
Abstract
Background:
The rising incidence of hilar malignant bile duct strictures poses challenges for diagnosis and treatment. While endoscopic treatment is essential for relieving obstruction, it carries a high risk of postoperative cholangitis. Sequential cutting of nasobiliary tubes as an alternative to stent placement after nasobiliary drainage may emerge as an effective strategy to mitigate these complications.
Objectives:
This study aimed to evaluate the efficacy and safety of nasobiliary tube cutting after nasobiliary drainage versus conventional stent placement in reducing postoperative cholangitis in patients with hilar malignant biliary strictures.
Design:
A retrospective cohort study.
Methods:
From 2015 to 2023, 208 patients were divided into two groups: nasobiliary tube cutting group (n = 103) and conventional stent group (n = 105). The primary outcome was postoperative cholangitis, with secondary outcomes including drainage success, bilirubin reduction, re-interventions, complications, and hospital stay.
Results:
Cholangitis occurred in 11.7% of the nasobiliary tube cutting group and 26.7% of the conventional stent group (p = 0.006). Successful drainage was achieved in 84 patients (81.6%) in the nasobiliary tube cutting group and 78 patients (74.3%) in the conventional stent group, with no statistically significant difference (p = 0.207). Patients whose total bilirubin reduction >50% within 7 days were significantly higher in the nasobiliary tube cutting group (48.5% vs 27.6%, p = 0.002). There were no significant differences between the groups in the number of endoscopic retrograde cholangiopancreatography procedures or re-interventions required (p > 0.05). Except for postoperative cholangitis, other postoperative complications were comparable between the groups (p > 0.05). The postoperative hospital stay was significantly longer in the nasobiliary tube cutting group, with a median duration of 10.0 (7.0, 14.0) days compared to 7.0 (5.5, 12.5) days in the conventional stent group (p = 0.024). Bismuth-Corlette Type IV was identified as an independent risk factor for cholangitis (OR = 3.207, 95%CI: 1.253–8.210, p = 0.015).
Conclusion:
For patients with hilar malignant biliary stricture, sequential cutting of nasobiliary tubes as an alternative to stent placement after nasobiliary drainage may reduce the incidence of postoperative cholangitis and achieve early successful drainage, but it may result in a prolonged postoperative hospital stay. Bismuth-Corlette Type IV is an independent risk factor for the development of postoperative cholangitis.
Keywords
Introduction
In recent years, the incidence of hilar malignant biliary stricture has been steadily increasing, garnering significant attention and presenting considerable challenges in diagnosis and treatment. Hilar malignant biliary stricture refers to the narrowing of the bile ducts in the porta hepatis region, primarily caused by malignant tumors such as cholangiocarcinoma, gallbladder cancer, pancreatic cancer, liver cancer, and so on.1 –3 Early clinical manifestations are often subtle and nonspecific, including symptoms such as upper abdominal discomfort, fever, fatigue, poor appetite, nausea, vomiting, weight loss, and skin itching. Most patients seek medical care due to progressive jaundice, which typically signals advanced disease. At this stage, worsening bile duct obstruction at the hepatic hilum leads to systemic jaundice, darkened urine, and pale stools. 4 The lack of specific early symptoms and effective diagnostic tools makes early detection difficult, leaving many patients ineligible for surgical intervention and with poor prognoses. Endoscopic treatment has become increasingly important as a key approach to alleviating bile duct obstruction and improving patient outcomes.
With the development of endoscopy technology, especially the maturity of the Endoscopic Retrograde Cholangiopancreatography (ERCP) technique, endoscopic treatment has become increasingly important in the management of biliary-pancreatic diseases. Nowadays, endoscopic drainage is a primary method for relieving bile duct obstruction and alleviating jaundice. The current endoscopic drainage methods include Endoscopic Retrograde Biliary Drainage (ERBD), Endoscopic Metal Biliary Endoprosthesis, and Endoscopic Nasobiliary Drainage (ENBD). The advantages of metal stents are long drainage patency time and rapid reduction of jaundice, but the drawback is that it is challenging to place multiple stents, and if the drainage is ineffective, it is difficult to conduct endoscopic treatment again.5 –7 Plastic stents are easy to place, but they have a short duration of patency, slower reduction of jaundice, and replacement will be required if the stent becomes blocked.8,9 Although multiple stents may be used in selected cases, they can increase the risk of biliary duct injury, biliary infection, and stent occlusion. Furthermore, their cost can be a significant limitation for widespread use in certain healthcare settings. Nasobiliary tubes have several advantages, such as multiple side holes for better drainage, soft texture for easier access to angled bile ducts, and they can be positioned in secondary bile ducts.10,11 During external nasobiliary drainage, bile drainage can be observed, and bile duct irrigation can be performed according to the drainage conditions. However, nasobiliary tubes can lead to displacement or dislodgement, increasing the risk of infection and causing discomfort to patients, affecting their quality of life. In addition to these methods, endoscopic ultrasound (EUS)-guided biliary drainage (EUS-BD) has emerged as an effective alternative when ERCP fails or is not feasible, providing internal drainage with minimal discomfort and reduced infection risks. 12 Similarly, percutaneous transhepatic biliary drainage (PTBD) remains a valuable option, particularly for acute obstructions or when endoscopic methods are contraindicated. 13
Although nasobiliary tubes and stents have been widely used in clinical practice, there is still a lack of consensus on the optimal drainage method for patients with hilar malignant biliary stricture. The clinical gap remains in identifying a drainage method that combines the benefits of effective internal drainage with minimized complications and improved patient comfort. Some scholars have proposed cutting the nasobiliary tube with endoscopic scissors outside the gastric antrum or duodenal papilla, retaining a portion inside the bile duct as an internal stent for drainage, to achieve the conversion of external drainage to internal drainage.14,15 However, the efficacy and safety of cutting of nasobiliary tubes as an alternative to stent placement in clinical practice have not been further confirmed.
This study aims to compare the incidence of postoperative cholangitis, as well as secondary outcomes such as drainage success rate, interventional procedures, postoperative complications, and length of hospital stay, between the nasobiliary tube cutting group and the conventional stent group. It seeks to explore the efficacy and safety of sequential cutting of nasobiliary tubes as a stent replacement in the treatment of malignant hilar bile duct strictures, providing a new treatment method for internal drainage of hilar malignant biliary strictures and improving patients’ quality of life.
Methods
Design
This was a retrospective cohort study. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 16
Patients
The patients diagnosed with hilar malignant biliary stricture who received ERCP at Hangzhou First People’s Hospital between January 2015 and January 2023 were assessed consecutively (Figure 1). Patients were identified using the hospital’s electronic medical record system. All eligible cases were checked to ensure adherence to inclusion and exclusion criteria.

Workflow diagram.
Inclusion criteria: (1) age ⩾18 years old, (2) hilar malignant biliary stricture was diagnosed by upper abdominal CT, magnetic resonance cholangiopancreatography (MRCP), or endoscopic ultrasound, (3) ERCP-guided endoscopic drainage was performed, utilizing either sequential cutting of nasobiliary tubes as an alternative to stent placement after nasobiliary drainage or conventional stent placement, (4) Bismuth-Corlette classification: Type II–IV was included. The Bismuth-Corlette classifications were initially assessed by radiologists based on imaging studies. For cases with ambiguous or borderline classifications, two experienced radiologists independently re-evaluated the imaging data. If disagreements arose, a third radiologist was consulted to facilitate consensus and ensure accurate classification. This systematic approach guarantees reliability and consistency in patient classification. Exclusion criteria: (1) previous biliary drainage (endoscopic, percutaneous, or surgical), (2) patients with acute cholangitis, and (3) incomplete clinical data. The diagnosis of acute cholangitis followed the Tokyo Guidelines 2013 gold standard: (1) purulent bile was observed, (2) clinical remission followed bile duct drainage, (3) remission was achieved by antibacterial therapy alone, in patients in whom the only site of infection was the biliary tree. 17 This study retrospectively diagnosed acute cholangitis based on comprehensive clinical evaluation and ERCP findings.
According to the different biliary drainage methods adopted in ERCP, the patients were divided into two groups: the nasobiliary tube cutting group and the conventional stent group. The data collection included demographic information, imaging data, laboratory parameters, and treatment situations. If key demographic or clinical variables were missing, the patient was excluded from the study to maintain data integrity. For secondary variables, multiple imputation was used to address missing values where appropriate, with sensitivity analyses performed to confirm the robustness of results. The proportion of missing data for each variable was less than 5%.
Patient data confidentiality was strictly maintained throughout the study. All patient identifiers were removed, and data were anonymized prior to analysis. Access to the data was restricted to authorized researchers only, in accordance with institutional and ethical guidelines.
ERCP procedure
All patients underwent full preoperative preparation according to standard ERCP procedures. The endoscope physician employs a duodenoscope (TJF-260V, Olympus Corporation, Tokyo, Japan) to orally navigate through the esophagus and stomach into the descending segment of the duodenum for observation of the major duodenal papilla. Subsequently, selective biliary cannulation is conducted using a guidewire, followed by cholangiography. Cholangiograms during ERCP were performed using ioversol injection (Jiangsu Hengrui Medicine Co., Ltd., Jiangsu, China), to visualize the biliary anatomy and guide interventions. Then, a reassessment of the Bismuth-Corlette classification is conducted and compared with MRCP results for confirmation. Then, a guidewire is inserted into the bile duct and advanced into position for subsequent placement of a dilation catheter. Next, in the nasobiliary tube cutting group, the nasobiliary tube is inserted (Figure 2(a)). The nasobiliary tube cutting procedure is performed 2–7 days after the operation, following the assessment that the nasobiliary drainage is unobstructed and the patient’s condition is stable. The gastroscope was advanced into the stomach or duodenum to identify the nasobiliary tube at the cutting location, which was outside the opening of the major duodenal papilla or inside the gastric antrum. After positioning the gastroscope, endoscopic scissors (JHY-FG-23-180-A6, Changzhou Jiuhong Medical Instrument Co., Ltd., Jiangsu, China) were used under direct visualization to precisely cut the nasobiliary tube. The remaining portion of the nasobiliary tube was retained within the bile duct to transition from external to internal drainage (Figure 2(b)). The success of the procedure was defined as the successful cutting of the nasobiliary tube at the intended location under endoscopic guidance without complications. Failure was defined as the inability to cut the tube at the intended site or the occurrence of complications during or after the procedure, including tube dislodgment, bile leakage, and so on. In the conventional stent group, plastic or metal biliary stents are placed based on the patient’s medical history, Bismuth-Corlette classification, and personal and family preferences (Figure 2(c)). In the context of bilateral biliary stenting, following ERCP-guided cholangiography, two guidewires are superselectively advanced into the left and right hepatic ducts, respectively. Subsequently, biliary stents (Advanix Biliary Stent, Boston Scientific Corporation, MA, USA) are placed into the left and right hepatic ducts. The endoscope physicians are chief physicians who are proficient in ERCP operation, have more than 10 years of ERCP operation experience, and the annual operation volume of ERCP is ⩾300 cases.

ERCP procedure. (a) ERCP-guided nasobiliary drainage. (b) Nasobiliary tube cutting as a biliary stent with endoscopy. (c) ERCP-guided biliary stent placement.
Outcome assessment
The primary outcome was the incidence of early postoperative cholangitis (<30 days). The diagnostic criteria for acute cholangitis refer to the diagnostic criteria of the 2013 and 2018 Tokyo Guidelines. 18
Secondary outcomes included drainage success rate, number of ERCP procedures, re-intervention rate, postoperative complications, and length of hospital stay. Drainage success was defined as a reduction of total bilirubin to less than 50% of the original preoperative level within 7 days after operation or 75% of the original preoperative level within 30 days after operation. The number of ERCP procedures was calculated as the total number of ERCP procedures including the first. Re-intervention refers to any endoscopic or percutaneous intervention performed after the first ERCP for drainage. Postoperative complications included pancreatitis after ERCP, hyperamylasemia, acute cholecystitis, gastrointestinal bleeding, stent migration, stent dislodgement, stent obstruction, gastrointestinal perforation, bile leakage, and intestinal obstruction. Post-ERCP pancreatitis is defined as abdominal pain accompanied by amylase levels elevated to at least three times the upper limit of normal, occurring more than 24 h after the ERCP procedure.19 –21 Hyperamylasemia refers to an elevated serum amylase level beyond the upper limit of normal. Acute cholecystitis is an acute inflammation of the gallbladder characterized by right upper quadrant pain, fever, and systemic inflammatory response. Gastrointestinal bleeding is the pathological loss of blood from any segment of the gastrointestinal tract. Stent migration, dislodgement, and obstruction refer to the stent migrating from its intended position becomes completely dislodged, or blocked, impairing biliary drainage.22,23 Gastrointestinal perforation is a full-thickness disruption of the gastrointestinal tract wall. Bile leakage is the abnormal extravasation of bile from the biliary system into the peritoneal cavity or surrounding tissues. Intestinal obstruction is a mechanical or functional blockage of the intestinal lumen, leading to abdominal distension, pain, and potential compromise of bowel viability. The details of the nasobiliary tubes and stents are provided in Tables S1 and S2.
Patients were further categorized into the postoperative cholangitis group and the non-postoperative cholangitis group based on the occurrence of postoperative cholangitis. Univariate and multivariate analyses were conducted between the two groups to investigate the risk factors for postoperative cholangitis.
Statistical analysis
The software IBM SPSS 26.0 was utilized to carry out the statistical analysis. Shapiro–Wilk test was used for normality. The measurement data of normal distribution were represented by the mean and standard deviation (
Results
Baseline
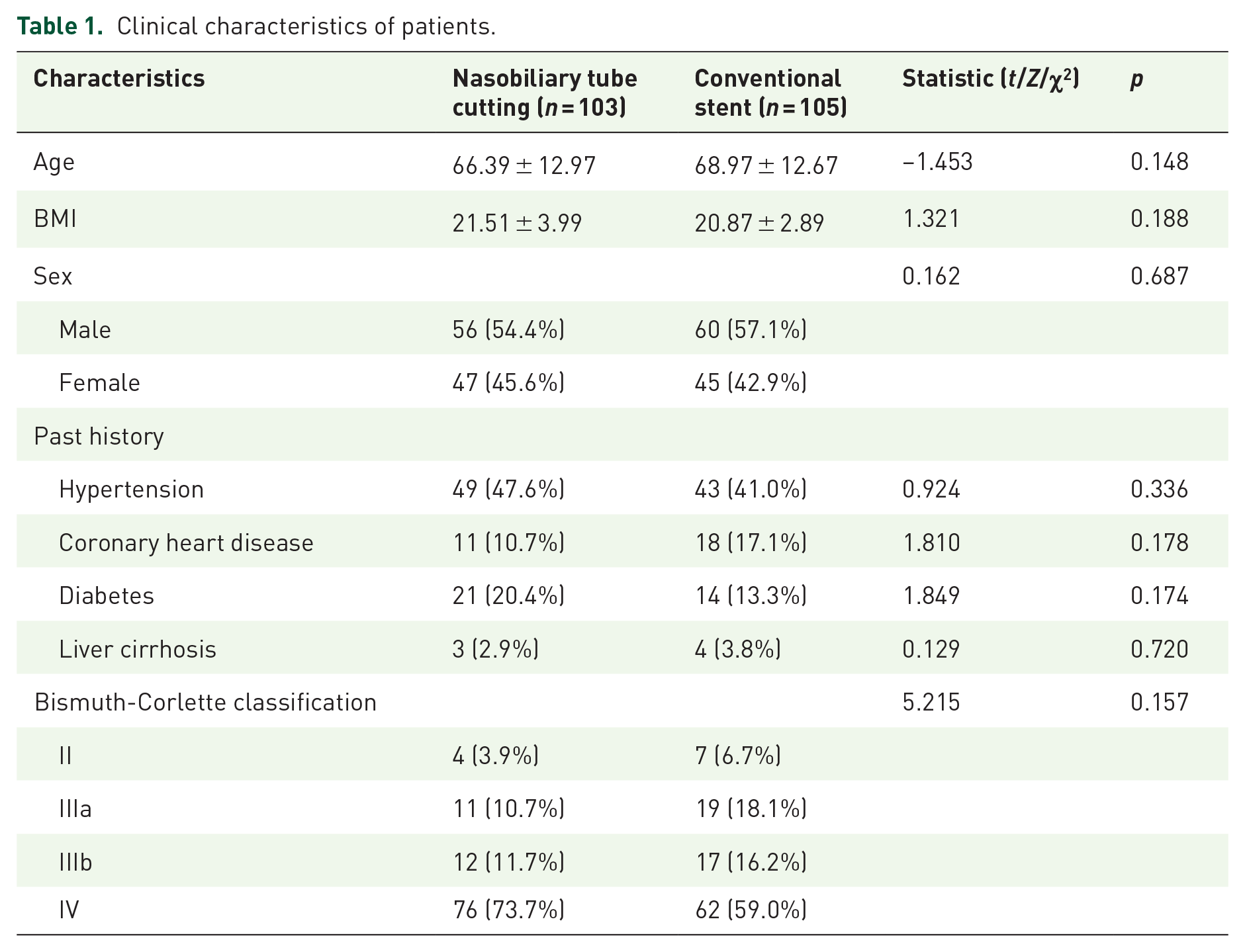
A total of 208 patients were included in this study, with 103 patients in the nasobiliary tube cutting group and 105 patients in the conventional stent group. The basic clinical characteristics of patients in the two groups are shown in Table 1.
Clinical characteristics of patients.
Laboratory parameters and ERCP procedures
Preoperatively, there were no statistically significant differences in laboratory parameters between the nasobiliary tube cutting group and the conventional stent group (p > 0.05). Postoperatively, compared to the conventional stent group, the nasobiliary tube cutting group showed significant reductions in TBil (79.1 μmol/L vs 123.7 μmol/L, p = 0.001), DBil (59.7 μmol/L vs 95.9 μmol/L, p < 0.001), and AST (50.0 U/L vs 63.0 U/L, p = 0.007). When comparing preoperative and postoperative changes in laboratory parameters, statistically significant differences were observed between the two groups in terms of AST and ALP intergroup comparisons (p < 0.05, Table 2). There were significant changes in ALT, AST, GGT, ALP, TBil, and DBil in the intragroup comparison within each group (p < 0.01).
Laboratory parameters of patients.

p < 0.05.
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; CRP, C-reactive protein; CT, computed tomography; DBil, direct bilirubin; EPBD, endoscopic papillary balloon dilatation; ERCP, endoscopic retrograde cholangiopancreatography; EST, endoscopic sphincterotomy; EUS, endoscopic ultrasonography; EUS-BD, EUS-guided biliary drainage; FFA, free fatty acid; GGT, γ-glutamyl transpeptidase; MRCP, magnetic resonance cholangiopancreatography; PTBD, percutaneous transhepatic biliary drainage; PTCD, percutaneous transhepatic cholangial drainage; TBil, total bilirubin; TC, total cholesterol; TG, triglyceride; WBC, white blood cell.
We compared the endoscopic treatment outcomes between the two groups and found no significant differences in the number of ERCP procedures, management of the duodenal papilla, and the number of reintervention (p < 0.05, Table 3). For reintervention, 14 patients in the nasobiliary tube cutting group underwent endoscopic re-placement of nasobiliary drainage, while 4 required PTBD. In the conventional stent group, 14 patients underwent endoscopic re-placement of stents, and 2 required PTBD.
ERCP procedures of patients.

Number of treatment procedures.
EPBD, endoscopic papillary balloon dilatation ERCP, endoscopic retrograde cholangiopancreatography; EST, endoscopic sphincterotomy.
Outcomes
Postoperative cholangitis was the primary observation outcome in this study. A total of 40 patients developed postoperative cholangitis, with 12 cases (11.7%) in the nasobiliary tube cutting group and 28 cases (26.7%) in the conventional stent group, showing a statistically significant difference between the groups (p = 0.006). In the subgroup analysis of patients with Bismuth-Corlette type IV classification (Table S3), the incidence of postoperative cholangitis was significantly lower in the nasobiliary tube cutting group compared to the conventional stent group (9.2% vs 40.3%, p < 0.001). The onset time of postoperative cholangitis was longer in the nasobiliary tube cutting group compared to the conventional stent group, although the difference between the groups was not statistically significant (5.5 days vs 3.0 days, p = 0.074). The majority of patients in both groups developed acute cholangitis within 7 days post-operation and experienced improvement with treatment, but the differences between the two groups were not statistically significant (Table 4).
Outcomes of patients.

p < 0.05.
TBil, total bilirubin.
In terms of drainage, 84 cases (81.6%) in the nasobiliary tube cutting group and 78 cases (74.3%) in the conventional stent group achieved successful drainage. A higher percentage of patients in the nasobiliary tube cutting group reached a reduction of TBil to less than 50% of the baseline within 7 days compared to the conventional stent group (p = 0.002). In addition, the nasobiliary tube cutting group required less time to achieve a decrease in TBil to less than 75% of the baseline (p = 0.021). Except for postoperative cholangitis, other postoperative complications were comparable between the groups (p > 0.05). Regarding the postoperative length of hospital stay, the nasobiliary tube cutting group had a longer duration than the conventional stent group (10.0 days vs 7.0 days, p = 0.024).
Risk factors for postoperative cholangitis
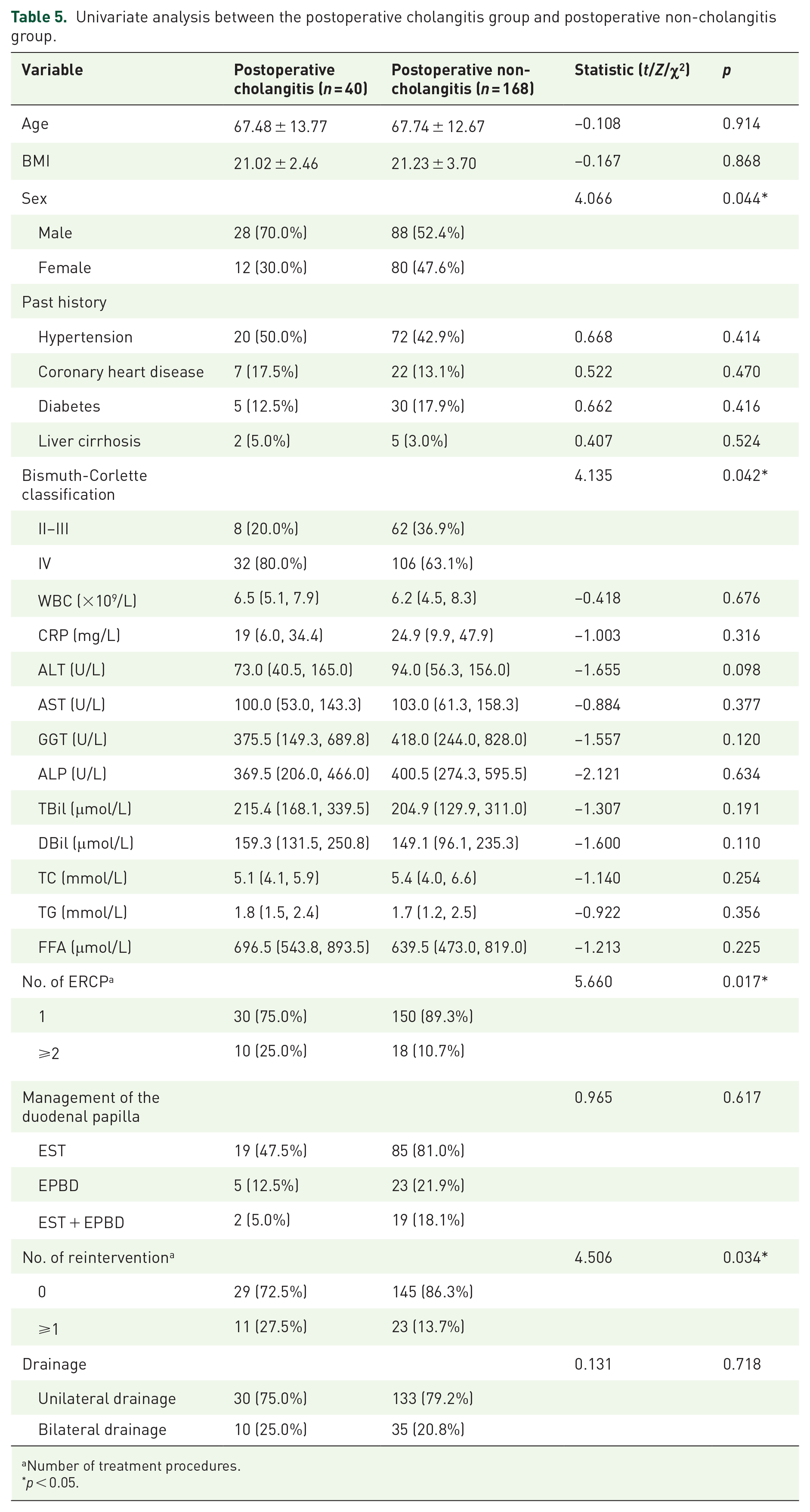
To further analyze the risk factors for postoperative cholangitis, patients were categorized into two groups based on the occurrence of postoperative cholangitis: the postoperative cholangitis group and the postoperative non-cholangitis group (Table 5).
Univariate analysis between the postoperative cholangitis group and postoperative non-cholangitis group.
Number of treatment procedures.
p < 0.05.
Regarding clinical characteristics, there were 28 cases of males (70.0%) in the postoperative cholangitis group, whereas in the postoperative non-cholangitis group, there were 88 cases of males (52.4%), indicating a statistically significant difference between the two groups (p = 0.044). Concerning the Bismuth-Corlette classification, there were 32 cases of type IV patients (80.0%) in the postoperative cholangitis group and 106 cases (63.1%) in the postoperative non-cholangitis group, showing a statistically significant difference (p = 0.042). There were no statistically significant differences between the two groups in terms of age, BMI, and underlying diseases (p > 0.05). The differences in laboratory indicators such as WBC, CRP, ALT, AST, GGT, ALP, TBil, DBil, TC, TG, and FFA between the two groups were not statistically significant (p > 0.05). In the context of ERCP procedures, among patients who developed postoperative cholangitis, 10 (25.0%) underwent the ERCP procedure two or more times, compared to 18 (10.7%) in the group without postoperative cholangitis. This difference was statistically significant (p = 0.017). Furthermore, the requirement for one or more reinterventions was observed in 11 (27.5%) patients in the postoperative cholangitis group and 23 (13.7%) patients in the non-cholangitis group, again showing a statistically significant difference (p = 0.034). However, the approaches to treating the duodenal papilla did not differ significantly between the two groups (p > 0.05).
Utilizing risk factors that were deemed statistically significant (p < 0.05) in the univariate analysis, a multivariate logistic regression model was developed. The analysis revealed that the Bismuth-Corlette classification, specifically type IV (OR = 3.207, 95%CI: 1.253–8.210, p = 0.015), serves as an independent predictor for post-ERCP cholangitis (Table 6).
Multivariate logistic regression analysis of postoperative cholangitis.

Number of treatment procedures.
p < 0.05.
Discussion
Recent studies have demonstrated that, under conditions of unobstructed biliary flow, there is no significant difference in drainage effectiveness between nasobiliary tubes and conventional stents; both can achieve optimal drainage outcomes.24,25 However, this study’s findings indicate that the group with nasobiliary tube cutting may have potential advantages in alleviating jaundice and improving liver function. Compared to conventional stents, nasobiliary tubes offer several drainage benefits. First, they have more side holes and a larger drainage area, facilitating bile flow. In addition, their flexible material allows for easier entry into angled bile ducts, and they can be placed in the secondary bile ducts, further enhancing drainage efficiency.26 –31 Second, in this study, the early phase of external drainage through nasobiliary tubes allowed for postoperative observation of bile drainage, including the volume and characteristics of the bile. This enabled an analysis of the drainage effectiveness to guide further treatment directions. For instance, if the drainage through the nasobiliary tube was insufficient, issues such as occlusion, displacement, or poor drainage in the placement area were considered. Depending on the situation, measures like suction, flushing, or endoscopic intervention were employed to ensure the effectiveness of the nasobiliary drainage.
Acute cholangitis is one of the common complications following endoscopic drainage guided by ERCP, with a postoperative incidence rate generally between 5% and 40%.32 –34 In this study, patients with preoperative acute cholangitis were excluded to specifically investigate the incidence of postoperative cholangitis. Given the retrospective nature of the study, the exclusion of acute cholangitis was determined using the gold standard based on ERCP findings. The diagnostic criteria in Tokyo Guidelines 2013/2018, validated in numerous studies, offer good sensitivity and specificity for diagnosing acute cholangitis.35 –38 Patients with hilar malignant biliary strictures often exhibited biliary narrowing and liver function abnormalities, with malignancy and associated factors often causing elevated inflammatory markers, potentially leading to diagnostic bias. Therefore, to enhance the reliability of the study, acute cholangitis was excluded based on comprehensive clinical evaluation and ERCP findings. In this study, the incidence of postoperative cholangitis in the nasobiliary tube cutting group (11.7%) was lower than that in the conventional stent group (26.7%), with a statistically significant difference between the two groups (p = 0.006). This outcome suggests that the operation of cutting nasobiliary tubes may be associated with a reduction in the incidence of postoperative cholangitis. Jiang et al. conducted a retrospective study to investigate the effectiveness of endoscopically cutting nasobiliary tubes as an alternative to biliary stenting in the treatment of cholangiocarcinoma at the hepatic hilum. Their findings indicated a significantly lower incidence of cholangitis in the nasobiliary tube cutting group compared to the ERBD group (15.40% vs 41.4%, p < 0.05). 39 Research by Kawakami et al. revealed that, in the treatment of cholangiocarcinoma at the hepatic hilum, ENBD significantly reduced the incidence of postoperative cholangitis compared to endoscopic biliary stent drainage. 40 Zhang et al. conducted a systematic review and meta-analysis to explore the outcomes of endoscopic nasobiliary drainage versus endoscopic biliary stent placement and drainage. Including nine studies, the results showed that endoscopic nasobiliary drainage significantly reduces the incidence of cholangitis. 41 Maeda and colleagues found that preoperative endoscopic nasobiliary drainage significantly reduces the incidence of cholangitis in patients with cholangiocarcinoma at the hepatic hilum. 42 Wan and associates conducted a retrospective study that revealed that temporary nasobiliary drainage following endoscopic metal stent placement, compared to the sole placement of an endoscopic metal stent, can prevent the occurrence of postoperative cholangitis. 43 The reduction of postoperative cholangitis through endoscopic nasobiliary drainage can be attributed to several factors. First, nasobiliary tubes are characterized by their large drainage capacity and high efficiency, which enable early and sufficient drainage to prevent infection caused by bile accumulation. In addition, the early phase of external drainage through nasobiliary tubes allows for the collection of bile samples and microbiological testing, which can guide postoperative treatment based on the results, thereby preventing cholangitis to some extent. Furthermore, the external drainage phase of nasobiliary tubes offers direct feedback on the bile drainage situation. If drainage is found to be inadequate, measures such as suction or flushing can enhance drainage. Clinically, flushing with saline solution mixed with antibiotics is also used, which can further prevent the occurrence of postoperative cholangitis. Postoperatively, there was no significant statistical difference between the two groups in the incidence of other complications, such as post-ERCP pancreatitis, hyperamylasemia, acute cholecystitis, gastrointestinal bleeding, issues with the stent post-operation, and gastrointestinal perforation. This result is consistent with previous studies.44,45 Building on this, our findings further complement existing literature by providing the role of nasobiliary tube cutting as an effective strategy in transitioning from external to internal drainage while maintaining low rates of cholangitis. However, given the retrospective design of this study, caution is warranted in interpreting these results. While they align with and extend the observations of prior studies, future research is needed to validate the benefits of nasobiliary tube cutting in reducing cholangitis and improving drainage outcomes.
The postoperative hospital stay was significantly longer in the nasobiliary tube cutting group, with a median duration of 10.0 (7.0, 14.0) days compared to 7.0 (5.5, 12.5) days in the conventional stent group (p = 0.024). The longer hospital stay in the nasobiliary tube cutting group was likely due to the need to assess the effectiveness of nasobiliary drainage and ensure patient stability before performing the cutting procedure. Although the extended hospital stay may add to the healthcare burden, it allowed for close monitoring of drainage success and early detection of complications, which potentially reduced the need for additional re-interventions. This trade-off between hospital stay and patient outcomes warrants further investigation to optimize treatment protocols and improve overall efficiency.
To further investigate the factors influencing postoperative cholangitis, patients were divided into two groups: the postoperative cholangitis group and the postoperative non-cholangitis group. The results indicated significant differences between the two groups in terms of gender, Bismuth-Corlette classification, number of ERCP procedures, and number of reinterventions. Multivariable logistic regression analysis suggested that Bismuth-Corlette type IV is a potential independent risk factor for the occurrence of postoperative cholangitis. Bismuth-Corlette type IV refers to tumors that involve the common hepatic duct, the confluence of the left and right hepatic ducts, and bilateral hepatic ducts. Sugiura et al. conducted a retrospective clinical study, which indicated that Bismuth-Corlette type IV is one of the risk factors affecting endoscopic biliary drainage. 46 The reasons that this classification may influence the occurrence of postoperative cholangitis include several aspects. First, this type involves a higher degree of stenosis at the hepatic hilum, which can increase the difficulty of the endoscopic procedure, thereby extending the operation time and increasing the risk of infection. Second, endoscopic operations in this classification are often more challenging, with the likelihood of repeated maneuvers during the operation, increasing the probability of bile duct mucosal damage and bacterial infection. Furthermore, despite the placement of stents for drainage under endoscopy, the effectiveness of bile drainage may still be less than ideal, potentially leading to the progression of bile accumulation and thus increasing the risk of infection.
This study still has limitations. As a single-center retrospective study, there might be selection bias, and the quality and accuracy of data included in retrospective studies may also raise concerns, both of which could lead to inaccuracies in statistical analysis. The lack of long-term follow-up also limits our ability to assess the sustainability of the observed benefits across diverse clinical scenarios and patient populations. Another limitation of this study is the 2–7 days interval for nasobiliary tube cutting, chosen based on clinical experience to ensure adequate drainage and patient stabilization after ENBD. However, the lack of validation from standardized guidelines or prospective studies may limit its generalizability. Future research should explore the optimal timing for this transition to establish evidence-based recommendations. In this study, statistical methods were chosen based on data distribution and type to ensure validity. Multivariable logistic regression included significant factors from univariable analysis to assess independent associations and control for potential confounding. We acknowledge that excluding non-significant factors from univariable analysis may have omitted potential confounders, and residual confounding is possible due to unmeasured variables. This study does not include patient stratification based on the Blumgart Preoperative Staging System for hilar cholangiocarcinoma. While the primary objective was to evaluate the outcomes of nasobiliary tube cutting versus conventional stenting in patients with hilar malignant biliary stricture, data regarding whether the drainage was performed for palliative or preoperative purposes were not collected. The absence of such stratification may limit the generalizability of the findings, as treatment outcomes could vary depending on the stage and resectability of the disease.
These limitations could affect the external validity of the findings when applied to different healthcare settings. Future research should aim to conduct multicenter, large-sample prospective randomized controlled trials to further clarify the effectiveness of nasobiliary tube cutting procedures in reducing the incidence of postoperative cholangitis.
Conclusion
In conclusion, for patients with hilar malignant biliary stricture, nasobiliary drainage followed by sequential cutting of the nasobiliary tube may be associated with a reduction in the incidence of postoperative cholangitis. This procedure may facilitate early bile drainage, providing potential benefits in managing biliary obstruction. However, it may be associated with a longer hospital stay compared to conventional stent drainage. While the overall success rate of drainage is comparable between the two methods, there was no significant difference in the incidence of other complications. Further research is needed to validate these findings in larger, multicenter prospective studies. In addition, the identification of Bismuth-Corlette type IV as an independent risk factor for postoperative cholangitis underscores the importance of risk stratification in the management of hilar malignant biliary stricture.
Supplemental Material
sj-doc-1-tag-10.1177_17562848251319809 – Supplemental material for Efficacy and safety of sequential cutting of nasobiliary tubes as an alternative to stent placement after nasobiliary drainage for the treatment of hilar malignant biliary stricture: a retrospective cohort study
Supplemental material, sj-doc-1-tag-10.1177_17562848251319809 for Efficacy and safety of sequential cutting of nasobiliary tubes as an alternative to stent placement after nasobiliary drainage for the treatment of hilar malignant biliary stricture: a retrospective cohort study by Wangyang Chen, Peiyao Huang, Xinyi Gu, Xiaodie Liu, Xiuzhiye Ying and Jianfeng Yang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848251319809 – Supplemental material for Efficacy and safety of sequential cutting of nasobiliary tubes as an alternative to stent placement after nasobiliary drainage for the treatment of hilar malignant biliary stricture: a retrospective cohort study
Supplemental material, sj-docx-2-tag-10.1177_17562848251319809 for Efficacy and safety of sequential cutting of nasobiliary tubes as an alternative to stent placement after nasobiliary drainage for the treatment of hilar malignant biliary stricture: a retrospective cohort study by Wangyang Chen, Peiyao Huang, Xinyi Gu, Xiaodie Liu, Xiuzhiye Ying and Jianfeng Yang in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.