
Abstract
Background:
Post-liver-transplant biliary anastomotic strictures (ASs) are currently managed with repeated endoscopic retrograde cholangiopancreatographies (ERCPs) inserting multiple plastic stents. Fully covered self-expanding metal stents (FCSEMSs) are being increasingly reported in the management of this condition, however no prospective randomized trials have been performed to date.
Aim:
The aim of this study was to determine whether FCSEMSs decrease overall numbers of ERCPs needed to achieve stricture resolution and to establish the safety, efficacy and cost-effectiveness in this setting.
Methods:
Two tertiary referral centres performed this open-label prospective randomized trial. A total of 32 patients consented and subsequently 20 were randomized with 10 in the FCSEMS arm and 10 in the plastic arm. The FCSEMS arm had the stent in situ for 12 weeks with the plastic stent arm undergoing 3-monthly multiple plastic stenting with or without dilatation over a year.
Results:
The median number of ERCPs performed per patient in the FCSEMS was 2 versus 4.5 (p = 0.0001) in the plastic stenting arm. Stricture resolution was achieved in all 10 patients with FCSEMSs compared with 8/10 in the plastic arm [p = not significant (NS)]. Complications occurred in 1/10 patients in the FCSEMS arm versus 5/10 in the plastic arm (p = 0.051). Days in hospital for complications was 6 in the FCSEMS versus 56 in the plastic arm (p = 0.11). Cost analysis shows that the FCSEMS arm was more cost effective. No cases of FCSEMS migration were seen.
Conclusions:
FCSEMSs reduced the number of ERCPs needed to achieve stricture resolution with similar recurrence rates between arms. The FCSEMSs may do so with fewer complications making it cost effective.
Introduction
Post-liver-transplant biliary anastomotic strictures (ASs) are the most common biliary complication of liver transplantation and have been documented to occur in between 5.8% and 39% of cases [Thuluvath et al. 2003; Abdullah et al. 2005; Gomez et al. 2009]. These strictures result from a combination of local ischaemia, fibrotic healing and surgical techniques. Endoscopic treatment is now accepted as first-line treatment rather than percutaneous interventions or surgery, however worldwide practice does vary. Success rates for endoscopic intervention in the treatment of ASs is quoted up to approximately 80% for cadaveric liver transplants (CLTs) and 60% for living donor related liver transplants (LDLTs) [Shah et al. 2004; Pascher et al. 2006; Tarantino et al. 2008]. The optimal endoscopic intervention remains a matter of debate with most publications suggesting insertion of multiple large diameter plastic stents with or without dilation of the stricture 3 months apart until resolution of the stricture often at 12 months [Thuluvath et al. 2003].
Self-expanding fully covered metallic stents have traditionally been used in malignant biliary obstruction. With the addition of covering, embedding of stents is prevented allowing for the possibility of removal. Early studies in partially covered stents and fully covered self-expanding metal stents (FCSEMSs) for benign biliary strictures including ASs have been positive [Kahaleh et al. 2008; Traina et al. 2009]. To date there are multiple publications of FCSEMSs in benign biliary strictures (BBSs) and ASs indicating good stricture resolution rates; however, problems such as stent migration have been reported [Hu et al. 2011; Park Do et al. 2011; Poley et al. 2012; Tarantino et al. 2012]. Other than stent migration, the key drawback of available FCSEMS is the length of the normal distal bile duct that needs traversing for the stent to cross the stricture.
In conjunction with Taewoong Medical, we designed a new FCSEMS that has an antimigration waist, a short stent length with a long removal string that rests in the duodenum for easy removal (Figure 1). After an initial trial in two cases [Tee et al. 2010] we proceeded to this prospective randomized multicentre study comparing this new stent with conventional endoscopic retrograde cholangiopancreatography (ERCP) stricture management.

Modified fully covered self-expanding metal stent (SEMS) with a central waist and a long removal string.
Materials and methods
This was a prospective randomized open-label trial comparing our novel FCSEMS (Taewoong Medical (Gveonggi-Do, Korea) with conventional plastic stenting protocols in two tertiary referral liver transplant centres in Australia: Royal Prince Alfred Hospital, NSW and Austin Hospital, Victoria. This study was approved by respective local ethics boards.
Patients
All patients referred by the liver transplant team for possible AS were approached for the study. All patients had a comprehensive clinical assessment including biliary imaging performed by the medical transplant team. In all patients where an AS was considered, informed written consent was obtained. The indications for liver transplant are outlined in Table 1. If at ERCP an anastomotic stricture was confirmed (defined as a narrowing occluding more than 70% of the lumen), patients were then randomized. Patients who did not consent to the trial would receive the standard treatment of repeated 3-monthly plastic stenting and stricture dilation and were not included in the study. The randomization was computer generated and once an AS was confirmed at ERCP an envelope was opened to reveal the treatment protocol. The protocol is outlined in Figure 2.
Indications for liver transplant.

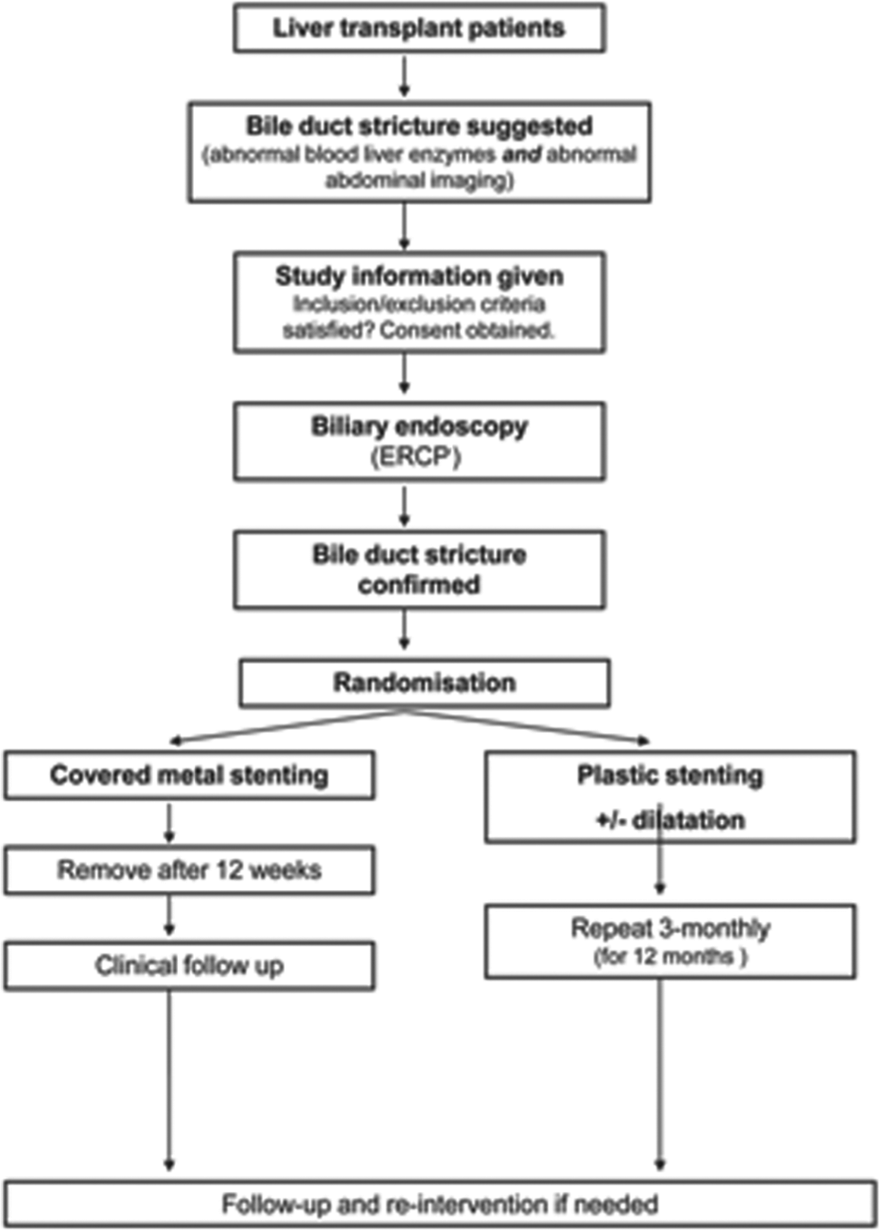
Post-transplant biliary structure study flow diagram. ERCP, endoscopic retrograde cholangiopancreatography.
The inclusion criteria included: a new diagnosis of post-liver-transplant biliary ASs, subjects older than 18 years of age and willing to take part in the trial, and CLT. Exclusion criteria included: non-ASs, hepatic artery thrombosis, intrahepatic biliary disease such as primary sclerosing cholangitis (PSC), and all strictures on ERCP proximal to and involving the hilum. Patients with leaks alone were not included.
Intervention
Protocol for the metal arm group (M)
Once the stricture was confirmed and the patient randomized to the metal arm, a long 480 cm guide wire (metro tracer, Cook Medical, Winston-Salem, NC) was inserted across the stricture. The metal stent was then placed into position. This stent has three radio-opaque markers placed equidistant with one at either stent end and one in the middle. The middle marker was positioned adjacent to the stricture and deployed by retracting the external sheath in a similar fashion to other self-expanding metal stents (SEMSs). Once the stent was fully deployed, the sheath was then completely retracted to release the removal string from the delivery mechanism. The patients would then be brought back to have the stents removed at approximately 12 weeks to assess the stricture. If the stricture had resolved, no further stenting was performed and patient was placed on clinical follow up.
Protocol for the plastic arm (P)
Once the AS was confirmed and the patient randomized to this arm, the proceduralist then aimed for multiple plastic stent insertion preferring a 10 Fr calibre. It was up to the discretion of the proceduralist to dilate. These patients were then brought back at 3-monthly intervals for the removal of the stents via ERCP and an assessment of the stricture. Should the stricture show cholangiographic resolution prior to the 12-month period, the patient was not stented and placed on clinical follow up instead. The proceduralist aimed for a maximum stent number and the preferred stents were 10 Fr stents (Cook Medical, Winston-Salem, NC).
All ERCPs were performed using an Olympus therapeutic TJF-Q180V Duodenoscope (Olympus Optical Co., Tokyo, Japan) and were performed under conscious sedation using Fentanyl, Midazolam or with the assistance of an anaesthetist using propofol sedation or occasionally a general anaesthetic (this was at the discretion of the anaesthetist). ERCPs were performed in the semiprone position (swimmers position) our in a supine position if intubated depending on the proceduralist’s preference. Prophylactic antibiotics were given in all cases as a preprocedural or periprocedural intravenous dose of 3.1g of ticarcillin sodium and potassium clavulanate (GlaxoSmithKline, Victoria, Australia).
Stents
The FCSEMSs used were produced by Taewoong Medical (Taewoong Medical, Seoul, Korea). All were made from Nitinol and the covering was polytetrafluoroethylene. The stent had a diameter of 10 mm at either end and had a gradual narrowing into the centre to 8 mm diameter. The fixed stent length was 40 mm with a 10 cm suture which allowed removal by using a standard endoscopic biopsy forceps.
Cost analysis
Hospital costs including the cost of a standard ERCP to be performed in the day stay ward and standard overnight stay on the transplant ward were provided by the area health facility and are as follows (all values reported are in Australian dollars): ERCP $4165, one inpatient day $1700, metal stent $2500. The costs of all accessories used were according to standard list prices of each device to the area health service. These components were then calculated for each treatment episode during each patient’s treatment protocol. The final costs were reported in two ways. The cost to complete the study protocol of stricture treatment, and the total costs of treatment and follow up including all additional ERCPs required.
Statistical analysis
All statistical analysis was carried out using STATA (v 10.0, Statacorp, Texas, USA). Baseline and demographic data along with outcome variables were compared. The Mann–Whitney U test was used to compare nonparametric continuous variables, Pearson chi-squared analysis was used to compare nonparametric categorical variables and Student’s t tests were used to compare parametric variables. Two-tailed tests with a significance level of 5% were used throughout. No sample size calculations were performed as there were too many unknowns to make accurate predictions.
An unrestricted research grant of 10 FCSEMSs was made available by the device manufacturer which predetermined the sample size. Preliminary calculations based on available data indicated that the study may be underpowered to detect superiority of FCSEMSs over multiple plastic stents for the primary end point; however, a true sample size calculation could not be reliably performed because of the lack of suitable published data in this area at the time of commencement of this study.
Results
Patient demographics
From August 2008 to July 2011, 32 patients consented with a total of 20 patients randomized. The 12 patients not randomized were excluded due to intrahepatic strictures, hilar involvement or no stricturing disease. The baseline characteristics of the patients are outlined in Table 2. The time to develop an AS was higher in the plastic stent arm was due to a single outlier who presented after 17 years but otherwise was not different between groups. All patients had received orthotopic liver transplants (OLTs) and there was no difference in indication for transplant between study groups.
Baseline characteristics of the randomized groups.

AS, anastomotic stricture; FCSEMS, fully covered self-expanding metal stent.
Procedure details
The median number of ERCP procedures for the FCSEMS arm was 2 (all had 2 procedures) compared with 4.5 (range 2–6) in the plastic stent arm (p = 0001). The median treatment time was 3.8 months (range 2.5–5) in the FCSEMS arm compared with 10.1 months (range 4–13) in the plastic stent arm. In the plastic stent arm, the median number of dilatations was 1.5 (range 0–2) per patient and 7.5 (range 3–13) plastic stents per patient. The follow up after protocol completion was 24.5 months (range 4–38 months) in the FCSEMS arm and 23 months (range 1–42 months) in the plastic arm [p = not significant (NS)]. These results are summarized in Table 3.
Treatment protocol details according to randomisation.

ERCP, endoscopic retrograde cholangiopancreatography; FCSEMS, fully covered self-expanding metal stent.
Outcomes
Stricture resolution
In the FCSEMS arm, the stricture resolution was achieved in all patients at stent removal. Stricture resolution was achieved in 8/10 patients in the plastic arm p = NS.
Recurrence rates
There were 3 AS recurrences (30%) in the FCSEMS arm treated successfully with ERCP however one patient developed severe ischaemic hilar stricturing requiring multiple ERCPs (10 additional ERCPs for hilar stricturing and AS recurrence during follow up). The total number of additional ERCPs in this group was 19. There were 3 AS recurrences (37.5%) in the plastic arm and this was not statistically different to the FCSEMS arm. All three were successfully treated with additional stenting as were the two cases that had not achieved stricture resolution at the end of their protocol. Additional ERCP treatment for ongoing or recurring strictures in the plastic group totalled 16. These results are outlined in Table 4.
Treatment outcomes according to stenting protocol randomisation.

FCSEMS, fully covered self-expanding metal stent.
Complication rates
During the treatment protocol, one patient (10%) had a complication in the FCSEMS arm with cholangitis post-FCSEMS removal and was successfully treated as an inpatient. In the plastic arm five (50%) patients experienced a complication with four experiencing cholangitis and one pain. This difference in complication rates did not achieve statistical significance (p = 0.0505). The total number of inpatient days for these complications was 6 for the FCSEMS arm versus 56 days in the plastic arm. This did not achieve statistical significance with a p value of 0.11.
There were no cases of stent migration with the FCSEMS and one case of proximal plastic stent migration leading to cholangitis and a prolonged ERCP to retrieve the stent.
Cost analysis
The cost of completing the protocol was lower in the metal arm when compared with the plastic arm: $10,830 compared with $23,580, respectively (p = 0.02). When additional procedures during post-protocol study follow up were included in the analysis, the metal arm was still more cost effective at $12,913 compared with $29,280 for the plastic arm; however, this did not reach statistical significance (p = 0.08).
Discussion
The conventional treatment for ASs has been repeated biliary plastic stenting and dilatation every 3 months until stricture resolution. This convention is not always agreed upon with some authors advocating longer periods of stent exchange whilst others preferring dilatation only to minimize the complication rates. In general, ERCP is effective and considered the first-line intervention for ASs. However, these approaches necessitate repeated ERCPs and hospital admissions and expose patients to the attendant complications of ERCP. Furthermore the small calibre and diameter of the available plastic stents mean that multiple stents need to be inserted to achieve adequate dilation and this can be technically challenging.
The potential benefits of a single FCSEMS are in its relative simplicity when compared with multiple plastic stents and its more attractive commitment to only two ERCP procedures for insertion and subsequent removal. There are now multiple case series published using such stents with generally good outcomes [Traina et al. 2009; Tee et al. 2010; Park Do et al. 2011; Poley et al. 2012; Tarantino et al. 2012]. Stricture resolution rates are high and often quoted at over 80% which is similar or better when compared with published series in plastic stent use [Shah et al., 2004; Pascher et al., 2006; Tarantino et al., 2008]. The key issues that remain are stent migration, failure to remove the stent from embedding and secondary stricturing. The stent migration rates vary from 0 to 41% [Park et al. 2011]; however, the migration rates seem to be at around 15–20% when all studies are considered. The secondary stricture rates and failure to remove rates are uncommon with isolated cases reported [Kasher et al. 2011]. In our series these were not an issue. We had no stent migration episodes and no cases where removal was difficult. At no stage during the protocol or in follow up did we encounter a secondary stricture.
The unique design in our FCSEMS probably explains why there were no migration cases. The design has a mid stent waist when compared with the stent ends: 8 mm centre diameter compared with the 10 mm diameter at the ends of the stent. This design produces a radial force and an additional force towards the stent centre. The additional benefit of this new design prevents excessive normal common bile duct (CBD) stenting. When a conventional FCSEMS is used they must traverse a long normal CBD segment to reach a short 1–2 cm benign stricture. This imbalance exposes the stent to forces dragging it down the duct and can lead to migration and poorer stricture resolution rates. The new design in our stent allows for the entire stent to be placed completely inside the duct with an even length of stent above and below the stricture.
Our study is the only prospective randomized study of metal stenting compared with plastic stenting. Even though we showed no superiority in stricture resolution or recurrence rates, our study shows that FCSEMSs can provide the same or better outcomes with fewer procedures and complications. This translated to a more cost-effective treatment protocol where the hospital stay costs far outweighed the metal stent cost. Even though our study failed to show a statistically significant reduction in complications and inpatient stay for these, it is likely a type 2 error due to our small sample size.
The small sample size is the main limitation of our study and occurred despite dual centres and an ample recruitment period of 3 years. Our other limitations include a high complication rate in the plastic stent arm. This may be explained in two ways. The majority of papers publishing outcomes with plastic stents are retrospective and it is well known that retrospective series under-report their complications. Complication reporting varies in the literature and has been reported to be high at approximately 20–28% [Dumonceau et al. 1998; Kassab et al. 2006]. However, when studied prospectively the rate is similar even in nontransplant studies [Van Der Gaag et al. 2010]. This highlights the well-known problem of plastic prostheses in the bile duct. This alone may lead to an under-reporting of this complication in retrospective series. Also, not all cholangitis required inpatient care and this may explain why our reports are so high.
The other possible limitation in our paper is an apparent suboptimal treatment of the plastic stent group. Despite a protocol aiming for 12 months of maximum stent intervention our cohort were treated for less than a year and with a median of 7.5 stents per patient. These numbers are skewed due to one patient who had complete AS resolution after one episode of plastic stenting with two 10 Fr stents. When compared with other published series our numbers fare quite well and accurately reflect the standard in clinical practice [Rerknimitr et al. 2002]; however, in the nontransplant setting maximal stenting above our efforts suggest better outcomes [Costamagna et al. 2001].
There was a discrepancy between our groups in the mean time to develop an AS and this may have played a role in the outcomes. The plastic stent arm had ‘older’ strictures (developed later post- OLT); however, due to our small sample size this was caused by a single outlier being a patient who presented 17 years after his OLT. When excluding this patient there was no difference between the two groups. There have been authors suggesting a different aetiology in early AS (less than 1 month) with the implication that these strictures are oedema related and probably easily resolved [Poley et al. 2013]. In our study some of our most resistant strictures with recurrences were early ASs, and our most easy to treat stricture being our oldest (17 years) resolving before completing protocol with plastic stents and not recurring in follow up. There is still uncertainty and little data to suggest the onset of ASs being a predictor of successful endoscopic intervention.
In conclusion, our FCSEMS achieved similar stricture resolution with similar stricture recurrence rates to conventional plastic stenting. These outcomes were achieved with fewer procedures and procedure-related complications making metal stenting a cost-effective strategy. Owing to our small sample size, we recommend further randomized studies to validate our results.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors have no conflicts of interest to declare.