
Abstract
Background:
A combination of immune checkpoint inhibitors and chemotherapy has emerged as standard therapy in advanced human epidermal growth factor receptor 2-negative advanced gastric cancer (AGC). However, the clinical benefit in patients with a low combined positive score (CPS) of 1–4 remains controversial.
Objectives:
To evaluate the efficacy and safety of nivolumab plus chemotherapy in AGC patients with low CPS (1–4) in a real-world clinical setting.
Design:
A retrospective single-center study conducted at Samsung Medical Center.
Methods:
We analyzed outcomes in AGC patients with CPS 1–4 who received nivolumab in combination with capecitabine and oxaliplatin (XELOX) or fluorouracil, oxaliplatin, and leucovorin (FOLFOX) as first-line therapy between April 2021 and December 2024. Tumor response was assessed using Response Evaluation Criteria in Solid Tumor version 1.1. Progression-free survival (PFS) and overall survival (OS) were estimated using Kaplan–Meier methods.
Results:
Of 336 patients receiving first-line nivolumab plus XELOX or FOLFOX, 63 had a CPS of 1–4. Median age was 61 years, and the most common CPS was 1, found in 26 patients (41%). One patient achieved a complete response (2%), and 25 patients achieved partial response (40%), for an overall response rate of 42%. Stable disease was observed in 23 patients, a disease control rate of 76%. Median PFS was 5.8 months (95% confidence interval (CI), 4.9–6.7), and median OS was 15.0 months (95% CI, 13.2–18.7). Any-grade adverse events were reported in 92% of patients, while grade 3 or 4 treatment-related adverse events occurred in 61% of patients, most commonly anemia and neutropenia.
Conclusion:
This real-world retrospective study suggests modest efficacy of AGC patients with low CPS treated with nivolumab with chemotherapy. Further studies are needed to determine the optimal treatment strategy and to identify predictive biomarkers for therapy selection in patients with low-CPS AGC.
Plain language summary
Gastric cancer is one of the most common and deadly cancers worldwide. For patients with advanced gastric cancer, treatment options are limited, and outcomes are often poor. In recent years, a new class of drugs called immune checkpoint inhibitors—such as nivolumab—has been used together with traditional chemotherapy. However, it is unclear whether patients with low levels of a protein called PD-L1 (specifically CPS 1–4) can benefit from this combination treatment. Doctors at Samsung Medical Center studied 63 patients with advanced gastric cancer who had low PD-L1 levels. All patients received a combination of nivolumab and standard chemotherapy as their first treatment. The goal was to understand how well this treatment worked and how safe it was in real-world clinical practice. Treatment Effectiveness: About 47% of patients showed tumor shrinkage or stable disease. Survival: On average, cancer did not worsen for 5.8 months after starting treatment, and patients lived for a median of 15.0 months. Most patients (92%) had some side effects. Serious side effects (grade 3 or higher) occurred in 61% of patients, most commonly anemia and low white blood cell counts. Immune-related side effects such as lung inflammation occurred in a few patients. This study suggests that even patients with low PD-L1 levels might benefit from nivolumab plus chemotherapy, though more research is needed. The side effects were generally manageable, but careful monitoring is important. Future studies should focus on identifying which patients are most likely to benefit from this treatment.
Introduction
Gastric cancer is the fifth most commonly diagnosed cancer globally, accounting for 4.9% of newly diagnosed cases, and is the fifth leading cause of cancer-related death. 1 Advanced gastric cancer (AGC) has long been associated with a poor prognosis, with an estimated 5-year survival of about 10%. 2 The treatment landscape of gastric cancer has experienced a major transformation in recent years, driven by increasing integration of immunotherapy in cancer management. The CHECKMATE-649 and ATTRACTION-04 studies have demonstrated that nivolumab, a PD-1 inhibitor, in combination with chemotherapy provides a clinical benefit over chemotherapy alone in regard to progression-free survival (PFS) in human epidermal growth factor receptor 2 (HER-2)-negative AGC. In addition, the CHECKMATE-649 trial reported significant improvement in overall survival (OS) compared to chemotherapy alone.3,4 Similarly, the KEYNOTE-859 trial demonstrated significantly improved survival outcomes with the addition of pembrolizumab to chemotherapy when used as a first-line treatment for HER2-negative AGC. 5 Based on these findings, the FDA has approved the combination of nivolumab and chemotherapy for patients with a combined positive score (CPS) ⩾1. 6 Current American Society of Clinical Oncology (ASCO) guidelines recommend the combination of immunotherapy and chemotherapy for patients with CPS ⩾5. 7 For those with CPS <5, treatment decisions should be individualized, whereas conventional chemotherapy remains the standard recommendation for patients with CPS 0. 7
These studies represent an important advancement in the treatment of AGC. Subgroup analyses of these clinical trials suggest that patients with CPS ⩾5 can expect reasonable benefit from combination chemotherapy with nivolumab. 8 In patients with PD-L1 expression of low CPS <5, further investigation is required to refine patient selection and optimize treatment strategies, especially considering cost-effectiveness and additional side effects of combination therapy. 9 This raises an important clinical question regarding the optimal treatment approach for patients with a CPS score of 1–4, a subgroup known to derive limited benefit from combination therapy of nivolumab and chemotherapy.
In the present study, we evaluated the efficacy and safety profile of nivolumab plus chemotherapy in AGC patients with PD-L1 expression of CPS <5 in routine clinical practice.
Methods
Study population
This study included patients with AGC receiving nivolumab with capecitabine and oxaliplatin (XELOX) or leucovorin, fluorouracil, and oxaliplatin (FOLFOX) as first-line treatment in routine clinical practice at Samsung Medical Center from April 2021 to December 2024. The data cutoff was March 12, 2025. Patients with a PD-L1 CPS score of 1–4 were identified from the treated cohort, and PFS and OS were analyzed. We reviewed the electronic medical records (EMRs) and extracted data on age, sex, Eastern Cooperative Oncology Group (ECOG) performance status, tumor mutation burden (TMB), microsatellite instability (MSI) status, tumor location, HER-2 positivity determined by immunohistochemistry, next-generation sequencing data, histopathological stage at initial diagnosis, and distant metastatic sites at initiation of nivolumab with chemotherapy and side effect profile. The PD-L1 CPS score was evaluated using the Dako PD-L1 IHC 28-8 pharmDx assay (28-8; Dako, Agilent Technologies, Inc,Santa Clara, CA, USA). For the FOLFOX regimen, patients received nivolumab at a fixed dose of 240 mg every 2 weeks, in combination with oxaliplatin 85 mg/m2 and leucovorin 200 mg/m2, followed by a 5-fluorouracil bolus of 400 mg/m2 and a continuous infusion of 2400 mg/m2 administered over 48 h, repeated every 2 weeks. For the XELOX regimen, nivolumab was administered at a fixed dose of 360 mg every 3 weeks, together with oxaliplatin 130 mg/m2 and oral capecitabine 1000 mg/m2 twice daily. Dose modifications or treatment adjustments were made according to clinical judgment and patient condition.
Outcomes
The data cutoff date for all analyses was March 12, 2025. Clinical outcomes were evaluated for objective response rate (ORR), disease control rate (DCR), PFS, and OS. Tumor response was evaluated as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD) according to the Response Evaluation Criteria in Solid Tumor (RECIST), version 1.1. The ORR was defined as the percentage (%) of patients with confirmed CR or PR, while DCR was defined as the percentage (%) of patients with confirmed CR, PR, or SD. PFS was measured from the start of the treatment to the date of disease progression or death from any cause, and OS was calculated from the start of the treatment to the date of death from any cause. The safety objectives were evaluated according to Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
Statistical analysis
Categorical and continuous variables were summarized using descriptive statistics. Survival analysis was performed using Kaplan–Meier curves, and results were compared using a log-rank test. All p values were two-sided, and confidence intervals (CIs) were at the 95% level, with statistical significance defined as p ⩽ 0.05. All statistical analyses were performed using IBM SPSS Statistics 27 (IVM Corp., Armonk, NY, USA) and R version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics
From April 2021 to September 2024, 336 AGC patients received nivolumab in combination with XELOX or FOLFOX as first-line therapy. Among 336 patients, 63 with PD-L1 expressions of low CPS 1–4 were included in this analysis (Figure 1).

Flow chart of patient selection.
Table 1 presents the baseline characteristics of the patients. The primary tumor was located in the stomach of 59 patients, while 3 patients had tumors involving the gastroesophageal junction, and 1 patient had esophageal adenocarcinoma. Eighteen patients (29%) were diagnosed histologically with poorly cohesive carcinoma or signet ring cell carcinoma, and three patients had other pathologies. Forty-six patients (73%) were diagnosed with stage IV cancer at the time of diagnosis. Median age was 61 years, with a range of 24–84 years, and 38 patients (60%) were male. High TMB was observed in six patients, one of whom had a MSI-high tumor. Metastases to the liver, peritoneum, bone, and lungs were observed in 23%, 65%, 15%, and 3% of patients, respectively; 12 of these were treated with FOLFOX and 51 with XELOX. Among 63 patients, 26 (42%) had a CPS of 1, 21 (34%) had a CPS of 2, 13 (21%) had a CPS of 3, and 2 (3%) had a CPS of 4.
Baseline demographics.
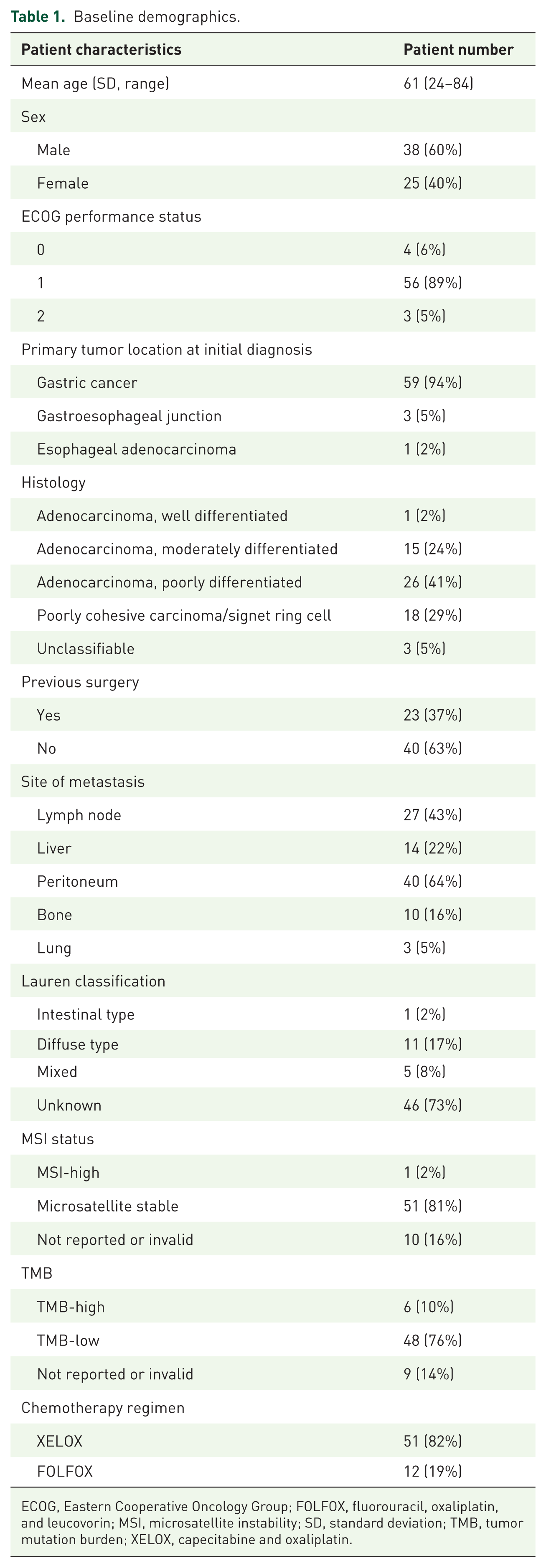
ECOG, Eastern Cooperative Oncology Group; FOLFOX, fluorouracil, oxaliplatin, and leucovorin; MSI, microsatellite instability; SD, standard deviation; TMB, tumor mutation burden; XELOX, capecitabine and oxaliplatin.
Treatment outcomes
Among 63 patients receiving nivolumab with chemotherapy, 1 achieved CR (2%) and 25 demonstrated PR (40%), an ORR of 42% (Table 2). SD was observed in 23 patients, a DCR of 76%. One patient was identified as having MSI-H with a CPS of 3 and received nivolumab plus XELOX for 21 months until disease progression. The median PFS of these treated patients was 5.8 months (95% CI, 4.9–6.7 months), and the median OS was 15.0 months (95% CI, 13.2–18.7 months; Figure 2). We evaluated PFS and OS after stratifying patients based on chemotherapy regimen, and Kaplan–Meier analysis showed no significant difference in PFS (p = 0.824) observed among the treatment groups (Figure 2). The median PFS was 5.6 months (95% CI, 4.7–6.5 months) for the XELOX group and 10.5 months for the FOLFOX group (95% CI, 4.2–16.8 months). The median OS was 13.3 months (95% CI, 8.8–17.8 months) for the XELOX group and 20.8 months (95% CI, 11.8–29.9 months) for the FOLFOX group. There was no significant difference between the two chemotherapy regimens (Supplemental Figure 1).
Response evaluation.


Kaplan–Meier curves of progression-free survival and overall survival.
Toxicity profile
Among the 63 patients included in the analysis, 58 (92%) experienced an adverse event, while 39 (61%) developed a grade 3 or 4 adverse event. The most frequently observed toxicities of any grade were decreased neutrophil count and platelet count, and an increase in aminotransferase (AST) or alanine aminotransferase (ALT) level, reported in 32 (51%), 23 (36%), and 37 (59%) patients, respectively. The most common grade 3 or 4 adverse events were anemia in nine patients (15%), neutropenia in three patients (5%), thrombocytopenia in three patients (5%), and elevated AST or ALT in three patients (5%). Additional commonly reported toxicities included sensory neuropathy and nausea (Table 3).
Side effect profile.

ALT, alanine aminotransferase; AST, aminotransferase; irAE, immune-related Adverse Event.
The most frequently observed treatment-related adverse event with a potential immune-mediated etiology was endocrinopathy, such as adrenal insufficiency or hypothyroidism. Grade 3 or 4 adverse events occurred in three patients: pneumonitis in two and toxic dermatitis in one.
Subsequent treatment after response failure to nivolumab plus chemotherapy
Ten patients continued nivolumab with chemotherapy without evidence of disease progression. Among the 52 patients who experienced disease progression, 14 did not receive subsequent systemic therapy due to poor ECOG performance status or other causes. The other 38 patients received subsequent second-line treatment, with paclitaxel plus ramucirumab administered in 30 patients. The remaining patients participated in clinical trials.
Discussion
This study showed the efficacy and safety profile of nivolumab combined with chemotherapy as routine clinical practice in patients with HER2-negative AGC harboring a low PD-L1 CPS of 1–4. The median PFS and OS were 5.8 and 15.0 months, respectively, and the ORR was 42%. Furthermore, most adverse events were easily managed. These findings suggest nivolumab plus chemotherapy as a useful first-line therapy in HER2-negative AGC patients harboring a low PD-L1 CPS.
Compared to pivotal clinical trials such as CHECKMATE-649 and ATTRACTION-4, which reported median PFS of 7.7 and 10.94 months, respectively, the PFS observed in our cohort was shorter.10,11 This discrepancy can be attributed to differences in patient populations, as our study included only patients with a CPS of 1–4, whereas the previous trials analyzed intention-to-treat populations that likely included patients with higher PD-L1 expression. There are limited data on outcomes in patients with low CPS from these pivotal trials; however, a post hoc analysis of the CHECKMATE-649 study reported no significant survival benefit from nivolumab plus chemotherapy in patients with CPS 1–4 (hazard ratio for PFS; 0.96, 95% CI, 0.74–1.24). 12 Furthermore, the higher proportion of patients with peritoneal seeding in our study compared to previous trials may also have contributed to the shorter PFS observed. Notably, the OS in our cohort was comparable to those of the referenced trials (13.7 and 17.45 months, respectively), which might be attributable to the homogeneous ethnic composition of our study population, consisting exclusively of East Asian patients. However, when benchmarked against retrospective real-world cohorts from other countries, the efficacy outcomes observed in our study were lower.13,14 Notably, previous pivotal trials have not specifically analyzed outcomes in patients with a CPS score of 1–4, a subgroup for which the clinical benefit of treatment remains uncertain. Therefore, our study adds value by focusing exclusively on this patient population.
For patients with CPS scores of 1–4, ASCO guidelines recommend immune checkpoint inhibitors in combination with fluoropyrimidine and platinum-based chemotherapy in a case-by-case manner, and the National Comprehensive Cancer Network guidelines endorse nivolumab plus chemotherapy with a category 2B recommendation.7,15 In prior trials, XELOX and FOLFOX regimens have demonstrated limited clinical efficacy, with a reported median PFS of less than 6 months.16,17 Our analysis indicates a possible trend toward improved efficacy with the addition of nivolumab in patients with low CPS, but definitive conclusions cannot be drawn.
The recent SPOTLIGHT trial has introduced claudin-18 isoform 2 (CLDN18.2)-targeted therapy as a novel treatment option for patients with HER2-negative gastric cancer. 18 Given the relatively small benefit of immunotherapy combination in patients with a CPS of 1–4, as observed in our cohort, CLDN18.2-targeted therapy is a promising alternative for those who are positive for CLDN18.2. Considering that the control arm of the SPOTLIGHT trial was chemotherapy alone rather than chemotherapy in combination with immunotherapy, it leaves questions regarding the best treatment options for patients with CPS 1–4 and positive CLDN18.2. As supplementary evidence for this patient subgroup, recent retrospective analyses have demonstrated that the efficacy of nivolumab in combination with chemotherapy is maintained irrespective of CLDN18.2 expression, suggesting potential utility in informing therapeutic decision-making.19,20 Furthermore, pivotal studies of CLDN18.2-targeted therapy demonstrated no significant differences in ORR compared with placebo, with separation of the survival curves occurring only at later time points. These observations indicate that zolbetuximab should not be regarded as the definitive preferred option in patients with low CPS and positive for CLDN 18.2, and additional evidence is required to establish an optimal treatment strategy. At present, treatment selection may reasonably be informed by subgroup analyses and guided by clinical factors such as tumor burden or a history of total gastrectomy. In patients with low CPS and negative CLDN18.2, further research is needed to identify predictive biomarkers of benefit from chemoimmunotherapy. Retrospective data have suggested that clinical features such as liver or peritoneal metastasis or genomic alterations such as SMARCA4 or BRCA2 mutations can increase responsiveness to chemoimmunotherapy regimens.21,22 These findings highlight the importance of continued biomarker-driven research in this heterogeneous patient population.
The safety profile of the regimen was generally tolerable. While most patients experienced a treatment-related adverse event of grade ⩾1, only a minority developed grade ⩾3 toxicities. Compared to pivotal trials, the incidence of diarrhea was lower, which might reflect underreporting inherent to a retrospective study design.3,4 By contrast, hematologic toxicities, including anemia and thrombocytopenia, were observed at relatively higher frequencies, possibly due to inclusion of patients with less favorable baseline organ function compared to those enrolled in clinical trials. Only a small number of patients experienced immune-related adverse events, such as pneumonitis and toxic dermatitis, which required permanent discontinuation of immune checkpoint inhibitors. Notably, patients with immune-related adverse events continued to show favorable outcomes, with OS exceeding a median of 15 months, which is that of the total cohort, despite discontinuation of immunotherapy.
Limitations of this study include its retrospective design, potential selection and documentation biases, and absence of a comparator arm. Adverse events were assessed via EMR and might not have been fully captured. In addition, as nivolumab is reimbursed only for patients with CPS ⩾5 in South Korea, the inclusion of patients with CPS 1–4 was limited to those able to afford the treatment out of pocket, which may have introduced selection bias. Despite these limitations, our findings provide valuable real-world evidence regarding the clinical efficacy and safety of chemoimmunotherapy in patients with low PD-L1 CPS AGC.
Conclusion
This real-world retrospective analysis suggests that nivolumab plus chemotherapy may provide modest efficacy with manageable safety in patients with HER2-negative AGC and low CPS (1–4). Given the growing role of CLDN18.2-targeted therapy, treatment decisions in this subgroup should be made cautiously on an individual basis, and prospective randomized studies are required to establish the optimal treatment strategy for this subgroup.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251396410 – Supplemental material for Nivolumab plus chemotherapy in metastatic gastric cancer with low combined positive score
Supplemental material, sj-docx-1-tag-10.1177_17562848251396410 for Nivolumab plus chemotherapy in metastatic gastric cancer with low combined positive score by Junkyu Kim, Changgon Kim, Ji Eun Shin, Sung Hee Lim, Jeeyun Lee and Seung Tae Kim in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-2-tag-10.1177_17562848251396410 – Supplemental material for Nivolumab plus chemotherapy in metastatic gastric cancer with low combined positive score
Supplemental material, sj-tif-2-tag-10.1177_17562848251396410 for Nivolumab plus chemotherapy in metastatic gastric cancer with low combined positive score by Junkyu Kim, Changgon Kim, Ji Eun Shin, Sung Hee Lim, Jeeyun Lee and Seung Tae Kim in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.