
Abstract
Background:
Several observational studies suggest a potential association between cholecystectomy and the risk of developing microscopic colitis (MC). However, the current findings remain inconsistent.
Objectives:
To address this discrepancy, we conducted a systematic review and meta-analysis to comprehensively assess the association between cholecystectomy and the risk of MC.
Design:
Systematic review and meta-analysis.
Data sources and methods:
A systematic search of PubMed, Embase, and Web of Science was conducted to identify studies evaluating the association between cholecystectomy and MC risk. Studies were eligible if they reported effect estimates or provided sufficient data for calculation. Two independent authors extracted the data and assessed the quality of included studies. A random-effects model was used to pool odds ratios (ORs), with subgroup analyses performed according to patient characteristics and study quality.
Results:
Six observational studies were included in the final analysis. The pooled OR was 0.80 (95% confidence interval: 0.52–1.22), and sensitivity analysis confirmed the robustness of the results, indicating no significant association between cholecystectomy and MC risk. Subgroup analyses based on geographic location, study design, study quality, methods of cholecystectomy data collection, control populations, and MC subtypes consistently showed no significant association.
Conclusion:
Current evidence suggests no statistically significant association between cholecystectomy and the risk of MC. Future research should include populations with diverse geographic and ethnic backgrounds, utilize medical records for accurate surgical history, and account for potential confounding factors. Large-scale prospective studies will be essential to obtain more reliable and definitive conclusions.
Trial PROSPERO registration:
CRD42024592056.
Plain language summary
Background:
Some studies suggest that removing the gallbladder (cholecystectomy) may increase the risk of developing microscopic colitis (MC), a type of chronic diarrhea-causing inflammation in the colon. However, these studies have shown mixed results, and it remains unclear whether there is a true link between gallbladder removal and microscopic colitis.
Objective:
We aimed to clarify this uncertainty by conducting a systematic review and meta-analysis, which is a scientific method that combines data from multiple studies to provide a more reliable conclusion.
Methods:
We searched major medical databases (PubMed, Embase, and Web of Science) to find studies that examined the connection between gallbladder removal and microscopic colitis. We only included studies that provided numerical data to measure the strength of this relationship. Two independent researchers carefully reviewed the studies, extracted data, and assessed their quality. We then used statistical methods to combine the results from different studies.
Results:
Our analysis included six observational studies. The combined data showed that gallbladder removal was not significantly associated with an increased risk of microscopic colitis. Additional tests confirmed that the results were stable and reliable. When we analyzed different factors such as study location, research methods, and types of patients, the findings remained consistent.
Conclusion:
Currently, there is no strong evidence that gallbladder removal increases the risk of microscopic colitis. However, future studies should include more diverse populations, use medical records to improve the accuracy of surgical history, and consider other factors that could influence the results. Large, high-quality studies are needed to confirm these findings and provide clearer conclusions.
Registration:
This study is registered with PROSPERO (CRD42024592056).
Background
Cholecystectomy is the standard treatment for gallbladder diseases. With the increasing incidence of these diseases and the introduction of laparoscopic techniques, the number of cholecystectomies has sharply risen. Although this procedure is common and relatively simple, its long-term health effects are controversial. Research suggests that cholecystectomy may influence the development of gastrointestinal diseases by altering bile acid metabolism, 1 causing gut dysbiosis, 2 modulating immune responses, 3 and impairing intestinal barrier function. 4 These changes may contribute to conditions such as irritable bowel syndrome (IBS), 5 Crohn’s disease, 6 and colorectal cancer. 7
Microscopic colitis (MC) is an inflammatory bowel disease characterized by chronic diarrhea; however, its pathogenesis is not fully understood. MC includes two major subtypes: collagenous colitis (CC) and lymphocytic colitis (LC), which share similar clinical symptoms but differ in histopathological features. 8 Recently, the potential association between cholecystectomy and MC has attracted increasing interest. Some studies have suggested that cholecystectomy may increase the risk of MC,9,10 but the findings remain inconsistent. 11
To date, no systematic review or meta-analysis has thoroughly assessed the relationship between cholecystectomy and MC risk. Consequently, a systematic review and meta-analysis are necessary to determine whether cholecystectomy increases the risk of MC and to quantify this association. This study evaluates the relationship between cholecystectomy and the risk of MC, providing evidence to guide clinical practice.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 12 The completed PRISMA 2020 checklist is available in the Supplementary Material . The study protocol was registered prospectively with PROSPERO (CRD42024592056).
Search strategy
Two independent researchers systematically searched the PubMed, Embase, and Web of Science databases for studies published up to July 2024. Predefined search terms related to MC and cholecystectomy were used. For example, the PubMed search strategy was as follows: ((((Correlation[Title/Abstract]) OR (risk[Title/Abstract])) OR (relation[Title/Abstract]))) OR (((gallbladder OR cholecyst OR biliary bladder OR vesica biliaris OR cystic duct organ OR biliary sac OR gall sac OR cholecystectomy OR gallbladderectomy OR gallbladder surgery OR gallbladder removal OR biliary surgery OR biliary tract surgery) OR cholecystectomy [MeSH] OR gallbladder [MeSH]))) AND (((microscopic colitides OR microscopic colitis OR collagenous colitis OR lymphocytic colitis) OR (microscopic colitis[MeSH])))). The search was limited to human studies but imposed no restrictions on language or geographic location. In addition, reference lists from the included studies were manually searched to identify any further eligible studies.
Study selection
Studies were included if they evaluated the association between cholecystectomy and the risk of MC and reported effect estimates such as odds ratios (ORs), relative risks, or hazard ratios, with corresponding 95% confidence intervals (CIs). Studies without effect estimates but with sufficient data for calculation were also considered. If multiple studies originated from the same database or cohort, only the most recent and comprehensive analysis was included. Exclusions were letters to the editor, case reports, case series, review articles, and studies lacking sufficient data for outcome assessment. No sample size restrictions were applied. Two researchers independently assessed each study for eligibility, resolving discrepancies by discussion.
Data extraction
Data were independently extracted by two researchers using the Critical Appraisal and Data Extraction for Systematic Reviews of Prediction Modelling Studies checklist. 13 Extracted information included the first author, publication year, study design, geographic location, population source, sample size, participant age and sex, MC diagnostic method, and quantitative estimates (including the incidence of MC associated with cholecystectomy or OR and 95% CI). Covariates used in multivariable analyses were also recorded. When necessary, original study authors were contacted for missing data.
Quality assessment
Two researchers independently assessed the risk of bias for each included study using the Newcastle–Ottawa Scale (NOS). 14 This scale evaluates studies based on three domains: selection of participants, comparability of study groups, and ascertainment of exposure or outcome. Studies were awarded up to 4 points for selection, 3 points for comparability, and 2 points for exposure/outcome, with a maximum total score of 9 points. Studies were classified as high quality (7–9 points), moderate quality (4–6 points), or low quality (0–3 points).
Statistical analysis
Effect estimates (OR and 95% CI) were extracted or calculated for each included study. When multiple adjusted effect estimates were available, the most comprehensively adjusted estimate was chosen. The DerSimonian and Laird random-effects model was used to pool data, accounting for expected heterogeneity. For meta-analyses, we calculated overall ORs from all eligible studies using this model. Subgroup analyses were based on factors such as study location, study design, study quality, adjusted OR, MC subtype, control group characteristics, and method of collecting cholecystectomy history. Heterogeneity was assessed using the I2 statistic and categorized as low (<25%), moderate (25%–55%), or high (>75%). Sensitivity analyses were performed by omitting individual studies to check the robustness of the findings. Meta-analyses were conducted using RevMan 5.3 (The Cochrane Collaboration, London, UK), while sensitivity analyses were performed using R software. If the analysis included >10 studies, publication bias was visually assessed with funnel plots and statistically with Egger’s test. 15
Results
Literature search and study characteristics
In total, 827 articles were identified from the PubMed, Embase, and Web of Science databases. After full-text screening, 34 studies were excluded for the following reasons: incomplete data (n = 31), irrelevant outcomes (n = 2),16,17 and the absence of a control group (n = 1). 18 Ultimately, six studies were included in the meta-analysis, comprising two cohort studies9,10 and four case–control studies.11,19–21 The literature search and study selection process are illustrated in Figure 1. The analysis included 786 MC patients and 1338 controls, including 745 healthy controls and 593 patients with functional diarrhea. Two studies were conducted in the United States,19,20 and four were conducted in Europe.9 –11,21 Three studies11,19,21 also explored the relationship between cholecystectomy and MC subtype. Data on cholecystectomy were collected via medical records, healthcare databases, or self-reported questionnaires. Only one study 20 adjusted for confounding factors such as age and sex, whereas the others did not, potentially introducing bias. The characteristics of the included studies are shown in Table 1. According to the NOS, half of the studies were rated as high quality9,11,21 (Table 2). Three studies9,10,20 may have introduced selection bias, as their control groups consisted of patients with functional diarrhea rather than healthy controls, although organic gastrointestinal diseases were excluded.
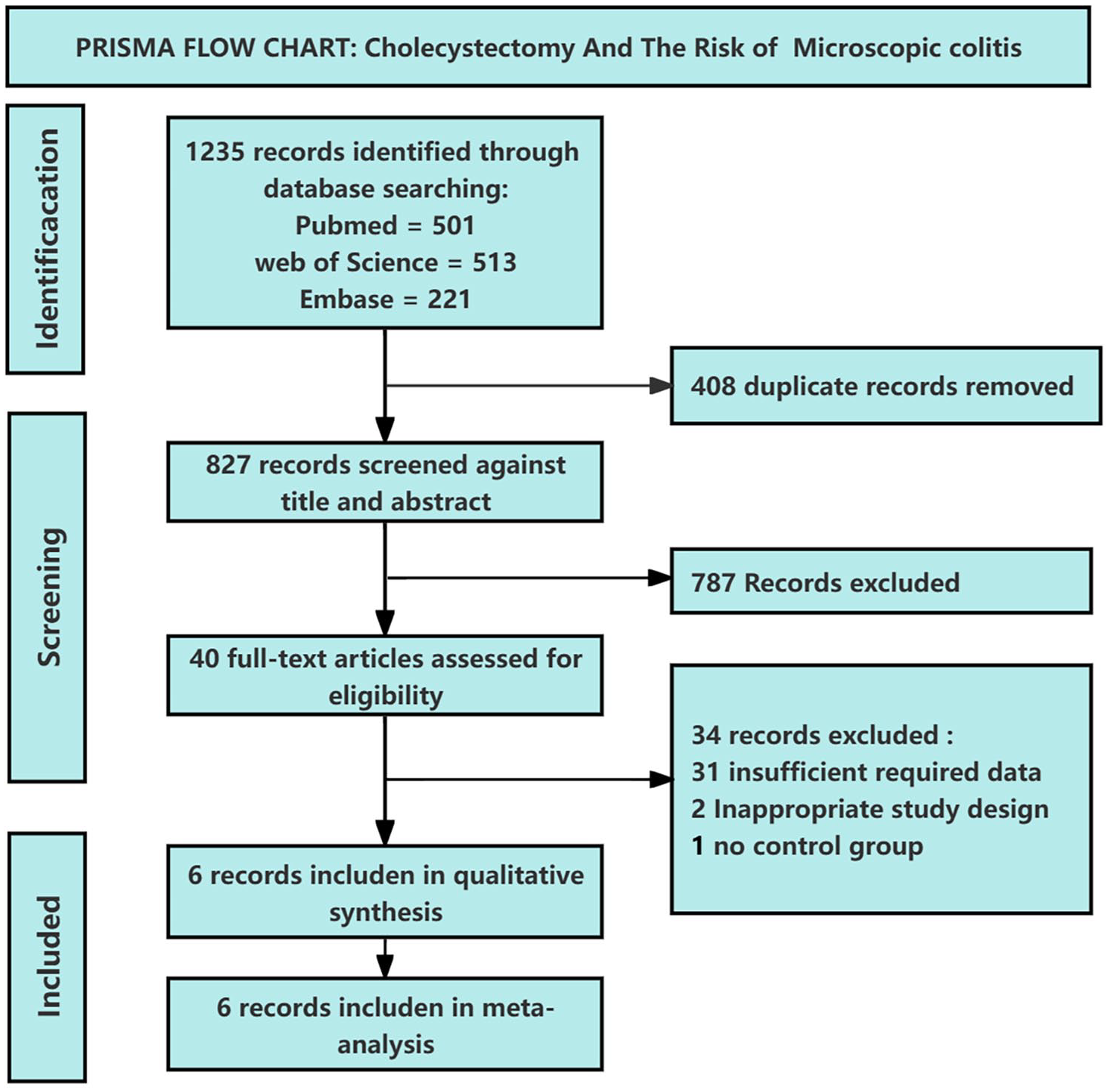
PRISMA flow chart: cholecystectomy and risk of microscopic colitis.
Study characteristics.

CC, collagenous colitis; CI, confidence interval; CNBD, chronic non‑bloody diarrhea; LC, lymphocytic colitis; MC, microscopic colitis; NR, not reported.
NOS of included studies.

NOS, Newcastle–Ottawa Scale.
Risk of MC after cholecystectomy
Of the six included studies, two9,10 reported that cholecystectomy increased the risk of MC, while three19–21 suggested it decreased the risk, and one study found no association between cholecystectomy and MC risk. 11 Risk estimates ranged from an OR of 0.33 (95% CI: 0.17–0.64) to an OR of 1.37 (95% CI: 0.57–3.29). 9 The pooled OR from the six studies was 0.80 (95% CI: 0.52–1.22), suggesting no statistically significant association between cholecystectomy and MC risk. However, the wide CI indicates considerable uncertainty regarding potential benefit or harm. This highlights limitations arising from the small number of studies and insufficient statistical power, warranting cautious interpretation of the conclusion (Figure 2).

Meta-analysis of cholecystectomy and microscopic colitis risk.
Subgroup, sensitivity, heterogeneity, and publication bias analysis
Subgroup analyses based on study design showed that the pooled OR was 1.35 (95% CI: 0.64–2.87) for the two cohort studies9,10 and 0.69 (95% CI: 0.41–1.15) for the four case–control studies.11,19 –21 High-quality, low-bias studies yielded a pooled OR of 1.03 (95% CI: 0.73–1.45),9,11,21 whereas moderate-quality studies produced a pooled OR of 0.55 (95% CI: 0.27–1.12).10,19,20 Geographically, no significant association between cholecystectomy and MC risk was found in the United States (pooled OR = 0.46, 95% CI: 0.23–0.93)19,20 or Europe (pooled OR = 1.04, 95% CI: 0.75–1.45).9 –11,21 Three studies11,19,21 examined the relationship between cholecystectomy and MC subtype, with pooled estimates showing no significant association for either CC (pooled OR = 0.88, 95% CI: 0.54–1.42) or LC (pooled OR = 0.94, 95% CI: 0.49–1.28). Subgroup analyses based on control group type or method of collecting cholecystectomy data also showed no significant association with MC risk.
Notably, subgroup analysis adjusting for confounding factors (age, sex, education) yielded a pooled OR of 0.33 (95% CI: 0.17–0.64), suggesting a potential inverse association between cholecystectomy and MC risk. However, this finding came from only one study, 20 which limits its generalizability and makes it particularly sensitive to potential residual confounding and methodological biases. The remaining studies, which did not adjust for these crucial confounders, produced a pooled OR of 0.97 (95% CI: 0.72–1.32), indicating no significant association. The considerable difference between the adjusted and unadjusted pooled effects underscores the uncertainty resulting from inadequate control of confounders in the existing literature, rather than confirming a protective effect conclusively. Detailed subgroup analysis data are presented in Table 3. Sensitivity analyses showed OR estimates ranging from 0.73 (95% CI: 0.45–1.16) to 0.97 (95% CI: 0.72–1.32), indicating that the results were robust and not driven by any single study. Moderate heterogeneity was detected among studies (p = 0.07, I2 = 50%; Figure 3). A pre-specified leave-one-out sensitivity analysis showed that temporarily omitting the study by Sandler et al. 20 reduced I2 to 12%, indicating that this study was the principal contributor to between-study variability—likely because it uniquely adjusted for major confounders (age, sex, education). Nonetheless, the study was retained in all primary analyses. Given the limited number of studies included, publication bias was not assessed.
Subgroup analysis.

CC, collagenous colitis; CI, confidence interval; LC, lymphocytic colitis; MC, microscopic colitis; OR, odds ratios.

Sensitivity analyses.
Discussion
This systematic review and meta-analysis is the first to comprehensively evaluate the association between cholecystectomy and the risk of MC. Our findings indicate no significant association between cholecystectomy and an increased risk of MC. Nonetheless, the wide CIs around the pooled estimate suggest substantial uncertainty regarding potential harm or benefit. Given the limited sample size and statistical power of the included studies, definitive conclusions cannot yet be drawn.
From a mechanistic standpoint, several factors may account for the apparent absence of an association between cholecystectomy and MC risk. Although cholecystectomy alters bile-acid composition and the gut microbiota, the relevance of these changes to MC pathogenesis remains unsettled. Bile acids play a dual role: they help preserve epithelial integrity and modulate immune defense, yet they can also promote diarrhea and destabilize microbial homeostasis. The literature is likewise divided: some studies report that post-cholecystectomy increases in secondary bile acids exert anti-inflammatory effects by limiting inflammatory-cell recruitment, 3 whereas others suggest that greater colonic bile-acid exposure may aggravate mucosal injury. 22 In addition, current evidence indicates that MC is driven chiefly by epithelial-barrier failure 23 and immune dysregulation, 24 modulated by both genetic predisposition and environmental triggers, rather than by bile-acid perturbations alone. Future work should more thoroughly dissect these complex, intersecting pathways to resolve these conflicting results.
Pronounced heterogeneity was detected across the six eligible studies (I2 = 50%). To diagnose its source, we performed a pre-specified leave-one-out analysis. Temporarily omitting the study by Sandler et al.—the only study rigorously adjusting for key confounders (age, sex, and education)—reduced I2 to 12%, resulting in only a modest shift in the pooled OR from 0.80 to 0.85. This indicates that Sandler et al.’s methodologically distinctive confounder control, rather than a fundamentally different risk estimate, is the principal driver of between-study variability. Because the adjusted subgroup result (adjusted OR = 0.33) stems entirely from this single study, the apparent protective effect should be interpreted with caution: it is highly sensitive to the design and residual bias of that one dataset and therefore cannot be viewed as definitive evidence. The scarcity of fully adjusted studies also limits the certainty of our meta-analytic conclusions, underscoring the need for future investigations that incorporate comprehensive confounder adjustment. Importantly, Sandler et al.’s confounder control was retained in all primary analyses; its temporary exclusion served only to identify heterogeneity, not to justify removal, and the overall null association remained broadly unchanged.
It is also worth noting that three of the included studies had control groups consisting of functional diarrhea patients. Because these patients’ gut environments and bile acid metabolism may differ from the general population, this could have impacted the results. First, patients with functional diarrhea may differ from healthy controls in baseline risk factors, potentially increasing study heterogeneity. Subgroup analysis revealed that heterogeneity was markedly higher in the functional diarrhea group compared to the healthy control group. In addition, the pooled effect estimate from the overall meta-analysis was OR = 0.80 (95% CI: 0.52–1.22), while the OR for functional diarrhea patients was 0.77 (95% CI: 0.26–2.24) and for healthy controls was 0.91 (95% CI: 0.65–1.28). Although the effect estimate for functional diarrhea patients was marginally lower, the wider CI suggests greater uncertainty, potentially due to differences in patient characteristics. This may also contribute to the overall uncertainty of the pooled estimates. Despite this variation, the combined OR from different control groups consistently showed no significant association between cholecystectomy and MC risk.
This study had several notable strengths. As the first systematic review and meta-analysis evaluating the relationship between cholecystectomy and MC risk, it addresses an important gap in the literature and holds substantial clinical relevance. The comprehensive literature search, combined with strict inclusion and exclusion criteria, ensured both a broad range of included studies and high data accuracy. In-depth subgroup analyses were conducted to investigate potential sources of heterogeneity, and sensitivity analyses confirmed the robustness of the results. These strengths enhance the methodological rigor of the study, providing scientifically valid and reliable findings.
However, several limitations should be acknowledged. First, a majority of the included studies were of moderate quality, highlighting possible selection and reporting biases that could influence our pooled estimates. Second, by combining cohort and case–control designs, we may have introduced additional selection bias, because the procedures used to recruit cases and controls in the case–control studies were not uniform and may therefore affect internal validity. Third, three studies depended on self-reported cholecystectomy histories, increasing their susceptibility to recall bias and misclassification; future work should preferentially verify surgical history through objective sources such as medical records or administrative healthcare databases to improve data accuracy. In addition, MC has many recognized risk factors, yet most of the primary studies did not adjust adequately for important confounders such as age, sex, smoking, or medication use, potentially attenuating the precision of the pooled effect. The geographical and ethnic restriction of the evidence base—predominantly Europe and the United States—may also limit generalizability, because lifestyle, dietary patterns, and healthcare systems differ worldwide. Finally, the relatively small sample size across studies reduces statistical power, hindering the detection of small but clinically relevant effects and lowering the reliability of subgroup analyses, thereby increasing the overall uncertainty of our conclusions.
Conclusion
Current evidence suggests no statistically significant association between cholecystectomy and the risk of MC. However, the conclusion is constrained by the limited number of studies and low statistical power, warranting cautious interpretation. Future studies should include populations with diverse geographic and ethnic backgrounds, verify surgical history using medical records, comprehensively adjust for confounders, and employ large-scale prospective designs to yield more robust conclusions.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251357067 – Supplemental material for Cholecystectomy and the risk of microscopic colitis: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848251357067 for Cholecystectomy and the risk of microscopic colitis: a systematic review and meta-analysis by Zhaoxu Tian, Hongying Tang, Guoming Sun, Jianjun Shen, Yangri Duan and Hangbin Jin in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.