
Abstract
Background:
The management of small intestinal bacterial overgrowth (SIBO) involves a range of therapeutic options such as antibiotics, probiotics, and prokinetic agents, yet their comparative clinical efficacy remains poorly characterized.
Objective:
To address this critical evidence gap, we systematically evaluated all empirically used treatment regimens through a network meta-analysis (NMA) of published randomized controlled trials (RCTs), with the goal of providing clearer guidance for therapeutic selection.
Design:
We conducted a systematic review and NMA following established methodological standards for evidence synthesis.
Data sources and methods:
Our comprehensive literature search covered PubMed/MEDLINE, Embase, and Web of Science from their inception through December 31, 2024. We included RCTs examining SIBO treatments in adult populations. The extracted data from qualifying RCTs were subjected to Bayesian NMA to (1) conduct pairwise comparisons of empirical SIBO treatment regimens and (2) determine their hierarchical efficacy ranking. The ranking probability for each regimen was evaluated by means of the surfaces under cumulative ranking values.
Results:
Our NMA incorporated 30 eligible RCTs, involving a total of 1552 participants and evaluating 12 distinct interventions. Based on comparative efficacy rankings, berberine was associated with the highest surface under the cumulative ranking curve (SUCRA) value, positioning it as a potentially favorable option for SIBO eradication. In the subgroup of patients with concurrent functional gastrointestinal disorders (FGIDs), the combination of rifaximin and a gastrointestinal motility drug also showed a high SUCRA value (89%), suggesting it may represent a particularly effective regimen in this clinical context. Furthermore, among SIBO patients with chronic liver disease, the gastrointestinal motility drug alone exhibited the most favorable ranking trend (SUCRA: 79.6%). While three of the included studies were assessed as having a high risk of bias (RoB), meta-regression analysis indicated that the RoB did not significantly influence the model outcomes. The confidence in network estimates was generally rated as high across the treatment comparisons.
Conclusion:
This NMA suggests that the management of SIBO may be optimized by considering specific patient comorbidities. Three principal clinical scenarios were identified: First, for patients with uncomplicated SIBO, berberine monotherapy displayed the highest ranking in terms of comparative efficacy. Second, in those with concomitant FGIDs, a combination of rifaximin and a prokinetic agent appeared to be the most promising approach. Finally, among individuals with SIBO and chronic liver disease, prokinetic therapy alone was ranked as the most favorable intervention. These findings highlight the potential for tailored treatment strategies; however, given the methodological heterogeneity and limited sample sizes in some subgroups, the results should be interpreted as generating hypotheses for future validation in well-controlled, direct-comparison studies.
Trial registration:
This NMA was registered with PROSPERO (Registration ID: CRD420251075028).
Introduction
Small intestinal bacterial overgrowth (SIBO) is characterized by excessive colonization of the small intestine by colonic-type bacteria, including both aerobic and anaerobic species.1,2 This condition manifests with a spectrum of gastrointestinal symptoms, most notably abdominal bloating, pain, nausea, and altered bowel habits (constipation or diarrhea).3–5 Despite ongoing controversies regarding optimal diagnostic criteria and detection methodologies,1,6–8 SIBO has emerged as a significant clinical concern due to its high prevalence and substantial impact on patients’ quality of life. Growing evidence suggests SIBO may play a pathophysiological role in numerous systemic conditions such as irritable bowel syndrome, 9 inflammatory bowel disease, 10 liver cirrhosis, 11 digestive system tumors, 12 diabetes, 13 hypothyroidism, 14 systemic sclerosis, 15 and Parkinson’s disease. 16
Despite the availability of multiple therapeutic modalities for SIBO, including antibiotic regimens, 17 probiotic supplementation, 18 dietary modifications, 19 prokinetic agents, 20 and fecal microbiota transplantation, 21 no international consensus exists regarding their hierarchical efficacy. Current treatment guidelines predominantly derive from limited evidence, consisting of small-scale randomized controlled trials (RCTs) of variable methodological quality and conventional pairwise meta-analyses. 1 These approaches fail to provide comprehensive comparisons across all available treatment options. Network meta-analysis (NMA) represents an advanced evidence synthesis methodology that enables simultaneous comparison of multiple interventions by integrating both direct and indirect evidence from RCT networks.22,23 This approach yields robust estimates of relative treatment effects among three or more competing interventions targeting the same clinical outcome. The present study aims to systematically evaluate the comparative effectiveness of all current SIBO treatment options using NMA methodology. Our findings may inform future clinical practice guidelines and facilitate evidence-based therapeutic decision-making for SIBO management.
Methods
Identification of studies and data extraction
This NMA was conducted according to a predefined protocol comprising four sequential phases: study identification, screening, eligibility assessment, and final inclusion. A comprehensive literature search was performed in three major biomedical databases (PubMed/MEDLINE, Embase, and Web of Science) for human studies published through December 31, 2024. The search strategy incorporated a combination of controlled vocabulary (Medical Subject Headings (MeSH) and Emtree terms) and free-text keywords related to SIBO and its treatments, including but not limited to: (“Small intestinal bacterial overgrowth” OR “small bowel bacterial overgrowth” OR “enteric bacterial overgrowth” OR “bacterial overgrowth” OR “SIBO” OR “SBBO”) AND (treatment OR therapy OR therapeutics) AND (“Randomized Controlled Trial” OR “Clinical Trials, Randomized” OR “Trials, Randomized Clinical” OR “Controlled Clinical Trials, Randomized” OR “RCTs”). To ensure comprehensive literature coverage, we supplemented our electronic database search with manual screening of relevant review articles, editorials, and reference lists of all retrieved original studies. Using a standardized data extraction form, two investigators independently abstracted study characteristics and outcome data, with discrepancies resolved through consensus discussion involving a third reviewer when necessary. This NMA was conducted in strict accordance with the PRISMA-NMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Network Meta-Analyses). 24 We employed the GRADE (Grading of Recommendations Assessment, Development and Evaluation) framework to assess the quality of evidence from both direct (pairwise) and indirect (network) comparisons. In addition, we systematically evaluated the confidence in NMA estimates using established methodology to ensure robust interpretation of treatment effect hierarchies. This NMA was conducted in accordance with a pre-defined protocol that was registered on the International Prospective Register of Systematic Reviews (PROSPERO; Registration ID: CRD420251075028).
Study selection
Prior to initiating the systematic review, we established rigorous inclusion and exclusion criteria through an a priori protocol. Studies were deemed eligible for inclusion if they (1) were published as full-text articles, conference abstracts from recognized medical societies, or presented at major gastroenterology congresses with extractable outcome data; (2) employed RCT designs comparing at least two treatment regimens for SIBO; (3) human RCTs only; and (4) to mitigate the risk of bias (RoB) in the systematic review, no language restrictions were applied to the literature search. Studies were excluded based on the following pre-specified criteria: (1) duplication of patient populations; (2) small sample size; (3) and failure to meet any of the other inclusion criteria outlined above. Given the considerable heterogeneity in SIBO treatment approaches across studies, we categorized all interventions into 12 clinically relevant therapeutic classes based on pharmacological mechanisms and treatment modalities identified in the literature. For this NMA, we defined the primary efficacy endpoint as successful SIBO eradication, operationalized through any of the following objective measures: (a) quantitative reduction in small intestinal bacterial density, (b) normalization of hydrogen breath test (HBT) results, or (c) clinically documented improvement in SIBO-related parameters.
Data extraction
Data extraction was conducted independently by two researchers utilizing a standardized form. This form encompassed critical information: author, publication year, country, participant demographics (number, age, gender), concomitant diseases, SIBO diagnostic method, treatment protocols, follow-up duration, and adverse events. SIBO eradication rates were specifically extracted for the NMA.
Subgroup analysis
Prior to data synthesis, we pre-specified three key comorbidity subgroups for analysis: (1) isolated SIBO, (2) SIBO with overlapping functional gastrointestinal disorders (FGIDs), and (3) SIBO with chronic liver disease. This selection was based on the following rationale:
Clinical prevalence and distinct pathophysiology: These three conditions represent the most frequently reported and clinically salient SIBO comorbidities in the extant literature. More importantly, they are hypothesized to involve distinct, yet characteristic, pathophysiological mechanisms leading to SIBO. Isolated SIBO serves as a benchmark for “pure” dysbiosis. SIBO-FGIDs overlap is thought to be driven by visceral hypersensitivity and altered gut–brain axis communication, while SIBO in chronic liver disease is primarily attributed to small intestinal dysmotility and bacterial translocation due to portal hypertension.
Data availability and methodological rigor: A preliminary scoping review of the literature revealed that these three subgroups were the only ones for which a sufficient number of primary studies reported extractable outcome data. This allowed for a statistically robust pooled analysis. By contrast, while comorbidities like diabetes, hypothyroidism, and systemic sclerosis are undoubtedly relevant, the available data in the context of SIBO were found to be too scarce, heterogeneous, or dispersed across studies to permit a meaningful and reliable meta-analysis.
Focus on testable hypotheses: By concentrating on these well-defined subgroups with adequate data, we aimed to provide the most precise and interpretable estimates of SIBO characteristics and treatment responses within these specific patient populations, rather than performing underpowered analyses across numerous comorbidities.
RoB of individual studies
RoB in RCTs was independently assessed by two authors using the revised Cochrane Risk of Bias tool for randomized trials (RoB 2.0). 25 The following five domains were evaluated for each outcome: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. Judgments for each domain were made according to the criteria outlined in the RoB 2.0 guideline and categorized as “Low risk,” “Some concerns,” or “High risk” of bias. The overall RoB for each study was determined based on the worst rating across all domains. Meta-regression was subsequently conducted to examine the influence of RoB. To ensure consistency, any disagreements in the RoB judgments were resolved through discussion between the two authors. In cases where a consensus was not possible, the final judgment was made by a third author.
Statistical analysis
For each pairwise comparison and outcome, risk ratios (RRs) with 95% confidence intervals (CIs) were calculated to quantify the association between interventions. Conventional meta-analyses were performed using both fixed-effects and random-effects models, employing the inverse variance method for each outcome and comparison. Statistical heterogeneity was assessed using the standard Chi-squared (χ2) test, with a significance level of p < 0.1. Significant heterogeneity was defined as an I2 value exceeding 50%. Inconsistency, a critical consideration in NMAs, was also evaluated. 26 To assess potential publication bias, comparison-adjusted funnel plots were constructed, and their symmetry was visually inspected to determine if studies with smaller sample sizes influenced the efficacy results. Potential effect modifiers were investigated through meta-regression. The surface under the cumulative ranking curve (SUCRA) values were employed within rankograms to present the cumulative rank probability for each intervention’s efficacy across the network. SUCRA values were interpreted as the probability of an intervention being among the best (or an ideal intervention) in terms of efficacy, with SUCRA = 1% or 100% indicating the highest achieved efficacy.22,23,27 All data processing and analyses were conducted using Bayesian NMA software, specifically Stata 16.0 (StataCorp, College Station, TX, USA). A two-sided p-value of <0.05 was considered statistically significant for all tests, except for the heterogeneity test, where a p-value of <0.1 was used.
Results
Literature search and quality assessment
Our systematic search initially identified 760 potentially relevant studies. Following the removal of 77 duplicate records, we screened the remaining 683 studies through title/abstract review and subsequent full-text evaluation. Ultimately, 30 RCTs comprising 1552 participants met our predefined inclusion criteria and were incorporated into the NMA (Table 1).28–57 Figure 1 presents the PRISMA-compliant flow diagram detailing the study selection process. The included trials consisted of 25 two-arm28–30,32,33,35–46,48,49,51,52,54–57 and 5 three-arm RCTs,31,34,47,50,53 evaluating 12 distinct therapeutic interventions: (1) rifaximin, (2) placebo, (3) probiotics, (4) metronidazole, (5) quinolones, (6) gastrointestinal motility drug, (7) tetracycline antibiotics, (8) rifaximin + gastrointestinal motility drug, (9) aminoglycosides, (10) ursodeoxycholic acid, (11) berberine, and (12) other combination treatment options. Quality assessment using the Cochrane Risk of Bias tool revealed three studies41,47,54 (10% of included trials) with a high overall RoB, primarily attributable to inadequate allocation concealment or absence of blinding procedures (Figure 2). Meta-regression analysis demonstrated that exclusion of these higher-risk studies did not significantly alter the primary outcome estimates; thus, all trials were retained in the final analytical model to maximize statistical power and clinical generalizability.
Basic demographic data of RCT studies included in the review.

/: Not reported.
GHBT, glucose hydrogen breath test; HMBT, hydrogen methane breath test; LHBT, lactulose hydrogen breath test.
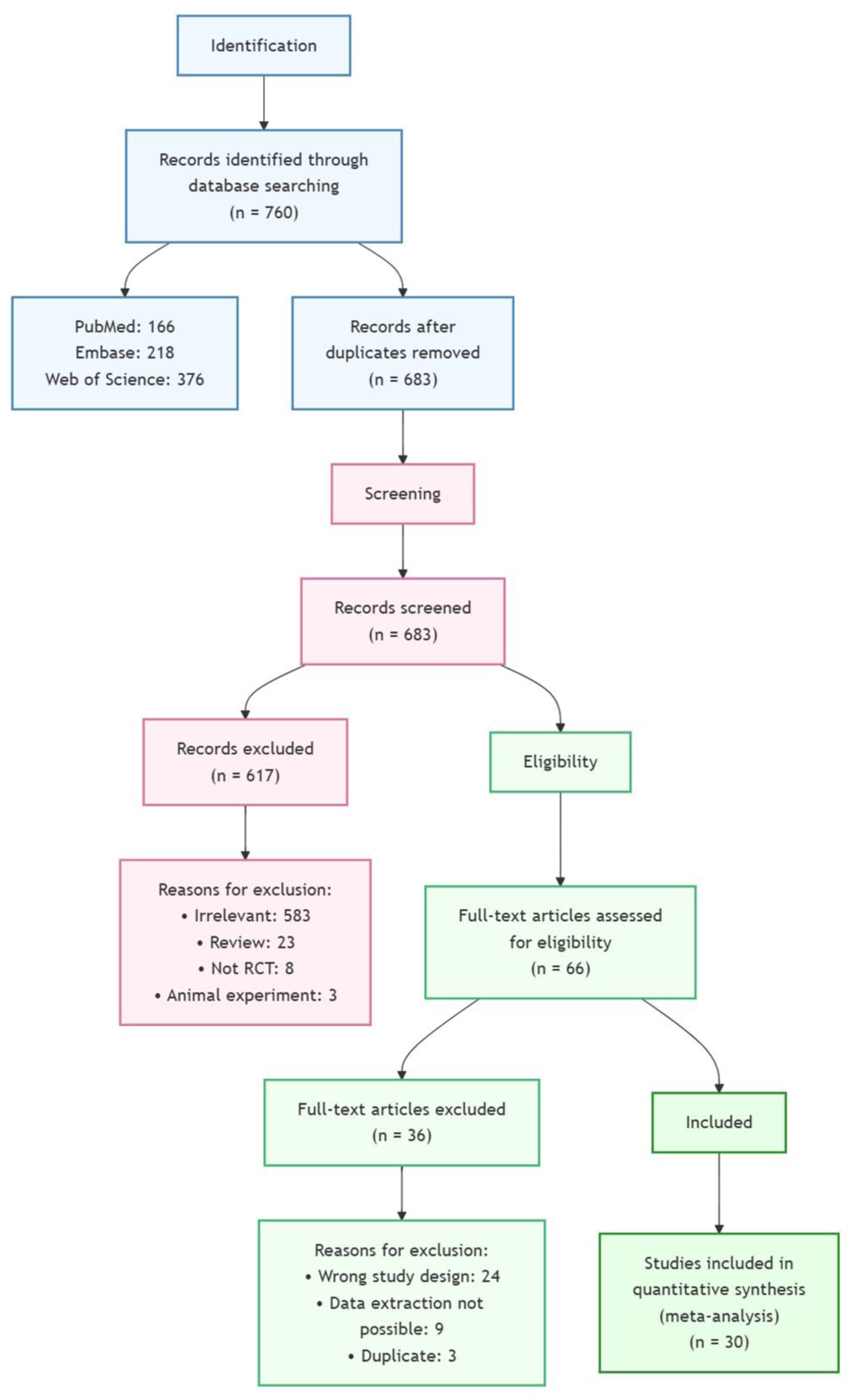
PRISMA flowchart for searching and selecting eligible studies.

Risk of bias summary. This plot provides an overview of the methodological quality assessment for each included randomized controlled trial, as evaluated using the revised Cochrane Risk of Bias tool (RoB 2.0). The studies are labeled as Study 1 through Study 30 for clarity of presentation in the figure. The corresponding author and publication year for each study are as follows: Study 1 (Biancone et al. 28 ), Study 2 (Di Stefano et al. 29 ), Study 3 (Pardo et al. 30 ), Study 4 (Madrid et al. 31 ), Study 5 (Castiglione et al. 32 ), Study 6 (Pimentel et al. 33 ), Study 7 (Lauritano et al. 34 ), Study 8 (Scarpellini et al. 35 ), Study 9 (Parodi et al. 36 ), Study 10 (Lauritano et al. 37 ), Study 11 (Furnari et al. 38 ), Study 12 (Chang et al. 39 ), Study 13 (Collins and Lin 40 ), Study 14 (Jun et al. 41 ), Study 15 (Khalighi et al. 42 ), Study 16 (Kwak et al. 43 ), Study 17 (Lunia et al. 44 ), Study 18 (Ghoshal et al. 45 ), Study 19 (Liang et al. 46 ), Study 20 (Vera et al. 47 ), Study 21 (Furnari et al. 48 ), Study 22 (Tuteja et al. 49 ), Study 23 (García-Collinot et al. 50 ), Study 24 (Kim et al. 51 ), Study 25 (Shi et al. 52 ), Study 26 (Kim et al. 53 ), Study 27 (Duan et al. 54 ), Study 28 (Jo et al. 55 ), Study 29 (Ohkubo et al. 56 ), and Study 30 (Redondo-Cuevas et al. 57 ).
Pairwise meta-analysis
We performed pairwise meta-analyses with corresponding forest plots for all treatment comparisons supported by two or more studies (Figure S1). The analysis revealed significant treatment effects for several therapeutic interventions in achieving SIBO eradication. Notably, rifaximin demonstrated superior efficacy compared to metronidazole (RR, 1.54; 95% CI: 1.17–2.02). When compared to placebo control, the following interventions showed statistically significant improvements in SIBO eradication rates: (1) rifaximin (RR, 2.43; 95% CI: 1.32–4.45), (2) probiotics (RR, 3.35; 95% CI: 2.29–4.89), (3) gastrointestinal motility drug (RR, 7.50; 95% CI: 1.14–49.54), and (4) aminoglycoside antibiotics (RR, 8.39; 95% CI: 1.10–64.16). Assessment of publication bias through funnel plot analysis (Figure S2) demonstrated symmetrical distribution of effect estimates, suggesting minimal likelihood of significant publication bias in our analysis.
NMA results and meta-regression
Figure 3 presents the network map of all treatment comparisons across the 30 included RCTs. In this network plot, node diameters correspond to the sample sizes of respective treatment arms, while edge thickness represents the precision (inverse variance) of each direct comparison. Our analysis encompassed 21 direct treatment comparisons for the primary outcome of SIBO eradication. We performed meta-regression analysis incorporating potential effect modifiers as covariates. Model comparison based on the deviance information criterion revealed minimal differences (<1) between models, indicating no substantial improvement with covariate adjustment. Consequently, the final analysis proceeded without covariate inclusion.
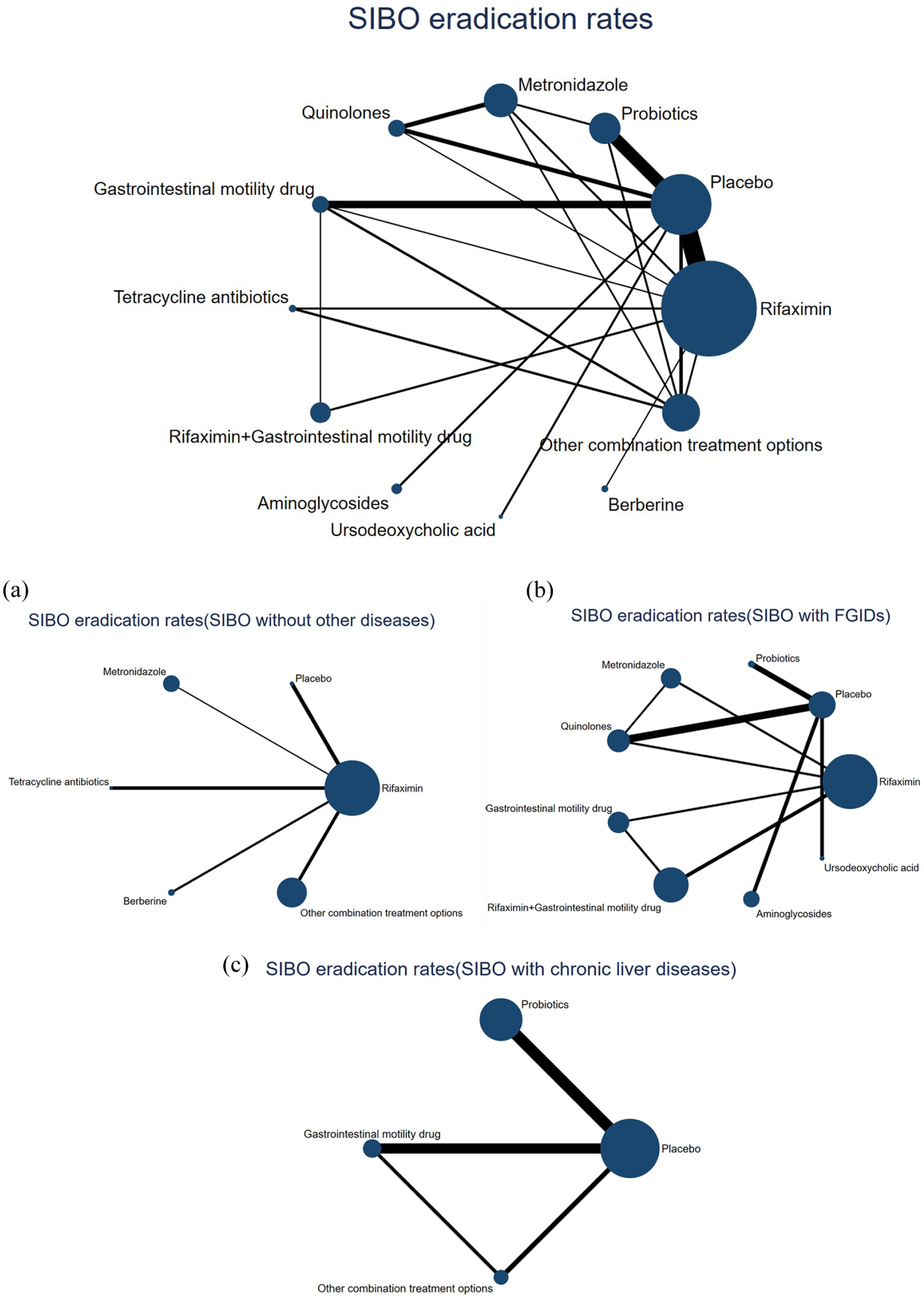
Network geometry for SIBO eradication therapies. Each dot represents a treatment modality. Lines between dots show a direct comparison, for example, a study comparing these two treatments. Thicker lines indicate more studies. (a) Network geometry of SIBO eradication therapy in the absence of other diseases. Each dot represents a treatment modality. Lines between dots show a direct comparison, for example, a study comparing these two treatments. Thicker lines indicate more studies. (b) Network geometry of SIBO eradication therapy in patients with FGIDs. Each dot represents a treatment modality. Lines between dots show a direct comparison, for example, a study comparing these two treatments. Thicker lines indicate more studies. (c) Network geometry of SIBO eradication therapy in patients with chronic liver diseases. Each dot represents a treatment modality. Lines between dots show a direct comparison, for example, a study comparing these two treatments. Thicker lines indicate more studies.
The forest plot using rifaximin as the reference treatment (Figure 4) demonstrated significantly lower efficacy for placebo (RR, 0.11; 95% CI: 0.04–0.28). Berberine, rifaximin + gastrointestinal motility drug, quinolones, and aminoglycosides showed numerically superior efficacy to rifaximin, though these differences did not reach statistical significance.
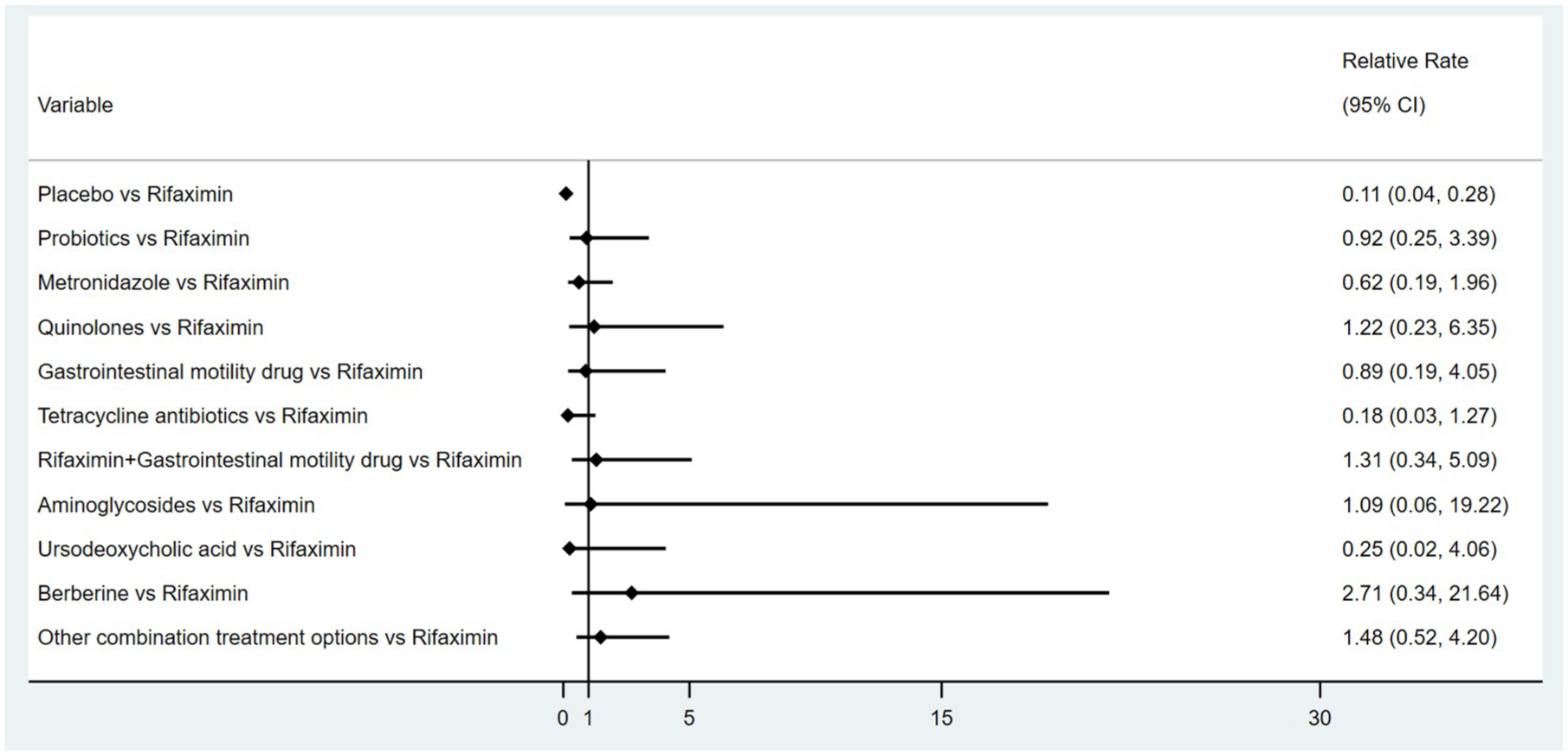
Forest plot for SIBO eradication. Rifaximin compared to the other treatments. Results are presented as differences in eradication of SIBO with 95% confidence intervals.
The SUCRA analysis (Figure 5) established the following efficacy hierarchy: Berberine (SUCRA 82.5%), other combination treatment options (72.5%), rifaximin + gastrointestinal motility drug (66.9%), quinolones (64.0%), aminoglycosides (59.4%), rifaximin (57.5%), probiotics (55.3%), gastrointestinal motility drug (53.5%), metronidazole (40.2%), ursodeoxycholic acid (25.9%), tetracycline antibiotics (16.5%), and placebo (5.9%). These findings were corroborated by the league table of comparative efficacy estimates (Table 2), demonstrating consistent ranking patterns across analytical approaches.

SUCRA plot for eradication of SIBO. SUCRA shows the probability of ranking for each treatment, illustrated by graphs. (a) SUCRA plot for the eradication of SIBO without other diseases. SUCRA shows the probability of ranking for each treatment, illustrated by graphs. (b) SUCRA plot for eradication of SIBO with FGIDs. SUCRA shows the probability of ranking for each treatment, illustrated by graphs. (c) SUCRA plot for the eradication of SIBO with chronic liver diseases. SUCRA shows the probability of ranking for each treatment, illustrated by graphs.
Comparative efficacy ranking league matrix.
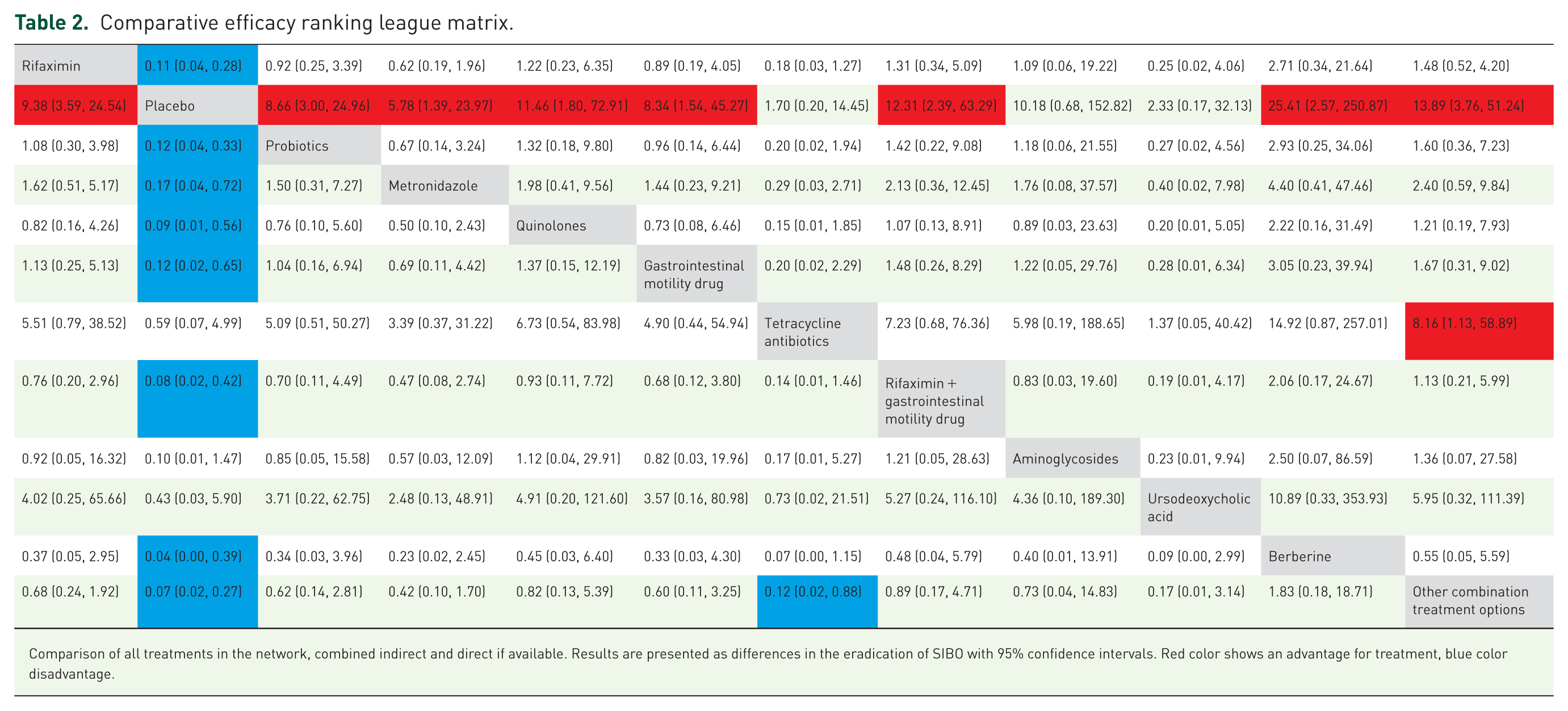

Comparison of all treatments in the network, combined indirect and direct if available. Results are presented as differences in the eradication of SIBO with 95% confidence intervals. Red color shows an advantage for treatment, blue color disadvantage.
Results of subgroup analyses
To evaluate differential treatment responses according to patient comorbidities, we stratified study participants into three clinically relevant subgroups: (1) isolated SIBO (without concomitant diseases), (2) SIBO with FGIDs, and (3) SIBO with chronic liver diseases. Subgroup analyses were performed based on the pre-specified comorbidities, which were selected a priori due to their high clinical relevance, distinct pathophysiological profiles, and the availability of sufficient data for a robust quantitative synthesis, as detailed in the “Methods” section. Publication bias assessment through funnel plot analysis (Figure S3) demonstrated symmetrical distribution of effect estimates across all subgroups, indicating minimal evidence of publication bias.
SIBO without other diseases
This analysis incorporated 8 RCTs29,34,35,37,38,49,54,57 comprising 652 participants, which evaluated 6 distinct therapeutic interventions: (1) rifaximin, (2) placebo, (3) metronidazole, (4) tetracycline antibiotics, (5) berberine, and (6) other combination treatment options. The network geometry for these interventions is presented in Figure 3(a). SUCRA analysis (Figure 5(a)) revealed the following efficacy hierarchy for isolated SIBO: Berberine (SUCRA value 79.4%), other combination treatment options (SUCRA value 74.2%), placebo (SUCRA value 60.4%), rifaximin (SUCRA value 48.8%), metronidazole (SUCRA value 27.7%), and tetracycline antibiotics (SUCRA value 9.5%).
SIBO with FGIDs
This subgroup analysis incorporated 7 RCTs33,45,47,51–53,55 encompassing 383 participants with concurrent SIBO and FGIDs. The evaluated therapeutic interventions comprised: (1) rifaximin, (2) placebo, (3) probiotics, (4) metronidazole, (5) quinolones, (6) gastrointestinal motility drug, (7) rifaximin + gastrointestinal motility drug, (8) aminoglycosides, and (9) ursodeoxycholic acid. The corresponding network geometry is presented in Figure 3(b). SUCRA ranking analysis (Figure 5(b)) demonstrated the following efficacy hierarchy for this patient population: rifaximin + gastrointestinal motility drug (SUCRA 89%), rifaximin (86.2%), gastrointestinal motility drug (61.7%), quinolones (60.3%), probiotics (52.9%), metronidazole (41.9%), aminoglycosides (36.6%), ursodeoxycholic acid (17.1%), and placebo (4.2%).
SIBO with chronic liver diseases
Five RCTs30,31,41,43,44 involving 112 patients with SIBO and underlying chronic liver diseases were included in this subgroup analysis. The investigated treatment modalities included: (1) placebo, (2) probiotics, (3) gastrointestinal motility drug, and (4) other combination treatment options. Network visualization of these interventions is provided in Figure 3(c). As evidenced by the SUCRA analysis (Figure 5(c)), the treatment efficacy ranking for this specific population was as follows: gastrointestinal motility drug (SUCRA 79.6%), other combination treatment options (73.7%), probiotics (46.1%), and placebo (0.6%).
Discussion
Since the 1990s, with the gradual deepening of the cognition of SIBO and the continuous improvement of detection methods, the treatment of SIBO has become an urgent need. SIBO is often complicated by various digestive system diseases, 12 cardiovascular system diseases, 58 endocrine system diseases, 13 and immune system diseases. 15 According to multiple studies, the radical cure of SIBO can enhance the efficacy of drugs for various common concomitant diseases.59,60 But the evidence for several antibiotic regimens recommended by the ACG Clinical Guidelines 1 for SIBO treatment has been limited to small clinical trials of poor to modest quality. Several recent meta-analyses on SIBO treatments have highlighted the efficacy of antibiotics and reported inconsistent results for probiotics. However, these analyses have predominantly focused on comparing single therapeutic strategies and are thus unable to provide comparative effectiveness estimates across different treatment modalities.61–63 To the best of our knowledge, this is the first Bayesian NMA comparing all drug regimens used to cure SIBO.
According to the results of this NMA, berberine demonstrated the highest SUCRA value (82.5%) for SIBO eradication, suggesting a potentially favorable efficacy profile among the interventions evaluated. The observed performance of berberine may be partly explained by its proposed dual mechanism of action, which includes not only direct antimicrobial properties but also a bidirectional interaction with the gut microbiota that may enhance its bioactivity. 64 This finding is clinically relevant as it highlights a potential non-antibiotic alternative at a time when therapeutic options remain limited. The 2020 ACG Clinical Guideline explicitly recognizes the need for expanding the SIBO treatment arsenal, particularly noting the promise of non-absorbable antibiotics and botanical preparations. 1 Nevertheless, these mechanistic insights remain largely derived from preclinical studies, and their direct contribution to clinical outcomes in SIBO patients warrants further validation.
Rifaximin, either as monotherapy (SUCRA: 86.2%) or in combination with a gastrointestinal motility drug (SUCRA: 89.0%), also showed considerable promise in the ranking, particularly in the subgroup of patients with concurrent FGIDs. This finding is consistent with its established position in current treatment guidelines and can be rationalized by its gut-targeted antibiotic activity and documented effects on bacterial load modulation and intestinal barrier function.1,65–67 The enhanced efficacy of the combination regimen underscores the potential benefit of addressing both microbial overgrowth and underlying dysmotility in this patient population. 68
The clinical relevance of addressing gut motility is further illustrated in the context of chronic liver disease. In cirrhosis, portal hypertension can lead to intestinal congestion, edema, and impaired smooth muscle function, which collectively contribute to slowed intestinal transit. This pathophysiological state is characterized by a reduction in the frequency of the small intestinal migrating motor complex, a key mechanism for clearing bacteria, thereby promoting bacterial stasis and overgrowth. 69 In line with this understanding, our subgroup analysis indicated that prokinetic agents (SUCRA: 79.6%) were ranked as the most favorable option for SIBO patients with co-occurring chronic liver disease. This result provides preliminary, clinically coherent evidence that therapies targeting the underlying motility defect may be particularly relevant in this specific subpopulation.
Several crucial limitations must be considered when evaluating the findings of this NMA. Several limitations of this NMA should be considered when interpreting the findings. As with any NMA, the validity of our results is inherently dependent on the quality and reporting transparency of the included trials. A primary concern is that approximately half of the incorporated RCTs were open-label, lacking double-blinding, which could potentially introduce performance and detection bias. However, the RoB was likely mitigated in most of these studies, as the outcome assessment relied on objective measures and the personnel conducting these assessments were often blinded. Furthermore, considerable heterogeneity was observed in the diagnostic methods and criteria for SIBO across studies, a known factor that significantly influences diagnostic yield and complicates cross-trial comparisons.8,70 The interpretability of some subgroup analyses was also constrained by limited sample sizes for certain treatment regimens. Finally, this NMA focused exclusively on comparative efficacy, and a formal assessment of the safety profiles across treatments was beyond its scope. These limitations collectively underscore that the current evidence is not definitive and that our findings should be viewed as generating hypotheses for future research rather than offering conclusive clinical guidance.
Treating SIBO continues to be a challenge. Although in vitro susceptibility testing should ideally guide antibacterial selection, the complexity and high cost of small intestinal bacterial culture limit its widespread use, with breath tests increasingly becoming the preferred diagnostic method. As SIBO management largely remains empirical, targeting both common aerobic and anaerobic bacteria, NMAs of numerous RCTs are essential for ranking treatment efficacy. Promisingly, recent research employing 16S rRNA gene sequencing to profile the gut microbiota in SIBO patients suggests this technology could be a next-generation diagnostic approach that directly informs therapeutic strategies.71,72 Moreover, deep learning-based AI models, by integrating breath test data, clinical symptoms, and gut microbiota features, show potential for SIBO subtyping. A recently developed algorithm, for example, can predict intestinal transit velocity from methane peak times, differentiating between motility-impaired and dysbiosis-related SIBO with over 85% diagnostic accuracy. 73
In summary, this NMA offers a comparative hierarchy of pharmacological treatments for SIBO, with findings suggesting that optimal therapeutic choices may depend on specific patient comorbidities. Berberine emerged with the highest ranking for overall efficacy, indicating it may be a particularly effective option, a profile that held consistent in patients with isolated SIBO. For the subpopulation of patients with concurrent FGIDs, the combination of rifaximin with a gastrointestinal motility drug was ranked as the most favorable regimen. Similarly, prokinetic agents alone were identified as the highest-ranked option for patients with SIBO and coexisting chronic liver disease. These results should be interpreted as generating clinically relevant hypotheses; they highlight promising therapeutic strategies for distinct patient profiles but require confirmation through future dedicated, well-controlled trials that address the limitations inherent in the current evidence base.
Supplemental Material
sj-jpeg-2-tag-10.1177_17562848251399033 – Supplemental material for Comparative efficacy of diverse therapeutic regimens for small intestinal bacterial overgrowth: a systematic network meta-analysis
Supplemental material, sj-jpeg-2-tag-10.1177_17562848251399033 for Comparative efficacy of diverse therapeutic regimens for small intestinal bacterial overgrowth: a systematic network meta-analysis by Qinlin Zhang, Hongliang Li, Changxi Chen, Mengting Li, Jian Song, Shiyu Pan, Baile Shen and Yijia Huang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-jpg-3-tag-10.1177_17562848251399033 – Supplemental material for Comparative efficacy of diverse therapeutic regimens for small intestinal bacterial overgrowth: a systematic network meta-analysis
Supplemental material, sj-jpg-3-tag-10.1177_17562848251399033 for Comparative efficacy of diverse therapeutic regimens for small intestinal bacterial overgrowth: a systematic network meta-analysis by Qinlin Zhang, Hongliang Li, Changxi Chen, Mengting Li, Jian Song, Shiyu Pan, Baile Shen and Yijia Huang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-jpg-4-tag-10.1177_17562848251399033 – Supplemental material for Comparative efficacy of diverse therapeutic regimens for small intestinal bacterial overgrowth: a systematic network meta-analysis
Supplemental material, sj-jpg-4-tag-10.1177_17562848251399033 for Comparative efficacy of diverse therapeutic regimens for small intestinal bacterial overgrowth: a systematic network meta-analysis by Qinlin Zhang, Hongliang Li, Changxi Chen, Mengting Li, Jian Song, Shiyu Pan, Baile Shen and Yijia Huang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-pdf-1-tag-10.1177_17562848251399033 – Supplemental material for Comparative efficacy of diverse therapeutic regimens for small intestinal bacterial overgrowth: a systematic network meta-analysis
Supplemental material, sj-pdf-1-tag-10.1177_17562848251399033 for Comparative efficacy of diverse therapeutic regimens for small intestinal bacterial overgrowth: a systematic network meta-analysis by Qinlin Zhang, Hongliang Li, Changxi Chen, Mengting Li, Jian Song, Shiyu Pan, Baile Shen and Yijia Huang in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.