
Abstract
Background:
Large common bile duct stones (CBDSs) often require endoscopic papillary large balloon dilation (EPLBD) for removal. However, stone removal is sometimes insufficient when EPLBD is performed using conventional devices such as balloon catheters, basket catheters, and mechanical lithotripsy. Adjunctive electrohydraulic lithotripsy (EHL) is suggested to be useful for large CBDSs that cannot be removed by conventional approach.
Objectives:
The present study aimed to identify pre-procedural predictors for the need for EHL.
Design:
A retrospective, single-center observational study.
Methods:
Patients with CBDSs ⩾10 mm in diameter who underwent EPLBD or EHL between December 2017 and March 2025 were included. Clinical factors associated with the need for EHL in EPLBD to remove large CBDSs were analyzed by multivariate logistic regression. Receiver operating characteristic (ROC) curve analysis was performed to determine the predictive value of the independent risk factors.
Results:
A total of 2881 patients underwent endoscopic retrograde cholangiopancreatography during the study period, 163 patients were included in this study. Among them, CBDS removal with EPLBD could be achieved with conventional devices in 123 patients, while 40 patients required EHL. Multivariate analysis suggested that independent risk factors for the need for EHL in EPLBD to remove CBDSs were a larger maximum bile duct diameter and a higher stone-to-distal bile duct diameter (SD) ratio. In ROC analysis, the SD ratio had the highest area under the curve of 0.82 (95% confidence interval, 0.75–0.89) with an optimal cut-off value of 1.17. The sensitivity, specificity, positive predictive value, and negative predictive value at this cutoff were 0.95, 0.51, 0.39, and 0.97, respectively.
Conclusion:
A higher SD ratio was shown to be a potential independent risk factor for the need for EHL in EPLBD for large CBDSs. Patients with a SD ratio ⩾1.17 may be more likely to require additional treatment. These findings are exploratory and require validation in future studies to confirm their robustness and support their generalizability.
Plain language summary
Large common bile duct stones (CBDSs) can sometimes cause pain or infection, which can occasionally be life-threatening. These CBDSs are often treated with a procedure called endoscopic papillary large balloon dilation (EPLBD), which widens the bile duct using a balloon and removes the CBDSs using conventional devices such as balloon catheters, basket catheters, and mechanical lithotripsy. Adjunctive electrohydraulic lithotripsy (EHL) is suggested to be useful for large CBDSs that cannot be removed by the conventional approach. The present study aimed to identify pre-procedural predictors for the need for EHL. This retrospective single-center study included patients with CBDSs ⩾10 mm in diameter who underwent EPLBD or EHL. A total of 163 patients were included in this study. Among them, CBDS removal with EPLBD could be achieved with conventional devices in 123 patients, while 40 patients required EHL. A higher SD ratio was shown to be a potential independent risk factor for the need for EHL in EPLBD for large CBDSs. Patients with a SD ratio ⩾ 1.17 may be more likely to require additional treatment.
Background
Common bile duct stones (CBDSs) are one of the most common digestive disorders, occurring in approximately 10%–15% of patients with gallstones, and their prevalence increases with age. 1 CBDSs sometimes cause cholangitis, which is accompanied by abdominal pain, and jaundice. Severe cholangitis sometimes progresses to life-threatening conditions. Abdominal computed tomography (CT) or magnetic resonance cholangiopancreatography (MRCP) is generally performed when patients are suspected to have CBDSs. Endoscopic sphincterotomy (ES) is then typical, followed by mechanical extraction to remove the CBDSs. However, large CBDSs (⩾10 mm in diameter) are often difficult to remove using only standard techniques, and alternative or adjunctive treatment strategies are often required.
Several endoscopic techniques have been reported for the treatment of large CBDSs. Among them, endoscopic papillary large balloon dilation (EPLBD), first reported in 2003, dilates the papilla using a large balloon (⩾12 mm) making it easier to remove large CBDSs, which can be difficult to remove with ES or conventional endoscopic papillary balloon dilation (EPBD). 2
EPLBD has been reported to achieve a high success rate (70%–98%) in removing large CBDSs.3,4 Sometimes, however, it is difficult to remove CBDSs even by EPLBD with conventional devices in patients who have large CBDSs, multiple CBDSs, dilated or angulated bile ducts, or impacted CBDSs. 4 Although EPLBD is generally considered to be a safe procedure, there have been reports of procedure-related adverse events such as pancreatitis, bleeding, and perforation. In patients whose CBDSs are difficult to remove with EPLBD, the procedure time and the number of procedures may increase, which potentially raises the risk of complications such as post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis and perforation.5,6
Electrohydraulic lithotripsy (EHL) has been reported to be effective for crushing large CBDSs during ERCP. 7 Recently, in cases in which it is difficult to crush and remove large CBDSs by EPLBD with conventional devices, adjunctive use of EHL has been used. Electrohydraulic shockwaves are used to break up CBDSs under cholangioscopic guidance, and when combined with digital cholangioscopy, this allows for safe and accurate removal of CBDSs under direct visualization. 8
EHL may achieve a higher rate of complete CBDS removal than EPLBD with conventional devices, especially for difficult CBDSs. However, the use of EHL with the cholangioscope (SpyGlass System; Boston Scientific, Natick, MA, USA) involves higher equipment costs and longer procedure times than EPLBD with conventional devices, and therefore its routine use in all cases is not currently recommended. 9 Reducing the number of treatment sessions is important for lowering overall healthcare costs, and selective use of EHL could decrease the need for repeated procedures. 10
Identifying patients at high risk of unsuccessful CBDS removal using EPLBD with conventional devices could help in the planning of the use of adjunctive treatments such as EHL in advance, which could improve efficiency and reduce complications. However, there is currently no universally applicable pre-procedural method to predict which patients will need additional lithotripsy. The present study aims to identify pre-procedural predictors for the need for EHL.
Methods
Study design and patients
This retrospective, single-center cohort study was approved by the institutional review board of Wakayama Medical University (approval number 3401), and procedures were performed in accordance with the Declaration of Helsinki. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement, as recommended by the Equator Network guidelines. The study flow diagram is presented as Figure 1, and the completed STROBE checklist is provided as Supplemental Table 1.

Flowchart showing the patient selection process in the present study conducted between December 2017 and March 2025. After excluding those who underwent other extraction methods, 163 patients were finally included. Among these, CBDS removal was successfully achieved using EPLBD with conventional devices in 123 patients, while 40 patients required EHL.
The study cohort comprised all the consecutive patients who underwent endoscopic CBDS removal for CBDSs at Wakayama Medical University Hospital between December 2017 and March 2025. Because this was a retrospective, single-center study including a relatively small number of patients and without an a priori sample size calculation, all eligible patients during the study period were included in the analysis. Patients were included if the maximum diameter of the CBDSs was ⩾10 mm and if complete CBDS removal was achieved by transpapillary EPLBD or EHL. Patients were excluded if they had surgically reconstructed intestines other than Billroth I, or if other extraction methods were used.
Procedures
When pre-procedural imaging such as CT or MRI reveals CBDSS with a short-axis diameter of ⩾10 mm, we initially attempt CBDS removal using EPLBD with a basket catheter. Sometimes, when the CBDSs are too large to be removed directly, mechanical lithotripsy is required to crush it before it can be removed. In cases where removal is not possible due to the inability to crush the CBDSs, EHL is scheduled on a subsequent day to fragment the CBDSs.
The procedures were performed with duodenoscopes (JF260 or TJF290; Olympus, Tokyo, Japan) under moderate sedation. After successful biliary cannulation, cholangiography was performed using diatrizoate meglumine and diatrizoate sodium (Urografin®; Bayer AG, Leverkusen, Germany) to confirm the presence of CBDSs. In patients with a native papilla, minor ES was usually performed following cannulation, except for patients with a prior ES, who did not generally undergo additional sphincterotomy.
Papillary dilation was performed using a wire-guided large balloon catheter, such as Giga II (Century Medical, Tokyo, Japan), REN (Kaneka Medix, Tokyo, Japan), or StoneMaster V (Olympus, Tokyo, Japan). The balloon was inflated under fluoroscopic guidance until the disappearance of the notch was observed. In accordance with international guidelines on EPLBD, balloon dilation was performed without exceeding the diameter of the distal bile duct. 11
Upon successful CBDS removal, an occlusion cholangiogram was performed using a balloon catheter to confirm the absence of residual CBDSs. If CBDS removal by EPLBD with conventional devices was unsuccessful, EHL was considered. In practice, failure was generally defined when stone removal could not be achieved despite attempts by multiple endoscopists for more than 20 min. In such cases, a plastic stent was placed, and the procedure was finished.
On a subsequent day, EHL was performed under peroral cholangioscopy using the SpyGlass™ DS system for crush of CBDSs. After successful fragmentation of the CBDSs with EHL, CBDSs were removed using a basket catheter, mechanical lithotripsy, and/or balloon catheter, followed by confirmation of complete ductal clearance.
Endpoints and outcome measurements
The primary endpoint of this study was to identify the risk factors associated with the need for EHL in EPLBD for large CBDSs. The secondary endpoints were the determination of optimal cutoff values for the identified risk factors and evaluation of their diagnostic performance, and assessment of procedure-related adverse events such as pancreatitis, bleeding, and perforation.
Number of CBDSs, maximum stone diameter, maximum bile duct diameter, and stone-to-distal bile duct diameter ratio (SD ratio) were used as factors. In addition, several morphological factors that may influence stone-removal difficulty were also evaluated, including impacted stones, cystic-duct insertion-level stones, distal CBD angulation, and distal CBD length. These variables were selected based on prior studies indicating that stone size and the relationship between stone and duct diameter are important determinants of the difficulty of stone clearance.
The parameters “maximum stone diameter/maximum bile duct diameter ratio” and “distal duct tapering” were excluded because both of their component variables or concepts overlapped with the SD ratio. Total bilirubin and periampullary diverticulum were also analyzed, as they have been reported to affect ERCP difficulty. A summary of candidate variables and the reasons for their inclusion or exclusion is provided in Supplemental Table 2.
All radiologic measurements, including the SD ratio, bile duct diameters, and other parameters, were performed on pre-procedural CT or MRCP by two investigators.
The two investigators worked together in the same room and reviewed the images while performing the measurements to ensure consistency. Because these variables were continuous, formal inter-observer agreement statistics such as κ could not be applied. To minimize measurement variability, all measurements were performed using the same digital caliper tool on the PACS system.
The maximum stone diameter was defined as the short-axis diameter of the largest CBDS. The maximum bile duct diameter was measured as the largest diameter in the common bile duct. The distal bile duct diameter was uniformly measured 1 cm above the ampullary orifice.
History of prior biliary interventions, including ERCP or surgery, and post-procedural adverse events were collected from electronic medical records and ERCP reports. Serum total bilirubin and periampullary diverticulum, as well as procedural factors such as the use of antithrombotic agents (single or dual, including direct oral anticoagulants), large balloon diameter, and ES (including prior ES), were also evaluated as potential predictors.
Based on previous reports indicating that both the maximum bile duct diameter and the distal bile duct diameter are associated with procedural difficulty, 9 the SD ratio was calculated and compared between groups as a potential predictor of the need for adjunctive EHL. As in previous studies, successful CBDS removal was defined as complete ductal clearance confirmed by occlusion cholangiogram during the same session.4,9
Statistical analysis
Statistical analyses were primarily performed using JMP software, receiver operating characteristic (ROC) curve analysis was conducted using EZR (Jichi Medical University, Tochigi, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were expressed as medians and interquartile ranges, and categorical variables as numbers and percentages. The Wilcoxon rank sum test was used for comparisons of continuous variables, and Fisher’s exact test was used for categorical variables.
Variables with p-values <0.10 in univariate analyses and other clinically relevant factors were included in the multivariate logistic regression analysis, and the adjusted odds ratios (OR) and 95% confidence intervals (CIs) were calculated. ROC curve analysis was performed for the significant variables in the multivariate analysis. The sensitivity, specificity, positive predictive value, and negative predictive value were also calculated for the optimal cutoff value determined by ROC analysis. All statistical tests were two-sided, with p-values <0.05 being considered statistically significant.
The statistical approach of this study was reviewed and confirmed by a biostatistician at the Clinical Study Support Center, Wakayama Medical University, Wakayama, Japan. Because this was a retrospective study including all eligible patients, no formal sample size calculation was performed.
Results
Patients
Of the 2881 patients who underwent ERCP between December 2017 and March 2025, 1340 underwent CBDSs extraction. Of these, 172 had surgically reconstructed anatomy other than Billroth I and were therefore excluded. Of the remaining 1068 patients with native or Billroth I anatomy, 214 had CBDSs ⩾10 mm in diameter. In total, 51 patients underwent CBDS removal with other extraction methods. After excluding those who underwent CBDS removal through non-transpapillary approaches, 163 patients were finally included in the present study, and EPLBD was attempted in all of them. Of these, complete CBDS removal was achieved using EPLBD with conventional devices in 123 patients, while 40 patients required additional lithotripsy using EHL (24%; Figure 1). The baseline characteristics, procedural details, and outcomes of all 163 patients included in the present study are shown in Table 1. Complications were infrequent in both groups. Post-endoscopic retrograde cholangiopancreatography pancreatitis occurred in two patients (1.6%) in the EPLBD with conventional devices group and two patients (5.0%) in the required EHL group (p = 0.253). Cholangitis occurred in three patients (2.4%) and one patient (2.5%), respectively (p = 1.000). Biliary bleeding occurred in three patients (2.4%) in the EPLBD with conventional devices group, while no cases were observed in the required EHL group (p = 0.427). None of these differences was statistically significant.
Baseline characteristics and outcomes of all included patients (n = 163).

ASA-PS, American Society of Anesthesiologists physical status; CBD, common bile duct; DOAC, direct oral anticoagulant; EHL, electrohydraulic lithotripsy; ES, endoscopic sphincterotomy; IQR, interquartile range; PEP, post-endoscopic retrograde cholangiopancreatography pancreatitis; T-Bil, total bilirubin.
Factors for the need for EHL in EPLBD to remove large CBDSs
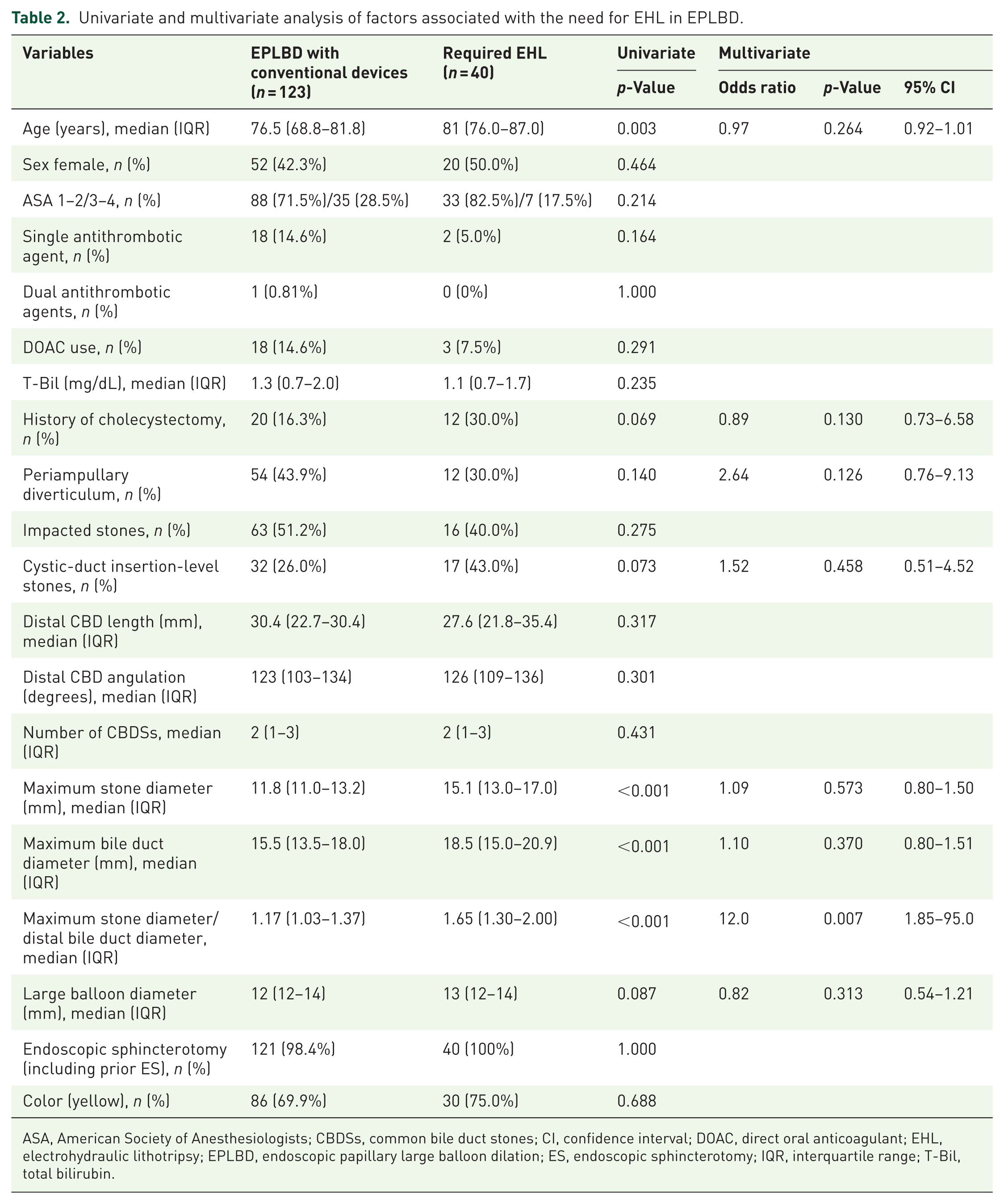
Univariate and multivariate analyses of factors for the need for EHL in EPLBD for large CBDSs are shown in Table 2. Univariate analysis identified seven candidate factors with p < 0.1: age, history of cholecystectomy, maximum stone diameter, maximum bile duct diameter, SD ratio, large balloon diameter, and cystic-duct insertion-level stones. Other factors, including sex, American Society of Anesthesiologists, serum total bilirubin, number of CBDSs, and ES, distal CBD angulation, distal CBD length, impacted stones, and periampullary diverticulum were not significantly associated with the need for EHL. In multivariate analysis, the sole independent significant risk factor was a higher SD ratio (OR, 12.0; 95% CI, 1.85–95.0; p = 0.007).
Univariate and multivariate analysis of factors associated with the need for EHL in EPLBD.
ASA, American Society of Anesthesiologists; CBDSs, common bile duct stones; CI, confidence interval; DOAC, direct oral anticoagulant; EHL, electrohydraulic lithotripsy; EPLBD, endoscopic papillary large balloon dilation; ES, endoscopic sphincterotomy; IQR, interquartile range; T-Bil, total bilirubin.
Predictive ability of the SD ratio
ROC curve analysis was performed to evaluate the predictive ability of the SD ratio for the need for EHL in EPLBD for large CBDSs (Figure 2). The area under the curve was 0.82 (95% CI, 0.75–0.89), indicating good predictive accuracy. The optimal cut-off value for the ratio was determined to be 1.17, with a sensitivity of 0.98 and a specificity of 0.49. The positive predictive value was 0.39, and the negative predictive value was 0.97.

ROC curve for predicting the need for EHL in EPLBD to remove large CBDSs based on the SD ratio. The AUC was 0.82 (95% CI, 0.75–0.89). The optimal cutoff value was 1.17, with a sensitivity of 0.98, and a specificity of 0.49.
Discussion
SD ratio was the sole independent factor associated with the need for EHL in EPLBD for large CBDSs in this study. Our results may indicate that EHL could be considered in cases with an SD ratio ⩾1.17, with high sensitivity and high negative predictive value.
Several studies have investigated strategies for the management of difficult CBDSs, especially when conventional extraction methods failed to remove CBDSs. One suggested a relationship between the anatomical configuration of the bile duct and the difficulty of removing large CBDSs.9,12 In a previous randomized controlled trial involving 66 patients, cholangioscopy-guided lithotripsy using laser was compared with EPLBD for the management of difficult CBDSs. They identified a stone-to-extrahepatic bile duct diameter ratio >1.0 to be a predictor of treatment difficulty (OR, 28.8; p = 0.038). Additionally, the presence of a tapered distal bile duct, defined as a distal-to-proximal duct diameter ratio <0.5, was also significantly associated with a higher failure rate of EPLBD (OR, 26.9; p = 0.034). 9 Another previous study suggested that a more acute distal CBD angulation and a shorter distal CBD arm may predict technical difficulty in CBDS removal procedures. 12
These previous studies have a limitation in that bile duct diameter parameters were measured using cholangiographic images during ERCP. The measured bile duct diameter may therefore have been affected by factors such as volume of contrast injection or the presence of an endoscopic biliary drainage tube placed prior to the procedure. In contrast, we measured bile duct diameter parameters by CT or MRCP to predict the technical difficulty of CBDS removal before the procedure.
In the present study, we first calculated the SD ratio using pre-procedural CT or MRCP. This ratio may be a useful predictor of the need for EHL when performing EPLBD for large CBDSs. The SD ratio reflects both the size of the CBDSs and the diameter of the distal bile duct, and a larger CBDSs is thought to be more difficult to remove. A narrower distal bile duct can prevent the crusher catheter from expanding sufficiently, and this can create difficulty in effectively grasping and breaking up the CBDSs.
The cutoff value identified in the present study was 1.17, with high sensitivity (95.0%) and high negative predictive value (96.9%). Cases below this threshold may be likely to achieve complete CBDS removal with EPLBD with conventional devices. Figure 3 shows the cases for which SD ratio is useful for predicting the need for EHL in EPLBD to remove large CBDSs.

Representative case of an 80-year-old woman with a large CBDS measuring 17 mm and a distal bile duct diameter of 14 mm (a), resulting in an SD ratio of 1.21. EPLBD was performed using a 15 mm balloon (b). After dilation, the CBDS was attempted to be grasped using a four-wire basket catheter. However, due to the narrow distal bile duct, the basket could not expand sufficiently to capture the CBDS (c), and the CBDS could not be removed. A plastic biliary stent was placed for temporary drainage (d). During a second session, peroral cholangioscopy revealed a large yellow CBDS (e). EHL was performed to fragment the CBDS under direct visualization (f). Complete removal of the stone was confirmed by balloon-occluded cholangiography (g).
In clinical practice, measuring the maximum stone diameter and distal bile duct diameter on CT or MRCP before the procedure allows calculation of SD ratio. If SD ratio is ⩾1.17, there may be a higher likelihood that EPLBD with conventional devices will fail in complete CBDSs clearance. In such cases, it may be reasonable to consider the possible need for EHL and to secure sufficient procedure time.
In terms of safety, the incidence of procedure-related complications in this study was low and comparable between the two groups. Post-ERCP pancreatitis occurred in two patients (1.6%) in the EPLBD with conventional devices group and two patients (5.0%) in the required EHL group, without a significant difference. Cholangitis and biliary bleeding were also infrequent and showed no significant group differences. In previous reports by Kim et al. 13 and Park et al., 14 the incidence of post-ERCP pancreatitis after EPLBD ranged from 1% to 4%.
Therefore, the complication rate observed in our study (2.5%) was consistent with these prior findings.
The present study had several limitations. It was a retrospective, single-center study including a relatively small number of patients and without an a priori sample size calculation; therefore, the findings should be regarded as exploratory, which may limit their robustness and generalizability.
In practice, EHL was considered in cases with CBDSs in which mechanical lithotripsy was unsuccessful after multiple endoscopists attempted stone removal for more than 20 min.
However, there were no strictly predefined criteria, and the decision to proceed with EHL was left to the endoscopist’s discretion, which may have introduced operator-dependent variability and potential selection bias.
Further studies are required to confirm these findings and to support their generalizability.
Conclusion
We identified that the SD ratio may be associated with the need for EHL during EPLBD for large CBDSs. SD ratio is a simple, objective, and easily measurable parameter that could aid in assessing treatment strategy for the removal of large CBDSs before ERCP.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251413129 – Supplemental material for Factors associated with the need for electrohydraulic lithotripsy in endoscopic papillary large balloon dilation for giant common bile duct stones
Supplemental material, sj-docx-1-tag-10.1177_17562848251413129 for Factors associated with the need for electrohydraulic lithotripsy in endoscopic papillary large balloon dilation for giant common bile duct stones by Tomokazu Ishihara, Takashi Tamura, Yuto Sugihara, Hiromu Morishita, Hirofumi Yamazaki, Akiya Nakahata, Takaaki Tamura, Yumi Iwahashi, Hiromu Koutani, Takahiro Shishimoto, Tomoya Emori, Yuki Kawaji, Keiichi Hatamaru, Yasunobu Yamashita, Masahiro Itonaga, Takao Maekita, Reiko Ashida, Ke Wan and Masayuki Kitano in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors thank all the members of the Second Department of Internal Medicine and the Clinical Study Support Center at Wakayama Medical University.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.