
Abstract
Background:
Endoscopic placement of fully covered self-expanding metal stents (FCSEMS) is a treatment for distal biliary strictures (DBS). However, there remains a notable gap in the research regarding the efficacy and safety of FCSEMS in benign distal biliary stricture (BDBS) and malignant distal biliary stricture (MDBS).
Objective:
To compare the short-term efficacy and long-term safety of FCSEMS in benign versus malignant DBS.
Design:
A retrospective, single-center cohort study.
Methods:
We conducted a retrospective analysis of 123 patients with DBS who underwent FCSEMS placement via endoscopic retrograde cholangiopancreatography (ERCP) at Shanghai East Hospital Affiliated to Tongji University from January 2019 to December 2024. Patients were stratified into BDBS (n = 46) and MDBS (n = 77) based on comprehensive diagnostic criteria, including medical history (underlying diseases, prior surgeries, etc.), clinical manifestations, laboratory tests (hepatic function panel, tumor biomarkers, IgG4, autoimmune antibodies, etc.), and multimodality imaging (Computed Tomography, magnetic resonance cholangiopancreatography, endoscopic ultrasound, etc.). The primary endpoint was short-term stricture resolution rate; secondary endpoints included ERCP-related complication rates (short- and long-term).
Results:
Median follow-up durations were comparable between BDBS (6 (4,9) months) and MDBS (7 (4,12) months) groups (p > 0.05). Short-term stricture resolution rates were 97.8% (45/46) in the BDBS group and 92.2% (71/77) in the MDBS group (p > 0.05). Early ERCP complications (hyperamylasemia, bleeding, perforation, cholecystitis) did not differ significantly between groups (all p > 0.05). However, the incidence of post-ERCP pancreatitis (PEP) was markedly higher in BDBS (37.0%, 17/46) than in MDBS (7.8%, 6/77; p < 0.05). Long-term complications (stent migration, occlusion) showed no intergroup differences (all p > 0.05), but late biliary infections were more frequent in MDBS (41.7%, 10/24) versus BDBS (7.7%, 3/39; p < 0.05).
Conclusion:
FCSEMS effectively alleviates strictures in both benign and malignant DBS, with comparable short-term efficacy. Notably, BDBS patients had a higher risk of early PEP, whereas MDBS patients were more prone to late biliary infections. Long-term stricture resolution was not analyzed due to divergent disease trajectories (e.g., limited survival in MDBS).
Plain language summary
This study looked back at 123 patients who received a small metal tube (stent) to open a blockage in their lower bile duct. The blockages were caused by either non-cancer (benign) conditions or cancer. Researchers compared how well and how safely the stent worked between these two groups. They found that the stent successfully opened the blockage in over 90% of patients in both groups. Short-term complication rates were similar, except for pancreatitis (pancreas inflammation), which occurred more often soon after the procedure in patients with non-cancer blockages. Over a longer period, problems like the stent moving or getting clogged were similar for both groups. However, patients with cancer-related blockages experienced more late bile duct infections. In summary, this stent treatment is effective for both non-cancer and cancer-related bile duct blockages. The main differences are that non-cancer patients have a higher risk of early pancreatitis, while cancer patients are more likely to develop infections later on. Long-term blockage relief was not compared because the underlying diseases, especially cancer, follow very different paths.
Introduction
Distal biliary strictures (DBS) refers to segmental narrowing of the distal common bile duct caused by various factors which leads to an increased incidence of cholangitis and cholestasis. DBS is composed of benign distal biliary stricture (BDBS) and malignant distal biliary stricture (MDBS). 1 The etiology of BDBS primarily includes iatrogenic injury (particularly post-laparoscopic cholecystectomy and liver transplantation), inflammatory conditions (notably chronic pancreatitis), and IgG4-related cholangitis and choledocholithiasis.2–4 MDBS are most frequently caused by malignancies originating from the pancreas, the bile duct itself, or the ampullary region.5,6
Historically, plastic stents are the mainstay therapy for DBS. Nonetheless, they need frequent replacement due to their small diameter which often causes suboptimal stricture dilation, and this imposes heavy physical and psychological burdens on patients. Fully covered self-expanding metal stents (FCSEMS), with patency rates exceeding 90%, has been widely acknowledged as the first-line and mainstream treatment.7–9 Compared with plastic stents, FCSEMS offer prolonged indwelling time meanwhile reduce the need for replacements. However, recent studies have increasingly reported10,11 the complications associated with the FCSEMS application, including stent migration, cholangitis, and acute pancreatitis.
Despite their widespread usage, the efficacy and safety of FCSEMS application in BDBS versus MDBS remain elusive. In this study, we conducted a retrospective study which analyzed 123 DBS patients undergoing FCSEMS placement at the Department of Gastroenterology, Shanghai East Hospital Affiliated to Tongji University, between January 2019 and December 2024. We aimed to evaluate the therapeutic efficacy and safety of FCSEMS across different pathological types of DBS and to address the evidence gap regarding the comparative efficacy of FCSEMS in benign versus malignant strictures.
Materials and methods
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE; Supplemental Material) statement. 12
Baseline characteristics
This study consecutively included 123 patients with DBS who underwent FCSEMS placement via endoscopic retrograde cholangiopancreatography (ERCP) at Shanghai East Hospital Affiliated to Tongji University from January 2019 to December 2024, comprising 78 males and 45 females, aged 26–101 years (mean ± SD: 73.54 ± 13.31 years). Among them, 46 cases were BDBS secondary to post-cholecystectomy stricture, choledocholithiasis, and cholangitis; 77 cases were MDBS attributed to cholangiocarcinoma, pancreatic cancer, gallbladder cancer, and regional lymph node metastasis. The specific etiologies of strictures, categorized by benign or malignant groups, are presented in the graph (Table 1).
Etiology.

BDBS, benign distal biliary stricture; MDBS, malignant distal biliary stricture.
No statistically significant differences between the two groups were observed in: age, sex, history of chronic cholecystitis/cholelithiasis, preoperative liver function, lipid profile, serum amylase, leukocyte count, maximum common bile duct diameter, ERCP cannulation time, stent diameter/length, or concurrent pancreatic stent placement (all p > 0.05). However, significant intergroup differences were noted for: preoperative bilirubin levels, stricture length, and main pancreatic duct dilation status (all p < 0.05; Table 2).
Risk factors for late-onset biliary infection after FCSEMS placement.

CBD, common bile duct; FCSEMS, fully covered self-expanding metal stents; OR, odds ratio; WBC, white blood cell.
Inclusion and exclusion criteria
Inclusion criteria: (1) definitive diagnosis of DBS based on symptomatology, laboratory investigations, and imaging (ACG Clinical Guideline: Diagnosis and Management of Biliary Strictures 13 ) with clear indications for ERCP; (2) written consent for ERCP with FCSEMS placement obtained from patients or legal representatives; (3) complete informed consent with a detailed treatment plan; (4) complete baseline and follow-up clinical data.
Exclusion criteria: (1) uncertain etiology of biliary stricture; (2) incomplete essential clinical data; (3) prior FCSEMS placement via ERCP; (4) failed endoscopic sphincterotomy (EST) procedure. 12
All patients who met the inclusion criteria were consecutively included in the study cohort. This diagram will show the complete process from the initial patient screening, through the application of inclusion and exclusion criteria, to the final analysis cohort (Figure 1).

Study flow.
Operating procedure
All procedures were performed by the same team, led by experienced endoscopists (>5000 ERCP cases). All patients received standard intravenous anesthesia administered by board-certified anesthesiologists, with continuous intraoperative hemodynamic monitoring. Strict aseptic techniques were followed. Preprocedural imaging was utilized to localize the biliary stricture. After successful biliary cannulation, contrast-enhanced cholangiography was performed to delineate the characteristics of stricture. All enrolled patients underwent standard EST, followed by biliary dilation using either balloon or catheter techniques. Under fluoroscopic guidance, appropriately-sized FCSEMS (BostonScientificCorporation, Marlborough, MA, USA) 14 were deployed with the proximal end extending about 2 cm above the stricture and the distal end positioned about 1 cm beyond the major duodenal papilla. For high-risk cases (prolonged cannulation >5 min or ⩾3 pancreatic duct wire passes), prophylactic pancreatic stents were placed to mitigate the risk of post-ERCP pancreatitis (PEP).
Postoperative management
Following ERCP, all patients will routinely receive a 50 mg indomethacin suppository administered rectally for prophylaxis. Patients remained fasting for 24 h with continuous monitoring of hemodynamic and abdominal symptoms. Serial laboratory assessments included: amylase levels and complete blood count at 3- and 24-h post-procedure, along with liver function tests at 24 h and 1 week. Complication-specific treatment was initiated immediately upon detection. For BDBS, our treatment strategy involves planned temporary stent placement, with a target indwelling duration of 6–9 months. Following this period, the stent is removed endoscopically via ERCP. Subsequent assessment of the stenosis is then performed to determine the need for any further intervention.
Observation indicators and evaluation criteria
Observation indicators
Short-term stricture resolution: Defined as intraoperative fluorographic evidence of contrast passage (residual diameter at the stenosis site not less than 75% of the diameter of the upper and lower bile ducts), sustained improvement of clinical symptom, and normalization of bilirubin levels or >50% reduction from baseline within 14 days.13,15
Long-term stricture resolution
BDBS: Demonstrated by successful contrast passage through the previously strictured segment on follow-up cholangiography after stent removal, with normalized liver function tests and sustained symptom resolution for 3–6 months post-removal.
MDBS: Maintained normal liver function during stent indwelling period, with verified contrast passage during scheduled stent exchange procedures (if performed). For surviving patients in both groups, stents were removed at 6–9 months, with reinsertion decisions based on stricture resolution status.
Complications
Short-term complications (⩽30 days post-procedure): hyperamylasemia, acute pancreatitis, bleeding, perforation, and cholecystitis. 16
Long-term complications (⩾31 days post-procedure): stent migration, stent occlusion, and recurrent biliary tract infections.17,18
Evaluation criteria: (1) acute pancreatitis: persistent abdominal pain >24 h with amylase/lipase ⩾3× ULN; (2) bleeding: clinically evident hematemesis/melena or hemoglobin reduction >2 g/dL; (3) biliary infection: documented fever (>38°C) >24 h with biochemical cholestasis and biliary dilation or gas accumulation supported by imaging (ultrasound/computed tomography); (4) perforation: radiologically confirmed extraluminal air or leakage of gastrointestinal content; (5) hyperamylasemia: serum amylase 3× ULN within 2–24 h post-ERCP without clinical symptoms19,20; (6) post-ERCP cholecystitis: occurrence of acute cholecystitis manifestations in the postoperative period.21,22
For BDBS, follow-up was continued until after the planned stent removal and subsequent evaluation. For MDBS, follow-up extended until the patient’s death or the study’s data cut-off date (December 31, 2024). In both groups, at least one post-procedural clinical or imaging assessment within the respective follow-up window was required for inclusion in the analysis.
Statistical analysis
Statistical analysis was performed using SPSS software (version 23.0; IBM Corp, Armonk, NY, USA). Continuous variables with normal distribution were compared using independent samples t tests, while non-normally distributed continuous variables were analyzed using the Mann–Whitney U test. Categorical variables were compared using either the chi-square test or Fisher’s exact test, as appropriate. A two-sided p-value < 0.05 was considered statistically significant.
Results
Baseline characteristics comparison
This retrospective study included 123 consecutive patients with DBS (BDBS: n = 46; MDBS: n = 77). Baseline characteristics showed no significant intergroup differences in age, sex distribution, history of chronic cholecystitis/cholelithiasis, preoperative liver function tests, lipid profiles, serum amylase levels, white blood cell counts, maximum common bile duct diameter, ERCP cannulation time, stent diameter/length, or concurrent pancreatic stent placement (all p > 0.05). However, elevated preoperative bilirubin levels, increased stricture length, and more frequent main pancreatic duct dilation compared to BDBS patients (all p < 0.05) 23 (Tables 3 and 4).
Comparison of complications between the two patient groups.
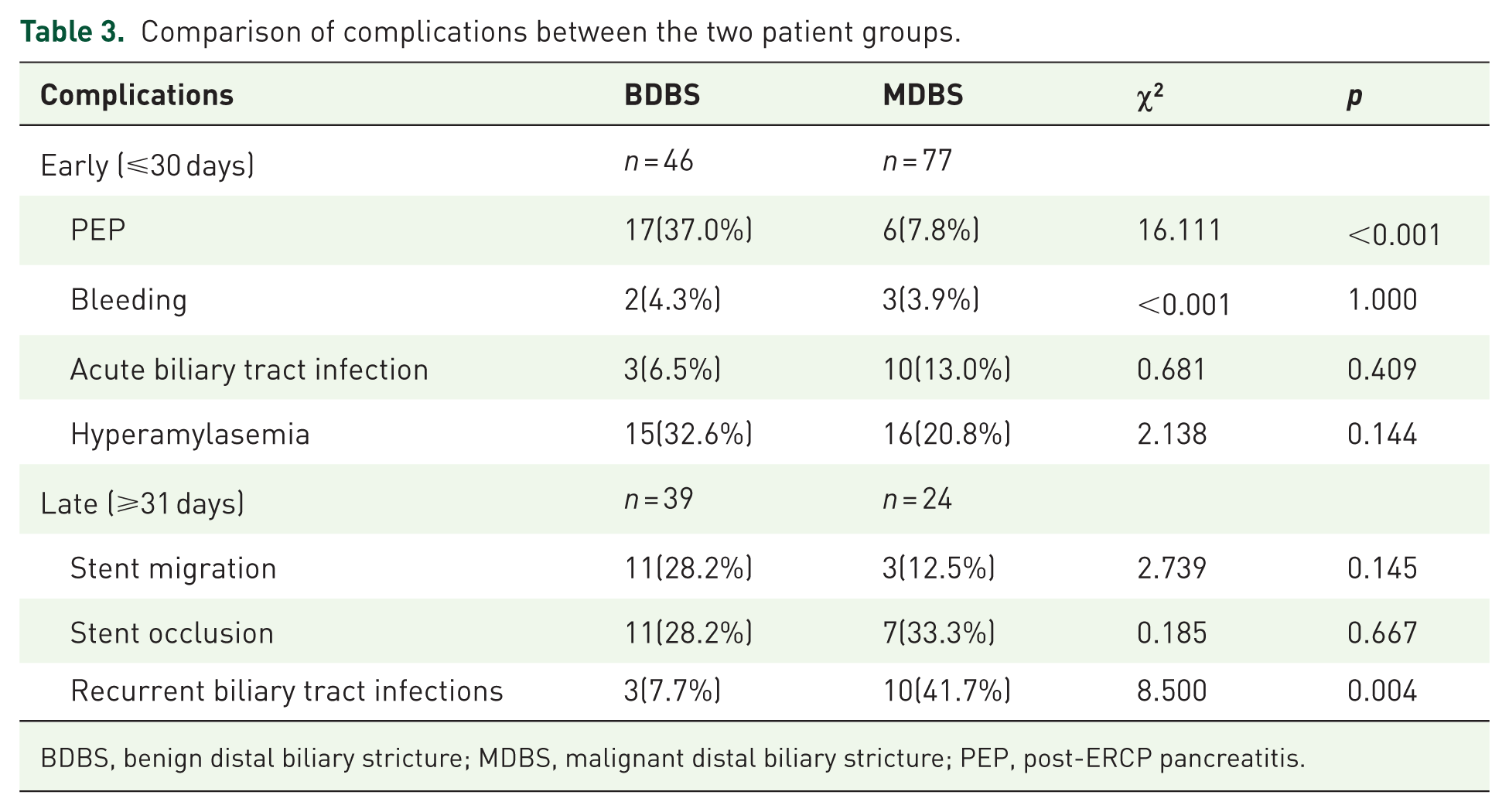
BDBS, benign distal biliary stricture; MDBS, malignant distal biliary stricture; PEP, post-ERCP pancreatitis.
Baseline characteristics of the patients.
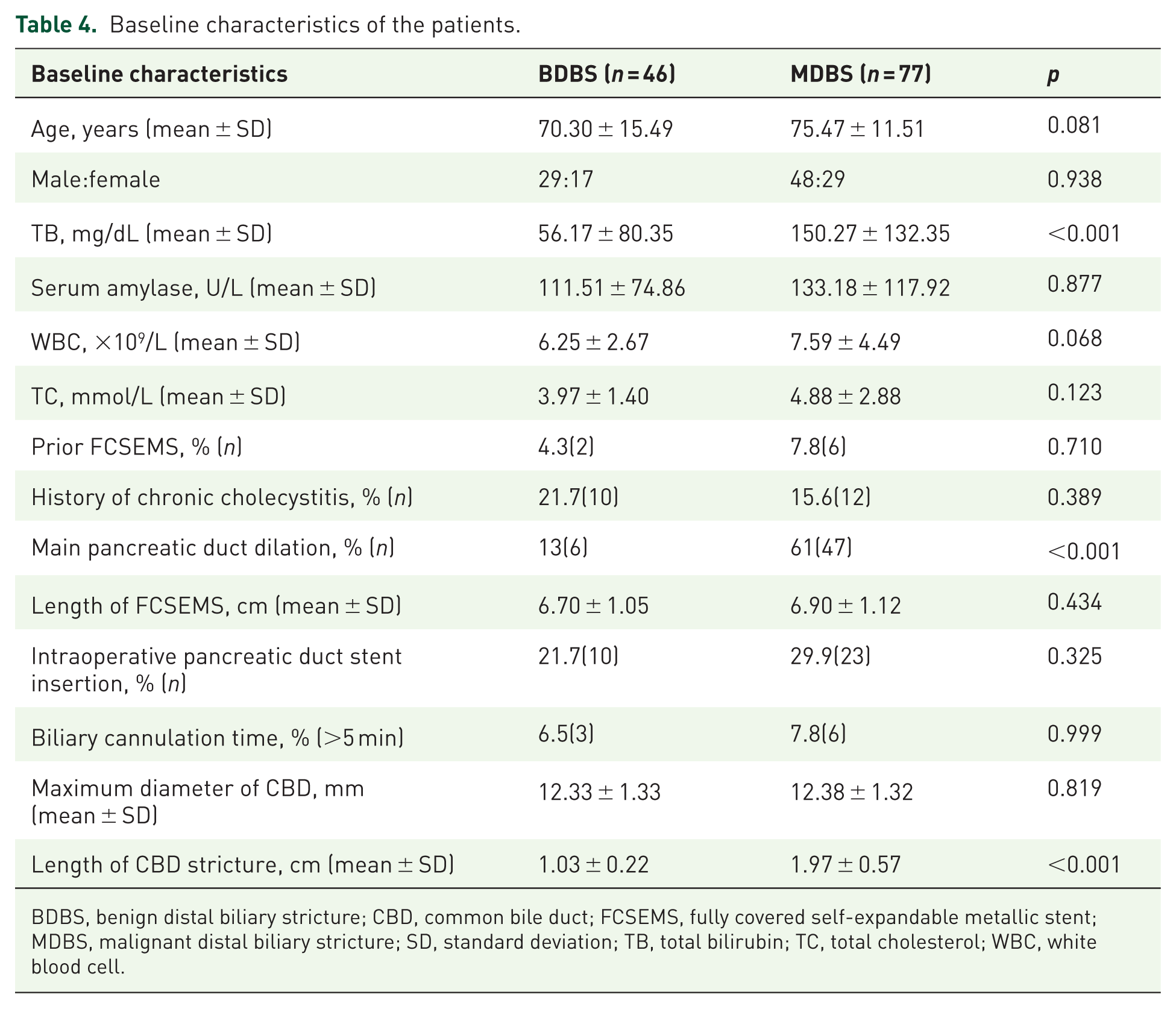
BDBS, benign distal biliary stricture; CBD, common bile duct; FCSEMS, fully covered self-expandable metallic stent; MDBS, malignant distal biliary stricture; SD, standard deviation; TB, total bilirubin; TC, total cholesterol; WBC, white blood cell.
Postoperative efficacy
Procedural success was confirmed by fluoroscopic demonstration of contrast medium passage through the strictured segment. Clinical outcomes were assessed through resolution of symptoms and serial measurements of serum total bilirubin, direct bilirubin, ALP, and GGT at 24 h, 1 week, and 2 weeks post-procedure. Short-term stricture resolution was defined as previously mentioned. 15 Resolution rates were 97.8% (45/46) in BDBS versus 92.2% (71/77) in MDBS (p = 0.369).
Comparison of postoperative complications
Short-term complications (⩽30 days post-ERCP): PEP incidence was significantly higher in BDBS patients compared with MDBS patients (17/46 vs 6/77, p < 0.05). No significant differences in hyperamylasemia, biliary infection, bleeding, perforation, or acute cholecystitis were observed between the two groups (all p > 0.05; Table 5).
Risk factors for early-onset acute pancreatitis after FCSEMS placement.

FCSEMS, fully covered self-expanding metal stents; OR, odds ratio; WBC, white blood cell.
Binary logistic regression analysis revealed BDBS may associated with PEP development (odds ratio (OR) = 0.217, p = 0.016). Preoperative bilirubin level (OR = 0.998, p = 0.399), and main pancreatic duct dilation (OR = 2.498, p = 0.176) were not significant predictors.
Stent indwelling time was 6 months (IQR, 4–9) in the BDBS group, compared with 7 months (IQR, 4–12) in the MDBS group.
Long-term complications (⩾31 days): Among 103 patients with complete follow-up (BDBS: n = 39, IQR of follow-up time: 6 month; MDBS: n = 64, IQR of follow-up time: 7 month; including 40 MDBS deaths during follow-up), biliary infections occurred more frequently in MDBS patients than that of BDBS patients (10/64 vs 3/39, p < 0.05). Stent migration and occlusion rates showed no differences between the two groups (p > 0.05).
Binary logistic regression identified MDBS may associated with long-term biliary infection (OR = 0.126, p = 0.041). Length of CBD stricture (OR = 1.339, p = 0.368), and main pancreatic duct dilation (OR = 1.952, p = 0.0.469) exhibited no obvious association with long-term biliary infection (Table 1).
Discussion
DBS classified into benign and malignant etiologies is a clinically significant biliary obstruction. ERCP with biliary stent placement is the established first-line therapy when biliary drainage is definitively indicated, with distinct therapeutic goals for each subtype: (1) for BDBS (e.g., post-surgical strictures or chronic pancreatitis-related strictures), stenting provides both relief of cholestasis and stricture remodeling through sustained radial force; (2) for unresectable MDBS, it serves as palliative care for obstruction management.24–26 The 2019 International Consensus Statement for Endoscopic Management of Distal Biliary Stricture strongly recommended endoscopic stenting as primary therapy for both BDBS and unresectable MDBS. 27
Current consensus and guidelines recommend both multiple plastic stents (MPS) and FCSEMS as effective treatment options for BDBS. Recent studies 17 have demonstrated equivalent therapeutic efficacy between FCSEMS and MPS, with FCSEMS offering significant advantages in reducing procedural frequency and shortening overall treatment durations. For unresectable MDBS, metal stent placement constitutes the standard of care. The selection between covered and uncovered SEMS is under continuous debate, though the emerging evidences indicate that FCSEMS provides superior median stent patency duration with comparable safety profiles.10,28,29 Consequently, the 2023 European Society of Gastrointestinal Endoscopy guidelines strongly recommend FCSEMS as the preferred option for pancreatic cancer-related malignant obstructions. 30 Therapeutic endoscopic ultrasound serves as a viable alternative when conventional ERCP fails or is not feasible due to anatomical alterations, tumor obstruction, or other complex factors. Its merits are demonstrated by the ability to perform single-session multi-site drainage, overcome anatomical barriers, and achieve high procedural success rates with a favorable safety profile.31,32
Current evidence7,33 confirm that FCSEMS demonstrates therapeutic efficacy for both BDBS and unresectable MDBS. However, this intervention carries non-negligible risks, including PEP, cholecystitis, non-obstructive cholangitis, hemorrhage, ulceration, perforation, and stent migration/occlusion. 34
Notably, comparative analysis of FCSEMS outcomes between BDBS and MDBS remains scarce in existing literature. In this study, our retrospective data reveal comparable short-term success rates between BDBS and MDBS groups (45/46 vs 71/77; p = 0.369), with significant biochemical improvements in both cohorts. Direct comparison of long-term resolution was precluded by fundamental disease trajectory differences, particularly the substantial mortality burden in the MDBS group.
Our findings demonstrate a significantly higher incidence of PEP in BDBS patients following FCSEMS placement compared with that of MDBS patients. This discrepancy may be explained by these distinct pathoanatomical characteristics: (1) Compared to BDBS, MDBS demonstrates more irregular and severe wall thickening, often with significantly longer stricture segments (median length: MDBS 1.97 ± 0.57 cm vs BDBS 1.03 ± 0.22 cm; p < 0.05); (2) BDBS often exhibits regularly concentric fibrotic wall thickening; (3) the uniform stricture morphology in BDBS generates greater radial force concentration at the pancreatic duct orifice during FCSEMS expansion.10,35
Our study reveals significantly higher prevalence of preoperative pancreatic duct dilation in MDBS compared with BDBS cases (61.0% vs 13.0%, p < 0.05). The MDBS cohort, particularly pancreatic head cancer patients with pre-existing pancreatic duct dilation, demonstrated an impaired pancreatic drainage with established ductal hypertension. 36 These patients characteristically lacked the symptoms or radiographic signs of acute pancreatitis preoperatively. In such cases, FCSEMS-induced compression of pancreatic orifice seldom precipitated PEP, likely due to concomitant pancreatic atrophy and exocrine insufficiency that collectively reduce pancreatic juice secretion. 37
Procedure-related PEP risk factors include cannulation duration, pancreatic duct wire passes, and prophylactic stent placement rates (BDBS: 10/46 vs MDBS 23/77; p = 0.325) showed no intergroup differences.38–41 Prolonged cannulation (>5 min) occurred in 6.5% (3/46) of BDBS procedures compared with 7.8% (6/77) of MDBS procedures (p > 0.999). Therefore, our study demonstrates that the incidence of PEP following FCSEMS placement is increased in BDBS.
Analysis of long-term complications demonstrates a significantly higher biliary infection rate in MDBS patients than that of BDBS patients. This discrepancy may be explained by two pathophysiological mechanisms: (1) MDBS patients exhibit more severe and longer strictures affected by the greater tumor burden. Although FCSEMS provides initial drainage, progressive tumor ingrowth and stent compression still lead to declining patency over time. 42 (2) FCSEMS compromises the native anti-reflux mechanism at the duodenal papilla, permitting duodenal-biliary bacterial migration. 43 In addition, the immunosuppressed state of MDBS patients also increases the risk of infection.
A significant proportion of patients in both the MDBS and BDBS groups were lost to follow-up due to death or other causes. To mitigate the potential bias introduced by these losses, we employed Kaplan–Meier analysis to assess long-term complication rates. Survival curves for the two groups were compared using the log-rank test. No significant difference was observed between the benign and malignant groups in terms of stent occlusion (p > 0.05), nor were there significant differences in their overall survival curves. Similarly, the difference in the incidence of long-term biliary infection between the groups did not reach statistical significance (p > 0.05).
These findings suggest that loss to follow-up, particularly due to mortality, may have influenced the final outcomes during the stent patency period. This lack of significant differences could be attributed to the limited number of events and the relatively short median follow-up time. Future studies with larger sample sizes and extended follow-up durations are warranted to confirm or refute these potential associations (Figures 2 and 3).
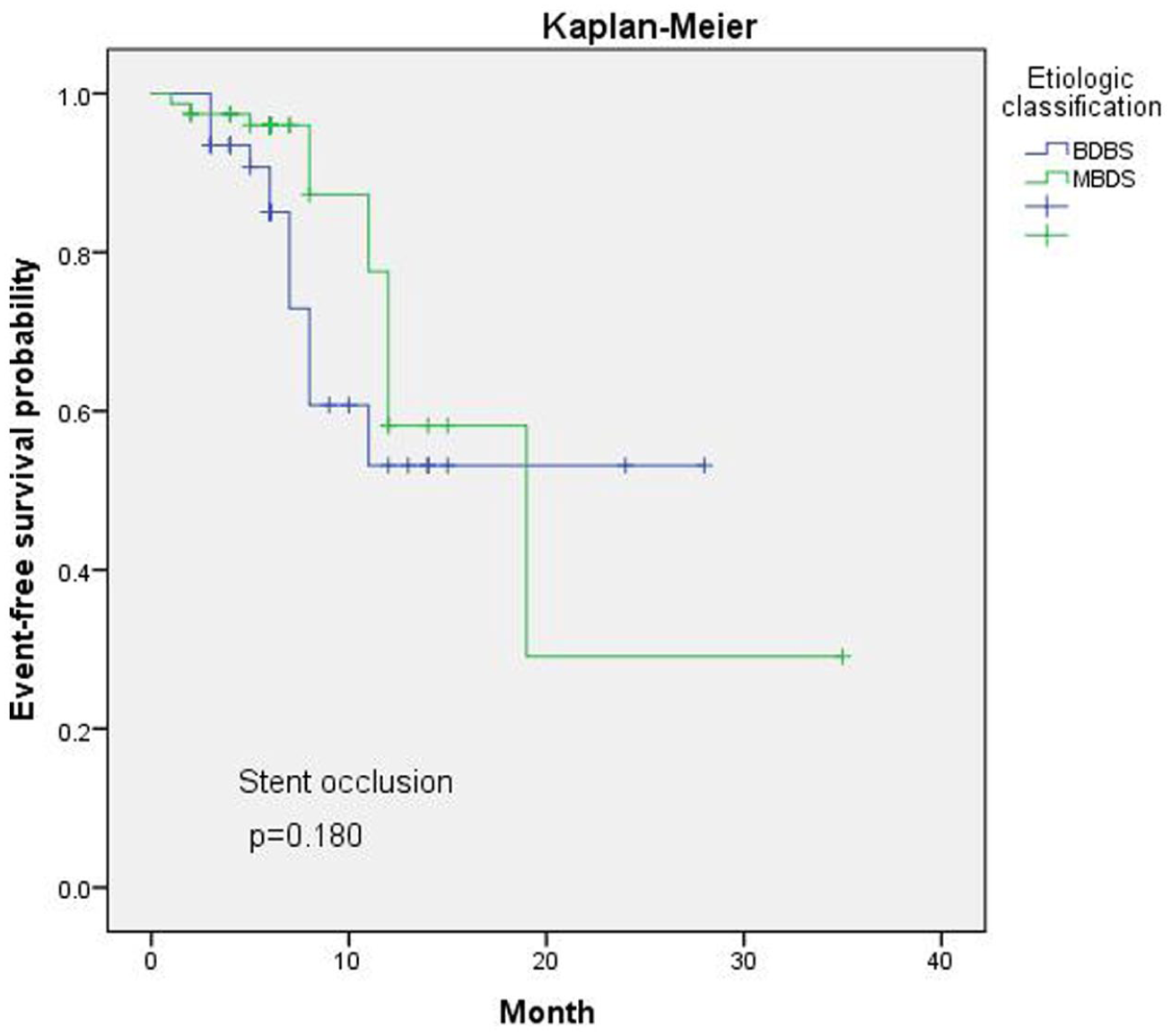
Kaplan–Meier of stent occlusion.

Kaplan–Meier of long-term biliary infection.
Our statistics still have limitations in the following aspects: (1) The observed differences in short‑term complications are preliminary and based on a relatively small number of PEP events; therefore, they require validation through larger-scale prospective studies in the future. (2) Data on certain important variables, such as the number of guidewire passages through the pancreatic duct, were missing to a substantial extent due to documentation gaps, which may have resulted in residual confounding.
Conclusion
In conclusion, FCSEMS demonstrates excellent efficacy for biliary decompression and clinical improvement in both BDBS and MDBS, with comparable short-term success rates. However, BDBS patients exhibited a significantly higher PEP incidence, particularly with prolonged cannulation (failed pancreatic stent placement). For these high-risk patients, intraoperative prophylactic pancreatic stent placement is strongly recommended. MDBS patients showed a greater long-term cholangitis risk, and stent indwell duration (<6 or ⩾6 months) showed no significant association with infection rates (p = 0.313).
This study still has several limitations which warrant consideration: restricted statistical power due to cohort size and follow-up duration, potential selection bias due to its single-center retrospective design, which lacks for multicenter validation, affecting generalizability.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261435331 – Supplemental material for Comparative study on the application of fully covered self-expanding metal stents in benign and malignant strictures of the distal bile duct
Supplemental material, sj-docx-1-tag-10.1177_17562848261435331 for Comparative study on the application of fully covered self-expanding metal stents in benign and malignant strictures of the distal bile duct by Ziyan Wang, Fei Xu, Weigang Shu, Xinyan Zhu and Feng Zhu in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors would like to express their gratitude to all individuals and institutions who contributed to the completion of this study. We also sincerely thank the reviewers and editors for their constructive comments, which have greatly improved the quality of this manuscript.
Declarations
Supplemental material
Supplemental material for this article is available online.