
Abstract
Background:
Endoscopic submucosal dissection (ESD) enables en bloc resection of large colorectal lesions, but it remains challenging due to thin walls and poor operability. Traction devices like SureClip traction band (SCTB, Micro-tech) and SO clip (SO-C, Zeon Medical Inc.) are used to address this. This study compared the differences in ESD outcomes between SCTB and SO-C.
Objective:
Comparative analysis of the efficacy of SO-C and SCTB for various therapeutic results, including procedure time in colorectal ESD.
Design:
A single-center retrospective study reviewed 982 colorectal ESD procedures for lesions 20–49 mm performed at Kyoto Prefectural University of Medicine from January 2015 to November 2024.
Methods:
Patients were categorized into no-traction, SCTB, and SO-C groups. Propensity score matching was performed to minimize baseline differences. The primary outcome was ESD procedure time, and secondary outcomes assessed various therapeutic results.
Results:
After matching, there were no differences in procedure time (56.0 ± 31.2 vs 59.8 ± 30.6 min, p = 0.206), en bloc resection (97.7% vs 98.3%, p = 0.589), and perioperative perforation (0.3% vs 1.4%, p = 0.101) between the traction (SCTB + SO-C) and no-traction groups. Regarding the comparison between the SCTB and SO-C groups after matching, there were no significant differences regarding ESD procedure time (58.7 ± 37.4 vs 59.1 ± 31.9 min, p = 0.469), en bloc resection (97.4% vs 97.4%, p = 1.000), and perioperative perforation (0% vs 0.9%, p = 0.316). The SCTB deployment was significantly faster than the SO-C (6.3 ± 3.8 vs 9.3 ± 5.9 min, p = 0.004).
Conclusion:
There were no significant differences in ESD therapeutic results between SCTB and SO-C, while the SCTB had a faster deployment time.
Keywords
Introduction
Colorectal cancer ranks third in incidence and second in mortality worldwide. 1 Its high prevalence and mortality rates make it a significant public health concern. Advances in colonoscopy have led to an increase in endoscopic treatments for early colorectal lesions. Among these, endoscopic submucosal dissection (ESD) has emerged as an advanced endoscopic technique designed to achieve en bloc resection of early gastrointestinal lesions, offering the potential for curative treatment and accurate histopathological evaluation.2–6 Colorectal ESD is especially difficult due to thin walls, the presence of folds, flexures, and peristaltic movements.7,8 The inherent difficulty of the procedure and the steep learning curve may contribute to the low adoption of ESD in Western countries. To address those challenges, traction methods have been developed to make submucosa exposure and improve ESD therapeutic results, especially during long procedure times.9,10 There are various types of traction devices, such as the SO clip (SO-C, Zeon Medical Inc., Tokyo, Japan) and the SureClip traction band (SCTB, Micro-Tech Co., Nanjing, China). The SO-C employs a clip-and-spring mechanism to provide traction and the SCTB utilizes an elastic band mechanism to create continuous tension.11,12 While both methods have shown potential to improve ESD efficiency and safety, there remains limited evidence directly comparing their efficacy and practical applicability in clinical settings.7,8,13,14 This study aims to perform a comparative analysis of the efficacy of SO-C and SCTB for various therapeutic results, including procedure time in colorectal ESD.
Methods
This was a single-center retrospective comparative study. We reviewed 982 consecutive patients who underwent colorectal ESD, lesions between 20 and 49 mm, at the Kyoto Prefectural University of Medicine between January 2015 and November 2024 (Figure 1). Although we have been performing ESD since 2006, the proposed time frame was selected to minimize the effects of the steep learning curve in colorectal ESD and other devices which developed before 2014. The indications of ESD were for lesions of ⩾20 mm in size that were deemed difficult to manage with en bloc resection via endoscopic mucosal resection (EMR) according to Japanese guidelines. 15 Endoscopic diagnosis of the lesion was performed by narrow band imaging (NBI), blue laser/light imaging (BLI), and pit pattern observation in all cases. Lesions with 50 mm or larger were excluded, as they were all treated using the SO-C according to institutional protocol.

Study flow.
The patients were divided into three groups: no-traction, traction with the SO-C, and traction with the SCTB. In Analysis 1, we examined the differences in mean procedure time between the SO-C group and the SCTB group, and compared various ESD therapeutic results between the two groups. The impact of lesion size (<30 mm vs ⩾30 mm) was analyzed based on our previous study, 16 along with the influence of operator experience. In Analysis 2, we examined the differences in various ESD therapeutic results, including mean procedure time between the traction group (SO-C + SCTB) and the no-traction group. The impact of lesion size <30 mm or ≧30 mm and operator experience was also analyzed. Various ESD therapeutic outcomes, including en bloc resection, R0 resection, perioperative perforation, delayed bleeding, and delayed perforation. Data regarding age, sex, use of antithrombotics (antiplatelet and anticoagulant), lesion morphology, lesion size, operator experience, ESD completion rate, lesion location (colon vs rectum), use of pocket-creation method (PCM), type of knife, and presence of severe fibrosis were also collected as cofactors.17,18 The mean deployment time of the traction devices was also calculated with representative 180 cases (the 90 most recent cases for each traction device). Traction device deployment time was defined as the time between the end of mucosal incision until the second clip was deployed. In addition, the comparison of ESD procedure time between the SCTB and SO-C groups was performed between lesions <30 mm and ⩾30 mm and between experts and non-experts. In both Analyses 1 and 2, propensity score matching was performed to minimize background differences for age, sex, and lesion/patient characteristics factors with p < 0.05. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. This research was conducted with the approval of the Ethics Committee of Kyoto Prefectural University of Medicine and carried out in accordance with the Helsinki Declaration of the World Medical Association.
Pretreatment and equipment for ESD
The patients were given a low-residue diet the day before ESD and 10 mL of sodium picosulfate hydrate at 9 PM. On the morning of the ESD day, the patients were administered 1.0 L of high-density polyethylene glycol solution with ascorbic acid (MoviPrep; Ajinomoto Pharmaceutical Co., Tokyo, Japan) or 0.5 L of oral sulfate solution (SULPREP; Fuji Pharma Co., Ltd., Tokyo, Japan). In all colorectal ESD cases, EC-L600ZP (Fujifilm Medical Co., Tokyo, Japan), EC-L600ZP7 (Fujifilm, Tokyo, Japan), or EC-760ZP7 (Fujifilm Medical Co., Tokyo, Japan) with a water supply system and carbon dioxide insulation (GW-100: Fujifilm, Tokyo, Japan) were used. Two kinds of transparent hoods (Elastic Touch, F-25: Top Co., Tokyo, Japan, or short ST hood, DH-29CR: Fujifilm Medical Co., Tokyo, Japan) were used, according to the degree of fibrosis. A lens cleaner (Cleash: Fujifilm, Tokyo, Japan) was used to prevent fogging of the endoscopic lens. During ESD, sedation was done using midazolam or propofol, and analgesia was provided with pentazocine. A small amount of 0.2% indigo carmine (final concentration: 0.06% indigo carmine) was added to a solution of 0.2% or 0.4% sodium hyaluronate (MucoUp; Boston Scientific Japan Co., Tokyo, Japan) or 0.3% or 0.6% sodium alginate (Liftal K; Kaigen Pharma., Tokyo, Japan) for submucosa elevation. The injection was performed using a 25-G puncture needle for the endoscope (ImpactFlow; TOP Corporation, Tokyo, Japan). The high-frequency electronic devices used were a VIO300D and VIO3 (Erbe Elektromedizin Co., Tubingen, Germany). Regarding the setting of VIO3: for marking (Forced coagulation 6.0), mucosal incision (Endocut I, Effect 1, Duration 4, Interval 1), submucosal dissection (Forced coagulation 3.0 and Endocut I), and hemostasis (Major: Soft coagulation 3.0; Minor: Forced coagulation 3.0) in all patients. Regarding the use of traction devices, SO-C was regularly used for all cases since 2018, and then, SCTB was regularly used for cases since 2022. The ESD procedures using both traction devices were performed according to our previous report 16 (Figure 2). Marking with the ESD knife was performed, followed by mucosal incision. After a full circumferential incision, the traction device was deployed on the anal side of the lesion. Then a second clip was positioned on the opposite wall to pull the traction device up. Submucosal dissection was then done, and during dissection, PCM was applied when severe breathing movement and poor operability were seen. Finally, en bloc resection was achieved.

Two traction devices and their use in colorectal ESD. (a) SO clip, consists of a spring 7 mm long and 1.8 mm wide with an attached metal clip at one end and a nylon loop at the other. (b) Non-polypoid lesion, located in the rectum with 40 mm in diameter. (c) Deployment of SCTB on the oral side of the lesion after full circumferential incision. (d) Good traction after deployment of the second clip in the opposite wall. (e) Sureclip Traction Band, a 11-mm clip preload onto three interconnected elastic silicone bands (one 1.5-mm ring and two 3.3-mm rings). (f) Non-polypoid lesion in ascending colon with 40 mm in diameter. (g) Deployment of SO-C in oral side of lesion after full circumferential incision. (h) Good traction after the deployment of second clip in opposite wall. Font: Authors’ personal archive.
Definitions
Tumor location was classified as proximal colon (from the cecum to the transverse colon) and distal colon (from the descending colon to the rectum). The tumor morphology was classified as polypoid or non-polypoid according to the Paris classification. 19 Experts were defined as those who had performed more than 5000 colonoscopies and 200 colorectal ESDs according to our previous paper. 20 Severe fibrosis was assessed endoscopically and classified according to the criteria proposed by Matsumoto et al., visualized as a dense, white, muscular-like structure without a blue transparent layer. 17 A procedure was only considered as a non-expert, if it was done 100% by the less experienced endoscopist. In cases where the operator was changed to an expert mid-procedure, they were counted as expert ones. Perioperative perforation was defined as a full-thickness defect occurring during the procedure. Delayed perforation was defined as the detection of free air by abdominal computed tomography within 14 days after ESD, which was not related to perioperative perforation. 21 Delayed bleeding was defined as the development of bleeding that required endoscopic hemostasis or resulted in a hemoglobin level decrease of more than 2 g/dL. The procedure time was defined as the duration from the initial injection to the completion of resection during ESD. The deployment time was defined as the interval from when the traction device appeared on the monitor to when effective traction was successfully achieved.
Statistical analyses
Categorical variables were compared using the chi-squared test, whereas continuous variables were analyzed using the Mann–Whitney U test. The confidence interval (CI) was 95% and statistical significance was set at p < 0.05. An analysis of the demographics (age, sex, use of antithrombotics, use of anticoagulants, lesion morphology, lesion size, operator expertise, completion rate, location, method, type of knife, and presence of severe fibrosis) of the patients was performed to look for differences between the study groups. To address potential bias, propensity score matching was performed using a logistic regression model for age, sex, and variables with p-values < 0.5. SPSS software (version 22.0; IBM Japan, Ltd., Tokyo, Japan) was used for all statistical analyses.
Results
A total of 982 procedures with lesions between 20 and 49 mm were enrolled in this study (Table 1). A total of 472 (48.1%) were resected without the use of traction devices, while 362 (36.9%) used the SO-C, and 148 (14.0%) used the SCTB. The mean lesion size was 27.1 ± 6.9 mm, with most of them being classified as non-polypoid (81.1%) and located in the colon (80.0%). The overall procedure time averaged 55.7 ± 27.5 min, and the R0 resection was achieved in 900 lesions (91.6%).
Patients characteristics.

Distal, descending, sigmoid colons and rectum; ESD, endoscopic submucosal dissection; PCM, Pocket-creation method; Polypoid, Is, Ip or Isp by Paris classification; Proximal, cecum, ascending and transverse colons; SCTB, Sureclip Traction Band; SD, standard deviation; SO-C, S-O clip.
The comparison of two different traction devices (SCTB vs SO-C) was performed (Table 2). Propensity score matching was performed to minimize the effects of group differences for age, sex, method (non-PCM or PCM), and type of knife (needle type or scissor type. A total of 114 cases were selected after matching for each group. Regarding ESD therapeutic results, there was no significant difference in ESD procedure time (min) (58.7 ± 37.4 vs 59.1 ± 31.9, p = 0.469). In addition, there were no significant differences in en bloc resection, R0 resection, and complications between the two groups.
Comparison of the traction band group versus SO-C group.

Distal, descending, sigmoid colons and rectum;, ESD, endoscopic submucosal dissection, PCM, Pocket-creation method; Polypoid, Is, Ip or Isp by Paris classification; Proximal, cecum, ascending and transverse colons; SCTB, Sureclip Traction Band; SD, standard deviation; SO-C, S-O clip.
Regarding lesion size, there were no significant differences in ESD procedure time (min) between SCTB and SO-C (48.0 ± 21.9 vs 50.4 ± 23.4, p = 0.270 for lesions <30 mm, 70.9 ± 46.8 vs 74.4 ± 38.9, p=0.639 for lesions ≧30 mm) (Table 3). Regarding operator experiences, there was no significant difference in ESD procedure time for both experts and non-experts between SCTB and SO-C.
ESD procedure time for different sizes and experience between SCTB and SO-C, after matching.

ESD, endoscopic submucosal dissection; SCTB, Sureclip Traction Band; SD, standard deviation; SO-C, S-O clip.
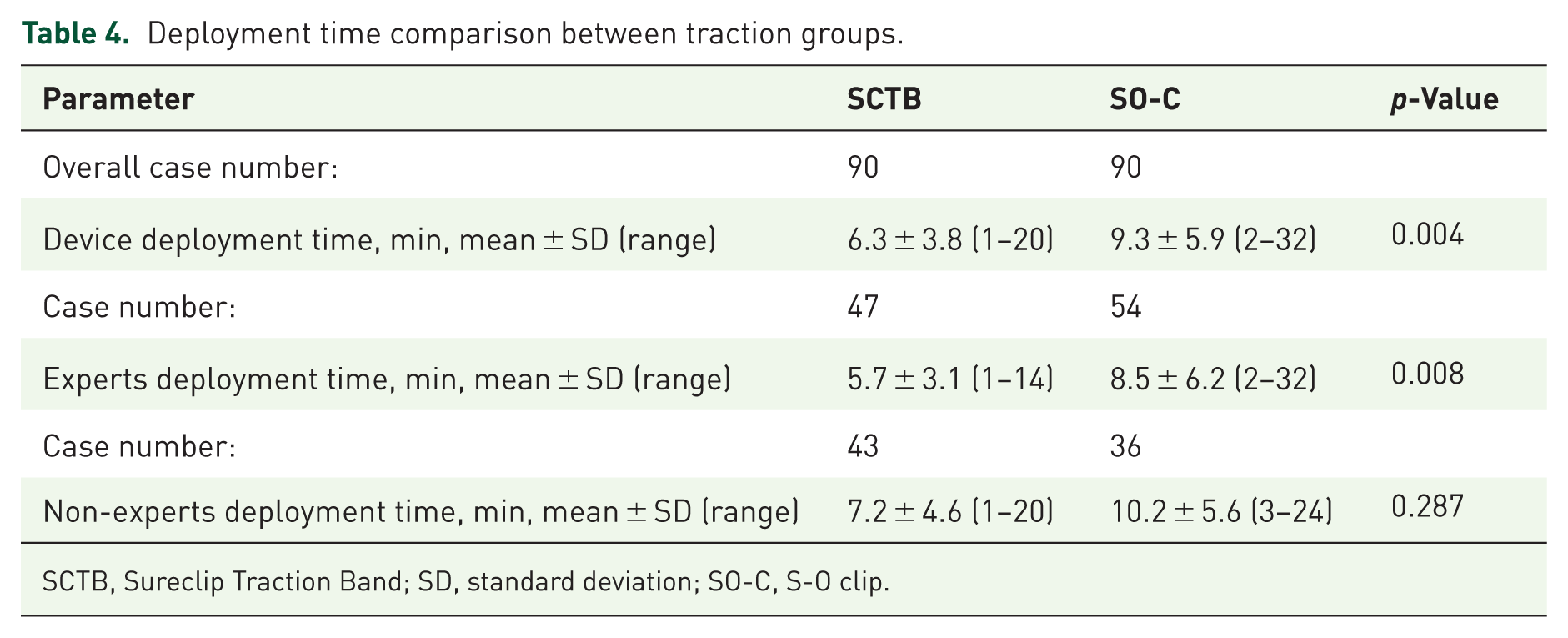
Regarding the device deployment, there was a significant difference in the time (min) between SCTB and SO-C groups (6.3 ± 3.8 vs 9.3 ± 5.9, p = 0.004) (Table 4). In only experts, the mean deployment time for SCTB was faster than that for SO-C (5.7 ± 3.1 vs 8.5 ± 6.2, p = 0.008). Regarding operator experience, the experts performed faster with the SCTB than the non-experts (7.2 ± 4.6 vs 5.7 ± 3.2, p = 0.009) (Table 5). On the other hand, there was no significant difference in the SO-C group (p = 0.869).
Deployment time comparison between traction groups.
SCTB, Sureclip Traction Band; SD, standard deviation; SO-C, S-O clip.
ESD procedure time for different sizes between and experience no traction and traction groups, after matching.

SCTB, Sureclip Traction Band; SD, standard deviation; SO-C, S-O clip.
Regarding the analysis of traction and non-traction groups, propensity score matching was performed, using age, sex, lesion morphology, operator experience, dissection method, and type of knife (Table 6). After matching, perioperative perforation was more common in the no traction group (0 vs 1.1% p = 0.044). Similarly, the other outcomes showed no differences between the two groups.
Comparison of the traction group versus no traction group.

Distal, descending, sigmoid colons and rectum; ESD, endoscopic submucosal dissection; PCM, Pocket-creation method; Polypoid, Is, Ip, or Isp by Paris classification; Proximal, cecum, ascending and transverse colons; SD, standard deviation.
We also evaluated the impact of the traction method according to lesion size and operator experience in matched cases (Table 7). The mean procedure time (min) in lesions of <30 mm was faster in the traction group, when compared with the traction group (46.6 ± 20.2 vs 52.6 ± 24.6, p = 0.005). However, this difference was not observed in lesions ⩾30 mm (66.9 ± 37.7 vs 70.9 ± 35.4, p = 0.613). The mean procedure time for non-experts was faster in the traction group when compared to the no traction group (55.8 ± 19.4 vs 62.1 ± 24.2, p = 0.026). Withing the experts, there was no diference in ESD procedure time between traction and no traction groups (56.2 ± 39.9 vs 57.6 ± 35.5, p = 0.930).
ESD procedure time for different sizes between and experience no traction and traction groups, after matching.

ESD, endoscopic submucosal dissection; SCTB, Sureclip Traction Band; SD, standard deviation; SO-C, S-O clip.
Discussion
When comparing the SCTB and the SO-C group using propensity score matching, there were no significant differences in ESD procedure time and other therapeutic results. However, the mean deployment time of the traction device was faster for SCTB than SO-C. This may be due to the easier handling of SCTB compared to the SO-C. In addition, this benefit was only achieved with experts. This suggested that the manipulation of SO-C was difficult for both experts and non-experts. Although the deployment time was faster with SCTB than SO-C, it did not affect the overall ESD procedure time. Thus, the choice of traction device can be made according to the operator’s preference. However, our study only included lesions of 20–49 mm. SCTB was not used for a lesion ≧50 mm clinically because SCTB did not keep enough traction for the lesion, as it did not have extended function like the spring of SO-C. Actually, a report showed several SCTB was used for ESD on a large colorectal lesion. 17 Further analysis should be expected for this.
About the impact of traction devices on procedure time, the CONNECT-C trial, a multicenter randomized control trial (RCT) comparing conventional ESD (no-traction) and traction ESD for lesions of ≧20 mm, showed no difference in overall procedure time. 8 The median procedure times (min) for conventional ESD and traction ESD were 61 (40–100) and 53 (40–76) (p = 0.18). There was a difference in the subgroup with lesions greater than 30 mm, with the median procedure time for no-traction being 89 (57−80) and 69 (50−104) (p = 0.05) for traction. It also showed a tendency for better dissection time in non-experts in the traction group (81 vs 64, p = 0.07). In the current study, there was no difference between the overall mean time in the no-traction and traction groups after propensity score matching (55.2 ± 27.9 vs 56.3 ± 31.6, p = 0.561), similar to the previous study. However, regarding lesion size, we found a faster dissection time in lesions <30 mm in the traction group, compared to the no-traction group (46.6 ± 20.2, vs 52.6 ± 24.6, p = 0.005). By contrast, there was no significant difference for lesions ⩾30 mm (66.9 ± 37.7, vs 70.9 ± 35.4, p = 0.613). Our study showed a different result compared to the previous one. 8 In the previous study, they only used SO-C for the traction group, and needle-type knives were mainly used (conventional group: 114/128, traction group: 116/123). These factors affected the results. On the other hand, regarding operator experience, we also showed a greater impact in procedure time with the use of traction in non-experts (55.8 ± 19.4 vs 62.1 ± 24.2, p = 0.026), and it was similar to the previous study. Our previous study about scissor knife comparing the use of SO-C to the non-use of it showed an improvement in dissection time for non-experts (42 vs 65 min, p = 0.036) but with no difference with experts (38 vs 36 min, p = 0.537). 22 This was consistent with our current result. Another multicenter RCT using only scissor-type knives in Japan for colorectal lesions of 20–50 mm showed that there was no significant difference between the traction and no-traction groups regarding resection speed (23.7 vs 25.6 mm2/min, p = 0.43). However, there was a significant difference in ESD procedure time (min) between the two groups (47.3 vs 62.3, p = 0.03). 23 In addition, for lesions of ⩾30 mm, the mean resection speed of the traction group tended to be faster than that of the traction group (34.6 ± 10.5 mm2/min vs 27.8 ± 11.9 mm2/min, p = 0.054). In the study, they used SO-C, hand-made clip and line, multiloop (Boston Scientific), and all operators were experienced. We suggested that the result of this study was different from ours due to operators’ experiences. Our previous study using scissor knives showed a better performance in the traction group when comparing the combination of the traction device with PCM than without PCM (57.8 ± 31.4 vs 81.7 ± 33.5 min, p < 0.01). 18 In the current study, we used PCM in 31.2% of traction groups after matching. The use of PCM and traction could make ESD procedure time short in the traction group compared to the no-traction group, though there was no significant difference. Various factors, including knife, operator experience, lesion size, PCM, and kinds of traction device, can affect the ESD procedure time. Future analysis should be performed to clarify the efficacy of the traction device.
In the current study, we analyzed the complication rates with or without the use of a traction device and showed no differences in delayed perforation (0.6% vs 0.9 p = 0.654) or delayed bleeding (0.3% vs 1.1%, p = 0.178). However, perioperative perforation (0 vs 1.1%, p = 0.44) was more common in the non-traction group. The previous two RCTs and our previous study showed there were no significant differences in complication rates between traction and no-traction.8,22,23 A study using an elastic-based traction similar to the SCTB, their overall complication rate was more common in the no-traction group (2.70% vs 20.59%, p = 0.020) and overall perforations (0% vs 11.76%, p = 0.048). 7 However, this study showed higher rates of complications in non-traction groups compared to our study. Complications are affected by various factors, including locations, size, antithrombotics, kinds of knives, operator experience, and severe fibrosis.15,22 The efficacy of traction devices for preventing complications should be examined in a further study. Regarding the perspectives for the clinical use of traction devices, considering their cost, it is important to select their use based on the difficulty of the lesion. In a recent multicenter study involving 178 cases, the rates of technical success in endoscopic resection, including ESD, were 78.8% for lesions with prior biopsy and 55.6% for recurrent lesions. These cases may be good indications for the use of traction devices. 24
Scissor-type knives were used in 78.9% of cases (Table 1), and knife type was included in the propensity score matching for comparisons (Tables 2 and 6). After matching, the proportion of scissor-type knife use was identical between groups, minimizing its influence on outcomes, although it may still have impacted the study with a lower complication rate. 25 Despite the high usage of scissor-type knives, traction still reduced procedure time in lesions <30 mm and in non-expert cases (Table 7), suggesting that its benefit remained relevant regardless of knife type.
This study had several limitations. It was a single-center retrospective study with a relatively small sample size, particularly when comparing the SCTB group to the SO-C group. In addition, hospital policy required the exclusion of lesions larger than 50 mm, which might have influenced the findings, as some benefits appear to be more pronounced for larger lesions. Despite matching case characteristics between SO-C and SCTB, temporal biases from 2018 to 2024—such as increased operator experience, advancements in endoscopic systems and electrosurgical units, and evolving ESD techniques like the pocket-creation method—may have influenced the comparative results. Traction devices may be useful for cases in challenging locations. However, we could not analyze it due to our retrospective setting. Other methods, such as clip and line, are also used as a kind of traction method in colorectal ESD. Rectal ESD is a good indication of this method. However, several papers showed the efficacy for decreasing the procedure time of colorectal ESD. 26 An RCT showed the self-completion rate of non-experts was higher in the clip and line method than conventional method. 27 In the current paper, we did not use the clip and line method. Although propensity score matching was applied to mitigate some biases, residual ones may still exist. Lastly, this study did not evaluate poor scope operability, a factor reported as a risk for ESD difficulties.
Conclusion
Our study found no significant differences in mean procedure time, en bloc resection, or R0 resection rates between the SCTB and SO-C groups, although the SCTB demonstrated faster and more consistent deployment for lesions between 20 and 49 mm. Traction devices were effective for decreasing ESD procedure time in non-experts.