
Abstract
Background:
Diagnosis of small intestinal bacterial overgrowth (SIBO) remains challenging. This study aimed at proving the diagnostic concept of carbohydrate-specific SIBO (cs-SIBO) using glucose, fructose and sorbitol hydrogen (H2)/methane (CH4) breath testing (HMBT).
Methods:
In this study 125 patients referred to our outpatient clinic for SIBO testing were included. All individuals underwent glucose (50 g), fructose (25 g) and sorbitol (12.5 g) HMBT at 3 consecutive days. Patients with cs-SIBO (i.e. early H2/CH4 peak) were given rifaximin (600 mg/day) in a 10-day treatment. HMBT results were reassessed in a subset of patients 3–6 months after antibiotic therapy. In view of cs-SIBO diagnosis, agreements between HMBT results obtained for different sugars were calculated using Cohen’s kappa (κ) with 95% confidence intervals (CIs).
Results:
A total of 59 (47.2%) patients presented an early H2/CH4 peak with one or more sugars. Among these, 21 (16.8%), 10 (8.0%) and 7 (5.6%) individuals had a positive HMBT result with either glucose, fructose or sorbitol, respectively. Another 21 (16.8%) patients with a positive glucose HMBT result were also found positive with an early H2/CH4 peak obtained after ingestion of fructose and/or sorbitol. Fair agreement was observed between glucose and fructose (κ = 0.26, p = 0.0018) and between glucose and sorbitol (κ = 0.18, p = 0.0178) HMBT results. Slight agreement was observed between fructose and sorbitol (κ = 0.03, p = 0.6955) HMBT results only. Successful antibiotic therapy with rifaximin could be demonstrated in 26/30 (86.7%) of patients as indicated by normal HMBT results and symptom remission.
Conclusions:
Combined glucose, fructose and sorbitol HMBT has the potential to optimize cs-SIBO diagnosis. Furthermore, the majority of patients with cs-SIBO seem to benefit from rifaximin therapy regardless of its carbohydrate specificity.
Introduction
Small intestinal bacterial overgrowth (SIBO) is defined as a heterogeneous syndrome with the presence of an increased number and/or abnormal type of bacteria in the small bowel [Bures et al. 2010; Sachdev and Pimentel, 2013]. The bacteria are mainly of the colonic type and are thus predominantly Gram-negative aerobic and anaerobic species [Lappinga et al. 2010].
SIBO diagnosis may be based on (a) small bowel aspirate culture, (b) hydrogen (H2)/methane (CH4) breath testing (HMBT) or (c) the clinical response to a trial of antibiotics [Grace et al. 2013]. Estimating the true prevalence of SIBO is hampered by the fact that validated standard procedures for the diagnosis of this condition have still not been established [Khoshini et al. 2008]. In addition, SIBO prevalence rates have been shown to vary with study population characteristics (e.g. age, ethnic or geographic origin), diagnostic procedures and nature/dose of substrates used for HMBT [Lupascu et al. 2005; Sachdev and Pimentel, 2013], with glucose and lactulose being most frequently deployed [Gasbarrini et al. 2009].
Although not yet standardized, glucose HMBT is considered a noninvasive, highly reproducible and inexpensive tool for SIBO diagnosis [Lauritano et al. 2009; Bures et al. 2010]. Since glucose is rapidly absorbed in the proximal small bowel, it usually does not reach the colon [Gibson and Barrett, 2010; Gabrielli et al. 2013]. Compared with duodenal aspirate culture, glucose HMBT has a low sensitivity (42%) but a high specificity (84%) for the detection of SIBO [Erdogan et al. 2015]. However, duodenal aspiration is cumbersome and has its own difficulties and limitations [Simren and Stotzer, 2006; de Lacy Costello et al. 2013; Enko et al. 2014], because many bacteria cannot be cultured and cell counts determined in vitro may not reflect the population in vivo [Gibson and Barrett, 2010].
Therefore HMBT has been suggested for SIBO diagnosis [de Lacy Castello et al. 2013]. After glucose administration, an early increase in breath H2 and/or CH4 (i.e. single early peak within 60 minutes after sugar ingestion) indicates bacterial glucose fermentation in the small bowel [Bures et al. 2010]. An early peak observed after the ingestion of other carbohydrates such as lactose, fructose or sorbitol is also considered to be indicative of SIBO [Nucera et al. 2005; Eisenmann et al. 2008; Enko et al. 2014, 2015; Goebel-Stengel et al. 2014]. A recent study putatively suggested carbohydrate-specific SIBO (cs-SIBO) to be present in 6.53% and 4.58% of 306 Austrian patients with suspected carbohydrate malabsorption syndromes by fructose and sorbitol HMBT, respectively [Enko et al. 2015].
The use of a broad-spectrum antibiotic therapy, capable of eradicating aerobes and anaerobes, is recommended for SIBO treatment with rifaximin being the substance of choice [Lichtenstein, 2007; Peralta et al. 2009]. Rifaximin is an intestinally targeted oral antibiotic with high luminal activity and minimal absorption (<0.4%) [Lichtenstein, 2007]. It has been proven to be effective against Gram-positive as well as Gram-negative bacteria, including aerobes and anaerobes [Scarpellini et al. 2007].
This study aimed at proving the diagnostic concept of cs-SIBO using glucose, fructose and sorbitol HMBT in a cohort of 125 patients referred to our outpatient clinic for SIBO testing. To furthermore substantiate our concept of carbohydrate specificity, patients were prescribed rifaximin (600 mg/day for 10 days), and treatment outcome was monitored in a subset of patients 3–6 months after antibiotic therapy.
Materials and methods
Ethical approval
This study was approved by the Ethical Committee of Upper Austria, Linz, Austria, and carried out in accordance with the Helsinki Declaration. All participants gave their written informed consent.
Study design and participants
A total of 125 adult patients, referred to our outpatient clinic for SIBO testing, were included in this prospective study. The study period was from 1 June 2014 to 30 June 2015. The inclusion criteria for this study were: patients referred for SIBO testing; a minimum age of ⩾18 years; an obligatory overnight fasting state and a nonsmoking period of >12 hours. Patients with abdominal symptoms during the first HMBT were able to perform further tests in a consecutive manner on the following workdays. The exclusion criteria were: colonoscopy or antibiotic-based therapy at least 4 weeks before HMBT; proton pump inhibitor intake at least 2 weeks before HMBT; and patients with active acute or chronic inflammatory bowel disease.
Glucose HMBT
Gas chromatography was employed using a QuinTron Model DP Plus MicroLyzerTM (QuinTron, Milwaukee, WI, USA). Baseline breath H2/CH4 concentrations were determined after an overnight fasting state 12 hours) with values < 20 parts per million (ppm) being a prerequisite for HMBT. After determining baseline breath H2/CH4 concentrations, glucose was given in a dose of 50 g dissolved in 200 ml of water, and end-expiratory breath H2/CH4 concentrations were measured at 15, 30, 45, 60, 75, 90 and 120 minutes after sugar ingestion. According to the literature [Gasbarrini et al. 2009; Rana et al. 2012], patients with a H2 and/or CH4 rise of ⩾10 ppm above baseline were diagnosed with cs-SIBO. cs-SIBO eradication after antibiotic therapy was defined by the absence of the H2 and/or CH4 peak [Parodi et al. 2008, 2009]. The preconditions for the interpretation of a positive response of glucose HMBT to antibiotic therapy were a decrease of ⩾5 ppm as well as H2 and CH4 measurements of <10 ppm above the baseline value anytime during recording. Patients were asked to report clinical symptoms and to refrain from physical effort, smoking or eating during the HMBT.
Fructose and sorbitol HMBT
Gas chromatography was employed using the QuinTron Model DP Plus MicroLyzerTM (QuinTron, Milwaukee, WI, USA). Baseline breath H2/CH4 concentrations were determined after an overnight fasting state (12 hours) with values < 20 ppm being a prerequisite for HMBT. After determining baseline breath H2/CH4 concentrations, fructose or sorbitol was given in a dose of 25 g and 12.5 g, respectively, dissolved in 200 ml of water [Eisenmann et al. 2008]. Based on former studies [Eisenmann et al. 2008; Enko et al. 2014, 2015; Goebel-Stengel et al. 2014], patients with an early H2 and/or CH4 increase ⩾20 ppm above baseline within 60 minutes after sugar ingestion (i.e. small intestinal passage) were diagnosed with cs-SIBO. cs-SIBO eradication after antibiotic therapy was defined by the absence of the H2 and/or CH4 peak [Parodi et al. 2008, 2009]. The preconditions for the interpretation of a positive response of fructose and sorbitol HMBT to antibiotic therapy were a decrease of ⩾10 ppm as well as H2 and CH4 measurements of <20 ppm above the baseline value anytime during recording. Patients with a H2/CH4 peak ⩾20 ppm within 60–120 minutes (i.e. colonic passage) were classified as malabsorbers [Eisenmann et al. 2008; Enko et al. 2014, 2015; Goebel-Stengel et al. 2014]. Patients with abdominal symptoms during the first HMBT were able to perform further tests in a consecutive manner on the following workdays.
Treatment modalities
Based on existing recommendations [Bures et al. 2010], rifaximin was administered to patients with cs-SIBO in a 10-day treatment (600 mg/day). A period of 3–6 months after antibiotic treatment, HMBT results were reassessed in 30/59 (50.8%) individuals diagnosed with cs-SIBO.
Statistical analysis
Descriptive statistics were performed to analyze glucose, fructose and sorbitol HMBT results. The exact chi-squared test for independence was used to compare HMBT results of different sugars before and after antibiotic therapy. The agreements between HMBT results obtained for different sugars were calculated using Cohen’s kappa (κ) with 95% confidence intervals (CI). The interpretation of κ was performed according to the literature (κ: 0.01–0.20 = fair; 0.21–0.40 = slight; 0.41–0.60 = moderate; 0.61–0.80 = substantial; 0.80–0.99 = almost perfect agreement) [Viera and Garrett, 2005]. No adjustment for type I error was made. Therefore the concerning p values are only descriptive. Analyse-it® software version 2.30 (Analyse-it Software, Ltd, Leeds, UK) was used for statistical analysis.
Results
Patient characteristics
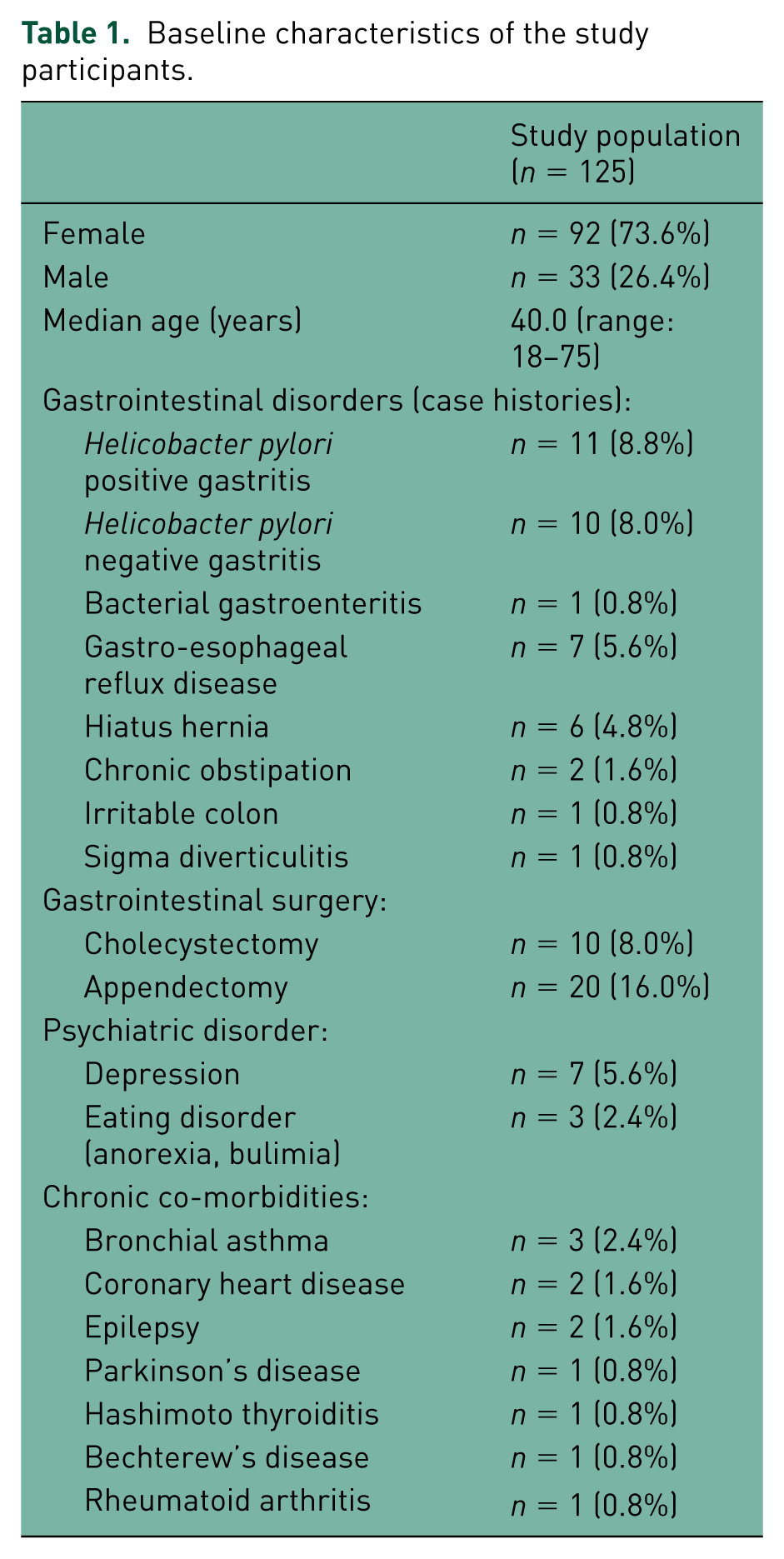
In total, 125 patients were included of whom 92 (73.6%) were female and 33 (26.4%) were male. The median age was 40.0 (range: 18–75) years. Baseline demographic and clinical characteristics are shown in Table 1. A total of 40 (32.0%) of all patients presented a pre-existing gastrointestinal disorder (e.g. gastritis, gastroesophageal reflux) in their case histories, 32/125 (24.0%) had already had gastrointestinal surgery and 10/125 (8.0%) individuals were identified with a psychiatric disorder diagnosis. None of the patients suffered from celiac disease, or showed signs of active acute or chronic inflammatory bowel or infectious disease.
Baseline characteristics of the study participants.
cs-SIBO diagnosis
As shown in Table 2, 59/125 (47.2%) patients presented an early H2/CH4 peak with ⩾1 sugars. In total, 21/125 (16.8%), 10/125 (8.0%) and 7/125 (5.6%) individuals had a positive HMBT result exclusively with either glucose, fructose or sorbitol. Another 21/125 (16.8%) patients with a positive glucose HMBT were also found positive with an early H2/CH4 peak obtained after ingestion of fructose and/or sorbitol.
Carbohydrate-specific small intestinal bacterial overgrowth (cs-SIBO) as diagnosed by hydrogen/methane breath test (HMBT).

All patients (n = 125) underwent glucose (50 g), fructose (25 g) and sorbitol (12.5 g) HMBT for 3 consecutive days. A total of 59/125 (47.2%) individuals presented an early H2/CH4 peak with ⩾1 sugars. The exact chi-squared test was used to demonstrate therapy success for different sugars (glucose: p = 0.0048; fructose: p = 0.0038; sorbitol: p = 0.0020).
Table 3 illustrates Cohen’s κ test results. Low-grade interobserver agreement between different carbohydrates was observed: fair agreement was observed between glucose and fructose (κ = 0.26, p = 0.0018) and between glucose and sorbitol (κ = 0.18, p = 0.0178) HMBT results. Slight agreement was observed between fructose and sorbitol (κ = 0.03, p = 0.6955) HMBT results only.
Interobserver agreement for glucose-, fructose- and sorbitol-specific small intestinal bacterial overgrowth.
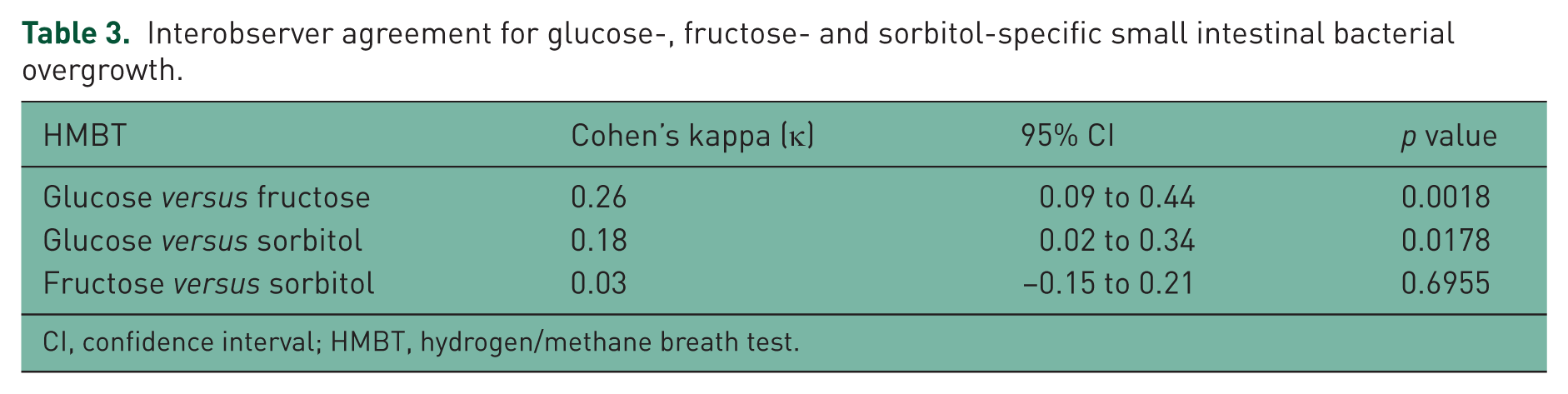
CI, confidence interval; HMBT, hydrogen/methane breath test.
cs-SIBO treatment
In total, 30/59 (50.8%) individuals with cs-SIBO were reassessed with HMBT 3–6 months after rifaximin therapy. Of note, a positive HMBT response after antibiotic treatment was obtained for 26/30 (86.7%) of these patients. In 4/30 (13.3%) individuals HMBT remained pathologic. Twenty-two (84.6%) and two (50%) individuals with successful and frustrane antibiotic therapy, respectively, reported either complete remission or distinct improvement of gastrointestinal symptoms. A positive response to antibiotic therapy for different carbohydrates was observed as follows: glucose: 15/17 individuals (p = 0.0048); fructose: 7/8 individuals (p = 0.0038); and sorbitol: 6/7 individuals (p = 0.0020). Figure 1 illustrates HMBT results obtained for three patients with cs-SIBO before and after antibiotic therapy.

Hydrogen/methane breath test (HMBT) results for three individuals diagnosed with carbohydrate-specific small intestinal bacterial overgrowth (cs-SIBO) before (a, c, e) and after (b, d, f) a 10-day treatment (600 mg/day) with rifaximin. ppm, parts per million.
Fructose/sorbitol malabsorption
Fructose and sorbitol malabsorption was diagnosed in 16/125 (12.8%), and 38/125 (30.4%) patients, respectively, with a positive fructose and sorbitol HMBT found in 11/125 (8.8%) individuals. Interestingly, concomitant cs-SIBO was observed in 12/125 (9.6%) and 9/125 (7.2%) patients with fructose and sorbitol malabsorption, respectively.
Self-reported symptoms during HMBT
Taken together, 42/125 (33.6%), 29/125 (23.2%) and 46/125 (36.8%) patients reported ⩾1 symptoms (i.e. abdominal pain, bloating, diarrhea, nausea, heartburn, burping, malaise, headache or dizziness) during glucose, fructose and sorbitol HMBT. Of these, 17/125 (13.6%), 16/125 (12.8%) and 22/125 (17.6%) individuals showed a positive HMBT with glucose, fructose and sorbitol, respectively, indicating cs-SIBO and/or carbohydrate malabsorption.
Discussion
This proof-of-concept study aimed at refining SIBO as diagnosed by HMBT and based on its carbohydrate specificity (i.e. cs-SIBO). For this reason, glucose, fructose and sorbitol HMBT was performed on 3 consecutive days for all 125 patients referred to our outpatient clinic for SIBO testing. Herein, 59/125 (47.2%) patients were diagnosed with cs-SIBO, of whom 21/125 (16.8%), 10/125 (8.0%) and 7/125 (5.6%) individuals were exclusively identified by glucose, fructose and sorbitol HMBT, respectively. These results indicate that 17/125 (13.6%) patients would not have been identified with cs-SIBO, if diagnosis had been based on glucose HMBT only.
Currently, glucose and lactulose are the most frequently used carbohydrates for SIBO diagnosis by HMBT. Regardless of substrate dose and test duration, glucose HMBT has shown greater diagnostic accuracy than that performed using lactulose [Gasbarrini et al. 2009; Rana et al. 2012]. In this study, and according to the literature [Gasbarrini et al. 2009; Rana et al. 2012], glucose HMBT was suggestive of SIBO, if breath H2 and/or CH4 increased ⩾10 ppm above baseline. While glucose HMBT is a well established method for SIBO diagnosis, a high degree of heterogeneity and multiple definitions for HMBT positivity exist [Khoshini et al. 2008]. For example, higher cutoff values were shown to reduce test sensitivity (i.e. <60%) [Gasbarrini et al. 2009].
Moreover, it has been demonstrated that a cutoff value ⩾20 ppm above baseline within 60 minutes after fructose or sorbitol ingestion (i.e. small intestinal passage) is indicative of cs-SIBO [Eisenmann et al. 2008; Enko et al. 2014, 2015; Goebel-Stengel et al. 2014]. For cs-SIBO testing by HMBT, this study observed fair (glucose and fructose: κ = 0.26, p = 0.0018; glucose and sorbitol: κ = 0.18, p = 0.0178) and slight (fructose and sorbitol: κ = 0.03, p = 0.6955) agreement. As shown in Table 2, 38/59 (64.4%) individuals diagnosed with cs-SIBO were exclusively identified by either glucose, fructose or sorbitol HMBT. This finding indicates that bacterial fermentation in the small bowel is carbohydrate-specific, with SIBO prevalence rates found to be dependent on the nature and dose of sugar used for HMBT in a clinical setting [Sachdev and Pimentel, 2013; Enko et al. 2015].
With respect to treatment, 59/125 (47.2%) patients diagnosed with cs-SIBO received antibiotic therapy with rifaximin. Of these, 30/59 (50.8%) individuals underwent a follow-up HMBT 3–6 months after antibiotic therapy. Of these therapeutic success and failure was found in 26 (86.7%) and 4 (13.3%) individuals, respectively. In contrast, numerous previously published studies demonstrated lower rates of successful therapy (62–70%) using a 10-day treatment with 1200 mg/day rifaximin [Parodi et al. 2008, 2009; Furnari et al. 2010].
Based on existing recommendations [Bures et al. 2010], rifaximin was administered in a 10-day treatment (600 mg/day). However, an optimal design of antibiotic treatment has not yet been established yet [Shah et al. 2013]. Although rifaximin is considered a safe and effective antimicrobial drug with minimal toxicity and negligible systemic side effects, more studies on optimal dosing and treatment duration schemes also assessing risks of Clostridium difficile colitis and microbial antibiotic resistance in patients with repeated courses of antibiotic therapy are required [Schoenfeld et al. 2014; Iorio et al. 2015].
Study limitations include that lactulose HMBT was not implemented to determine the oro-cecal transit time and only a subset of patients with cs-SIBO was reassessed after antibiotic therapy. Furthermore, the costs associated with additional personell and laboratory consumables for the diagnostic procedure presented here were not evaluated.
Conclusion
The low-grade interobserver agreement between glucose, fructose and sorbitol HMBT observed in the present study suggests, that SIBO diagnosis may be made on the basis of carbohydrate specificity. Furthermore, the majority of patients with cs-SIBO were shown to benefit from antibiotic therapy with rifaximin, regardless of its carbohydrate specificity. However, further studies are warranted to corroborate our findings and to evaluate costs associated with additional personnel and laboratory consumables for the diagnostic approach proposed here.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.