR and U-CSP) corroborates and extends the growing evidence base supporting their use.19,20 The mechanism for this advantage is thought to be related to the buoyancy and clearer visual field provided by water immersion, which facilitates resection.21–23 This evidence supports specific clinical upgrades: For non-pedunculated polyps ranging from 4 to 10mm (where CSP is standard) to larger lesions (typically resected by EMR), adopting a water-assisted approach may significantly enhance the quality of resection, potentially reducing recurrence rates. U-CSP, in particular, emerges as a highly effective and likely safe upgrade to conventional CSP for smaller lesions. 20 For larger lesions, EMR and its variants were consistently ranked among the top techniques, reinforcing its established role as the gold standard, as per guidelines. 24 Within this domain, U-EMR emerges as a compelling advanced option, performing comparably in efficacy while our analysis and prior meta-analyses suggest it offers a more favorable safety profile, supporting its preferential consideration when safety is paramount, particularly for higher-risk patients. 25
Our analysis provides a clear, evidence-based contraindication for certain practices. CFP and CSP-SI were ranked lowest for R0 resection. For CFP, this reinforces the imperative to adhere strictly to guideline recommendations: it should be reserved for diminutive (1–3 mm) polyps only, as its use on larger lesions risks incomplete resection.26–28 For CSP-SI, the finding is more actionable: routine submucosal injection for small (3–10 mm) polyps is not only unnecessary but appears detrimental to resection quality and should be avoided. 29 The likely mechanism—fluid obscuring margins—offers a technical rationale for this clinical recommendation.
Clinicians must be aware that the potential for higher efficacy with HS-EMR comes at a cost of significantly greater procedural risk. A paramount safety finding of our analysis is the significantly elevated risk of both bleeding and perforation associated with HS-EMR, providing a clear explanation for the conflicting safety reports in the literature.30,31 This risk is inherent to the use of electrocautery for mucosal resection, where technical factors can lead to deep thermal injury.32,33 Consequently, HS-EMR should be employed with particular caution. Its use should be reserved for scenarios where its potential efficacy advantages are deemed essential, and it should be performed only by experienced endoscopists in settings equipped to manage potential complications.
The profile of ESD emerging from our analysis is that of a high-efficacy, high-precision technique with a distinct and disparate safety profile. It ranked among the top for complete resection and among the safest for bleeding. However, it was also associated with the highest probability of being the worst technique for perforation. This apparent contradiction can be reconciled by considering the procedure’s context: the favorable bleeding profile likely reflects the expert-level, controlled dissection with proactive hemostasis typical of ESD,34,35 while the elevated perforation risk underscores the profound technical complexity and the consequences of inadvertent deep injury. Therefore, ESD represents a specialized tool: it offers superior efficacy for complex lesions where En bloc resection is paramount, but this comes with a traded and specific risk of perforation that must be expertly managed. Its use should be confined to settings with the expertise to navigate this specific risk-benefit equation.
The long-standing debate on the comparative merits of cold versus HSP lacks a definitive, one-size-fits-all answer. Our NMA, consistent with several authoritative large-scale meta-analyses, failed to demonstrate a statistically significant difference in efficacy between the two modalities.36–38 On safety, our integrated analysis (encompassing both immediate and delayed bleeding) also showed no clear superiority of either technique, reflecting a trade-off: HSP carries a known risk of delayed bleeding from thermal injury, whereas CSP is more associated with immediate intraprocedural bleeding.4,27,30 This equilibrium suggests that the choice between CSP and HSP can be individualized. The decision may reasonably be guided by specific lesion characteristics (e.g., size, presence of high-risk stigmata) and, crucially, by the endoscopist’s expertise and confidence in managing the distinct bleeding patterns associated with each technique.
The interpretation and application of our findings must be tempered by several study limitations, many of which reflect gaps in the underlying evidence base. First, the clinical applicability of our results is constrained by the significant heterogeneity in polyp characteristics (size, morphology, histology) and operator expertise across studies. While we performed meta-regression, the statistical power was insufficient to conduct definitive subgroup analyses that could guide technique selection for specific polyp subtypes, which is a critical need in clinical practice. Second, and fundamentally, the nomenclature for polypectomy techniques remains notably inconsistent in the literature. The lack of standardized definitions means that techniques under the same name (e.g., EMR) might have subtle but important variations in execution between studies, while different names might describe essentially the same method. This classification ambiguity introduces a potential source of misclassification bias that our analysis could not fully overcome. Furthermore, our network for some advanced techniques relied heavily on indirect comparisons and sparse data, leading to imprecise estimates and, in the case of techniques like TEM, extreme ranking instability based on single-study connections. Consequently, our results represent a synthesis of the average treatment effects across a heterogeneous landscape of studies, and they highlight an urgent need for both standardized terminology and larger, more granularly designed trials.
Conclusion
This NMA provides the most comprehensive comparative assessment to date of the efficacy and safety of mainstream endoscopic resection techniques for colorectal polyps. The findings demonstrate that U-EMR and conventional EMR are among the most effective techniques for achieving R0 and En bloc resection, while ESD and EMR rank highest for complete resection. CSP-based methods exhibit a favorable safety profile, particularly regarding perforation risk. In contrast, HS-EMR is associated with a significantly higher risk of bleeding. Advanced techniques such as ESD show high efficacy but require further high-quality direct comparisons to robustly establish their relative effectiveness against other modalities. These results offer an evidence-based hierarchy to inform clinical decision-making and guideline development. They highlight the importance of selecting a resection technique that balances efficacy and safety based on polyp characteristics and endoscopist expertise. Furthermore, this synthesis identifies critical evidence gaps-particularly the lack of standardized technique definitions and direct comparisons between advanced resection methods-that should be prioritized in future research to refine endoscopic practice and improve colorectal cancer prevention outcomes.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261436116 – Supplemental material for Efficacy and safety ranking of endoscopic resection techniques for colorectal polyps: a systematic review and network meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848261436116 for Efficacy and safety ranking of endoscopic resection techniques for colorectal polyps: a systematic review and network meta-analysis by Shirui Li, Yue Lei, Yunfan Deng, Sheng Dai, Dehai Xiong, Qi Fan and Xiuyang Li in Therapeutic Advances in Gastroenterology