
Abstract
Background:
Endoscopic retrograde cholangiopancreatography (ERCP) may not provide adequate drainage for patients with malignant hilar biliary obstruction (MHBO). Endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) is a salvage method for malignant distal biliary obstruction (MDBO); however, its effectiveness for MHBO remains unclear.
Objectives:
We aimed to evaluate the short- and long-term outcomes of EUS-HGS for MHBO.
Design:
This was a single-center retrospective cohort study.
Methods:
Unresectable patients who underwent initial EUS-HGS because of ERCP failure were recruited. Distal biliary stenosis or Bismuth types I and II–IV were defined as MDBO and MHBO, respectively. We defined EUS-HGS for MDBO as the control and analyzed the outcomes for MHBO.
Results:
The MDBO group (n = 208) was treated using EUS-HGS alone. In the MHBO group (n = 63), EUS-HGS alone (unilateral drainage, n = 26), EUS-HGS with bridging (EUS-HGSB, bilateral drainage, n = 21), and ERCP + EUS-HGS (bilateral drainage, n = 16) were performed. In EUS-HGS (MDBO), EUS-HGS (MHBO), EUS-HGSB, and ERCP + EUS-HGS, the technical success rates were 98.6%, 96.3%, 95.5%, and 94.1%; clinical success rates were 88.5%, 76.9%, 85.7%, and 75.0%; adverse event rates were 19.7%, 15.4%, 9.5%, and 25.0%; and non-recurrent biliary obstruction (RBO) rates at 180 days were 45.5%, 19.8%, 61.9%, and 68.4%, respectively. In multivariate analysis of the MHBO group, EUS-HGSB tended to have a lower risk of RBO (adjusted hazard ratio (aHR), 0.39; p = 0.09), and ERCP + EUS-HGS showed a significantly lower risk (aHR, 0.25; p = 0.03) compared to EUS-HGS alone (unilateral drainage).
Conclusion:
ERCP + EUS-HGS followed by EUS-HGSB, providing bilateral drainage, can offer preferred palliation for MHBO. These drainages may serve as potential salvage options in the management of MHBO.
Keywords
Introduction
Endoscopic biliary drainage performed using endoscopic retrograde cholangiopancreatography (ERCP) is the standard biliary drainage procedure for malignant biliary obstruction (MBO). However, technical failure can result from factors such as reconstructed anatomy and duodenal stenosis.1,2 In addition, ERCP with multisegmental drainage for malignant hilar biliary obstruction (MHBO) is technically challenging because of difficulties in selectively cannulating tight and complicated strictures. 3 In MHBO with Bismuth types II–IV, drainage of >50% of the liver volume contributes to overall survival (OS). 4 Therefore, further interventions for effective biliary drainage in MHBO are warranted.
In cases of inadequate drainage using ERCP alone, percutaneous transhepatic biliary drainage (PTBD) is conventionally performed. However, PTBD is a non-physiological drainage technique with potential problems, including decreased quality of life due to external fistula management and the risk of catheter-related problems, such as self-extraction.5,6 Accordingly, endoscopic ultrasound-guided biliary drainage (EUS-BD) has been recently described as a salvage drainage technique for malignant distal biliary obstruction (MDBO).7–10 Particularly, EUS-guided hepaticogastrostomy (EUS-HGS) is among the most common approaches in EUS-BD and has been established as an effective and safe drainage method.11–13
Given that EUS-HGS involves drainage from the left hepatic lobe, combination drainage using ERCP and EUS-HGS,6,14 as well as EUS-HGS with bridging (EUS-HGSB), which involves bridging the left and right lobes under EUS-HGS, has been developed recently as a novel salvage drainage method and has allowed bilateral internal drainage for MHBO.15–20 However, their efficacies and safety profiles remain unclear. Although recent reviews have described their short-term outcomes, such as technical and clinical success,9,19,21 the long-term outcomes, including time to recurrent biliary obstruction (TRBO), have not yet been reported. Therefore, this study aimed to comprehensively evaluate the clinical outcomes of EUS-HGS for MHBO with those of EUS-HGS for MDBO, which has been established as a salvage method until now.
Methods
Ethics statements
This study was approved by the institutional review board (approval number: 2018-149), and all patients provided written informed consent. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 22
Study patients
Consecutive patients who attempted to undergo initial EUS-HGS for unresectable MBO between March 2018 and October 2024 at a single center (National Cancer Center Hospital) were retrospectively evaluated. We collected baseline data, procedure data, short- and long-term outcomes, and survival data. We included patients who attempted to undergo initial EUS-HGS (including hepatojejunostomy) for unresectable MBO because of malignant gastroduodenal stenosis, surgically altered anatomy, ERCP failure (including incomplete ERCP), or other reasons. We excluded patients who underwent EUS-HGS with antegrade stenting, forward-viewing EUS-BD, and combined EUS-guided hepaticoduodenostomy (EUS-HDS).
Procedure details
Endoscopic ultrasound-guided hepaticogastrostomy
A linear echoendoscope (GF-UCT260 and GF-UCT240; Olympus, Tokyo, Japan; EG-580UT; FUJIFILM Medical, Tokyo, Japan) was used for EUS-guided imaging under moderate sedation. B2 or B3 was punctured using a 19-gauge (G) fine-needle aspiration (FNA) needle (EZ Shot 3 plus (Olympus Medical, Tokyo, Japan)). The intrahepatic bile duct (IHBD) was confirmed using fluoroscopy, followed by placement of a 0.025-inch guidewire in the IHBD. In some cases, the puncture was performed using a 22-G FNA needle and a 0.018-inch guidewire. Subsequently, the fistula was dilated using a Bougie (ES Dilator; ZEON Medical, Tokyo, Japan), balloon (REN; KANEKA, Osaka, Japan), drill (Tornus ES; Asahi Intec, Aichi, Japan), and/or electric cautery dilator (Fine 025; Medico’s Hirata, Osaka, Japan). Fully covered self-expandable metal stents (SEMSs; diameter: 8 mm) or plastic stents (PS, 7Fr) were then deployed from the left IHBD to the stomach (the stent was selected based on the time of sale and the judgment of each physician). 23 The drainage method was determined according to our institutional strategy (Supplemental Figure 1), while also considering clinical factors, such as performance status and life expectancy. The final decision was made based on the judgment of each physician. Prophylactic antibiotics were regularly administered before all procedures and until the following day.
Endoscopic retrograde cholangiopancreatography + endoscopic ultrasound-guided hepaticogastrostomy
Combination drainage with ERCP and EUS-HGS was performed as a salvage method in patients who did not achieve adequate drainage (unilateral drainage) with ERCP alone. Under ERCP, the uncovered SEMS (UCSEMS, diameter: 8 mm) was deployed into the right IHBD. Subsequently, EUS-HGS was performed for the left IHBD with inadequate drainage to achieve bilateral drainage, either during the same session or within 1 week after the ERCP procedure.
EUS-HGSB (EUS-HGS with bridging)
A 0.025-inch guidewire was placed into the left-to-right IHBD after puncturing B2 or B3. Next, an 8-mm-diameter UCSEMS (laser-cut type) was deployed to bridge the right and the left IHBD. 24 In cases of Bismuth type IIIa or IV, in which stenting was also required in both anterior and posterior branches, we deployed UCSEMSs in each branch using the partial stent-in-stent technique. Finally, we performed EUS-HGS as aforementioned. All EUS-HGSB procedures were performed to achieve bilateral drainage, either during the same session or within 1 week after the ERCP procedure.
Re-intervention
Endoscopic re-intervention (ERI) strategies were determined based on the initial stent type and drainage method. In EUS-HGSB and ERCP + EUS-HGS, when a UCSEMS had been placed across the hilar stricture, one or more PSs were deployed into its lumen using the stent-in-stent technique. In the ERCP portion of ERCP + EUS-HGS, a fully covered SEMS was removed and replaced if used. For an endosonographically/EUS-guided created route, if the initial stent was PS, it was replaced; if a covered SEMS had been used, it was removed and exchanged when feasible, or if not, PS was deployed inside the existing SEMS lumen.
Definitions
Distal biliary stricture and Bismuth type I were classified into the MDBO group (reference group), and Bismuth types II–IV were classified into the MHBO group, according to the Bismuth–Corlette classification. 25 Procedure time was defined as the total duration for cases involving two sessions.
For EUS-HGS, the technical success rate was defined as the rate of successful stent deployment in the appropriate position. For combination drainage (ERCP + EUS-HGS), the technical success rate was defined as the rate of successful deployment in both ERCP (deployment into the right IHBD) and EUS-HGS (as aforementioned) at the end of all procedures. For EUS-HGSB, the technical success rate was defined as the rate of successful deployment in both EUS-HGS (as aforementioned) and bridge stenting (one stenting or more for right-to-left IHBD) at the end of all procedures.
Clinical success rate was defined as the rate of achieved reduction in serum total bilirubin levels by 50% or <2 mg/dL within 2 weeks after all procedures. TRBO was defined as the time between stent deployment (the latter procedural day if two sessions) and the occurrence of cholangitis and jaundice, stent revision, or other biliary interventions due to recurrent biliary obstruction (RBO).11,26 Procedure-related adverse events (AEs) were defined as events other than RBO. If the procedure was performed in two sessions, procedure-related AEs were comprehensively accounted for in both sessions. Among AEs, cholangitis was defined as transient cholangitis after the procedure, non-obstructive cholangitis, or cholangitis caused by direct obstruction of the left bile duct due to EUS-HGS stent deployment other than RBO. Peritonitis was diagnosed based on the presence of clinical symptoms of peritoneal inflammation and corresponding fluid collection on computed tomography. Bleeding was defined as a reduction in serum hemoglobin levels by >2.0 g/dL from the pretreatment value. AEs were divided into early (occurring within 14 days of the endoscopic procedure) and late (occurring >14 days after the procedure) AEs. AEs were graded according to the American Society for Gastrointestinal Endoscopy lexicon. 27
Statistical analyses
Continuous and categorical variables are expressed as medians (interquartile ranges) and numbers (percentages), respectively. Qualitative and quantitative between-group differences were evaluated using the χ2 or Fisher exact test for categorical parameters and the Mann–Whitney U test and Kruskal–Wallis test for continuous variables. The median cumulative TRBO with the 95% confidence interval (CI) was calculated using the Kaplan–Meier analysis, with between-group comparisons using the log-rank test. Univariate and multivariate Cox hazard regression analyses were performed to calculate hazard ratios (HRs) and 95% CIs for comparative RBO risk. Variables for the multivariate Cox model were preselected based on prior evidence and clinical relevance to avoid overfitting. Patients who were lost to follow-up or who died before RBO were censored. In addition, binary logistic regression was used to calculate odds ratios with 95% CIs for comparative AE risk. As the standard treatment, the MDBO group was set as the control group. All reported p-values were two-sided, and statistical significance was set at a p-value < 0.05. All statistical analyses were performed using SPSS (version 27.0; IBM Corp., Armonk, NY, USA).
Results
Study population
We enrolled 271 patients who achieved technical success, including 208 and 63 in the MDBO and MHBO groups, respectively (Figure 1). The MDBO group was treated using EUS-HGS alone. In the MHBO group, unilateral drainage (EUS-HGS alone) and bilateral drainage were performed in 26 (41.3%) and 37 (58.7%) patients, respectively. Among the bilateral drainage procedures, EUS-HGSB and ERCP + EUS-HGS were performed in 21 and 16 patients, respectively. Their baseline characteristics are summarized in Table 1. EUS-HGS was performed as a re-intervention procedure after ERCP in 57 (27.4%), 7 (26.9%), 6 (28.6%), and 12 (75.0%) patients in the EUS-HGS (MDBO), EUS-HGS (MHBO), EUS-HGSB, and ERCP + EUS-HGS groups, respectively (p = 0.004 within the MHBO group). There were no significant differences in laboratory data and the observation period. Furthermore, there was no significant difference in OS between each group (Supplemental Figure 2).
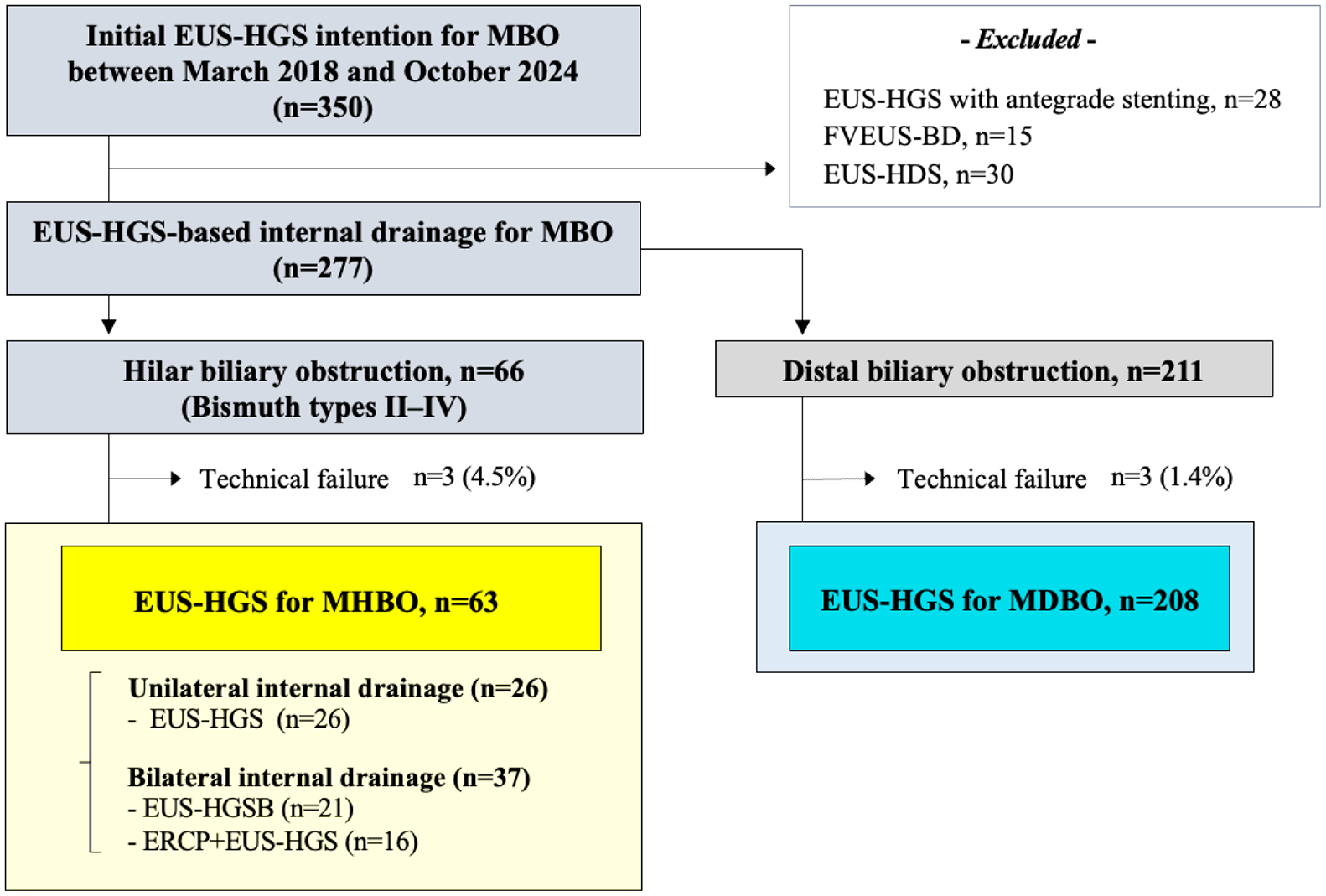
Study flowchart.
Baseline characteristics.

Data are presented as n (%) or median (IQR).
p-Values were analyzed within the MHBO group (among the three groups).
ERCP, endoscopic retrograde cholangiopancreatography; EUS-HGS, endoscopic ultrasound-guided hepaticogastrostomy; EUS-HGSB, endoscopic ultrasound-guided hepaticogastrostomy with bridging; IQR, interquartile range; MDBO, malignant distal biliary obstruction; MHBO, malignant hilar biliary obstruction.
Procedure background and details
The background and details of each drainage method are presented in Table 2. Among the MHBO groups, Bismuth types were significantly different in drainage methods for MHBO, including EUS-HGS alone, EUS-HGSB, and ERCP + EUS-HGS (p = 0.023). The reasons for performing EUS-HGS were also significantly different in drainage methods for MHBO (p < 0.001). Particularly, EUS-HGSB was performed mainly because of gastric outlet obstruction and altered anatomy, whereas ERCP + EUS-HGS was performed mainly because ERCP was not completed. The procedure time was significantly longer with bilateral drainage than with unilateral drainage (p = 0.032). There was no significant difference between stent types (metal stent vs PS) using EUS-HGS (p = 0.524).
Procedural background and details of the drainage techniques.

Data are presented as n (%) or median (IQR).
p-Values were analyzed within the MHBO group (among the three groups).
Duplicated number.
22-G, 22-gauge; B2 and B3, intrahepatic bile ducts of liver segments 2 and 3; B-II/IIIa/IIIb/IV, Bismuth type II/IIIa/IIIb/IV; ERCP, endoscopic retrograde cholangiopancreatography; EUS-HGS, endoscopic ultrasound-guided hepaticogastrostomy; EUS-HGSB, endoscopic ultrasound-guided hepaticogastrostomy with bridging; EUS-HJS, endoscopic ultrasound-guided hepatojejunostomy; IQR, interquartile range; MDBO, malignant distal biliary obstruction; MHBO, malignant hilar biliary obstruction.
Technical, clinical success, and AE rates
The short-term outcomes are summarized in Table 3. There was no significant difference in the technical success rate between the groups (p = 0.945). The clinical success rates were lower with EUS-HGS (MHBO) and ERCP + EUS-HGS in the MHBO group (76.9% (20/26) and 75.0% (12/16), respectively) than with EUS-HGSB; however, there was no significant difference (p = 0.671). In univariate logistic regression analysis, no significant factors were associated with clinical failure in the MHBO group (Supplemental Table 1(a)).
Short-term outcomes of drainage techniques.

Data are presented as n (%).
p-Values were analyzed within the MHBO group (among the three groups).
ERCP, endoscopic retrograde cholangiopancreatography; EUS-HGS, endoscopic ultrasound-guided hepaticogastrostomy; EUS-HGSB, endoscopic ultrasound-guided hepaticogastrostomy with bridging; MDBO, malignant distal biliary obstruction; MHBO, malignant hilar biliary obstruction.
The AE rates were 19.7% (41/208), 15.4% (4/26), 9.5% (2/21), and 25.0% (4/16) in the EUS-HGS (MDBO), EUS-HGS (MHBO), EUS-HGSB, and ERCP + EUS-HGS groups, respectively. The ERCP + EUS-HGS group showed the highest risk among the MHBO group, but this was not significant (p = 0.441; Figure 2). In univariate logistic regression analysis, no significant factors were associated with AEs in the MHBO group (Supplemental Table 1(b)).

Adverse events.
Time to recurrent biliary obstruction
There was no significant difference in median TRBO between the MDBO and MHBO groups (144 days (95% CI: 86.9–201) and 138 days (95% CI: 80.3–196), respectively, p = 0.658; Figure 3(a)). Among the MHBO group, TRBO was significantly longer with bilateral drainage than with unilateral drainage (p = 0.018; Figure 3(b)). Among the drainage methods, TRBO was longer with ERCP + EUS-HGS than other methods (p = 0.059; Figure 3(c)). Non-RBO rates at 180 days were 19.8% for EUS-HGS (MHBO), 61.9% for EUS-HGSB, and 68.4% for ERCP + EUS-HGS, respectively. For Bismuth type II, TRBO was longer with ERCP + EUS-HGS, followed by EUS-HGSB, compared with EUS-HGS (MHBO; p = 0.397; Figure 4(a)). In addition, for Bismuth type ⩾III, TRBO was longer with ERCP + EUS-HGS and EUS-HGSB than with EUS-HGS (MHBO; p = 0.208; Figure 4(b)).

TRBO. Kaplan–Meier curves for TRBO according to (a) MHBO (red line) versus MDBO (black line), (b) unilateral (red line) versus bilateral drainage (blue line), and (c) drainage methods (EUS-HGS, red line; EUS-HGSB, green line; ERCP + EUS-HGS, blue line).

TRBO by drainage techniques in Bismuth type II or ⩾III cohorts. Kaplan–Meier curve for the TRBO in three drainage methods (EUS-HGS, red line; EUS-HGSB, green line; ERCP + EUS-HGS, blue line) in the Bismuth type (a) II and (b) III or more.
In multivariate analysis of the MHBO group, EUS-HGSB tended to have a lower risk of RBO (adjusted hazard ratio (aHR), 0.39; p = 0.09), and ERCP + EUS-HGS showed a significantly lower risk (aHR, 0.25; p = 0.03) than EUS-HGS alone (unilateral drainage; Table 4).
Multivariate adjusted RBO analysis results of the MHBO group.

aHR, adjusted hazard ratio; CI, confidence interval; ERCP, endoscopic retrograde cholangiopancreatography; EUS-HGS, endoscopic ultrasound-guided hepaticogastrostomy; EUS-HGSB, endoscopic ultrasound-guided hepaticogastrostomy with bridging; HR, hazard ratio; MHBO, malignant hilar biliary obstruction; RBO, recurrent biliary obstruction; ref., reference.
Short-term outcomes of ERI
During the observation period, RBO occurred in 102 (37.6%) patients. Based on the patients’ general condition, 96 patients underwent ERI for RBO. In the EUS-HGSB and ERCP + EUS-HGS groups, re-bilateral drainage was achieved after ERI in all cases. The clinical success rates of ERI after EUS-HGS (MHBO) and EUS-HGSB were low at 66.6% (8/12) and 66.6% (2/3), respectively (p = 0.240; Table 5).
Short-term outcomes of ERI.

Data are presented as n (%).
Excluded the no intention of ERI: MDBO group (n = 3), unilateral drainage (EUS-HGS, n = 1), and EUS-HGSB (n = 2).
p-Values were analyzed within the MHBO group (among the three groups).
Technical success after ERI in bilateral drainage was defined as the appropriate stenting and re-achievement of bilateral drainage.
Clinical success was analyzed in patients who achieved technical success.
ERCP, endoscopic retrograde cholangiopancreatography; ERI, endoscopic re-intervention; EUS-HGS, endoscopic ultrasound-guided hepaticogastrostomy; EUS-HGSB, endoscopic ultrasound-guided hepaticogastrostomy with bridging; MDBO, malignant distal biliary obstruction; MHBO, malignant hilar biliary obstruction; RBO, recurrent biliary obstruction.
Discussion
This study showed that EUS-HGS for MHBO, especially bilateral drainage such as ERCP + EUS-HGS and EUS-HGSB, had an acceptable stent patency and safety profile. Limited evidence exists regarding the utility of EUS-HGS for MHBO; moreover, there have been no reports of its long-term outcomes. Therefore, this study may provide new insights into the short- and long-term outcomes and potential applications of EUS-HGS for MHBO.
Previous reviews have reported a high technical success rate of EUS-HGS for MHBO (98%); however, the clinical success rate was low (77%). 9 Here, the technical and clinical success rates were 95.4% and 79.4%, respectively. Although we did not identify any significant factors associated with clinical failure in the MHBO group, this low clinical success rate could be attributed to the fact that many patients with MHBO had extensive liver tumors, and clinical success could not be achieved by only removing the obstructive jaundice factor. This may also explain why re-intervention often failed to achieve clinical success, despite technically successful drainage. However, the clinical success rate of EUS-HGSB was high at 85.7% among the MHBO group. This technique may help prevent early liver dysfunction, but further studies are warranted to confirm it.
In our study cohort, the AE rates were comparable between the MHBO and MDBO groups. However, our study also showed that ERCP + EUS-HGS had the highest AE rate (25.0%). This is consistent with the results of previous studies reporting high AE rates for ERCP + EUS-HGS (range, 26.3%–35.0%).6,21 This could be attributed to both the use of different modalities (ERCP and EUS-HGS) and extended procedure time. 9 These findings may help with the clinical selection of internal drainage techniques for MHBO. By contrast, EUS-HGSB had a low AE risk (9.5%) and showed acceptable safety profiles. To reduce the risk of AEs such as bile juice leakage, sufficient suction of bile juice when selecting the bridging route, which is a difficult step and may consume a certain amount of time during EUS-HGSB, is deemed to be crucial. Our study revealed that the AE rate did not increase in EUS-HGSB owing to these considerations. In addition, although there was no significant difference in stent types between the groups, our previous report suggested that PSs may be associated with fewer AEs. 28 Therefore, the safety profile of stent types should be considered in future investigations.
There has been no previous report of stent patency in EUS-HGS for MHBO. Although TRBO was short with unilateral drainage, in our study, bilateral drainage methods, including EUS-HGSB and ERCP + EUS-HGS, resulted in favorable stent patency. Liver volume drainage of ⩾50% in MHBO patients with impaired liver function is required for effective biliary drainage. 29 In other words, bilateral drainage is required in most cases of MHBO. In ERCP for MHBO, bilateral drainage has a significantly longer stent patency than unilateral drainage.2,30 As a salvage method of ERCP as well, bilateral drainage using ERCP + EUS-HGS, EUS-HGSB, or EUS-HDS (which is expected in the future16,31) could be required when possible. Future studies are needed to confirm this robustly.
Bilateral drainage with ERCP only was effective in patients with Bismuth type III but not in those with Bismuth type IV. 4 However, our study demonstrated that ERCP + EUS-HGS resulted in acceptable outcomes even in Bismuth type III–IV cases. EUS-HGS does not traverse malignant biliary strictures and can be less affected by tumor progression. It was considered that acquiring two drainage routes, including this EUS-HGS route and other transpapillary routes, resulted in the longest TRBO in any hilar stenosis. Therefore, the addition of EUS-HGS to ERCP was thought to be effective even for Bismuth type IV. Given the AE risk, however, we should consider patient backgrounds, such as the performance status, prognosis, and remaining chemotherapy, when deciding to add EUS-HGS.
PTBD has been the standard rescue drainage method in cases in which ERCP fails for several reasons. However, PTBD carries burdens, such as external fistula management, risk of catheter dislodgement, and concerns over peritoneal seeding. By contrast, EUS-HGS is a minimally invasive option, with previous studies demonstrating a comparable or even superior safety profile, stent patency, and re-intervention success rates compared to PTBD.6,10 Furthermore, in this study, we showed that even in more complicated hilar obstructions, the outcomes of EUS-HGS for MHBO were comparable to those for MDBO. In addition, the efficacy of EUS-HGS in patients with duodenal obstruction has been increasingly reported.32,33 Based on these findings, we consider that, when the patient’s general condition allows for endoscopic intervention, EUS-HGS (particularly bilateral drainage combining ERCP + EUS-HGS or EUS-HGSB) should be considered in MHBO not only from the perspective of quality of life but also in terms of treatment outcomes.
This study has some limitations. First, the study design was retrospective, which has inherent limitations. We adjusted for potential confounding factors using multivariate Cox regression analysis as much as possible. Second, the definition of clinical success may underestimate outcomes in patients with advanced disease or extensive tumor burden. In the MHBO group, clinical failure may not necessarily indicate complete drainage failure, and alternative measures may be needed in the future. Third, most procedures were performed by non-expert endoscopists, defined as those with fewer than 30 EUS-HGS cases. Although outcomes were acceptable, the impact of operator experience on outcomes could not be assessed and should be investigated in future studies. Finally, the MHBO group had a small sample size, which might have limited the statistical power to detect significance. Therefore, the statistical power of the study must be factored in, considering the absence of significant differences. Further prospective and large-scale studies on EUS-HGS for MHBO are warranted.
Conclusion
EUS-HGS for MHBO, especially bilateral drainage using ERCP + EUS-HGS and EUS-HGSB, provided a comprehensively acceptable safety profile and effectiveness compared with that for MDBO. These bilateral drainages may serve as potential salvage options in the management of MHBO, although further validation in prospective multicenter studies is needed.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251356099 – Supplemental material for Clinical outcomes of endoscopic ultrasound-guided hepaticogastrostomy-based internal drainage for unresectable malignant hilar biliary obstruction: a comprehensive evaluation with malignant distal biliary obstruction
Supplemental material, sj-docx-1-tag-10.1177_17562848251356099 for Clinical outcomes of endoscopic ultrasound-guided hepaticogastrostomy-based internal drainage for unresectable malignant hilar biliary obstruction: a comprehensive evaluation with malignant distal biliary obstruction by Daiki Yamashige, Susumu Hijioka, Yoshikuni Nagashio, Shota Harai, Yasuhiro Komori, Aoi Kita, Masaru Kuwada, Soma Fukuda, Shin Yagi, Kohei Okamoto, Daiki Agarie, Shunsuke Sugawara, Miyuki Sone, Yutaka Saito and Takuji Okusaka in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848251356099 – Supplemental material for Clinical outcomes of endoscopic ultrasound-guided hepaticogastrostomy-based internal drainage for unresectable malignant hilar biliary obstruction: a comprehensive evaluation with malignant distal biliary obstruction
Supplemental material, sj-docx-2-tag-10.1177_17562848251356099 for Clinical outcomes of endoscopic ultrasound-guided hepaticogastrostomy-based internal drainage for unresectable malignant hilar biliary obstruction: a comprehensive evaluation with malignant distal biliary obstruction by Daiki Yamashige, Susumu Hijioka, Yoshikuni Nagashio, Shota Harai, Yasuhiro Komori, Aoi Kita, Masaru Kuwada, Soma Fukuda, Shin Yagi, Kohei Okamoto, Daiki Agarie, Shunsuke Sugawara, Miyuki Sone, Yutaka Saito and Takuji Okusaka in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We would like to thank the members of the Endoscopy Team of the Department of Hepatobiliary and Pancreatic Oncology, National Cancer Center Hospital, for their support of this research.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.