
Abstract
Objectives:
Three-dimensional virtual reality (3D VR) permits precise reconstruction of computed tomography (CT) images, and these allow precise measurements of colonic anatomical parameters. Colonoscopy proves challenging in a subset of patients, and thus CT colonoscopy (CTC) is often required to visualize the entire colon. The aim of the study was to determine whether 3D reconstructions of the colon could help identify and quantify the key anatomical features leading to colonoscopy failure.
Design:
Retrospective observational study.
Methods:
Using 3D VR technology, we reconstructed and compared the length of various colonic segments and number of bends and colonic width in 10 cases of CTC in technically failed prior colonoscopies to 10 cases of CTC performed for non-technically failure indications.
Results:
We found significant elongation of the sigmoid colon (71 ± 23 cm versus 35 ± 9; p = 0.01) and of pancolonic length (216 ± 38 cm versus 158 ± 20 cm; p = 0.001) in cases of technically failed colonoscopy. There was also a significant increase in the number of colonic angles (17.7 ± 3.2 versus 12.7 ± 2.4; p = 0.008) in failed colonoscopy cases.
Conclusion:
Increased sigmoid and pancolonic length and more colonic bends are novel factors associated with technical failure of colonoscopy.
Keywords
Introduction
Colon cancers account for one-third of all cancer-related deaths in the United States.1–3 The high prevalence and mortality rates have prompted the development of screening tests to detect premalignant conditions. 4 These include colonoscopy and computed tomography colonography (CTC). CTC has a reported sensitivity of 89% and a specificity of 75% for tumors and adenomas exceeding than 6 mm.4,5 The indications for CTC include patients who refuse standard colonoscopy, a tendency to bleed and/or anticoagulation therapy, or failure in completing colonoscopy.6–9 Patient, technical, and operator factors may be related to an incomplete colonoscopy. Common patient factors include inadequate bowel preparation, discomfort, female sex, young age, and low body mass. Operator factors are related to the expertise of the endoscopist. Technical factors include ineffective sedation, colonic tortuosity, adhesions due to previous surgeries, angulation or fixation of bowel loops, long redundant colons, and diverticulosis.10–16 However, there are only scant actual evidence on the relationship between well-defined anatomical features and colonoscopy failure.
In the past two decades, three-dimensional (3D) imaging has gained popularity in medicine for anatomical evaluation and procedure planning. Virtual reality (VR) which explores computational technology has entered in the clinical toolbox in recent years. The dynamic nature of VR provides users with a more comprehensive understanding of the anatomical properties of the structure, by making it possible to measure cross-sectional areas and volumes, evaluate flexures, and explore the structure from within. In addition, since the colon interacts with different organs, VR allows the operator to understand the relationship between organs in the patient’s abdominal cavity. Lastly, VR reconstruction enables better understanding of inner-lumen structure. Using our VR technology, the operator can enter the colon from within, better visualizing the lumen, and can rehearse the colonoscopes’ path through the colon (Figure 1).

3D reconstruction of a normal colon.
Therefore, the aim of this study was to identify colon characteristics on CTC that were associated with incomplete colonoscopy.
Methods
Study population
This retrospective analysis was approved by the Sheba Medical Center internal review board. The sample was composed of 20 adult patients who underwent virtual colonoscopy for CRC screening at Sheba Medical Center from February 2018 to June 2020. Patients with inadequate bowel preparation were excluded from the study. The group of patients was divided into two groups of 10 patients each, 20 in total. To be eligible, patients were included if they underwent a CTC as a result of technical failure of their previous colonoscopy (within 6 months). Technical failure was defined as a colonoscopy without cecal intubation. 4 The control group included patients who had a CTC as a primary screening exam based on personal choice or contraindication for colonoscopy. The contraindications for colonoscopy were severe illness (American Society of Anesthesiology Classification ASA ⩾ 3B), bleeding disorders, and advanced age.
CT image acquisition and 3D modeling
CT scanning was performed with 16-channel or higher multidetector CT scanners using 120 kVp and 100 mAs, Brilliance iCT 256, Brilliance 64 (Ramat Gan, Israel). All CTCs were performed according to the colonoscopy protocol after bowel preparation with a standard laxative as previously reported.16,17 The scans were reviewed by an experienced, board-certified radiologist (OS) using Carestream Vue PACS in Sheba medical center, Israel. For purposes of the data analysis, this study used axial images taken in the supine position, exclusively.
VR-simulated colon models were created based on the CTC data collected for each patient. The images were uploaded as Digital Imaging and Communications in Medicine files into D2P® software (3D Systems Inc. Littleton CO, USA) for segmentation. The mesh files were converted into stereolithography (.STL) format files that depict 3D objects’ surface geometry. The operator was able to see the resulting segmentation in a stereoscopic view using the Vive System (HTC, San Francisco, CA, USA).
Colon VR analysis
Four measurements were taken to quantify the factors described in the literature as likely causes of colonoscopy failure: the colon segment length, the intersegmental angles, the number of loops in each segment, and the average girth of each segment. The objective of this study was to measure the bowel’s anatomical properties, to quantify their association with colonoscopy failure.
Colon segment length analysis
The colon was divided according to its anatomical distribution into ascending colon, transverse colon, descending colon sigmoid colon, and rectum. The ascending colon length was defined as the length between the edge of the cecum and the hepatic flexure. The transverse colon length was defined as the length between the hepatic and splenic flexure. The descending colon was defined as the length between the splenic flexure and the first angle turning medially from the retroperitoneum. The sigmoid colon length was defined as the length between the first angle turning medially from the retroperitoneum to the recto-sigmoid angle. The rectum length was defined as the length between the recto-sigmoid angle and the beginning of the anal verge. The purpose of this measurement was to identify a cutoff length above which the risk for colonoscopy failure was higher.
Intersegmental angles analysis
Three angles were measured between the segments of the colon – the recto-sigmoid angle, the angle between sigmoid colon and the descending colon, and the splenic flexure and the hepatic flexure. The purpose here was to identify the minimum number of acute intersegmental angles (<90°) associated with an increased risk for colonoscopy failure.
Number of loops in each segment
The number of bowel loops was counted in each segment as well as the total number of bowel loops in the whole colon. The purpose was to identify the minimum number of bowel loops in each bowel segment associated with an increased risk for colonoscopy failure.
Average girth of each segment
The average girth of every segment was calculated using the average of two different measurements from two different points along each segment. The purpose was to identify the average girth in each bowel segment. We excluded the rectum in our measurements due to its over-inflation secondary to the placement of the intrarectal insufflator which would have skewed our measurements.
Statistical analysis
Independent samples t-tests with a Welch correction were calculated. The p value was corrected for a false discovery rate. p Values less than 0.05 were considered significant.
A sample size of 20 patients (at 80% power level) was calculated given a 30% difference in total colon length and an alpha value of 0.5.
Backward linear regression model was performed for identification of factors associated with incomplete colonoscope.
The reporting of this study conforms to the STROBE statement. 18
Results
Patient characteristics
The study cohort consisted of 20 patients. The overall mean age was 65.4 ± 12.9 years, 16 were males (53%) and 14 were females (47%). The demographic data are listed in Table 1.
Breakdown of age and sex in different population groups.

p Value = 0.225.
IQR, interquartile range.
Measurements
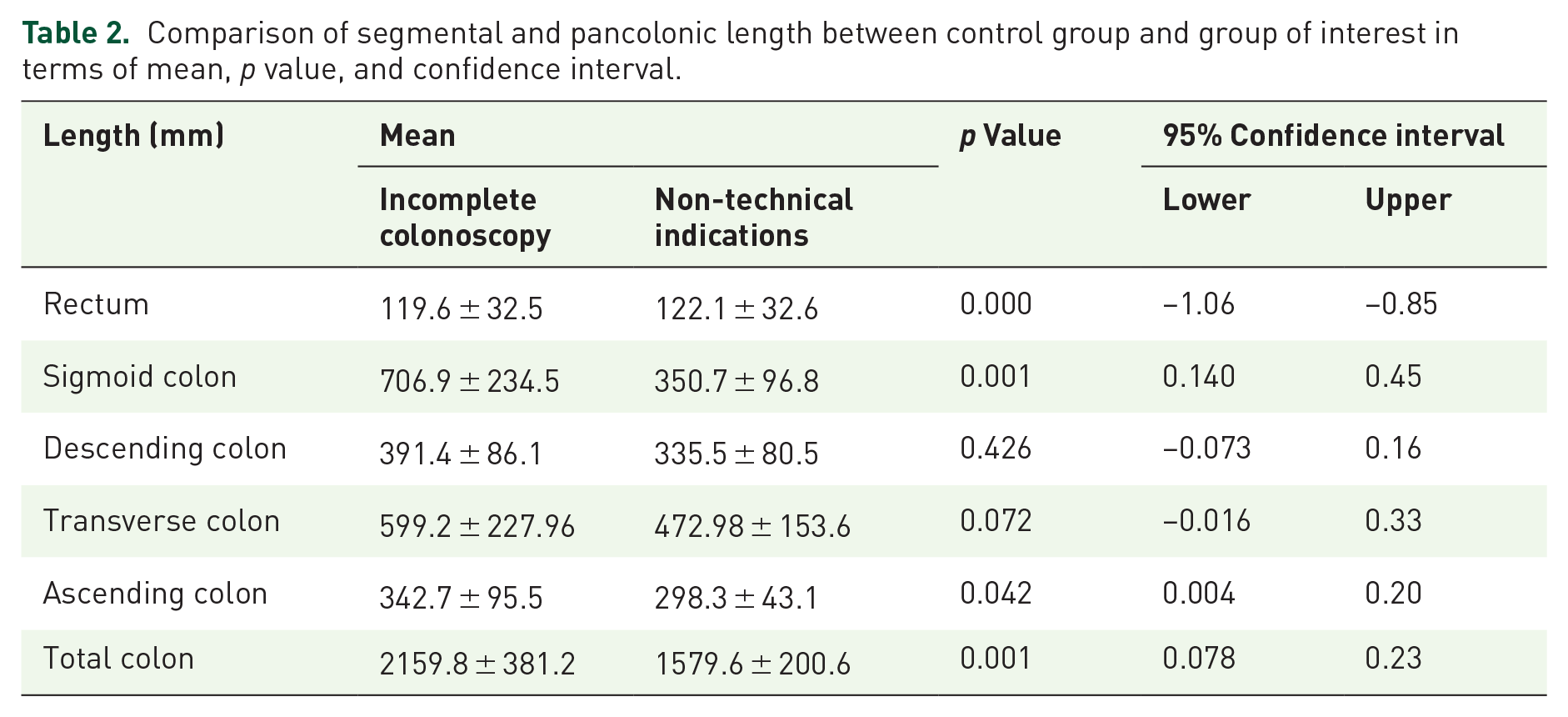
Patients of the incomplete colonoscopy group had an average sigmoid colon length of 706.9 ± 32.5 mm which was significantly longer than the 350.7 ± 96.8 mm in the non-technical indications group (p = 0.001). Other segments that were also significantly longer in the incomplete colonoscopy group included the descending colon length of 391.4 ± 86.1 mm versus 335.48 ± 80.52 mm and the pancolonic length of 2159.7 ± 381.2 mm versus 1579.6 ± 200.5 mm (Table 2).
Comparison of segmental and pancolonic length between control group and group of interest in terms of mean, p value, and confidence interval.
There was a significant increase in the number of overall loops in the colon in the incomplete colonoscopy group in comparison to the non-technical indications group; 17.7 ± 3.2 loops versus 12.7 ± 2.4 (Table 3). Patients in the incomplete colonoscopy group had an average of 6.8 ± 2.6 loops in their sigmoid colon versus 4 ± 1.2 in the non-technical indications group. These increases in bowel loops in both sigmoid and entire colon were significantly different between groups (Table 3).
Comparison of segmental and pancolonic bowel loops between control group and group of interest in terms of mean, p value, and confidence interval.

Eight acute intersegmental angles ⩽90° were found in the incomplete colonoscopy group compared to four in the non-technical indications group. Of the eight acute angles in the study group, three (37.5%) constituted the recto-sigmoid angle. In the non-technical indications group, of the four acute angles, two (50%) were the recto-sigmoid angle. These differences between groups were statistically significant (Table 4).
Comparison of segmental widths and sharp angles between the study and control groups.

Number represents absolute number of angles, not mean.
Number represents absolute number of angles, not mean.
By contrast, no statistical difference was found between the average girth of each bowel segment between the incomplete colonoscopy and control group (Table 4).
Using backward linear regression model, demographic data (age and sex) had no statistically significant impact on the difference between both study groups (p = 0.134 and p = 0.34, respectively).
3D reconstruction of colon with tortuous sigmoid colon is demonstrated in Figure 2.

3D reconstruction of colon with tortuous sigmoid colon.
Discussion
The primary goal of this study was to identify and quantify the possible features associated with colonoscopy failure. The significant differences reported here may contribute to future better training and assist in planning procedures as well as the choice of equipment. The findings of the study also point to the value of a 3D VR reconstruction of the colon in defining the exact anatomy of the colon in technically difficult cases.
Measurements of the length of each segment as well as the whole colon, the number of bowel loops in each segment and in the colon, the average width of colonic segments, and the number of acute angles exceeding 90° throughout the colon were significant between groups. The greater differences were found for the colonic length and the number of bowel loops. Several studies have reported an association between increased colonic length and tortuosity in incomplete colonoscopies.19–23 The results presented here are consistent with previous studies that found an association between failed colonoscopy and increased length of the sigmoid, transverse and total colorectal length, total colonic length, and a higher number of total colonic loops.22,23 These results innovate by providing a precise definition of the parameters that correlate with technical failure.
The major difference between this study and previous studies has to do with patient selection. In both previous studies, all patients underwent a colonoscopy as well as a CTC. In this study, the control group was comprised of patients who had a contraindication for a classic colonoscopy and therefore only underwent a CTC. The study group was composed of patients who had a failed colonoscopy and then underwent a CTC. In addition, this study measured the number of bowel loops in each segment as well as the total colon. The results revealed increased descending colon length and sigmoid colon tortuosity in the study group. There was also an increase in the number of acute angles in patients with a failed colonoscopy, which is a novel finding. Interestingly, unlike previously published studies, there was no statistical difference between groups with respect to increased transverse colon length and colonic diameter.
The main contribution of this study is related to the way the colon was reconstructed. Previous studies have used an automated tool built into their workstation together with an automatically generated central line. Here, by contrast, a 3D building tool consisted of a semi-automated and a manual tool. In our view, this technique is more accurate for reconstructing the colon as well as for measuring the different parameters used in this study. One of the major reasons relates to bowel preparation. Although good colonic preparation and sufficient colonoscopic mural visualization are prerequisites for virtual colonoscopy, even with good preparation most colons still contain residual amounts of feces. This is where the major difference comes in. The automated tool does not register the small fecal content as bowel and may miss it resulting in a reconstruction defect. The tool used here enables manual corrections so that we can account for these situations. In addition, some patients have an incompetent ileocecal valve which can cause insufflation of the small intestine. This can alter the colon reconstructed by the automated tool but again can be corrected with our setup. Finally, the ileocecal valve can be tricky for the human eye to identify and for tools used in previous studies. 17 In our study, board-certified radiologists identified the ileocecal valve, which thus led us to a more precise 3D model.
Our laboratory can convert the 3D model into a VR model. Hypothetically, we could take an abdominal CT of a patient scheduled to undergo a colonoscopy, reconstruct the patient’s colon as a 3D model, measure, and predict the chance of colonoscopy failure based on our findings. In technically challenging cases, the endoscopist can review the 3D model in VR to prepare for the colonoscopy.
Our study has limitations. First, selection bias can be caused by the retrospective design of the study. Second, as no colonoscopies were performed in the control group, the possibility of failure due to technical cause can occur.
Conclusion
Overall, the findings suggest that there is an association between colon anatomical features (long sigmoid colon and high number of colon loops) and incomplete colonoscopy. Our innovative 3D tool also converts our 3D model into VR. VR in its own right can contribute to training and give experienced endoscopist an idea of the colon before the colonoscope is inserted. Ideally, in the not so distant future, an augmented reality version can be developed where the endoscopist can perform the colonoscopy with the reconstructed colon overlaid on the patient.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231160625 – Supplemental material for Three-dimensional reconstruction of computed tomography colonography discloses anatomic features associated with colonoscopy failure
Supplemental material, sj-docx-1-tag-10.1177_17562848231160625 for Three-dimensional reconstruction of computed tomography colonography discloses anatomic features associated with colonoscopy failure by David Hochstein, Shai Tejman-Yarden, Olga Saukhat, Oliana Vazgovski, Yisrael Parmet, Netanel Nagar, Edward Ram and Dan Carter in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.