
Abstract
Background:
Hidradenitis suppurativa (HS) is a chronic, recurrent skin disease that may be associated with inflammatory bowel disease (IBD).
Objectives:
This study aimed to describe the features and therapeutic requirements of IBD and HS in patients who present both entities and the risk factors for HS development in patients with IBD.
Methods:
Case-controlled, retrospective study of all patients diagnosed with IBD-HS in the ENEIDA registry. Cases were paired 1:2 with controls (IBD without HS).
Design:
This was a retrospective, case–control study.
Results:
A total of 819 patients were included: 273 patients with IBD-HS and 546 controls. Female sex (62% vs 44%, p = 0.0001), active smoking (45% vs 18%, p = 0.0001), Crohn’s disease (CD; 83% vs 55%, p = 0.0001), perianal disease (59% vs 33%, p = 0.0001), extraintestinal manifestations (38% vs 17%, p = 0.0001), and psychiatric disorders (18% vs 2%, p < 0.05) were more frequent among patients with IBD-HS than in controls. The average body mass index was greater in the IBD-HS group. The most frequently HS-affected locations were axillary (57%) and genital (43%) areas. Use of biologicals and CD-related perianal surgery was more common among patients with CD-HS (77% vs 66%, p = 0.003; 37% vs 13%, p < 0.001), compared to controls with only CD.
Conclusion:
Patients with IBD-HS exhibit a distinctive phenotype with higher therapeutic requirements for the subset of patients with CD-HS compared to those without HS. Assessment of this comorbidity should be considered in patients with suggestive skin lesions and IBD to improve the outcomes of both conditions.
Plain language summary
Keywords
Introduction
Inflammatory bowel diseases (IBD), including Crohn’s disease (CD) and ulcerative colitis (UC), are chronic, progressive, and disabling conditions characterized by a relapsing course. Up to 50% of IBD patients will develop at least one extraintestinal manifestation (EIM) in their lifetime. EIMs most frequently involve joints, eyes, or skin. 1 The most common cutaneous EIMs are aphthous stomatitis, pyoderma gangrenosum, and erythema nodosum, although other skin conditions have also been associated with IBD, including hidradenitis suppurativa (HS).2–4 HS or acne inversa is a chronic disease of the pilosebaceous unit characterized by recurrent, deep, painful nodules, tunnels, and abscesses in apocrine gland-rich areas, such as the anogenital, groin, and axillary regions. 5 It predominantly affects young adults, and has well-established risk factors, including smoking, obesity, and female gender.5,6 Genetics also contributes significantly, as a family history of the disorder is observed in more than 30% of individuals affected. 7 The pathogenesis of HS is multifactorial, and some studies have linked HS with dysregulation of the interleukin (IL)-12/23 and tumor necrosis factor-α (TNF-α) pathways, pointing toward an immune origin.8,9 In addition, several studies have reported an association between HS and IBD, based on histological similarities (development of sinus tracts, granulomatous inflammation, and scarring), shared environmental factors, and good response to anti-TNF treatment in both diseases.10–15 Moreover, epidemiological studies indicate that the prevalence of HS in patients with IBD ranges from 7% to 23%, with a 9-fold higher relative risk than the general population.11,16–18
Although evidence on risk factors for HS in patients diagnosed with IBD is scarce, some studies suggest that these patients are more likely to be overweight or obese, current or former smokers, and to have ileocolonic and/or perianal disease involvement.19,20 Infliximab and adalimumab are effective in the treatment of both HS and IBD.21,22 Ustekinumab, approved for treating patients with IBD, has also been effective in some case series of HS.23–25
Although the association between HS and IBD has been described, there is a need for more studies that better characterize the link between these two conditions. This study, therefore, aimed to comprehensively describe the clinical features and therapeutic requirements of patients with IBD-HS and to determine the risk factors for developing HS in this large real-world cohort of patients with IBD.
Methods
Study design and patients
We conducted a case-controlled, retrospective, nationwide study based on the ENEIDA 26 registry, sponsored by the Spanish Working Group in IBD (GETECCU), a prospectively maintained database with continuous external monitoring to ensure the completeness and consistency of the data entered. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Material). 27 The case group comprised patients with IBD-HS over 18 years, included in the ENEIDA registry from 2006 to 2022. All of them had an established diagnosis of UC, CD, or unclassified IBD according to the European Crohn’s and Colitis Organisation, 28 with a coexistent diagnosis of HS confirmed by a dermatologist. The control group consisted of patients with IBD and without HS who attended the same centers during the same time period of time. The non-occurrence of HS was confirmed by designating control subjects from the ENEIDA registry who lacked an HS diagnosis within their spectrum of documented comorbidities. Cases were randomly paired with twice the number of controls. Considering the study design, matching techniques were not appropriate since the investigated factor (HS development) was definitive of the case condition.
Data collection and definitions
Inflammatory bowel disease
Data collection included demographic characteristics, including age, sex, most recent body mass index (BMI), smoking status (never smoker, former smoker, or current smoker), and relevant comorbidities. IBD-related features were also collected, including age at IBD diagnosis, disease duration, type of disease (UC, CD, or unclassified IBD), disease location, phenotype according to the Montreal classification, 29 family history of IBD, and EIMs. Therapeutic requirements, including biological or non-biological treatments and the need for IBD-related surgery, were also recorded.
Hidradenitis suppurativa
Diagnosis of HS was confirmed clinically by dermatologists at each participating center, based on the presence of typical lesions (deep nodules, abscesses, and tunnels), characteristic topography (intertriginous areas), and a chronic relapsing course. HS characteristics were collected using a disease-specific questionnaire, recording timing of HS diagnosis (before or after IBD diagnosis), disease duration, family history of HS, location (axilla, groin, extremities, genital, perianal, gluteal, mammary, or other), type of lesion (nodules, abscesses, and tunnels), and severity stage as defined by the Hurley system (stage 1—formation of abscesses (single or multiple) without tunnels and healing/scarring; stage 2—recurrent abscesses with tunnels and healing, with distinct single or multiple lesions; and stage 3—diffuse or nearly diffuse involvement, or multiple interconnected tunnels and abscesses throughout the area). HS-related treatment was also recorded (antibiotics, metformin, retinoids, biological and non-biological therapies, and surgery).
The response to HS treatment was defined by the Hidradenitis Suppurativa Clinical Response criteria as a reduction of ⩾50% in the count of inflammatory lesions (abscesses and inflammatory nodules) with no increase in abscesses or draining fistulas. It was also noted whether HS was a paradoxical manifestation of any advanced therapy received by the patients. Paradoxical HS was defined as the occurrence of HS during treatment with biologicals, confirmed by dermatologists.
Statistical analysis
A descriptive analysis was conducted on baseline demographic characteristics and IBD manifestations. Continuous variables were presented as mean and standard deviation or median with interquartile range (IQR), as appropriate. The Shapiro–Wilk normality test was performed to test normality. Categorical variables were presented as numbers and percentages and compared using the Chi-square test or Fisher’s exact test when any expected cell counts are less than 5. Quantitative variables that followed a normal distribution (verified using the Shapiro–Wilk test) were analyzed using the Student’s t test. If the distribution was not normal, the U-Mann–Whitney non-parametric test was applied. A p-value of <0.05 was considered statistically significant.
The analysis of potential risk factors that could influence HS development was performed using a multivariate logistic regression analysis. Collinearity was assessed using a correlation matrix. Pairwise correlations <0.7 between predictors indicated no substantial collinearity. A maximum of 12 non-collinear variables (female sex, active smoking, age at diagnosis, BMI, CD, extent of CD, perianal disease, EIMs, psychiatric disorders, hepatic steatosis, ischemic cardiopathy, and hypothyroidism) were included in the multivariate logistic regression analysis since a total of 273 events (HS cases) were available, exceeding the criterion of a minimum of 10–20 events per variable included in the analysis. Results from the logistic regression analysis were expressed using odds ratios and 95% confidence intervals (CIs), with p-values.
Results
Patient characteristics
Forty hospitals participated in the study across Spain, including a total of 819 patients. At the time of data extraction from the ENEIDA database, we identified a total of 273 patients with IBD-HS (cases) who were paired with 546 patients with IBD and without HS (controls; Figure 1). The main demographic features of patients are described in Table 1. Patients with IBD-HS had a significantly greater average BMI compared to controls (27.8 ± 6.6 vs 25.7 ± 4.6; p < 0.001). Patients with HS and IBD were also significantly more likely to be obese (35.6% vs 16.9%, p < 0.001) than patients without HS. The prevalence of female sex was higher in the IBD-HS cohort (62.3% vs 44.1%, p < 0.001) than in the control group. Patients with IBD-HS were younger and more frequently active smokers than controls (43 ± 12 vs 53 ± 15 years, p < 0.05; 45.2% vs 18%, p < 0.001). No differences were found between both cohorts regarding the overall rate of comorbidities (34.8% vs 36.3%, p = 0.68). However, hepatic steatosis (5.2% vs 1.7%, p = 0.005), hypothyroidism (4.4% vs 1.1%, p = 0.003), and psychiatric disorders (17.9% vs 2%, p < 0.001) were more prevalent among patients with IBD-HS.
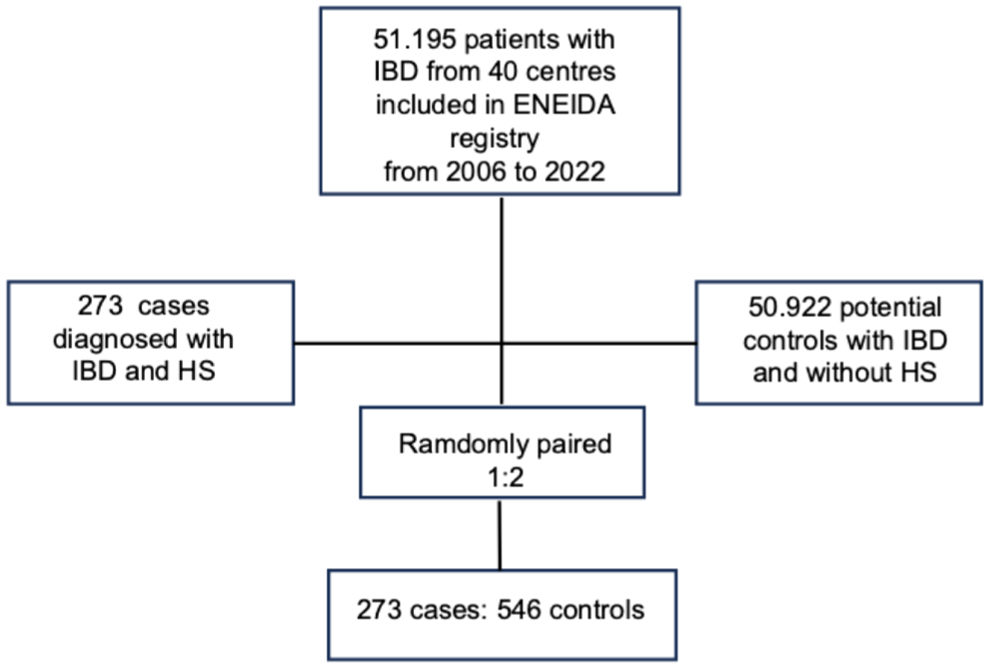
Flow chart of patients with inflammatory bowel disease included in the study.
Patient baseline demographic characteristics.

HS, hidradenitis suppurativa; IBD, inflammatory bowel disease; IBD-HS, patients with both IBD and HS; SD, standard deviation.
The clinical IBD-related characteristics in both cohorts are detailed in Table 2. Patients with IBD-HS were younger at the time of IBD diagnosis than controls. The prevalence of CD diagnosis was higher in the IBD-HS group (83.2% vs 54.6%, p < 0.001), and perianal involvement was more common among IBD-HS patients (55% vs 20%, p = 0.001). In CD, upper gastrointestinal location was less frequent in IBD-HS patients compared to controls (3.1% vs 14.4%, p < 0.001), and fewer patients were >40 years at CD diagnosis (15.9% vs 32.2%, p < 0.001). There were no differences between groups in either CD behavior or UC extent. EIMs were more frequent among IBD-HS than in controls (38% vs 17%, p < 0.0001), with statistically higher rates of joint (25.3% vs 8.8%, p < 0.001) and skin manifestations (12.5% vs 7.3%, p = 0.01).
Inflammatory bowel disease characteristics in patients with and without hidradenitis suppurativa.

CD, Crohn’s disease; HS, hidradenitis suppurativa; IBD, inflammatory bowel disease; IBD-HS, patients with both IBD and HS; SD, standard deviation; UC, ulcerative colitis.
Figure 2 summarizes therapeutic requirements by IBD type. In CD, biological agents were used more frequently (77.5% vs 65.8, p = 0.003) and perianal CD surgical procedures were also more common among CD-HS versus CD controls without HS (37.6% vs 13.1, p < 0.001). No differences regarding abdominal surgery or biological and non-biological use were observed between groups in the UC subset of patients. A detailed description of the non-biological and biological therapies used in both study groups is provided in Table 3.

Therapeutic requirements by inflammatory bowel disease type: (a) ulcerative colitis and (b) Crohn’s disease.
Use of non-biological and biological therapies.

HS, hidradenitis suppurativa; IBD, inflammatory bowel disease; IBD-HS, patients with both IBD and HS.
Characteristics of HS in patients with IBD
The diagnosis of IBD preceded HS diagnosis in 208 patients (77.6%), and the duration of HS showed a median value of 6 years (IQR 3–11). The most frequent location was the axillary region (58%), followed by the genital (42.9%), perianal (31.3%), gluteal (27%), groin (21.6%), and mammary (17.5%) locations. Patients presented a median of 2 affected areas (IQR 1–3). Main characteristics and therapeutic requirements of HS are described in Table 4. The severity of HS measured by the Hurley system was mild (stage 1) in 95 (42.2%) patients, moderate (stage 2) in 69 (30.9%), and severe (stage 3) in 59 (26.5%) patients. One hundred twenty-seven patients (47%) underwent surgical excision of HS. Paradoxical HS was observed in 19 (7%) patients, associated with infliximab (n = 4, 21%), adalimumab (n = 11, 58%), ustekinumab (n = 3, 16%), and other unspecified biological therapy (n = 1, 5%), leading to discontinuation of the biological agent in 7 (41%) patients.
Characteristics of hidradenitis suppurativa in patients with inflammatory bowel disease.

HiSCR, Hidradenitis Suppurativa Clinical Response; HS, hidradenitis suppurativa; IBD, inflammatory bowel disease; IBD-HS, patients with both IBD and HS; IQR, interquartile range; SD, standard deviation.
Risk factors associated with HS in IBD patients
In the multivariate analysis, the factors that predicted the development of HS were female sex, active smoking, increased BMI, CD diagnosis, perianal involvement, the presence of EIMs, and a history of psychiatric disorders, while upper gastrointestinal involvement in CD appeared to be associated with a lower risk of HS (Figure 3).

Logistic regression analysis of hidradenitis suppurativa risk factors in inflammatory bowel disease patients.
Discussion
Despite current evidence supporting the association between HS and IBD, 30 little information is available on the risk factors for HS developing in patients with IBD.
The present study is the largest cohort of patients with coexistent IBD-HS reported to date and reveals that these patients exhibit a particular and distinctive phenotype. The subgroup of patients with CD-HS has higher therapeutic requirements compared to patients with CD without HS. Our data could help to identify the risk factors that contribute to HS development among patients with IBD.
We observed that patients with IBD-HS are younger than controls, and that female sex is an independent predictive factor for the development of HS among patients with IBD. In accordance with our results, Janse et al. 11 also found that patients with both IBD and HS were significantly younger than patients with IBD alone. Other independent risk factors for HS that emerged from the multivariate analysis of the present study are active smoking and increased body weight, findings that align with previous studies.11,19 Furthermore, smoking, overweight, and female sex are well known factors that contribute to HS in the general population. 5 Female predominance of HS in the general population (with a female-to-male ratio of approximately 3:1) has been observed in Europe and North America. 31 Conversely, a higher prevalence among males was observed in Asian populations, with an approximate female-to-male ratio of 1:2. 32 It has been hypothesized that genetics, hormones, and variations in smoking habits may contribute to the discrepancies observed in gender distribution. Epithelial thickening potentially caused by nicotine may be the link between a smoking habit and HS pathology. 33
Another notable finding in our study is that the odds of psychiatric disorders among patients with IBD-HS are 5.7 times greater (95% CI 2.08–15.7) compared with patients with only IBD. Ramos-Rodríguez et al. 17 similarly found that patients with IBD-HS had an increased prevalence of depression compared to controls without HS. Although the precise mechanisms underlying the association between HS, depression, anxiety, and/or suicidality remain unclear, several potential explanations have been proposed. HS is characterized by significant symptoms, including pruritus, skin pain, disfiguring lesions, sexual disturbances, psychological distress, and a diminished quality of life. 34 In fact, up to 30% of adults and 16% of children with HS in the general population suffer from depression. 35 On the other hand, patients with IBD-HS are affected by two chronic diseases interrelated with depression and/or anxiety, undoubtedly contributing to the high rate of psychiatric disorders reported in our study.
We also found that CD was the most prevalent IBD type among patients with IBD-HS, which is consistent with previous studies that have demonstrated a strong association between HS and CD.11,14,19 This connection suggests common pathophysiological features between these two disease processes, mediated not only by shared risk factors but also by common immunological pathways, such as IL-23/Th-17 and TNFα dysregulation. 9 In addition, we observed a higher prevalence of perianal disease in patients with both conditions, as suggested in earlier research.18–20 Perianal HS may have been misdiagnosed as perianal CD due to their similar clinical features. 36 Furthermore, the existence of isolated perianal CD poses a diagnostic challenge, as it can mimic other perianal pathologies, notably HS. In such confusing cases, MRI serves a valuable role in distinguishing between the two entities. 37 Nevertheless, all patients in our study were evaluated and treated according to a multidisciplinary pathway in which gastroenterologists worked alongside dermatologists, reducing the likelihood of an incorrect diagnosis.
Age does not account for the lower frequency of upper GI involvement in the cases of our research given that the IBD-HS cohort was significantly younger than the control group. Nonetheless, given the low prevalence of this localization in our cohort, we must be careful not to overstate the potential protective effect of upper GI Crohn’s involvement on HS development.
Interestingly, a higher use of anti-TNF agents was observed in the CD-HS population compared to controls. Nevertheless, previous data regarding therapeutic requirements in patients with IBD-HS are conflicting.11,19,38 Our findings may reflect an increased need for biological therapy associated with CD, perianal disease, and EIMs, which were more prevalent in the IBD-HS group. In addition, anti-TNF agents might be the best option for this patient group because a single medication can address both conditions. 22 Another explanation for the greater use of biologicals in our study could be the severity of HS, compared to other series that did not find differences in anti-TNF use between patients with IBD-HS and those without HS. 19 Perianal CD-related surgery was also more frequent among the CD-HS subgroup in our series. Unfortunately, the clinical activity of IBD was not recorded in our study, but these findings suggest a more aggressive perianal phenotype in the CD-HS subgroup. In line with this, a Canadian study 20 found that patients with IBD-HS were more likely to have active endoscopic IBD and concurrent active perianal CD compared with IBD controls without HS.
In line with previous studies, we found that the axillae were the most commonly affected HS sites, followed by the genital area,10,20 while other studies, in contrast, showed that groin areas were the most common HS location.18,19,38 Depending on the age and sex of those affected by HS in the general population, there are some differences in the location of lesions. 5 The axillae are the most affected area in patients younger than 18 years and adult men, while adult women have more often involvement in the groin areas.
In our study population, almost 70% of patients with HS responded to the anti-TNF agents and ustekinumab. In fact, both anti-TNF and ustekinumab have been used successfully in patients with severe HS, 39 although currently only case series and case reports are available regarding ustekinumab. 40
Finally, a remarkable finding was the presence of paradoxical HS in 7% of patients with IBD-HS, mostly associated with anti-TNF or ustekinumab treatment. Echoing our results, in a retrospective analysis of 25 patients with autoimmune conditions, Faivre et al. identified 12 instances of paradoxical HS secondary to adalimumab therapy. Notably, clinical improvement followed drug discontinuation, whereas treatment re-challenge triggered a recurrence of HS. It is noteworthy that CD is one of the most frequent comorbidities among patients experiencing paradoxical HS reactions.41,42 However, the exact mechanism linking paradoxical HS manifestation and CD is still unclear.
This collaborative study has several strengths that should be highlighted. First of all, this is the largest cohort of patients with IBD and concomitant HS reported to date. Our results are bolstered not only by the sample size but also by a robust control cohort, enabling us to clinically characterize patients with IBD at risk of presenting HS. Furthermore, the collection of HS-related variables using a disease-specific questionnaire ensures the quality of the data and the reliability of the obtained results. Nonetheless, several limitations, mainly arising from the retrospective study design, must be acknowledged. This study, relying on data from multiple tertiary referral centers, may over-represent patients with more severe disease (severe HS, complex IBD, or the combination of both) as they are more likely to be referred and recorded. The study population might not be representative of all patients with IBD and HS in the general population. On the other hand, a significant limitation of this study is the absence of data on the clinical activity of IBD at the time of data collection. This deficiency prevents us from correlating IBD activity with HS activity, and future prospective studies are needed to comment on the relationship between bowel disease activity and skin disease activity to further understand this association. In addition, IBD preceded HS in a high percentage of cases; this fact could have conditioned the choice of treatment, opting for therapies effective for both diseases.
Conclusion
In conclusion, we have characterized factors linked to the coexistent diagnosis of HS and IBD. These insights enable clinicians to more effectively screen IBD patients for HS risk, particularly those presenting with female sex, obesity, smoking history, CD, perianal involvement, and EIMs. The subset of patients with CD-HS often requires biologicals as well as CD-related perianal surgery.
Supplemental Material
sj-doc-1-tag-10.1177_17562848261423351 – Supplemental material for Hidradenitis suppurativa in patients with inflammatory bowel disease: a national multicenter study from the GETECCU-ENEIDA Registry
Supplemental material, sj-doc-1-tag-10.1177_17562848261423351 for Hidradenitis suppurativa in patients with inflammatory bowel disease: a national multicenter study from the GETECCU-ENEIDA Registry by Lucía Madero-Velázquez, Ruth de Francisco, Belen Herreros, Carmen Yagüe, Luis Bujanda, Xavier Calvet, Angel Ponferrada, Mariam Aguas, Francisco Rodríguez-Moranta, Ignacio Marín-Jiménez, Lourdes Catalá, Carla Gargallo-Pueyo, José Huguet, Francisco Mesonero, David Monfort, Mónica Sierra-Ausín, Laura Igualada, Elena Ricart-Gomez, María González-Vivo, María José García, Alejandro Hernandez Camba, Ainara Elorza, Lucía Zabalza-San Martín, Laura Ramos, María Dolores Martín-Arranz, Isabel Ruiz-Núñez, Pilar Martínez-Montiel, Pilar Soto, Cristina Roig, María Molina, Miriam Mañosa, Cristina Alba, Manuel Barreiro-de Acosta, Javier P. Gisbert, Patricia Ramírez de la Piscina, Rufo Lorente, Yamile Zabana, Belen Botella, Sabino Riestra, Olivia Belen-Galipienso, David Busquets, Federico Argüelles, José Carlos Pascual, Pedro Zapater, Eugeni Domènech and Ana Gutiérrez in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
None.
Declarations
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.