
Abstract
Background:
Endoscopic resection (ER) is increasingly utilized for ulcerative colitis-associated neoplasias (UCANs); however, these lesions demonstrate higher rates of local residuals and recurrences compared with sporadic neoplasias. This may be partly explained by challenges in accurately delineating lesion borders preoperatively, though their clinicopathologic features remain incompletely understood.
Objectives:
This study aimed to characterize the endoscopic and histologic features associated with local residuals and recurrences following ER for UCAN.
Design:
A retrospective observational study.
Methods:
Patients diagnosed with UCAN exhibiting a p53 mutation pattern between 2005 and 2024 and suspected of having local residual or recurrent lesions after ER were included. Endoscopic and histologic features were evaluated.
Results:
Of 122 UCAN patients, 13 (6 underwent initial ER at our institution before 2018, and 7 underwent initial ER elsewhere) were identified with suspected local residuals or recurrences. Prior to initial ER, p53 immunostaining was not performed in eight cases (five without biopsy and three with biopsy specimens not stained), and only two patients underwent biopsy of the surrounding tissue. Ten tumors had positive or potentially positive horizontal margins (HMs) that were not identified endoscopically at the time of ER. All local recurrences were associated with suspected positive HMs, with a median time to recurrence of 16.5 (8.5–23.8) months. At recurrence, 50% of the lesions appeared flat, while the remaining 50% were superficial elevated lesions with adjacent flat dysplasia.
Conclusion:
Inadequate preoperative assessment of the horizontal extent of UCANs may contribute to residual or recurrent disease after ER. Comprehensive evaluation—including p53 immunostaining and careful inspection for surrounding flat dysplasia—may improve curative outcomes in UCAN management.
Keywords
Introduction
Ulcerative colitis (UC) is a chronic inflammatory disease associated with an elevated risk of colorectal cancer. The global prevalence of UC is rising, including in Japan. 1 As of 2023, the number of patients with UC in Japan is estimated at 316,900 with a male-to-female ratio of 1.31:1. 2 The standard treatment for UC consists of 5-aminosalicylic acid, followed by systemic corticosteroids and immunomodulators when needed. In recent years, several biologic agents and small-molecule inhibitors—including anti-TNF antibodies, anti-integrin therapy, anti-IL-12/23 antibodies, anti-IL-23 antibodies, and Janus kinase inhibitors—have also become widely used in Japan. Despite these therapeutic advances, disease control remains insufficient in a subset of patients, placing them at risk of developing UC-associated neoplasia (UCAN). Among the molecular alterations implicated in UC-associated carcinogenesis, p53 mutation is recognized as an early and critical event, serving as a key diagnostic biomarker in this setting. 3 When a lesion is identified as high-grade UCAN, proctocolectomy is generally recommended because of the risk of synchronous or metachronous neoplastic lesions. However, following the publication of the SCENIC consensus guidelines in 2015, endoscopic resection (ER) has become increasingly used for the management of early-stage, endoscopically resectable neoplasms in patients with UC.4,5
Despite substantial advancements in endoscopic imaging and resection techniques, the diagnosis and characterization of UCAN remain challenging. These lesions frequently exhibit varied macroscopic presentations, including flat morphologies, which complicate accurate visual delineation.6,7 Furthermore, discrepancies between endoscopic assessment and histologic findings, particularly regarding the depth of invasion, have been reported. 8 While numerous studies have demonstrated the efficacy of ER for dysplasia and early neoplasms in UC, the majority—including our previous investigation 9 —have incorporated substantial numbers of sporadic tumors, limiting the generalizability of findings to inflammation-driven UCAN. Moreover, these studies have predominantly emphasized therapeutic efficacy, with relatively limited focus on the clinicopathologic features associated with local residuals and recurrences.9–24 Local residuals and recurrences occur more frequently in the UC population, yet the endoscopic and histologic predictors of such outcomes remain poorly defined. Given that UCAN often presents with flat dysplasia extending laterally beyond an elevated lesion, we hypothesized that incomplete ER may result from under-recognition of these surrounding flat components. In this study, we sought to clarify the endoscopic and histologic characteristics of UCAN in patients with suspected local residual or recurrent disease following ER.
Materials and methods
Patient selection and data collection
This retrospective observational study was conducted at Keio University Hospital, Tokyo, Japan, and included patients diagnosed with UC-associated dysplasia or adenocarcinoma between January 2005 and December 2024. Both patients who underwent ER for UCAN at our institution and those referred after undergoing ER at other facilities were considered for inclusion. UCAN was defined as neoplasia arising through inflammation-driven carcinogenesis, characterized by the early acquisition of a p53 mutation. As previously described,6–8,25–28 diagnoses were confirmed based on endoscopic features and final histopathological evaluation by at least two experienced gastrointestinal pathologists.
Only patients who underwent ER and were subsequently suspected of having local residual or recurrent lesions were included in the present analysis. Cases without recurrence or with metachronous recurrence were excluded. Metachronous recurrence was defined as the emergence of new neoplastic lesions at anatomically distinct sites occurring at least 6 months following the complete resection of the primary lesion. 29 Additionally, cases involving ER for non-dysplastic lesions, neuroendocrine tumors, sporadic adenomas or carcinomas, serrated lesions, traditional serrated adenomas, or histologically indeterminate UCAN were excluded. Demographic and clinical data were collected retrospectively from medical records and included patient sex, age at UC onset, age at initial detection of UCAN, duration of UC at the time of UCAN detection, disease extent, presence of concomitant primary sclerosing cholangitis, smoking status, UC treatment history, and tumor location. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 30
Endoscopic procedures
Endoscopic procedures were performed using the following instruments: CF-H290I, CF-H260AZI, CF-Q260AZI, PCF-Q260AZI, CF-Q260AI, PCF-H290I, PCF-H290ZI (Olympus, Tokyo, Japan), as well as FUJI-L600ZP7 (Fujifilm, Tokyo, Japan). Following standard white light imaging, adjunctive techniques—including narrow band imaging or blue laser imaging, indigo carmine dye spraying, and magnifying endoscopy—were selectively applied at the discretion of each endoscopist.
Since the implementation of a standardized pre-ER evaluation protocol at our institution in approximately 2018, particular attention has been directed toward the detection of flat dysplasia in suspected UCAN cases.6,7 This is achieved via magnifying colonoscopy in conjunction with indigo carmine dye spraying, as previously described. Prior to ER, targeted biopsies were obtained from mucosal areas surrounding the dysplastic lesion that lacked obvious surface abnormalities, to ensure thorough assessment of the lesion’s lateral extent. For cases managed before 2018 or at other institutions, pre-ER assessments and resection techniques were non-standardized; adherence to our protocol was retrospectively evaluated based on the presence of its key components. Endoscopic findings were reported in accordance with the SCENIC consensus guidelines. 4 The choice of therapeutic modality—surgical resection, cold snare polypectomy (CSP), endoscopic mucosal resection (EMR), or endoscopic submucosal dissection (ESD)—was determined independently by each institution without predefined criteria. ER technique selection and instrument use were left to the discretion of the endoscopist. For ESD procedures, submucosal injection with glycerol and/or sodium hyaluronate was followed by resection using a hook knife or dual knife, according to standard protocols.
The following endoscopic data were retrospectively collected: macroscopic lesion type, whether pre-resection biopsy or p53 immunostaining was done, whether indigo carmine dye spraying or magnifying observation was performed, whether indigo carmine dye spraying or magnification was used, colonoscopy dates, and whether en bloc resection was achieved. For cases referred from other institutions, available endoscopic images and reports were reviewed. Curative resection was defined as R0 resection with submucosal invasion <1000 μm from the muscularis mucosae and absence of lymphovascular invasion, tumor budding, and poorly differentiated components. Local recurrence was defined as histologically confirmed tumor regrowth at the site of initial ER scar after 6 months of initial ER. Local residual tumor was defined as a lesion requiring additional endoscopic or surgical resection because of positive or uncertain margins and/or lymphovascular invasion within 6 months of initial ER. In cases where argon plasma coagulation was applied within 3 months for unclear horizontal margins (HM), patients were categorized as having local recurrence if histologically confirmed recurrence was detected more than 6 months after the initial ER.
Histologic evaluation
Histologic evaluation was performed as previously described,6,27 using targeted biopsy samples, ER specimens, and surgical resection specimens. The final diagnosis of UCAN was established based on routine hematoxylin and eosin staining, with additional consideration of immunohistochemical expression patterns of p53 and Ki67,31,32 including characteristic p53 expression patterns (either diffuse or unique basal overexpression, cytoplasmic localization, or complete absence). In addition, the presence of UC-associated inflammation and dysplasia in the tissue surrounding the lesion supported the diagnosis.6,27 Histopathological characteristics—including tumor type, depth of invasion, lymph node metastasis, lymphovascular invasion, tumor budding, HM, vertical margin (VM), and residual tumor following ER—were assessed in accordance with the Japanese Classification of Colorectal Carcinoma. 33
Statistical analysis
Continuous variables were presented as medians with interquartile ranges (IQR), while categorical variables were reported as percentages.
Results
Patient profile
Between January 2005 and December 2024, 122 consecutive patients were diagnosed with UCAN. Of these, 21 patients underwent ER for UCAN either at our institution or at an external facility. After excluding 6 patients who remained recurrence-free during follow-up and 2 patients who developed metachronous recurrence after ER, 13 patients were identified as having suspected local residual or recurrent disease and were included in the present analysis (Figure 1). Eight of the excluded patients were considered potential candidates for curative ER (Supplemental Figure 1); however, given the limited duration of follow-up, this study did not focus on curative outcomes and instead concentrated on patients with suspected residual or recurrent lesions. The clinical timeline for these 13 patients is shown in Figure 2.

Flow of patients through the study. Of 122 patients with UCAN, 21 underwent ER; 13 with local residual or recurrent lesions were included in the analysis.

Clinical time course of 13 patients. Each line represents an individual patient and concludes with proctocolectomy, except for one patient who achieved complete resection via ER and remained under observation. Arrowheads indicate the timing of local recurrence.
Clinicopathologic characteristics of the included patients are summarized in Table 1. Among the 13 patients, 6 (46%) underwent initial ER at our institution. At the time of UCAN diagnosis, the median age was 54 years, and the median disease duration was 21 years. Consistent with previous reports, 6 the rectum was the most frequent tumor site, accounting for 77% of cases. In terms of endoscopic morphology, 10 lesions (77%) were classified as superficial elevated, and 1 lesion each (8%) as flat or depressed type, with non-polypoid morphology observed in 92% of cases. Most tumors were evaluated using indigo carmine dye spraying (69%) and/or magnifying endoscopy (85%). Prior to ER, biopsies were performed in eight cases (62%), but only two patients (15%) had negative biopsies from the surrounding mucosa, indicating that resectability had been determined primarily based on endoscopic appearance. Additionally, p53 immunostaining was not performed in three of these eight biopsy specimens, resulting in a total of eight tumors (62%) that lacked histologic evaluation for p53 status prior to ER.
Clinical and histologic characteristics of UC and UCAN in included patients.
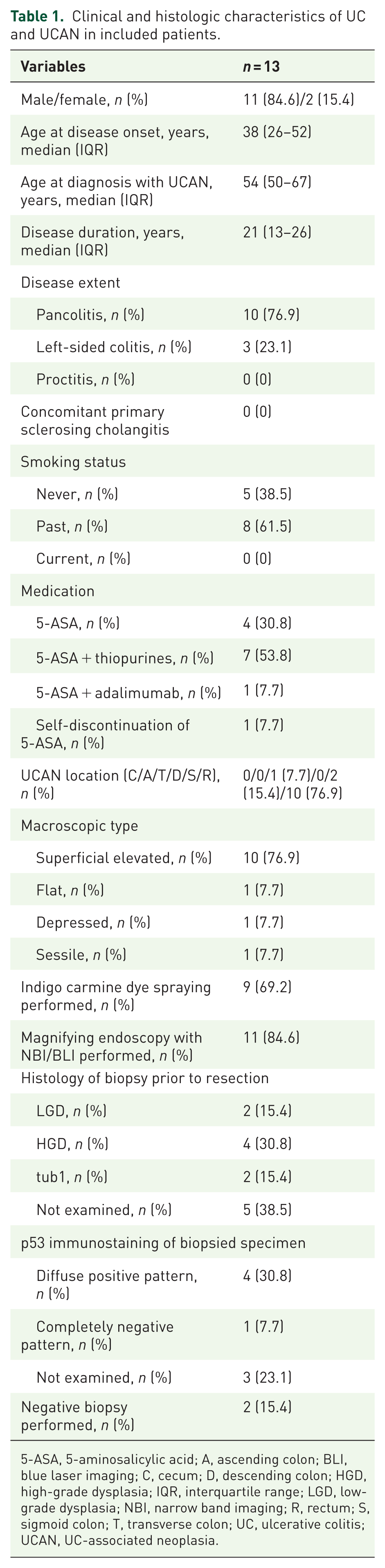
5-ASA, 5-aminosalicylic acid; A, ascending colon; BLI, blue laser imaging; C, cecum; D, descending colon; HGD, high-grade dysplasia; IQR, interquartile range; LGD, low-grade dysplasia; NBI, narrow band imaging; R, rectum; S, sigmoid colon; T, transverse colon; UC, ulcerative colitis; UCAN, UC-associated neoplasia.
Analyses of initial ER
Details of the initial ER procedures are presented in Table 2. Of the 13 tumors, 6 were resected at our hospital—5 by ESD between 2015 and 2017, and 1 by EMR before 2014. All ERs performed after 2018 occurred at other institutions, using CSP, EMR, or ESD techniques. Notably, although the ESD procedures were performed by ESD specialists at each institution, none of these ERs were performed by physicians who are currently board-certified as IBD specialists by the Japanese Society for Inflammatory Bowel Disease. Histologically, 1 tumor (8%) was classified as low-grade dysplasia (LGD), while the remaining 12 lesions represented high-grade dysplasia or more advanced pathology. The depth of invasion was intramucosal in nine cases and submucosal or deeper in four cases. In some cases, thermal effects, proximity to the resection margin, and admixture of dysplastic and non-dysplastic cells hindered accurate assessment of the HM and/or VM, preventing definitive confirmation of negative margins. Three tumors were initially judged to be completely resected; however, additional surgery was performed solely because of lymphovascular invasion. Of the remaining two tumors, retrospective review revealed that negative HMs could not be definitively confirmed. Ten tumors (77%) were confirmed as UCANs with a p53 mutation pattern, but three cases (23%) still lacked p53 immunostaining at this stage.
Clinical and histologic characteristics of UCAN in initial ER.
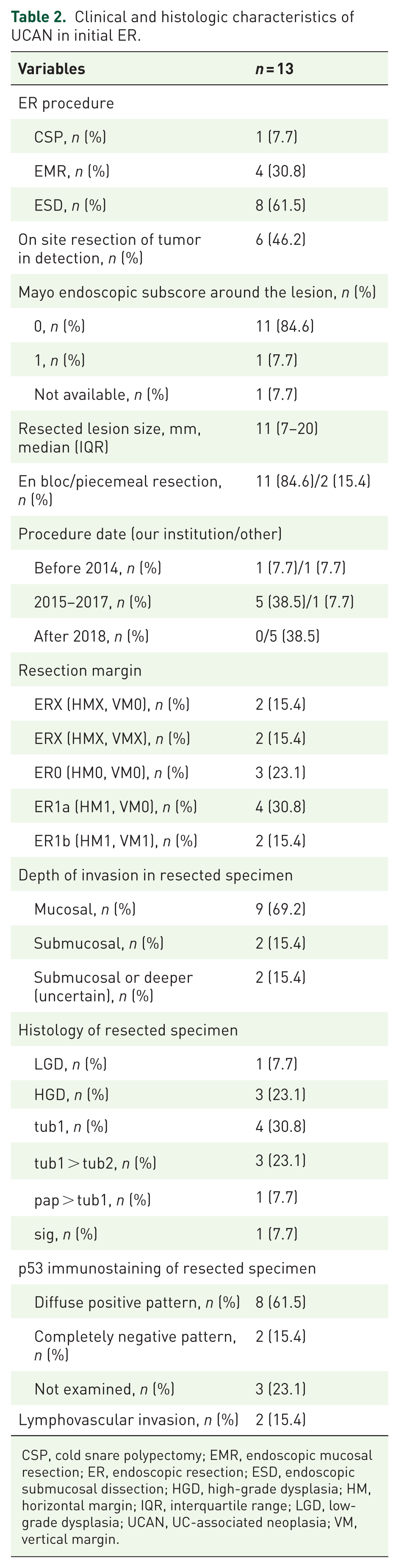
CSP, cold snare polypectomy; EMR, endoscopic mucosal resection; ER, endoscopic resection; ESD, endoscopic submucosal dissection; HGD, high-grade dysplasia; HM, horizontal margin; IQR, interquartile range; LGD, low-grade dysplasia; UCAN, UC-associated neoplasia; VM, vertical margin.
Local residual and recurrence after ER
Clinicopathological features of local residual and recurrent disease following initial ER are summarized in Table 3. Local residuals were suspected in five patients based on histologic findings obtained after ER. Local recurrence was identified in eight patients during a median observation period of 16.5 (IQR: 8.5–23.8) months. Among these eight patients, four (50%) presented with flat lesions at recurrence, and the remaining four (50%) exhibited superficial elevated lesions with adjacent flat dysplastic components. Notably, all flat lesions were diagnosed as local recurrences harboring p53 mutation patterns, despite being resected initially as superficial elevated lesions. The widespread lateral extension of dysplastic tissue was detectable only through detailed endoscopic and histologic assessment—including indigo carmine dye spraying and p53 immunostaining (Figure 3(a) and (b))—highlighting the diagnostic challenge of delineating the horizontal extent of UCAN compared with sporadic tumors (Figure 3(c)).
Clinical and histologic characteristics of local residual or recurrent tumors.

ESD, endoscopic submucosal dissection; IQR, interquartile range; LGD, low-grade dysplasia.

Representative presentation of local recurrence following ER for UCAN. (a) Endoscopic images from two patients who developed local recurrence of dysplasia following ER. Images are shown at three time points: before ER, during ER (top; other institution), and at the time of confirmed local recurrence. (b) Hematoxylin and eosin staining (top) and p53 immunohistochemistry (bottom) of the surgically resected specimen. Scale bars: 1 mm. (c) Schematic illustration comparing local recurrence patterns in sporadic neoplasia (top) versus UCAN (bottom). In UCAN, local recurrence is associated with flat dysplasia extending beyond the elevated lesion.
At the time of recurrence, eight patients underwent proctocolectomy, while repeat ER was attempted in five. Of these five patients, four demonstrated uncontrolled or persistent lesions on repeat ER and subsequently required proctocolectomy. In total, 12 of 13 patients (92%) ultimately underwent proctocolectomy. In the local recurrence group, three patients (38%) had carcinomas that contained previously undetectable components of poorly differentiated, signet-ring cell, or mucinous carcinoma (por/sig/muc; Table 3). Lesion depth was categorized as mucosal in seven cases (54%), submucosal in two (15%), and muscularis propria in one (8%). In the local residual group, two patients had no tumors on the surgical specimen. In the local recurrence group, one patient had a tiny lesion that could be detected endoscopically but was not identifiable in the resected surgical specimen due to its small size. Lymph node metastasis was observed in one case.
Importance of assessing dysplasia in the tissue surrounding the tumor
Of the 13 tumors included in this study, 6 (46%) demonstrated positive HMs and 4 (31%) had margins considered potentially positive following initial ER (Table 2). Notably, six of the eight cases with local recurrence were either confirmed or suspected to have positive HMs. In the remaining cases, recurrences occurred at the post-ER scar margin despite initially histologically negative HMs, which could not be definitively confirmed on retrospective review, strongly suggesting the presence of residual tumor at the initial resection site (Figure 4(a) and (b)). Importantly, as previously described in a single case report, 34 a lesion initially found to have positive HMs on p53 immunohistochemistry was re-evaluated at our institution shortly after ER. Detailed endoscopic examination revealed surrounding flat LGD, and a subsequent ER with appropriately extended margins achieved curative resection without recurrence (Figure 5(a)–(c)). These findings suggest that most local residuals and recurrences resulted from underestimation of the horizontal spread of dysplasia surrounding the elevated neoplastic component (Figure 3(c)).

Representative images of a recurrent lesion with submucosal invasion presenting as a superficial elevated type. (a) Endoscopic images from the same patient before ER (top; our institution, pre-2018) and at the time of local recurrence (bottom), with recurrence detected at the margin of the ER scar (arrowhead). (b) Hematoxylin and eosin staining (top) and p53 immunohistochemistry (bottom) showing poorly differentiated clusters and signet-ring cells in the submucosal layer. (c) Endoscopic images from another patient before ER (other institution) and at recurrence, where inadequate initial assessment complicated evaluation of the vertical margin. (d) Corresponding histologic findings of the surgical specimen (hematoxylin and eosin, top; p53 immunohistochemistry, bottom). Scale bars: 1 mm.

Representative case of successful resection of residual dysplasia after precise identification of the horizontal margin. (a) Sequential endoscopic images at four time points: prior to initial ER, during initial ER (other institution), before additional ER, and during additional ER. (b) Hematoxylin and eosin staining (top) and p53 immunohistochemistry (bottom) of the specimen obtained after additional ER. Scale bars: 1 mm. (c) Schematic illustration showing complete resection of the lesion, including the surrounding flat dysplasia, guided by accurate margin assessment.
Regarding the depth of invasion, three cases were ultimately determined to have submucosal or muscularis propria involvement based on final surgical specimens. Two of these lesions had initially been managed by ER based on their superficial elevated morphology and presumed suitability for endoscopic treatment. However, positive VMs were suspected post-ER, prompting proctocolectomy based on concern for residual disease (Figure 4(c) and (d)). The third lesion, also initially appearing as a superficial elevated tumor, was resected endoscopically with negative HM and VM; however, local recurrence subsequently developed, and histopathologic evaluation of the resected surgical specimens revealed submucosal invasion with a poor component (Figure 4(a) and (b)). These observations suggest that even lesions with a superficial elevated appearance and presumed intramucosal depth may harbor deeper, more aggressive invasion than anticipated based on endoscopic impression alone.
Discussion
This study is the first to detail the endoscopic and clinicopathologic characteristics of patients with UCAN who experienced local residual or recurrent disease following ER, providing valuable insights for endoscopists managing UC-related neoplasia. Our findings suggest that incomplete ER was frequently attributable to under-recognition of the true extent of dysplasia, particularly in flat lesions surrounding superficially elevated tumors. Although local residuals and recurrences were recorded separately, all recurrences in this cohort were considered to have originated from incompletely resected lesions. These results highlight the critical importance of identifying surrounding flat dysplastic areas before and after ER—supported by the use of p53 immunohistochemistry—to minimize the risk of residual disease.
Proctocolectomy has historically been the standard treatment for UCAN; however, ER is increasingly performed, particularly following the publication of the SCENIC consensus guidelines.4,5,35 A growing body of literature has reported local recurrence rates after ER in UC ranging from 0% to 15.3%,9–24 markedly higher than the <1% recurrence rates observed in sporadic colorectal carcinoma. 36 Nevertheless, many of these studies emphasized the technical efficacy and safety of ER, often including a substantial proportion of sporadic tumors arising in patients with UC. Such inclusion may overestimate the effectiveness of ER in true UCAN cases. We are particularly concerned that ER may be applied inappropriately—using paradigms developed for sporadic tumors—without adequate consideration of the unique pathogenesis of UCAN, which frequently originates from flat dysplastic epithelium. This oversight may contribute to increased rates of residual and recurrent disease.
In the present study, the majority of UCANs exhibited a superficial elevated morphology, and ER was frequently performed without sufficient evaluation of the surrounding flat dysplasia. Notably, only 38% (5/13) of tumors were assessed prior to initial resection by p53 immunohistochemistry. Many lesions were managed as if they were sporadic in origin, especially among those initially resected at institutions without specialized expertise in UC. Although this study did not statistically validate this observation, the local residual or recurrence rate was 25% in cases with comprehensive pre-ER assessment—including indigo carmine dye spraying, negative margin biopsy, and p53 immunostaining—compared with 85% in those without such evaluation (Supplemental Figure 1). Our previous work has emphasized the necessity of delineating the horizontal spread of flat dysplasia adjacent to elevated lesions using indigo carmine dye spraying.6,7 Since the implementation of standardized assessments at our institution in 2018, no local residual or recurrent disease has been observed in UCAN cases with p53 mutation patterns, although the number of cases and follow-up duration remain limited. Together, these findings underscore that underestimation of the horizontal extent—often arising from insufficient endoscopic and/or histologic evaluation—may be a key contributor to incomplete resection and disease recurrence in UCAN.
ER may influence subsequent endoscopic interpretation and complicate clinical decision-making, particularly when residual lesions are subtle or masked. In several cases within our cohort, the depth of tumor invasion was underestimated (Figure 4(a)–(d)), and some lesions with flat morphology concealed invasion extending beyond the submucosal layer. Nevertheless, even when the initial ER was incomplete, timely and thorough follow-up assessment—including indigo carmine dye spraying and targeted biopsies of the surrounding mucosa—enabled disease control through additional ER, thereby avoiding surgical intervention in select cases (Figure 5(a)–(c)). These findings suggest the importance of histologic reassessment of resected specimens, particularly in patients with UC, even when lesions are presumed to be sporadic. Routine application of p53 immunohistochemistry can aid in identifying residual flat dysplasia that may not be apparent endoscopically. It is also notable that 38% (3/8) of local recurrence cases in this study harbored por/sig/muc components, which are associated with unfavorable prognosis. 8 These histologic subtypes were not initially detected, suggesting that incomplete resection may facilitate histologic progression of residual neoplasia over time, ultimately increasing the risk of advanced disease. This concern is supported by prior studies on the natural history of UCAN, which have demonstrated that early lesions can progress to advanced carcinoma within approximately 30 months. 37 Collectively, these findings reinforce the necessity of appropriate pre-ER and post-ER histologic evaluation when considering ER as a treatment strategy in UC, and do not support its indiscriminate application in this high-risk population.
This study has several limitations. First, it was a retrospective, single-center investigation with a relatively small sample size, and the results require validation in larger, multicenter cohorts. Nevertheless, to our knowledge, no previous studies have included more than 100 patients with confirmed UCAN while systematically evaluating detailed clinical and histologic outcomes related to ER failure. Second, potential selection bias must be acknowledged. A considerable number of UC-associated tumors are managed as sporadic lesions and may not undergo p53 immunostaining, particularly in cases resected at non-specialist institutions. Moreover, there is substantial variability across institutions in both diagnostic workup and ER technique. Although the ideal approach would involve comprehensive assessment of all UCAN cases undergoing ER—regardless of residual or recurrent outcomes—this was not feasible given the referral-based limitations. Consequently, we were unable to determine the overall recurrence rate among all UC patients undergoing ER. Our analysis therefore focused specifically on residual or recurrent disease in cases definitively diagnosed as UCAN based on p53 mutation patterns, all within our institutional cohort.
Conclusion
This study demonstrated that failure of ER for UCAN frequently results from underestimation of the lesion’s horizontal extent prior to resection. When ER is considered for neoplastic lesions in patients with UC, meticulous pre- and post-procedural evaluation—including indigo carmine dye spraying and immunohistochemical analysis—may reduce the risk of residual disease and recurrence.
Supplemental Material
sj-doc-1-tag-10.1177_17562848261416193 – Supplemental material for Underestimation of the horizontal extent of ulcerative colitis-associated neoplasia may lead to incomplete endoscopic resection and subsequent recurrence
Supplemental material, sj-doc-1-tag-10.1177_17562848261416193 for Underestimation of the horizontal extent of ulcerative colitis-associated neoplasia may lead to incomplete endoscopic resection and subsequent recurrence by Soichiro Murakami, Shinya Sugimoto, Yasushi Iwao, Kaoru Takabayashi, Hiroki Kiyohara, Yusuke Yoshimatsu, Ryoya Sakakibara, Yuta Kaieda, Arina Shigehara, Naoki Hosoe, Motohiko Kato, Yohei Mikami and Takanori Kanai in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-jpg-2-tag-10.1177_17562848261416193 – Supplemental material for Underestimation of the horizontal extent of ulcerative colitis-associated neoplasia may lead to incomplete endoscopic resection and subsequent recurrence
Supplemental material, sj-jpg-2-tag-10.1177_17562848261416193 for Underestimation of the horizontal extent of ulcerative colitis-associated neoplasia may lead to incomplete endoscopic resection and subsequent recurrence by Soichiro Murakami, Shinya Sugimoto, Yasushi Iwao, Kaoru Takabayashi, Hiroki Kiyohara, Yusuke Yoshimatsu, Ryoya Sakakibara, Yuta Kaieda, Arina Shigehara, Naoki Hosoe, Motohiko Kato, Yohei Mikami and Takanori Kanai in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.