
Abstract
Background:
Inflammatory digestive diseases can majorly impact the physical and mental well-being of affected patients.
Objectives:
This meta-analysis aimed to assess the efficacy of psychological interventions (including psychotherapy, mindfulness, cognitive-behavioral therapy, relaxation techniques, meditation, stress management, self-help strategies, psychoeducation, motivational interviewing, hypnotherapy, solution-based therapy, and counseling) on mental parameters and disease-related outcomes in this population.
Design:
This was a systematic review and meta-analysis.
Data sources and methods:
The systematic search was conducted on July 31, 2025. Randomized controlled trials (RCTs) were eligible. Outcomes were assessed at the end of therapy and at various time points during the follow-up period (short-, mid-, and long-term follow-up). Owing to the differences in scales and questionnaires, the standardized mean difference (SMD) was used to pool effect sizes, along with corresponding 95% confidence interval (CI). Higgins and Thompson’s I2 statistics were used to assess heterogeneity.
Results:
We included 24 RCTs that investigated the effect of psychological interventions on depressive symptoms in inflammatory digestive diseases, totaling 1572 participants. The pooled analysis found that psychological interventions resulted in a moderate reduction of depression compared to controls (SMD −0.46; CI: −0.75; −0.18). Data from 19 RCTs with 1593 patients also demonstrated a moderate reduction in anxiety symptoms in subjects undergoing psychological interventions (SMD −0.58; CI: −0.94; −0.22). The pooled analysis of 13 RCTs with 772 participants found that psychological therapy was associated with a moderate decrease in stress (SMD −0.53; CI: −1.04; −0.03). The additional analysis of follow-up data showed that benefits resulting from treatment gradually decreased, showing no significant difference at the end of the long-term follow-up period.
Conclusion:
Psychological interventions effectively improve mental health-related outcomes in patients with inflammatory digestive diseases. Since benefits from therapy seem to decrease during the follow-up period, repeated interventions may be necessary.
Trial registration:
The study protocol was prospectively registered on PROSPERO (CRD42021282965).
Keywords
Introduction
Inflammatory diseases of the gastrointestinal tract—including inflammatory bowel diseases (IBD), chronic liver diseases, celiac disease, peptic ulcer disease, pancreatitis, gastroesophageal reflux disease, and cystic fibrosis—affect millions worldwide and impose a substantial burden on physical and mental health. Psychological distress in these populations can arise from the persistent nature of symptoms, dietary and lifestyle restrictions, and the impact of disease on work and social life. While IBD has been the primary focus of research into psychological comorbidities, 1 other inflammatory GI conditions remain understudied. It is important to note that psychological stress has the potential to adversely impact gastrointestinal function,2,3 thereby influencing other chronic inflammatory digestive system diseases as well.
Up to 20% of patients with gastrointestinal afflictions suffer from depression, whereas the prevalence of anxiety is even higher, with a staggering 25%. 4 The interaction between the digestive tract and psychological symptoms is bidirectional, which can be explained by the brain–gut axis. This relationship indicates that stress, anxiety, or depression can contribute to intestinal inflammation. Conversely, intestinal inflammation has the potential to adversely impact mood and mental well-being, establishing a reciprocal relation.4,5 Studies suggest that gastrointestinal and liver diseases may be influenced by the pathophysiological mechanisms of brain–gut and brain–liver communication.6,7
A previously published meta-analysis concludes that psychological comorbidities, such as anxiety, depression, and stress, are not only associated with active disease but are also seen during remission. Studies indicate that depression in IBD can increase the need for surgery and hospitalizations by potentially exacerbating disease flare-ups. 8 Recent evidence also indicates that psychological interventions can influence not only emotional well-being but also markers of inflammation in IBD. Treatments targeting mood have been found to reduce systemic inflammation and disease-specific biomarkers, such as fecal calprotectin and C-reactive protein. Moreover, interventions that achieve greater improvements are linked to more pronounced biomarker changes. 9 These findings highlight the potential for mental health therapies to serve as complementary treatments in IBD, with possible relevance to other inflammatory digestive diseases.
Despite these findings, no comprehensive meta-analysis has evaluated the efficacy of psychological interventions across a broader spectrum of inflammatory digestive system diseases. Given the shared inflammatory pathways and overlapping psychosocial challenges, pooling evidence across conditions could clarify whether psychological therapies yield consistent benefits beyond IBD. Therefore, we aimed to investigate the effect of psychological interventions in individuals with various inflammatory diseases of the digestive tract in the context of randomized controlled trials (RCTs).
Methods
We conducted our research and reported our findings based on the recommendations of the PRISMA 2020 guideline 10 and the Cochrane Handbook. 11 The study protocol was prospectively registered on PROSPERO (CRD42021282965), and there were no deviations.
Eligibility criteria
We included RCTs assessing the effect of psychological interventions in adult patients with various inflammatory digestive diseases. In this review, the term “inflammatory digestive diseases” is used to refer to nonmalignant inflammatory conditions affecting the gastrointestinal tract and associated organs. Psychological interventions were defined as structured therapeutic approaches that aim to improve emotional, cognitive, or behavioral functioning through psychological or psychosocial techniques (rather than pharmacological or surgical methods). Eligible interventions encompassed first-wave behavioral therapy, second-wave cognitive-behavioral approaches, and third-wave interventions (e.g., mindfulness-based stress reduction, Acceptance and Commitment Therapy). Expressive and integrative methods such as guided imagery, music therapy, and relaxation-based training were also considered eligible, as were supportive approaches such as psychoeducation, motivational interviewing, and counseling. These interventions were administered in group or individual settings, through face-to-face sessions, over the telephone, or via the Internet. The interventions could be carried out by physicians, psychologists, nurses, or social workers. The comparator comprised either standard care, no treatment, placebo, other psychological interventions, or other disease-specific treatments.
Studies conducted on animals, cancer patients, functional gastrointestinal diseases, subjects with severe mental illness (e.g., schizophrenia, bipolar disorder), and alternative medicine (e.g., traditional Chinese medicine, Ayurveda, homeopathy, herbal medicine, aromatherapy) were excluded.
Outcomes related to mental health included changes in the level of depression, anxiety, perceived stress, total and mental quality of life (QoL), self-efficacy, and fear, while disease-related outcomes referred to physical QoL, fatigue, pain, disease activity, relapse rates, length of hospital stay, and changes in inflammatory markers.
Information sources
The systematic search was performed on July 31, 2025, in three main databases: MedLine (via PubMed), CENTRAL, and Embase.
Search strategy
The search key included three primary domains: related to psychological interventions, digestive tract diseases, and the concept of randomization (as we only included RCTs). For a detailed description, refer to Table S2. No filters were applied, and there were no restrictions regarding language or publication date.
Selection process
Duplicates were removed using a reference management software (EndNote X9; Clarivate Analytics, Philadelphia, PA, USA). The title abstract and full-text selections were performed by five independent authors (B.F., B.S., L.S., A.S.B., and E.T.) based on prespecified criteria. Inter-rater agreement was assessed by calculating the Cohen’s kappa coefficient (κ). Disagreements were resolved by a third independent reviewer (B.T.).
Data collection process and data items
Pertinent data from eligible articles were collected independently by six authors (D.-E.F., B.F., B.S., L.S., A.S.B., and E.T.) into a standardized data table. A third reviewer (B.T.) resolved any disagreements.
The following data were extracted: first author, year of publication, study site, study period, type of disease, details on the intervention type, duration, and control, provider of the intervention, number of patients, demographics, data regarding the continuous (mean, standard deviation (SD), standard error, median, range, interquartile ranges) and dichotomous outcomes (presence of the events of interest in the intervention and control groups, total number of participants in each group). If multiple scales or questionnaires were used to measure the outcome, we made our selection based on each questionnaire’s sensitivity and specificity indicators. When measuring anxiety, trait anxiety was excluded from the pooled analysis. In the case of data reported as graphs, GetData Graph Digitizer was used to extract information. The results were collected both immediately post-intervention and during follow-ups, using intention-to-treat data. The analysis incorporated a time component, considering various time points from the articles. Due to variations in follow-up periods and the use of booster sessions in some studies, a multivariate statistical model was used to account for these effects.
Risk of bias and quality of evidence assessment
The risk of bias was assessed using the RoB 2 tool. 10 Two authors (D.-E.F. and B.F.) independently assessed each outcome, while a third author (B.T.) resolved the disagreements. To evaluate the quality of evidence, we used the Grading of Recommendations Assessment, Development, and Evaluation system. 12
Statistical synthesis
A random-effects model was used to pool effect sizes, as we assumed considerable between-study heterogeneity.
Subgroup analysis was carried out based on intervention type, which was categorized according to the incorporation of cognitive-behavioral techniques (CBT; as this method is recognized as one of the most efficacious evidence-based psychological therapies 13 ). Additional assessments were performed based on patient population (IBD vs others). Data analysis included results reported at the end of the treatment period (immediately post-intervention) and during follow-up at short-term (up to 4 weeks following the intervention), medium-term (up to 16 weeks), and long-term (more than 16 weeks) intervals.
Due to the differences in the scales and questionnaires used to assess the outcomes of interest, the standardized mean difference (SMD; represented by exact Hedge’s g 14 ) with a 95% confidence interval (CI) was used as an effect size measure. For its calculation, the sample size, the mean, and its corresponding SD were extracted or calculated from each study (for each study group separately). A value between 0.2 and 0.5 represented a small effect, values between 0.5 and 0.8 indicated a moderate effect, while values above 0.8 were considered large. The impact on symptomatic improvement was extracted as mean changes or calculated based on score values at baseline, at the end of treatment, and/or at various time points during follow-up.
The results were considered statistically significant if the pooled CI did not contain the null value. We summarized the findings related to the meta-analysis on forest plots. Where applicable (if there were enough and not excessively heterogeneous studies), we reported the prediction intervals (the expected range of effects of future studies). We reported the results as SMD value (95% CI lower limit–95% CI upper limit).
Additionally, between-study heterogeneity was described using Higgins and Thompson’s I2 statistics. 15 Publication bias was assessed by inspecting funnel plots and calculating Pustejovsky’s (modified Egger’s) test p-value. 15 Potential outlier publications were explored using different influence measures and plots following the recommendation of Harrer et al. 16
All statistical analyses were performed with R software 8 (v4.3.2) 17 using the meta 18 (v6.5.0) package for basic meta-analysis calculations and plots and the dmetar 19 (v0.1.0) package for additional influential analysis calculations. For multivariate models, package metafor 20 (v4.4.0) was used, while package clubSandwich 21 (v0.5.10) was applied to perform the cluster-robust inference correction method.
For additional details, see Supplemental Material, Statistical Analysis.
Results
The systematic search yielded 20,248 records, with 17,030 entries left after duplicate removal. One hundred eighty-two full texts were assessed for eligibility (κ = 0.85), out of which 47 proved to meet the criteria for inclusion in the meta-analysis (κ = 0.9; Figure 1).

PRISMA flowchart detailing the search and selection process.
Basic characteristics of included studies
Table 1 summarizes the main characteristics of the included studies. Different types of psychological interventions were assessed, with varying frequencies and durations of treatment across the eligible studies. These included individual and group therapy, weekly and biweekly sessions, and day-long to year-long interventions. The follow-up time varied between 1 month and 2 years.
Basic characteristics of the included studies.

IBD, inflammatory bowel disease; QoL, quality of life; SD, standard deviation; N/A, not available.
Mental health-related outcomes
Depression
The impact on depressive symptoms at the end of therapy was reported in 29 RCTs, totaling 2037 participants. The pooled change to baseline analysis showed that psychological interventions resulted in a statistically significant moderate reduction in depression in patients with inflammatory digestive diseases, compared to controls (SMD −0.53 (−0.77; −0.28); Figure 2).
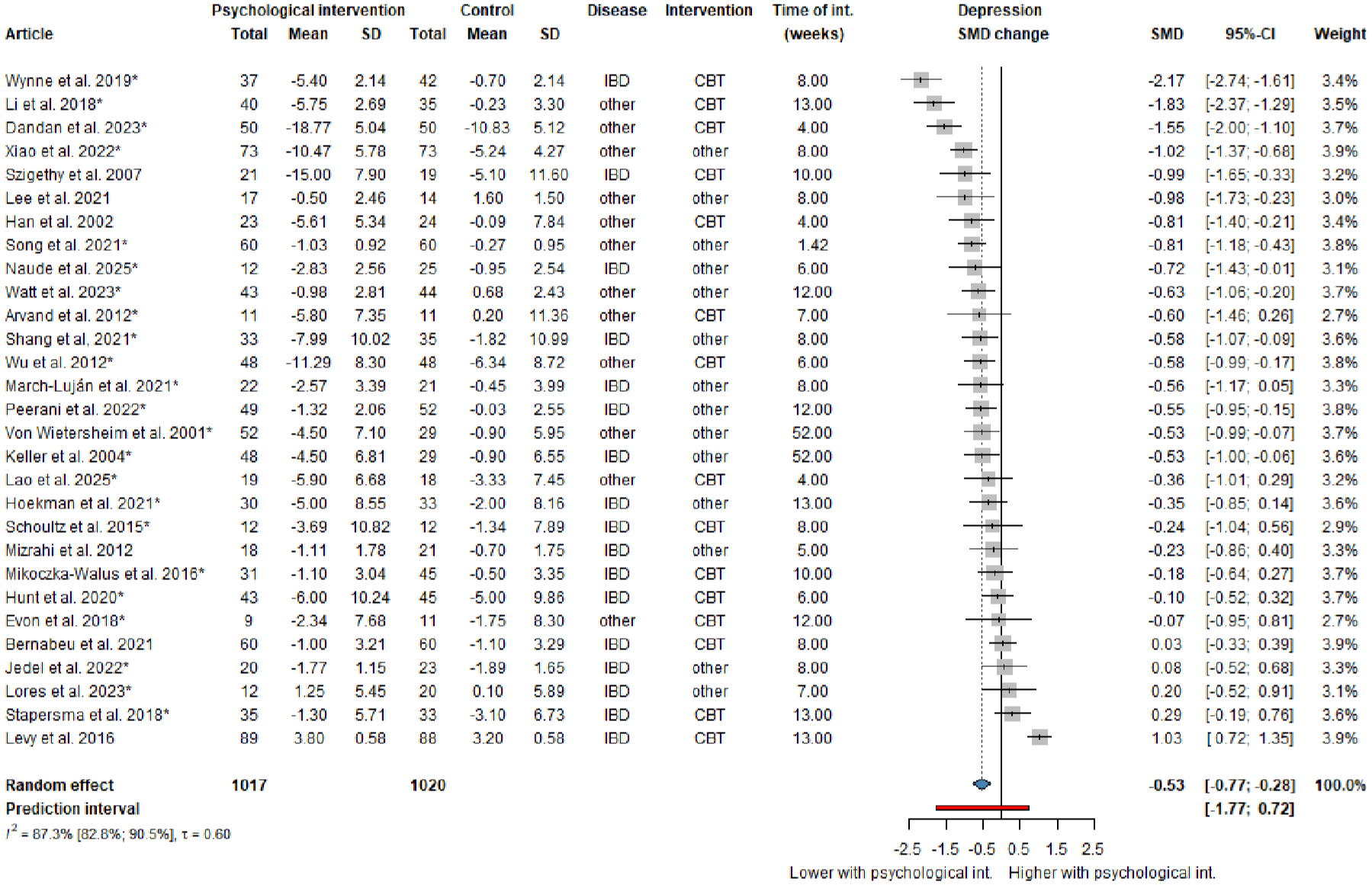
Forest plot demonstrating a moderate reduction in depressive symptoms at the end of the treatment period in patients receiving psychological interventions compared to standard care (for the studies marked with ‘*’ changes from baseline mean and SD values are estimated by imputing an assumed correlation coefficient).
Additional assessments were performed based on patient population (IBD vs others; refer to Figure S1). In the subgroup of participants with other inflammatory diseases (non-IBD patients), the effect was statistically significant, with a moderate reduction in depressive symptoms (SMD −0.53 (−0.77; −0.28)).
We also aimed to investigate how certain aspects of the intervention influenced clinical outcomes. Subgroup analysis based on intervention type, categorized according to the incorporation of CBT, found no significant difference between subgroups (refer to Figure S2).
The estimated heterogeneity was considerable (I2 = 87.3% (82.8; 90.5)). The leave-one-out (LOO) analysis revealed that the heterogeneity was not driven by an isolated outlier publication, as this statistical approach resulted in only a nonrelevant reduction in the I2 value (see Figure S23). The observed heterogeneity could arise from differences in the quality of the included studies, as well as from specific characteristics of the psychological interventions, including their delivery methods, the providers involved, and the context in which the sessions are conducted—although there was not enough information for performing meta-analytical calculations. The LOO did not reveal a relevant change in the effect size omitting any of the studies.
Anxiety
Twenty-four RCTs, including 1997 patients, reported data regarding the impact on anxiety at the end of the treatment period. Pooled change to baseline analysis demonstrated a statistically significant moderate effect on reducing anxiety symptoms in participants undergoing psychological interventions compared to standard treatment (SMD −0.63 (−0.98; −0.28); Figure 3).

Forest plot demonstrating a moderate effect on reducing anxiety at the end of the treatment period in patients receiving psychological interventions compared to standard care (for the studies marked with ‘*’ changes from baseline mean and SD values are estimated by imputing an assumed correlation coefficient).
Further analysis was conducted based on disease type among the subgroups (IBD vs others; refer to Figure S3). Statistically significant moderate reductions in anxiety were noted in both subgroups (SMD 0.38 (−0.65; −0.10) and SMD −0.63 (−0.98; −0.28), respectively).
The impact of intervention methodology was also investigated. Subgroup analysis was conducted based on the type of intervention (CBT vs others), yet no significant differences were found between the subgroups (refer to Figure S4).
Regarding heterogeneity, a similar trend was observed for this outcome as for depression. The estimated heterogeneity was considerable (I2 = 91.9% (89.2%; 93.9%)). The LOO analysis revealed that isolated outliers did not markedly impact the heterogeneity, with only a small reduction in the I2 value (see Figure S24). However, LOO showed an important change in effect size when the publication by Xiaomei and Qing 67 was omitted, resulting in an SMD of −0.54 (−0.83; −0.24).
Stress
Eighteen RCTs, which included 1002 patients with inflammatory digestive diseases, assessed the change in stress levels at the end of the treatment period. The pooled change to baseline analysis of the reported data showed that psychological interventions caused a statistically significant moderate reduction in stress compared to controls (SMD −0.46 (−0.83; −0.09); I2 = 81.1% (71; 87.6%); Figure 4).

Forest plot demonstrating the moderate reduction in stress levels at the end of the therapy in patients receiving psychological interventions compared to standard care (for the studies marked with ‘*’ changes from baseline mean and SD values are estimated by imputing an assumed correlation coefficient).
Similar to previous outcomes, additional analyses were carried out based on patient population and intervention type, with no significant subgroup differences. For the detailed results, refer to Figures S5 and S6. The results of the LOO analysis can be found in the Figure S25, showing an important change in effect size when the publication by Wynne et al. 66 was omitted, resulting in an SMD of −0.35 (−0.60; −0.09).
Total and mental QoL
Twenty-eight RCTs on 1614 participants investigated the improvement in total QoL scores at the end of therapy. Our pooled change to baseline analysis of the data did not find a significant amelioration in the QoL (SMD 0.23 (−0.01; 0.47); I2 = 84.1% (78; 88.5%); Figure 5).

Forest plot regarding the effect on total QoL scores at the end of the treatment period in patients receiving psychological interventions compared to standard care (for the studies marked with ‘*’ changes from baseline mean and SD values are estimated by imputing an assumed correlation coefficient).
Eight included studies assessed the effect on mental QoL at the end of the treatment period in 538 subjects. The pooled change to baseline analysis did not find a significant effect on improving this outcome (SMD 0.38 (−0.48; 1.21); I2 = 95.2% (92.5; 96.9); Figure 6).

Forest plot regarding the effect on mental QoL at the end of the treatment period in patients receiving psychological interventions compared to standard care (for the studies marked with ‘*’ changes from baseline mean and SD values are estimated by imputing an assumed correlation coefficient).
Other outcomes
We also investigated two other mental health-related outcomes, namely, self-efficacy and fear. Five studies with 168 participants reported the impact of psychological interventions on self-efficacy without significant results (SMD 0.98 (−0.51; 2.47); I2 = 82.8% (55.8; 93.3%)). Regarding fear, we found an SMD of −0.10 (−1.21; 1.02), which was statistically not significant based on three studies (I2 = 66% (0; 90%); refer to Figures S7 and S8).
Disease-related outcomes
It is well known that inflammatory digestive diseases can significantly impact the physical well-being of affected patients. Psychosocial factors may alter the behavior associated with the disease and influence treatment results. Therefore, we also investigated a series of disease-related outcomes.
Our pooled analysis of data reported by 9 studies totaling 467 participants did not find a significant or clinically relevant effect on improving the physical QoL immediately after the intervention (SMD 0.15 (−0.61; 0.31); I2 = 58.8% (13.9; 80.3%); refer to Figure S9).
The assessment of the impact on other subjective physical outcomes such as fatigue and pain yielded similar conclusions (SMD 0.13 (−0.50; 0.24); I2 = 70.5% (35.6; 86.5%) and SMD 0.25 (−0.48; 0.99); I2 = 94.9% (92.7; 96.5%), respectively; refer to Figures S10 and S11).
Regarding disease activity, we could not demonstrate a significant reduction in patients with inflammatory digestive diseases receiving psychological interventions compared to standard care (SMD −0.03 (−0.25; 0.18); I2 = 21.7% (0; 59.8%); refer to Figure S12).
Meta-regression analysis
Meta-regression analysis was performed to assess the linear relationship between the duration of the psychological intervention and the change in symptoms. No clinically significant correlations were observed (refer to Figures S13–S18).
Follow-up data
Benefits seen with psychological therapy seem to decrease during the follow-up period (Table 2). Therefore, repeated interventions may be necessary.
The effect of psychological interventions on the outcomes of interest immediately post-intervention and during short-, medium-, and long-term follow-ups (up to 4 weeks, up to 16 weeks, and more than 16 weeks of follow-up, respectively). Values in bold represent statistically significant values.

CI, confidence interval; QoL, quality of life; SMD, standardized mean difference.
Heterogeneity
The between-study heterogeneity in most of the analyses was substantial or considerable. This could be explained by differences in inclusion criteria, outcome measurements, or varying intervention protocols. We performed LOO influential analyses, but this method only marginally reduced heterogeneity (Figures S23–S25). This suggests that heterogeneity arises from broader study characteristics rather than isolated outliers. An additional subgroup analysis by intervention type and patient population found statistically significant effects in some outcomes but did not identify definitive sources of heterogeneity.
Risk of bias
There was a significant risk for bias in most of the included studies (Figure S19). Although the inability to blind may be considered intrinsic to the interventions being studied, the resulting bias remains important and was a major contributing factor to the high risk of bias classification in most of the included articles.
Publication bias
Publication bias was assessed for the outcomes of interest. All funnel plots were symmetrical, and Pustejovsky test p-values exceeded 0.1 in each instance. Thus, no evidence of publication bias was detected (Figures S20–S22).
Certainty of evidence
The certainty of evidence was estimated as very low quality for anxiety, stress, and depression (refer to Table S3). A high proportion of the included studies showed moderate-to-high risk of bias, largely due to challenges in blinding participants, deliverers of the interventions, and outcome assessors. Additionally, there was significant heterogeneity in the results, suggesting substantial variability in the effects of the interventions across studies. The treatment protocols varied widely in their methodologies, durations, comparison groups, and follow-up periods, contributing to inconsistency and further reducing confidence in the evidence.
Discussion
Psychological comorbidities such as anxiety, depression, and perceived stress have been frequently reported in patients suffering from IBD. 8 Previous meta-analyses investigated the effects of psychological interventions in IBD patients, focusing on parameters of psychological well-being, and found that psychological therapy, especially CBT, offers short-term improvements in terms of depression and QoL.1,69 The present study aimed to assess the effects of psychological interventions across a more diverse patient population, encompassing individuals with various inflammatory digestive disorders. Our results are consistent with previous reports, showing that psychological therapies effectively improve mental health-related outcomes such as depression, anxiety, and stress in these patients immediately after treatment.
We recognize that interpreting such pooled results can be challenging. To address the issue of variability, we performed a subgroup analysis comparing patients with IBD and those with other inflammatory digestive conditions, which revealed no significant difference in therapeutic response. Consequently, psychological interventions were found to be effective across a range of inflammatory conditions and should not be exclusively recommended to IBD patients.
The additional analysis of follow-up data showed that benefits resulting from therapy gradually decreased, showing no significant difference at the end of the long-term follow-up period. A similar trend was highlighted in previous works, which indicated that psychological interventions could offer short-term benefits for patients with IBD, although these effects seemed to diminish and eventually be lost with time.1,69 Possible explanations for this trend include patients facing new or ongoing stressors without continued therapeutic reinforcement, as well as a decrease in adherence to coping techniques over time. These results underscore the importance of conducting further studies to explore the effects of repeated interventions with extended follow-up periods, especially in chronic diseases.
Establishing the optimal protocol for psychological therapy poses a significant challenge. There is considerable heterogeneity in the literature concerning the timeframe, number, and duration of sessions, and types of interventions. Currently, CBT is considered to have the most robust evidence supporting its efficacy. 13 Therefore, we have performed a subgroup analysis based on the type of intervention used, comparing CBT-based therapy to other psychological interventions. Although CBT is commonly regarded as particularly effective, we found that the impact of treatment did not seem to differ significantly between these two subgroups. Third-wave therapies, including acceptance and commitment therapy, dialectical behavior therapy, and mindfulness-based approaches, represent a modern class of cognitive and behavioral treatments. 70 In patients with inactive IBD, a recent meta-analysis found that third-generation therapies seemed to be more effective compared to classical CBT in reducing depression and stress. This positive effect persisted throughout the follow-up, suggesting a potentially superior long-term treatment approach. 69 Acceptance, mindfulness, and value-focused approaches represent third-wave therapies in psychological interventions. These interventions are based on a shift from the first- (behavioral therapy) and second-wave therapies (CBT). 70
Our work also assessed the effect of psychological therapies on disease-related outcomes, such as fatigue, pain, physical QoL, and disease activity. Similar to the results of previous works, which focused mainly on patients with IBD, we found that despite an improvement in parameters pertaining to mental health, there was no significant improvement in physical well-being and QoL. 69 In contrast to these findings, one recent meta-analysis concluded that psychological interventions may exert anti-inflammatory effects, with reductions observed in biomarkers such as C-reactive protein and fecal calprotectin. 9 This biological link supports the plausibility that improvements in mental health could translate into measurable changes in disease activity. However, in our analysis, self-reported physical health outcomes did not show significant improvement. Several factors may explain this discrepancy; firstly, physical outcomes are often influenced by multiple biological and environmental determinants beyond psychological state. In addition, the improvements in inflammatory biomarkers may not have translated into perceptible symptom relief during the study follow-up periods.
An important limitation of reporting pooled (“average”) effects lies in the considerable degree of heterogeneity of the results, possibly driven by variability in patient populations, intervention types or durations, follow-up periods, and methodologies. While statistical methods partially addressed these issues, they did not fully resolve them, highlighting the need for standardized methodologies and targeted research to identify optimal intervention strategies tailored to specific populations. Subgroup analyses by intervention type and patient population found statistically significant effects but did not identify the source of heterogeneity. LOO sensitivity analyses showed that the study by Xiaomei and Qing 67 was an influential factor in assessing the effect on anxiety, with its omission resulting in a reduced overall effect. This tendency could be explained by the fact that the population in this study was comprised of patients with severe acute pancreatitis, markedly different from the rest of the included studies, which mainly discussed cases of patients with chronic diseases. The effect of psychological interventions could vary widely based on the type of underlying disease. Another possible source of variability may lie in the quality of the included studies, as the estimated risk of bias varied across included trials. Moreover, certain characteristics of the psychological interventions, such as delivery methods (in-person vs telehealth), providers (psychologists, social workers, nurses), or context (individual vs group therapy), may influence efficacy and consistency across included studies.
Strengths
This systematic review and meta-analysis provide a comprehensive overview and interpretation of results for the main inflammatory digestive diseases. By including various diseases and not focusing only on IBDs, our findings have implications for different gastroenterology areas. We included only RCTs and adhered to rigorous methodology, enhancing the validity of our results. Another strength lies in the substantial number of studies and patients included in the analysis.
Limitations
One limitation lies in the high risk of bias in many of the included studies. The limited number of studies within specific disease subgroups also restricted our analysis. Another limitation was the high heterogeneity among the included studies due to varying populations, scales, interventions, and follow-up periods.
Implications for practice
Translating scientific knowledge into community benefits is essential.71,72 Based on our findings, psychological interventions have a positive impact on mental health in patients with various inflammatory digestive diseases. Therefore, integrating psychological interventions into the standard care of patients with inflammatory gastrointestinal diseases is recommended to reduce depression, anxiety, and stress. Given the fact that symptomatic improvement derived from psychological therapies seems to decrease over time, repeated interventions can be useful in the management of such patients.
Implications for future research
To achieve high-quality results, it is important to standardize scales and measurements used in psychological studies. Future trials should focus on identifying the most effective intervention types, including their duration and methodology. These findings highlight the need for future research to investigate the impact of repeated interventions with long-term follow-ups.
Conclusion
This systematic review and meta-analysis provide a comprehensive overview of the role of psychological interventions in patients with various inflammatory digestive diseases. Based on the results reported by RCTs, we found that psychological interventions positively impact mental health-related outcomes, such as depression, anxiety, and stress. However, this improvement appears to be limited to the short term, indicating the potential need for repeated interventions.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251386324 – Supplemental material for Psychological interventions improve mental health in inflammatory digestive diseases: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-1-tag-10.1177_17562848251386324 for Psychological interventions improve mental health in inflammatory digestive diseases: a systematic review and meta-analysis of randomized controlled trials by Diana-Elena Floria, Beatrix Fogarasi, Edina Tari, László Szabó, Dániel Sándor Veres, Anna Sára Bognár, Beáta Sikó, Bálint Erőss, Brigitta Teutsch and Péter Hegyi in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.