
Abstract
Background:
Ulcerative colitis (UC), a chronic and relapsing inflammatory bowel disease, has long depended on physician-led objective evaluations for clinical management. However, physicians’ assessments of symptoms often differ from patients’ subjective experiences, creating a cognitive gap that may influence treatment decisions and overall disease outcomes.
Objective:
This study aimed to compare the cognitive discrepancy between UC patients and gastroenterologists throughout the diagnosis and treatment process.
Design:
Multicenter retrospective study.
Methods:
A nationwide survey was conducted across 39 Inflammatory Bowel Disease centers in China using a convenience sampling method, enrolling 457 UC patients and 170 gastroenterologists. A two-way questionnaire survey was administered to both groups to assess perceptions of disease status, treatment goals, medication use, follow-up preferences, economic burden, and decision-making models.
Results:
This multicenter study identified significant cognitive gaps between UC patients and gastroenterologists across key domains of disease management. Physicians prioritized objective clinical indicators such as hematochezia (51.18% vs 41.58%, p = 0.031), whereas patients emphasized subjective symptoms like rectal urgency (19.69% vs 4.12%, p < 0.001). Treatment goals also differed: patients valued quality-of-life improvement most, while physicians ranked endoscopic mucosal healing highest. Discrepancies extended to follow-up, with physicians favoring bi-monthly visits and patients preferring intervals exceeding 6 months. In decision-making, although 47.06% of physicians supported shared decision-making, only 10.72% of patients endorsed this model (p < 0.001). Notably, patients’ willingness to allocate >50% of household income to treatment (21.44%) substantially surpassed physicians’ expectations (5.29%, p < 0.001).
Conclusion:
These findings indicate a clear disconnect between current clinical management approaches and the lived experience of patients with UC in China. To bridge this gap, practice must shift toward models that actively integrate patient priorities into treatment plans.
Plain language summary
This study reveals significant perceptual gaps between ulcerative colitis patients and gastroenterologists regarding symptoms, treatment goals, follow-up, and decision-making. It highlights the urgent need for enhanced communication and patient-centric care strategies.
Introduction
Ulcerative colitis (UC) is a chronic inflammatory bowel disease characterized by persistent inflammation and damage to the colorectal mucosa. 1 With evolving lifestyles and environmental changes, the incidence of UC in China and other newly industrialized countries has risen sharply, entering an “accelerated incidence phase.” The associated disease burden continues to intensify, severely compromising patients’ physical and mental health and imposing substantial healthcare and economic costs. This situation poses a major challenge to the healthcare system.
As the UC patient population continues to expand, developing a scientifically robust and clinically effective framework for disease assessment and management has become a central priority. Currently, the clinical evaluation of UC typically integrates multidimensional indicators, including clinical manifestations, endoscopic findings, biological markers, and histological examinations, while patient-reported outcomes are also gaining increasing attention. 2 However, the existing assessment framework remains predominantly physician-centric, 3 and patients’ subjective experiences and individualized needs have not yet been fully incorporated into it. The relapsing nature of UC and the diversity of treatment options may lead to cognitive differences—defined as a systematic divergence in perspectives, priorities, and expectations between patients and physicians arising from their distinct roles and sources of information regarding disease concerns, treatment goals, and decision-making preferences—which can subsequently influence disease management, satisfaction, and adherence. 4 Previous studies have consistently indicated discrepancies in perspectives and opinions between patients and physicians regarding colitis, its management, and specific therapeutic approaches.5,6 For instance, the UC: New Observations on Remission, Management and Lifestyle (UC: NORMAL) survey found that physicians often underestimated the disease burden experienced by patients, while many patients perceived their own symptoms or disease relapses as “normal.” 6
In terms of treatment strategies, the management philosophy for UC has gradually shifted from the traditional “step-up treatment” 7 to an evidence-based “treat-to-target” approach. 8 This strategy not only focuses on short-term symptom control but also emphasizes achieving mucosal healing and normalization of inflammatory markers (such as C-reactive protein and fecal calprotectin) as medium-to-long-term treatment goals, 9 aiming for a more comprehensive disease control. Yet, studies have suggested that physicians often underestimate the impact of the disease on patients’ quality of life during clinical decision-making and fail to fully recognize patients’ core concerns. Therefore, promoting consensus between physicians and patients on treatment goals and implementing shared decision-making through effective communication have become key components in optimizing the management of UC. 10 Currently, research on physician–patient cognition and decision-making models primarily originates from Western populations.6,11 As the largest developing country, China differs significantly from Western nations in terms of its healthcare system, cultural background, and health beliefs, which limit the direct applicability of Western findings in the Chinese context. Moreover, existing studies are mostly confined to binary comparisons between physician and patient groups and lack in-depth analysis of the cognitive structures among physicians of different professional titles (e.g., residents, attending physicians, and associate chief physicians or above) and patients with varying healthcare statuses (e.g., outpatient and inpatient). These gaps hinder the development of targeted intervention strategies.
Based on the aforementioned research gaps, we conducted a multicenter retrospective survey to systematically assess the similarities and differences between Chinese UC patients and gastroenterologists in terms of disease cognition, treatment goals, and physician–patient relationships. Breaking from the traditional binary physician–patient comparison, this study is the first to integrate physicians across professional tiers and patients across care settings within a large-scale sample, revealing the complex structure of physician–patient cognitive differences from multiple dimensions. Our findings aim to provide a theoretical foundation for constructing a patient-centered, clinically practical UC management pathway.
Methods
Study design and participant recruitment
This multicenter study was conducted from July 2020 to July 2021 across 39 IBD centers in China. Physicians were recruited using a convenience sampling method (Registered at ClinicalTrials.gov, Registration Number: ChiCTR2000034872). Eligible physicians who were capable of diagnosing, identifying, and treating UC were recruited to complete a structured questionnaire. The participating physicians then recruited outpatient or inpatient UC patients who met the inclusion criteria. The inclusion criteria for patients were (1) followed up by the same physician for >1 year, with ⩾1 visit in the first 6 months; (2) receiving treatment regimens recommended by the Third European Evidence-based Consensus on Diagnosis and Management of UC 12 ; (3) able to complete the questionnaire independently. The exclusion criteria for patients were (1) females who were pregnant or lactating; (2) involved in the recruitment activities of this survey; (3) had changes in their treatment regimen within the 2 weeks prior to the survey; (4) had a history of partial or total colectomy; (5) diagnosed with malignant tumors or severe comorbidities affecting systems other than the digestive tract (e.g., cardiovascular, hepatic, renal, pulmonary, hematological, endocrine); or (6) presence of psychiatric disorders or cognitive impairment (Figure 1(a)).

Physician and patient perceptions of UC disease status. (a) Study flowchart. (b–d) Focus of UC concerns—physicians versus patients, outpatients versus inpatients, physicians by professional title. (e) Disease control status (past year). (f–h) Understanding of disease remission—physicians versus patients, outpatients versus inpatients, physicians by title.
Ethical considerations
The study protocol was reviewed and approved by the Ethics Committee of Xijing Hospital, Fourth Military Medical University (Xi’an, China; Approval No.: ChiECRCT20200202) and the ethics committees of all participating centers. The survey was strictly conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. All physicians and patients provided written informed consent. Additionally, the study design and reporting procedures of this study complied with all specifications of the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). 13
Questionnaire design and implementation
This study was based on the Crohn’s and Colitis Knowledge Score (CCKNOW) 14 and the Inflammatory Bowel Disease Knowledge Assessment Device 2 (IBD-KID2). 15 The questionnaires were revised under the direction of the head of the Chinese Society of IBD and the Chinese Medical Association, and were reviewed by 10 IBD experts to compare disease cognition differences between UC patients and physicians. The physician questionnaire comprised 74 questions across 4 domains: basic information, symptom cognition, medication therapy, and physician–patient relationships (Supplemental Appendix 1). The patient questionnaire included 95 questions spanning 5 domains: basic information, symptom cognition, medication therapy, physician–patient relationships, and quality of life (Supplemental Appendix 2). The quality of life was assessed using the SF-36 Health Survey, which covers physical, psychological, social, and environmental dimensions.
Prior to data collection, all participating doctors and researchers underwent centralized training and consistency was assessed through simulated case tests. During the study, the research team monitored progress through regular meetings, online supervision, and data consistency checks (including calculation of the Kappa coefficient) to ensure the consistency of results across centers and doctors. The electronic system also featured an outlier detection function to flag potential biases in physician assessments and analyzed the completion times to identify abnormal patterns. Finally, some patients provided feedback after completing the questionnaires, which helped further optimize the clarity and acceptability of the questionnaires.
This study strictly adhered to the design process of “pilot testing, optimization, and formal study.” All participants in the formal study completed the final version of the questionnaire, which was optimized through pilot testing. We added additional information to the basic details of the patient and physician questionnaires, such as initials and contact numbers, to facilitate better follow-up and data tracking. These additions did not alter the core assessment questions of the questionnaire, and therefore did not impact its validity as a validation tool. For data collection, a pilot test was conducted with five doctors and five patients before the official launch, modifying the questionnaires based on their feedback. After their outpatient visits, patients immediately filled out the questionnaires in a private room at the hospital to ensure data independence and accuracy and minimize external interference. Patients could request assistance from the hospital staff when needed to ensure smooth completion of the questionnaires. The doctors completed the corresponding questionnaires based on their clinical observations after the patient’s visit. All questionnaires were designed using standardized and easily understandable language and underwent three rounds of pilot testing to ensure consistent comprehension. The questionnaires were distributed via an electronic system that tracked completion time and automatically sent reminders.
Assessment of disease classification and clinical manifestations
The Montreal classification was determined based on colonoscopy and pathological biopsy findings, primarily according to the maximal extent of inflammation: E1 (proctitis), E2 (left-sided colitis), and E3 (extensive colitis). Extraintestinal manifestations were identified through a systematic clinical evaluation, which included (1) targeted collection of medical history regarding joint, mucocutaneous, ocular, and hepatobiliary symptoms; (2) documentation of physical examination findings; (3) review of existing specialist records (e.g., imaging reports, diagnoses from rheumatology, dermatology, ophthalmology, or hepatology departments); and (4) referral of patients to appropriate specialty clinics for further confirmation when clinical suspicion existed without definitive prior documentation.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics 26.0 (IBM Corp., Armonk, NY, USA) and RStudio 4.3.2 (Posit Software, PBC, Boston, MA, USA). Data collected in the study were primarily summarized and analyzed using descriptive statistical methods. To thoroughly investigate the cognitive differences between UC and their treating physicians across multiple aspects—including disease cognition, treatment goals, and disease burden—the core analysis focused on comparisons between the physician and patient groups. Categorical variables were compared using the Chi-square test or Fisher’s exact test, as appropriate. Comparisons of continuous variables between two groups that followed a normal distribution were conducted using the independent samples t test. In contrast, the Mann–Whitney U test or the Kruskal–Wallis H test was used for continuous variables that did not follow a normal distribution. All statistical analyses employed two-tailed tests, with a p value < 0.05 considered statistically significant.
Results
Demographic characteristics
A total of 536 UC patients from 24 provinces and cities across China were enrolled, with 457 completing the survey. Among the completers, 363 were outpatient patients and 94 were inpatient patients. Male patients accounted for 257 cases (56.24%). Most patients (92.56%) were aged 19–60 years. Urban residents constituted the largest proportion (67.61%), while those residing in rural and urban–rural junction areas accounted for the remaining 32.39%. A total of 180 patients (63.89%) had a higher education background (undergraduate degree or above). The majority of patients (70.24%) had a low- to middle-income, earning less than 6000 RMB (approximately $860 USD) per month. Only 6.35% of patients reported a family history of UC, among whom 55.17% were first-degree relatives (parents or children). The most common type of UC lesion was extensive colitis (E3; 42.23%). Regarding disease activity, 46.61% of patients had active disease, primarily moderate to severe in nature. Extraintestinal manifestations were present in 6.35% of patients, with erythema nodosum (2.41%) and ankylosing spondylitis (2.19%) being the most frequent. Nearly half of patients (49.67%) had been diagnosed within the 6 months preceding the survey. Regarding current medication therapy, the three most frequently used drugs were 5-aminosalicylic acid (77.68%), probiotics (28.88%), and biologics (27.13%).
A total of 170 physicians participated in the survey, with associate chief physicians or higher comprising 45.29%. Among them, 169 physicians (99.41%) were from Class A tertiary hospitals, and 95.29% specialized in UC research. Furthermore, 82.35% had more than 2 years of independent clinical experience, and 92.94% reported prior experience with biologic prescribing. The detailed demographic and professional characteristics of patients and physicians are summarized in Tables 1 and 2, respectively.
Demographic and baseline characteristics of patients with UC.

UC, ulcerative colitis.
Demographic and baseline characteristics of the physicians.
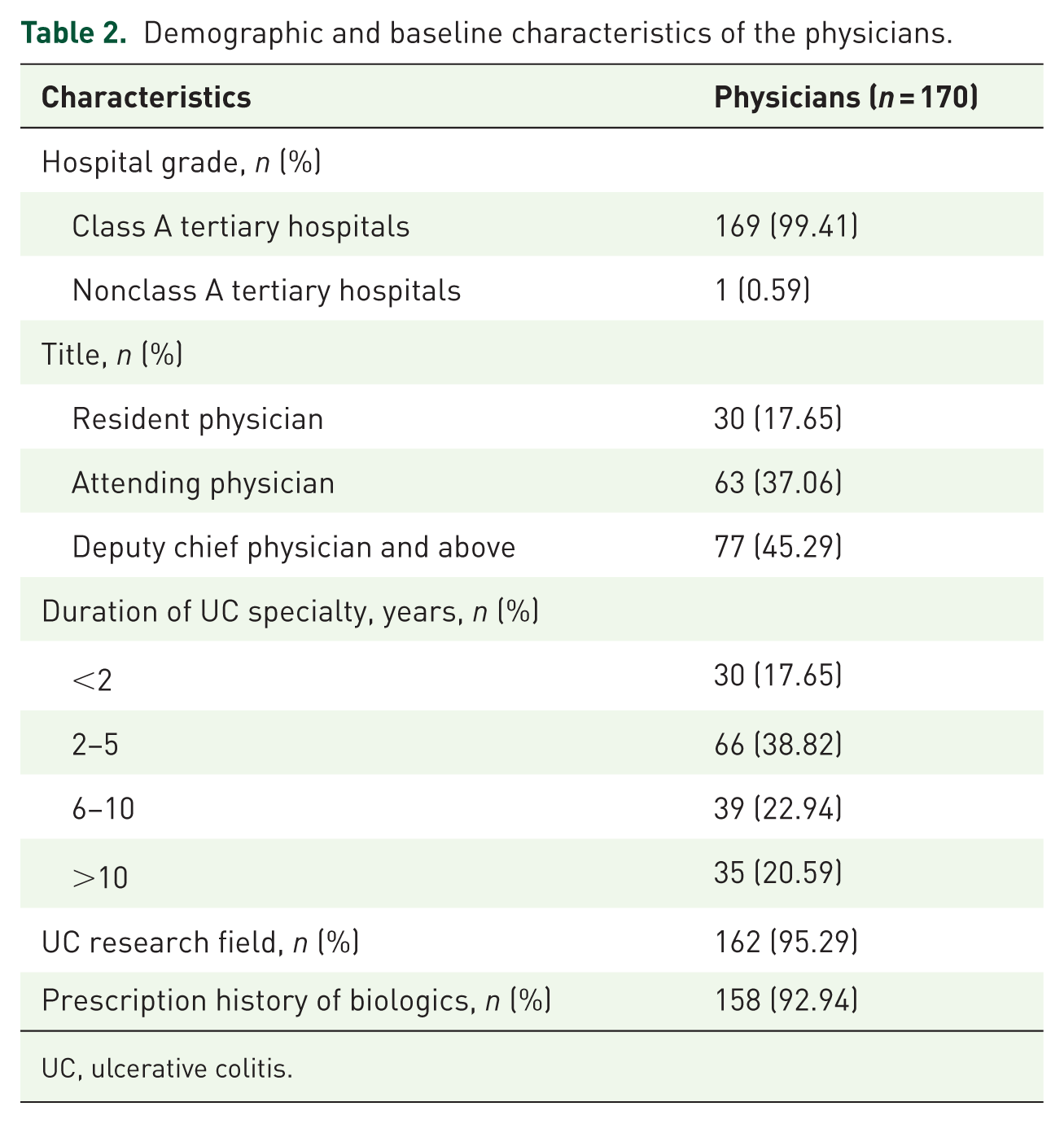
UC, ulcerative colitis.
Disease awareness
Our study identified significant differences in the focus of UC concerns between physicians and patients (Figure 1(b)): Physicians placed greater emphasis on objective clinical indicators, such as bloody stools (51.18% vs 41.58%, p = 0.031) and daily stool frequency (28.82% vs 12.04%, p < 0.001). In contrast, patients were more likely to report subjective symptomatic experiences, with the difference in perception of rectal urgency being particularly pronounced (19.69% vs 4.12%, p < 0.001). Further stratified comparisons revealed (Figure 1(c)) that outpatients were more concerned about bloody stools (42.70% vs 37.23%), abdominal pain (7.16% vs 3.19%), and the number of pills required for intake (3.86% vs 1.06%). In contrast, inpatients placed greater importance on daily stool frequency (15.96% vs 11.02%), rectal urgency (27.66% vs 17.63%), and the need for repeated medical visits (14.89% vs 13.22%). At the physician level (Figure 1(d)), the focus on the core objective sign “bloody stools” progressively increased with higher professional titles, rising from 36.67% among residents to 41.27% among attending physicians, and reaching 64.94% in the group of associate chief physicians and above. Conversely, attention to “daily stool frequency” was higher among residents (36.67%) and attending physicians (39.68%) but declined to 16.88% among senior physicians, suggesting that higher-ranking physicians concentrate more on core clinical indicators.
Further analysis revealed that this cognitive disparity directly influenced the assessment of disease status. Specifically, 30.20% of patients believed their UC symptoms were completely or mostly controlled over the past year, compared with physicians’ estimate of 40% (p = 0.02, Figure 1(e)). Among UC patients, 53.39% were in disease remission, while 46.61% had active disease. Notably, the proportion of patients with active disease was significantly higher among inpatients at 65.96%, far exceeding the 41.60% observed in outpatients, and their disease severity was more pronounced (Table 1). Regarding the perception of disease remission, physicians and patients demonstrated different priorities (Figure 1(f)): patients focused more on subjective experience indicators, such as treatment satisfaction (77.68%), whereas physicians emphasized objective biological markers, particularly the normalization of laboratory inflammatory indicators (92.94%). Stratified analysis further revealed that while both outpatients and inpatients highly valued treatment satisfaction, inpatients demonstrated greater recognition of objective remission criteria (e.g., steroid-free status: 56.38% vs 48.76%; normal endoscopy: 40.43% vs 34.71%, Figure 1(g)). Furthermore, as physician rank increased, there was a significant rise in the importance placed on deep remission targets such as mucosal healing and steroid-free status (Figure 1(h)).
Treatment target
There is a significant difference in the perception of treatment goals between physicians and patients (Figure 2(a)): the patient group most values “improving quality of life and returning to society” (31.29%), while the physician group lists “endoscopic mucosal healing” as the primary goal (40.00%). For symptom management, physicians place greater importance on “rapid control of abdominal pain and diarrhea” (31.18%) compared to patients (21.88%, p = 0.016). Regarding long-term management goals, physicians place greater importance on “long-term maintenance of disease remission” (16.47%), more than twice that of patients (7.44%, p < 0.001). Further subgroup analysis revealed that inpatients have a more urgent need for symptom control compared to outpatients (Figure 2(b)), with a greater emphasis on rapid control of abdominal pain and diarrhea (29.79% vs 19.83%) and a significantly reduced focus on long-term remission (2.13% vs 8.82%). Among physicians (Figure 2(c)), the importance of rapid symptom control increases with seniority: Resident Physicians (20.00%), Attending Physicians (26.98%), and Deputy Chief Physicians or above (38.96%).

Physician and patient perceptions of UC treatment goals and medication use. (a–c) Treatment goals—physicians versus patients, outpatients versus inpatients, physicians by title. (d) Understanding of medication therapy. (e) Satisfaction with medication therapy. (f) Concerns about corticosteroid therapy. (g–i) Corticosteroid side effects—physicians versus patients, outpatients versus inpatients, physicians by title. (j, k) Understanding of biologics and safety. (l–n) Biologic side effects—physicians versus patients, outpatients versus inpatients, physicians by title.
The majority of patients (84.25%) have some or a very good understanding of UC-related drug therapy (Figure 2(d)). Further analysis revealed that 79.43% of patients are satisfied with the current treatment plan (Figure 2(e)). In terms of treatment composition, traditional treatment regimens still dominate, with 77.68% of patients adopting a treatment strategy primarily based on oral 5-ASA. Analysis of glucocorticoid use found that only 13.13% of patients have received hormone therapy (Table 1). Notably, concern about hormone-related harms is significantly higher among patients (89.27%) than among physicians (54.71%, p < 0.001; Figure 2(f)). Among those treated with hormones, 57.33% experienced adverse events (Figure 2(g)), most commonly weight gain (33.92%), osteoporosis (25.82%), skin changes (24.73%), and psychiatric symptoms (21.66%). Both outpatients and inpatients, as well as physicians of various titles, consider weight gain to be the primary side effect (Figure 2(h) and (i)). Additionally, the usage rate of biologics in UC patients is approximately 27.13% (Table 1). In the assessment of biologics cognition (Figure 2(j)), physicians significantly overestimated patients’ understanding (76.47% vs 47.92%, p < 0.001). Regarding biologics safety (Figure 2(k)), 42.45% of patients indicated understanding, whereas physicians overestimated this proportion (71.76%), p < 0.001. The results from Figure 2(l) to (n) show that both inpatients and outpatients are most concerned about the risk of malignant tumors/lymphoma (62.80%), while resident and attending physicians focus on the risk of serious infection (36.47%), and senior physicians prioritize the risk of new or recurrent tuberculosis (33.77%).
Diagnosis and treatment mode
During the diagnostic phase, patients generally faced significant diagnostic delays, with more than 50% reporting misdiagnoses and over 25% undergoing three or more consultations before confirmation (Table 1). Regarding current treatment management (Figure 3(a)–(c)), 96.06% of patients (both outpatient and inpatient) and 98.82% of physicians (across different professional titles) consistently identified “frequent medical visits impacting work/studies” as the most troubling issue (p = 0.122). Further analysis of follow-up patterns (Figure 3(d)–(f)) revealed that although most physicians and patients in principle agreed with “regular follow-up,” clinical practice showed clear stratification: physicians at the associate chief level and above believed in adhering to the principle of “regular follow-up” (66.23%), whereas patients treated by residents primarily adopted a response-driven follow-up model (i.e., seeking medical attention only upon discomfort or onset of symptoms, accounting for 73.33%). Regarding preferences for follow-up frequency (Figure 3(g)–(i)), a significant cognitive disparity existed between physicians and patients: most outpatients (63.09%) and inpatients (59.57%) preferred intervals ⩾6 months, whereas physicians across all ranks recommended follow-up every 2 months (residents 46.67%, attending physicians 46.03%, senior physicians 55.84%).

Physician and patient perceptions of diagnosis and treatment models. (a–c) Troublesome issues in current consultation model—physicians versus patients, outpatients versus inpatients, physicians by title. (d–f) Perceptions of follow-up models—physicians versus patients, outpatients versus inpatients, physicians by title. (g–i) Perceptions of follow-up frequency—physicians versus patients, outpatients versus inpatients, physicians by title. (j–l) Treatment decision-making—physicians versus patients, outpatients versus inpatients, physicians by title.
In the choice of treatment decision-making models, physicians and patients exhibited different inclinations (Figure 3(j)). The patient cohort leaned toward more passive or semi-passive decision-making roles, primarily selecting “autonomous decision-making after physician recommendation” (47.26%) and “physician-dominated decision-making” (42.01%). In contrast, physicians strongly advocated for shared decision-making (47.06% vs 10.72%, p < 0.001). Further stratified analysis found that both outpatient and inpatient patients (Figure 3(k)) favored “autonomous decision-making after physician recommendation” and “physician-dominated decision-making.” Conversely, physicians of different professional titles (Figure 3(l)) showed greater agreement with “having an equal partnership and making shared decisions” and “autonomous decision-making after physician recommendation.”
Disease burden and quality of life
This study further revealed the multifaceted burden of UC on patients’ quality of life, psychological well-being, and economic status. First, regarding quality of life, although most patients (65.21%) achieved IBDQ scores indicating “good or very good” quality of life, scores were significantly lower among patients without mucosal healing compared with those meeting the mucosal healing criteria (90.59% vs 98.24%, p < 0.001). Patients with active UC had lower total IBDQ scores than those in remission (87.75% vs 96.50%, p < 0.001). Furthermore, the disease imposed a heavy psychological burden: over 90% of both physicians and patients (Figure 4(a)) consistently agreed that UC had a disruptive impact on social activities, physical exercise, and career development (p = 0.244). Even during remission, 85.34% of patients reported fear of relapse, a concern even more prevalent among physicians (97.65%, p < 0.001; Figure 4(b)). Finally, concerning economic burden and treatment willingness (Figure 4(c)–(e)), UC placed significant pressure on families: although most respondents believed patients were willing to pay 10%–30% of their household income for treatment, in reality, 21.44% of patients were willing to pay over 50%, a proportion far exceeding physicians’ expectations (5.29%), p < 0.001. Moreover, inpatients demonstrated a greater willingness to pay than outpatients did.

Physician and patient perceptions of disease burden. (a) Impact of UC on patient life. (b) Concern about relapse risk during remission; (c–e) Household income required for UC treatment—physicians versus patients, outpatients versus inpatients, physicians by title. (f–h) Most impactful factor on long-term treatment adherence—physicians versus patients, outpatients versus inpatients, physicians by title.
These multifaceted burdens collectively point to the core challenges in long-term disease management. The study further found that “uncertain long-term treatment efficacy” was jointly identified by both physicians and patients as the most critical factor affecting patients’ adherence to long-term therapy (Figure 4(f)). However, stratified analysis revealed that outpatients were most concerned about potential side effects, whereas inpatients prioritized uncertainty of long-term efficacy (Figure 4(g)). Physicians across various professional titles all believed that the most influential factor affecting patients’ adherence to long-term treatment was the uncertainty of long-term efficacy (Figure 4(h)).
Discussion
This study, through a nationwide multicenter survey, provides an in-depth analysis and comparison of the cognitive differences between Chinese UC patients and physicians across multiple dimensions, including perceptions of disease status, treatment goals, medication use, follow-up preferences, economic burden, and decision-making models. The unique value of this research lies in its dual-perspective questionnaire design, which systematically identifies both disparities and consensus between these two groups by posing parallel questions to both parties. Furthermore, this investigation represents the first study to compare perceptions of UC disease burden and management across different physician hierarchies (from residents to chief physicians) and patients with varying healthcare statuses (outpatient vs inpatient).
The demographic characteristics of the respondents (including age at diagnosis and gender distribution) suggest that they represent a general UC patient population; therefore, these findings are potentially applicable to broader UC populations.6,16–18 Our study confirmed significant differences in UC-related concerns: physicians placed greater emphasis on objective clinical indicators (such as bloody stools and daily stool frequency), whereas patients were more inclined to report subjective symptomatic experiences, with particular attention to rectal urgency. This observation aligns with findings from European and North American studies.4,6,19 The research by Rubin et al. 4 demonstrated that one of the most significant discrepancies between patients and physicians lies in the latter’s potential underestimation of the severity of rectal urgency in UC patients or the urgency to defecate shortly after meals. Similarly, another study highlighted that issues related to toilet access and use substantially impact the quality of life of UC patients, indicating that these challenges may impose an additional psychosocial burden on them. 19 This cognitive divergence may lead to differing definitions of disease remission status between physicians and patients. In our study, physicians’ definition of remission focused more on the normalization of objective biological markers (e.g., laboratory inflammatory indicators). In contrast, patients prioritized improvement in subjective well-being and treatment satisfaction. This aligns with the report by Higgins et al., 20 who found that endoscopic inflammation was still commonly present in patients during their self-reported remission, suggesting that subjective perceptions might underestimate disease activity. However, patient-reported outcomes remain indispensable references, and neglecting them can lead to treatment disengagement and reduced satisfaction.
Regarding the perception of treatment goals in UC, a notable disparity exists between physicians and patients. Consistent with the international STRIDE-II consensus,8,21 physicians typically prioritize “endoscopic mucosal healing” as the primary treatment goal, reflecting their emphasis on long-term disease prognosis. Endoscopic mucosal healing is crucial for UC patients, as it reduces the risks of disease relapse, hospitalization, and surgery. 22 Patients who fail to achieve mucosal healing are more prone to symptom exacerbation. Furthermore, physicians focus on “long-term maintenance of disease remission” at rates more than twice those observed among patients. In contrast, patients place greater importance on “improving quality of life and resuming normal social functioning.” This tendency has been corroborated by studies in both Spain and Switzerland, 23 indicating that patients are more concerned with improving short-term quality of life. In contrast, physicians are more focused on long-term treatment objectives. The differences described above highlight a fundamental distinction between patient-reported outcome—centric evaluation systems and biomarker-driven medical frameworks. 3 Stratified analysis further revealed that hospitalized patients, being in the acute phase of the disease, have a more urgent need for rapid control of symptoms such as abdominal pain and diarrhea. At the same time, their focus on long-term remission is significantly reduced. Concurrently, as physicians’ seniority increases, their emphasis on rapid symptom control also shows an increasing trend. This phenomenon may reflect the greater ability of senior physicians to listen to and understand the importance that patients place on quality of life. By promptly alleviating symptoms, they aim to enhance patient trust in the physician and adherence to the treatment plan, thereby laying the groundwork for subsequently implementing more complex and longer-term strategies, such as achieving mucosal healing. 24
Regarding medication perceptions, although both physicians and patients share similar awareness of specific corticosteroid side effects (such as weight gain and osteoporosis), consistent with the steroid side effects reported in the study by Waljee et al., 25 patients’ concern levels regarding corticosteroid-related risks are significantly higher than those of physicians.4,19 The first recommendation of both the Canadian and the U.S./European Union “Choosing Wisely” programs for IBD treatment states that physicians should not use corticosteroids for maintenance therapy in IBD,26,27 as they are associated with various adverse effects. 28 Second-generation corticosteroids may offer better tolerability, 29 but further research is still needed. When assessing perceptions regarding biologics, physicians tend to overestimate patients’ knowledge of biologics and their safety profiles. This cognitive bias reflects the issue of information asymmetry present in current physician–patient communication: based on their professional background, physicians might assume patients possess relevant knowledge, while in reality, patients have a limited understanding. This knowledge gap directly impacts the efficiency of clinical communication, potentially leading to mismatched information delivery and suboptimal treatment decisions.
Regarding the diagnostic stage, over half of the patients experienced misdiagnosis and significant diagnostic delays, a finding consistent with global reports.19,30 Furthermore, more than one-quarter required three or more consultations before receiving a definitive diagnosis. Diagnostic delays can exacerbate patient frustration and anxiety. Still, they may also adversely affect the physician–patient relationship, 31 and more importantly, they can delay treatment initiation, thereby increasing the risk of complications, including intestinal surgery. 32 These results suggest that the early recognition of UC remains a clinical challenge, underscoring the urgent need for standardized diagnostic tools and support systems to enhance the differentiation of non-specific intestinal symptoms. A striking finding is that there was near-unanimous agreement among both physicians and patients that “frequent medical visits disrupt work/studies” is the most troubling issue within the current management model (physicians: 98.82%, patients: 96.06%), highlighting the time and economic burden of frequent appointments as key factors affecting adherence and quality of life. 33 At the level of follow-up models, although both physicians and patients acknowledge the necessity of regular follow-up, there is a significant disparity in the preferred frequency: most patients prefer to extend the interval to 6 months or longer, whereas physicians generally recommend shortening it to every 2 months. 34
Interestingly, although the physician cohort theoretically endorsed the “shared decision-making” model (47.06%), patients leaned more toward passive or semi-passive roles, primarily selecting “autonomous decision-making after doctor’s recommendation” (47.26%) and “doctor-led decision-making” (42.01%). Patients with UC who participate in shared decision-making often report higher satisfaction with their treatment experience compared to those who are not fully involved. 35 However, when examining decision-making models, only 10.72% of patients experienced shared decision-making. The vast majority fell into categories of physician-guided (e.g., autonomous decision after physician’s recommendation) or physician-dominated models. The lack of shared decision-making might be related to the current reality of busy outpatient clinics. Physicians, within the constraints of brief consultations, are unable to convey disease and management information to patients fully. Physicians expect patients to increase their follow-up frequency, which is crucial for assessing clinical status, optimizing medication, and planning the next stages of treatment. Some studies suggest that physicians should utilize online tools or smartphone applications to monitor patients more effectively and track their activities and symptoms, thereby improving adherence and clinical outcomes.36–39
This study also provided an in-depth exploration of the multifaceted burden associated with UC. Regarding quality of life, the results confirm a significant association between mucosal healing and improved quality of life. Although most patients reported good quality of life scores, the total IBDQ scores of those who had not attained mucosal healing were significantly lower than those of patients who had met the mucosal healing criteria. Concurrently, the quality of life for patients in the active disease phase was significantly lower than that of patients in remission. In terms of mental health, over 90% of both physicians and patients agreed that UC has a disruptive impact on patients’ social activities, physical exercise, and career development. This high level of consensus reveals the extensive psychosocial consequences of the disease. Of particular note, even during clinical remission, 85.34% of patients continued to be troubled by the fear of relapse, and physicians perceived this issue to be even more prevalent. This phenomenon of “psychological burden during remission” suggests that traditional clinical remission criteria may not fully capture the patient’s experience; future treatment goals should incorporate mental health assessment and intervention. 40 Regarding the economic burden, the long-term treatment of UC places significant pressure on patients’ families, 41 and patients’ willingness to pay far exceeds physicians’ expectations. Specifically, 21.44% of patients were willing to allocate over 50% of their household income for treatment, a proportion significantly higher than physicians’ estimation (5.29%). This discrepancy may reflect physicians underestimating patients’ financial capacity or patients’ willingness to assume higher financial risks driven by urgent disease control needs. Hospitalized patients demonstrated a stronger willingness to pay, potentially related to the acute phase need for rapid symptom control. In summary, this study suggests that UC management necessitates a comprehensive approach. While pursuing biological targets such as mucosal healing, it is essential to address patients’ psychosocial needs and economic burdens fully.
However, this study has several limitations. First, the questionnaire employed a closed-ended design and was relatively lengthy (74 items for physicians and 95 for patients), which may have affected respondents’ willingness to participate and the depth of their answers. Second, the retrospective survey design may introduce recall bias. Furthermore, the perspectives of physicians and patients were collected from specific geographic regions and healthcare settings, which may limit the generalizability of the findings. In addition, the gastroenterologists who participated in the study were predominantly from tertiary hospitals; however, this sampling bias could also be regarded as an added value, as these clinicians possess in-depth expertise in the disease. Finally, although basic demographic information was collected, the study did not further analyze how variables such as education level, occupation, gender, and socioeconomic status might influence patients’ perceptions and decision-making. Future research could incorporate these variables to more comprehensively explore patients’ subjective experiences and perspectives throughout the diagnostic and treatment process.
Conclusion
In conclusion, this study is the first to reveal, at a national level, the cognitive differences between Chinese physicians and patients with UC regarding symptom focus, treatment goals, follow-up, and decision-making preferences. These findings have clear implications for clinical practice in China. Against a backdrop of uneven distribution of medical resources, traditional doctor–patient dynamics, and significant economic burdens, targeted measures are essential. These include developing decision aids tailored for Chinese patients, establishing flexible and accessible follow-up systems, and placing greater emphasis on patients’ subjective experiences and economic concerns during communication. Future efforts should focus on building localized pathways to support doctor–patient communication and promoting the genuine implementation of patient-centered management models.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261430110 – Supplemental material for Discrepancies between patients’ and gastroenterologists’ perceptions of diagnosis and treatment in ulcerative colitis: a multicenter retrospective study
Supplemental material, sj-docx-1-tag-10.1177_17562848261430110 for Discrepancies between patients’ and gastroenterologists’ perceptions of diagnosis and treatment in ulcerative colitis: a multicenter retrospective study by Zhenzhen Fan, Ruixia Li, Xin Liu, Qian Cao, Weiming Zhu, Minhu Chen, Yihong Fan, Naizhong Hu, Yufang Wang, Xiaoping Lv, Mei Ye, Liangru Zhu, Xiaoyun Yang, Hong Guo, Fang Xiao, Ning Chen, Hongjie Zhang, Yan Chen, Kaichun Wu and Jie Liang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848261430110 – Supplemental material for Discrepancies between patients’ and gastroenterologists’ perceptions of diagnosis and treatment in ulcerative colitis: a multicenter retrospective study
Supplemental material, sj-docx-2-tag-10.1177_17562848261430110 for Discrepancies between patients’ and gastroenterologists’ perceptions of diagnosis and treatment in ulcerative colitis: a multicenter retrospective study by Zhenzhen Fan, Ruixia Li, Xin Liu, Qian Cao, Weiming Zhu, Minhu Chen, Yihong Fan, Naizhong Hu, Yufang Wang, Xiaoping Lv, Mei Ye, Liangru Zhu, Xiaoyun Yang, Hong Guo, Fang Xiao, Ning Chen, Hongjie Zhang, Yan Chen, Kaichun Wu and Jie Liang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-pdf-3-tag-10.1177_17562848261430110 – Supplemental material for Discrepancies between patients’ and gastroenterologists’ perceptions of diagnosis and treatment in ulcerative colitis: a multicenter retrospective study
Supplemental material, sj-pdf-3-tag-10.1177_17562848261430110 for Discrepancies between patients’ and gastroenterologists’ perceptions of diagnosis and treatment in ulcerative colitis: a multicenter retrospective study by Zhenzhen Fan, Ruixia Li, Xin Liu, Qian Cao, Weiming Zhu, Minhu Chen, Yihong Fan, Naizhong Hu, Yufang Wang, Xiaoping Lv, Mei Ye, Liangru Zhu, Xiaoyun Yang, Hong Guo, Fang Xiao, Ning Chen, Hongjie Zhang, Yan Chen, Kaichun Wu and Jie Liang in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors are grateful to the CHASE-IBD and MIMIC IBD team for support in this research project. We thank Professors Zhang Yujie, Masai, Zhao Xiaoxing, and Tang Bihua for data collection and quality control, and especially Professor Xi Peng for strategic assistance.
Declarations
Availability of data and materials
All data are available from the corresponding author upon reasonable request (
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.