
Abstract
Background:
Upper gastrointestinal bleeding (UGIB) is a major medical emergency. Although older citizens have an increased risk of UGIB, guidelines do not fully address specific concerns in this population.
Objectives:
We aimed to report characteristics/differences between the older (⩾65 years) and the younger adult patients (<65 years) with UGIB.
Design:
Retrospective multicenter cohort study.
Methods:
Adult patients consecutively admitted due to evidence of UGIB at six participating centers or who developed UGIB while hospitalized for another reason during a 6-month enrollment period, were eligible for this study.
Results:
Of 600 patients included, 58.2% were men. Patients aged ⩾65 years comprised 72.8% of the cohort; in this group, most comorbidities (except liver cirrhosis) and use of antiplatelet/anticoagulant therapy were more frequent (p < 0.001). Variceal UGIB was more common in the younger group and non-variceal UGIB in the older (p < 0.001). The risk scores Glasgow–Blatchford (p = 0.003) and Complete Rockall (p < 0.001) were higher in the older group. Peptic ulcer disease was the most common cause in both groups, and angiodysplasia was an almost exclusive diagnosis in the elderly. Overall mortality was 15% (n = 90), with 76 deaths attributed to non-bleeding causes. In a post hoc subgroup analysis excluding cirrhotic patients, older adults required hospitalization (p = 0.007) and longer hospital stays (p = 0.005) more frequently, while younger patients had higher intensive care unit admission rates (p = 0.018). Multivariate analysis in this subgroup suggested that antiplatelet (p = 0.047) or anticoagulant use (p = 0.021), Rockall score (p < 0.001), and Charlson Comorbidity Index (CCI, p = 0.011) were independently associated with in-hospital mortality. The CCI, higher in older patients, also correlated with the need for blood transfusions (p = 0.001), rebleeding (p = 0.013), second-look endoscopy (p < 0.001), and re-hospitalization (p = 0.028).
Conclusion:
Older adults with UGIB exhibit clinical features associated with higher healthcare resource utilization and worse outcomes. Cirrhosis was linked to adverse outcomes in younger patients. In non-cirrhotic patients, UGIB may share features of geriatric syndromes, reflecting multifactorial risks in this population.
Introduction
Upper gastrointestinal bleeding (UGIB) is one of the most common medical emergencies managed by gastroenterologists, 1 accounting for 50% of admissions for gastrointestinal bleeding worldwide. 2 Despite advances in pharmacological/endoscopic therapy, this condition is still associated with considerable morbidity and mortality. 3 Patients with UGIB experience significantly higher 12-month healthcare resource utilization and cost than those without this condition. 4 The most common causes of UGIB include peptic ulcer disease (PUD), erosive gastroduodenitis, and gastroesophageal varices. 5
The increased life expectancy with a higher burden of comorbid conditions/factors and the use of drugs such as nonsteroid anti-inflammatory drugs (NSAID), antiplatelet/anticoagulant therapies, and corticosteroids, 6 predispose older patients to an increased risk of UGIB. This observation potentially validates the observed mortality rate of 5%–10% for severe UGIB, which has remained stable since the 1970s. 1 In fact, age, Helicobacter pylori infection, and the use of NSAIDs and/or anticoagulation are well-known independent risk factors for death from UGIB. 7 Furthermore, the geriatric population tends to have fewer herald symptoms before gastrointestinal bleeding, such as heartburn, dyspepsia, or abdominal pain, resulting in reduced opportunities for prevention and delayed diagnosis. This subset of patients is at higher risk of hospitalization and adverse outcomes. 4
Older adults have common health conditions that do not fit into distinct organ-based categories, often with multifactorial causes, named geriatric syndromes. 8 The first geriatric syndromes described were incontinence, immobility, and cognitive impairment, but since then other syndromes such as sarcopenia and frailty have been added. 9 These conditions are common in older adults, and they may have a major impact on quality of life and disability. 10
By the year 2050, the global population of individuals aged 60 years and over is predicted to increase from 12% to 22%, with the proportion of those aged 80 and over rising threefold. 11 This demographic shift underscores the necessity for an evidence-based clinical approach. However, the 2021 guidelines from the European Society of Gastrointestinal Endoscopy (ESGE) do not fully address specific concerns regarding the management of UGIB in the geriatric population. 12
In the present study, we aimed to characterize UGIB in the Portuguese reality and report essential characteristics and differences between the older (⩾65 years) and the younger adult patients (<65 years). Besides this objective, the following secondary objectives were defined: (1) to characterize the UGIB causes of patients admitted to the emergency room; (2) to describe clinical approaches associated with UGIB; and (3) to establish prognostic factors that may influence adverse outcomes, such as need for blood transfusion, length of hospital stay, endoscopic or surgical treatment, intensive care unit (ICU) admission, rebleeding, and in-hospital mortality.
Methods
Study design
We conducted an observational retrospective multicenter study that consecutively included all patients admitted to the emergency department with UGIB and underwent upper endoscopy in all six participating tertiary centers in Portugal: one from the center, four from the Lisbon metropolitan area, and one from the Azores.
The study was designed and conducted in accordance with the standards of the Declaration of Helsinki, and local ethics committees of each participating hospital approved the final protocol. Due to the noninterventional nature, routine practice at each participating center dictated patient management.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 13
Patient selection
Patients (male and female) aged ⩾18 years who were consecutively admitted to participating centers due to evidence of UGIB during a 6-month enrollment period (July 1–December 31, 2023) or who developed UGIB while hospitalized for another reason during this timeframe, were eligible for this study.
Evidence of UGIB was defined as hematemesis (coffee ground vomiting), melena, hematochezia, and other clinical or laboratory evaluation suggestive of blood loss (e.g., symptomatic iron deficiency anemia) confirmed by upper gastrointestinal endoscopy.
Patients with documented gastrointestinal bleeding and a confirmed etiology on rectosigmoidoscopy or colonoscopy were excluded. The patient flowchart of this study is detailed in Figure 1 Supplemental material.
Data collection
Data relevant to the initial UGIB episode and for up to 30 days afterward were collected retrospectively from patient medical records. The following characteristics were reviewed for each patient: demographic data (sex, age), comorbidities (namely, liver cirrhosis, congestive heart failure (CHF), diabetes mellitus), Charlson Comorbidity Index (CCI), previous UGIB episode, and drug use: NSAID’s, selective serotonin reuptake inhibitors, oral corticosteroids, and antiplatelet/anticoagulant agents. Clinical presentation (hematemesis, melena, hematochezia, and symptomatic iron deficiency anemia) and laboratory evaluation at admission (i.e., hemoglobin, platelets, international normalized ratio, creatinine, urea, and C-reactive protein) were also recorded.
Risk scores such as the Glasgow–Blatchford score (GBS) and the complete Rockall score (RS) were calculated as previously described.14,15 Data were also obtained regarding pre- and post-endoscopic management (i.e., proton pump inhibitor (PPI), prokinetic (erythromycin, metoclopramide, and domperidone)), etiology of UGIB, stigmata of recent bleeding, and hemostatic endoscopic therapy.
Different outcomes were analyzed: the need for endoscopic and/or surgical treatment, hospital admission, length of hospital stay, rebleeding, and in-hospital mortality were considered adverse outcomes.
Definition of variables, comorbidities, and other covariates
Older patients were considered to have a chronological age equal or above 65 years old as previously suggested. 16 Cirrhosis and CHF were defined in patients with a known history or clinical, laboratory, and imaging findings compatible with liver disease and CHF.17,18 Diabetes mellitus was considered in patients with a known history or who fulfilled the diagnostic criteria. 19 For patients with confirmed PUD as the underlying cause of UGIB, the Forrest classification system was employed. 20
Endoscopic hemostatic therapy included one or more of the following methods: sclerotherapy with polidocanol, cyanoacrylate, bipolar electrocoagulation therapy, argon plasma coagulation, topical hemostatic spray/powder, band ligation, through-the-scope, and over-the-scope clip, with or without epinephrine injection.
Surgery was regarded as the need for laparotomy/laparoscopic intervention due to refractory UGIB not amenable to all methods of endoscopic hemostasis. Rebleeding was defined as evidence of an overt bleeding episode or a decrease of at least 2 g/dL in hemoglobin levels after initial treatment and stabilization. 11
A subgroup analysis was performed, excluding all patients with liver cirrhosis, and both groups were subject to the same analysis as the complete sample.
Statistical analysis
All statistical analyses were performed using SPSS version 28 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize patients’ clinical data. Continuous variables were reported as mean ± standard deviation (SD), and categorical variables were expressed as absolute frequencies and percentages. Comparisons between age groups (<65 vs ⩾65 years) were performed using independent t tests or Mann–Whitney U tests for continuous variables (depending on data distribution) and χ² tests or Fisher’s exact tests for categorical variables. Multivariable regression models were developed for the entire cohort and non-cirrhotic subgroup to evaluate factors associated with clinical outcomes. Independent variables included age, sex, clinical risk scores (e.g., Rockall and CCI), and antithrombotic therapy. A stepwise backward elimination approach (Wald test; retention threshold p < 0.05) was used for variable selection. Binary logistic regression modeled binary outcomes (e.g., mortality and re-hospitalization), with results reported as adjusted odds ratios (ORs) and 95% confidence intervals (CIs). Negative binomial regression (log-link function) modeled count outcomes (e.g., blood transfusions and hospitalization days), accounting for overdispersion, with results expressed as incidence rate ratios (IRRs) and 95% CIs. The Wald test was used to assess the statistical significance of the OR/IRR. A p value less than 0.05 was considered statistically significant.
Results
A total of 600 patients were included during the 6-month enrollment period. Patients were aged from 18 to 100 years, with a mean age of 72 ± 16 years. 72.8% (n = 437) of all patients were older than 64 years, and 58.2% (n = 349) were male.
Smoking habits and alcohol consumption were significantly higher in younger patients, as well as the diagnosis of cirrhosis. Other comorbidities such as CHF, diabetes mellitus, and CCI were more frequent/higher in the older patients. The intake of antiplatelets and anticoagulants was more common in the elderly. No other differences were found regarding medication at admission.
Table 1 presents the demographic and clinical characteristics of both study groups.
Baseline demographic and clinical characteristics.

Bold data refers to statistical differences found on Z-test for proportions within multilevel categorical variables.
DOAC, direct oral anticoagulants; LMWH, low molecular weight heparin; NSAID, nonsteroid anti-inflammatory drugs; SD, standard deviation; SSRI, selective serotonin reuptake inhibitors; VKA, vitamin K antagonists.
The most frequent clinical presentation differed between the two groups: melena was more common in the older group, and hematemesis was more common in the younger group.
The causes of UGIB differed between the two groups, with variceal GIB significantly more frequent in the younger group and non-variceal GIB more common in the older group. PUD was the most common cause of UGI in both cohorts, with prevalence rates of 34.3% and 35.5%, respectively. The subsequent most prevalent diagnoses were angiodysplasia, erosive gastroduodenitis, and variceal bleeding. Angiodysplasia was predominantly observed in the elderly population. In patients with chronic liver disease, variceal bleeding emerged as the predominant cause of UGIB (n = 43, 43.9%), followed by PUD (n = 18, 18.4%).
In general, risk assessment scores were not widely used in all patients. Overall, the GBS and Complete RS were available for 85.5% and 81.8%, respectively. The RS and the GBS were higher in the older group, with a higher risk of adverse outcomes. Bleeding episode characteristics upon presentation, according to age group, are summarized in Table 2.
Bleeding episode characteristics.

Bold data refers to statistical differences found on the Z-test for proportions within multilevel categorical variables.
GAVE, gastric antral vascular ectasia.
Prior to the initial endoscopy, 84%–86% of patients from both groups had received PPI treatment in accordance with local treatment protocols. Concerning prokinetic therapy, less than 20% of patients received this pharmacological approach, with metoclopramide being the most commonly prescribed in older patients and erythromycin in younger patients. Furthermore, vasopressor and antibiotic prophylaxis were more frequently prescribed to the younger group. Therapeutic procedures were performed during initial endoscopy in 35.6% (age <65) and 39.3% (age ⩾65). Combination therapy was the most common hemostatic therapy, using epinephrine injection plus a second hemostasis modality (contact, thermal, or mechanical therapy). Band ligation (p = 0.016) and isolated polidocanol (p = 0.042) were preferentially used in the younger group, in all cases due to variceal bleeding. In contrast, argon plasma coagulation was more commonly used ⩾65 years (p = 0.032). No patient in this study underwent interventional radiology therapy. Management of bleeding episodes, according to age group, is summarized in Table 3.
Management of bleeding episode.

Bold data refers to statistical differences found on the Z-test for proportions within multilevel categorical variables.
Mean hospitalization time was 10 ± 16 (age <65) and 11 ± 16 (age ⩾65) days. ICU admission was more common in the younger group (p = 0.012). Most patients required at least one blood transfusion before or after the endoscopy (56.3%), and almost half of both groups required transfusion(s) before the endoscopy (48.7%). Length of hospitalization, re-hospitalization, blood transfusions, or need for surgery did not differ between the two groups. Globally, in-hospital mortality was 13% (78 patients) and 30-day mortality was 15% (90 patients) in this study, most of the cases (n = 76) due to non-bleeding occurrence. Both in-hospital mortality and 30-day mortality were similar between the two groups.
The multivariate analysis of the entire cohort indicated that liver cirrhosis was a significant predictor of several adverse outcomes: blood transfusions (p = 0.032), prolonged hospitalizations (p < 0.001), subsequent re-hospitalization (p = 0.023), and in-hospital mortality (p = 0.002).
UGIB in non-cirrhotic patients
A subgroup analysis was performed, excluding all patients with liver cirrhosis. A total of 502 patients were included, 107 with age <65 years and 395 with age ⩾65 years.
Smoking habits and alcohol consumption were higher in younger patients. Comorbidities such as CHF, diabetes mellitus, and CCI were more frequent/higher in older patients, as well as the intake of antiplatelets/anticoagulants. Table 4 summarizes the demographic and clinical characteristics of both study groups.
Baseline demographic and clinical characteristics.
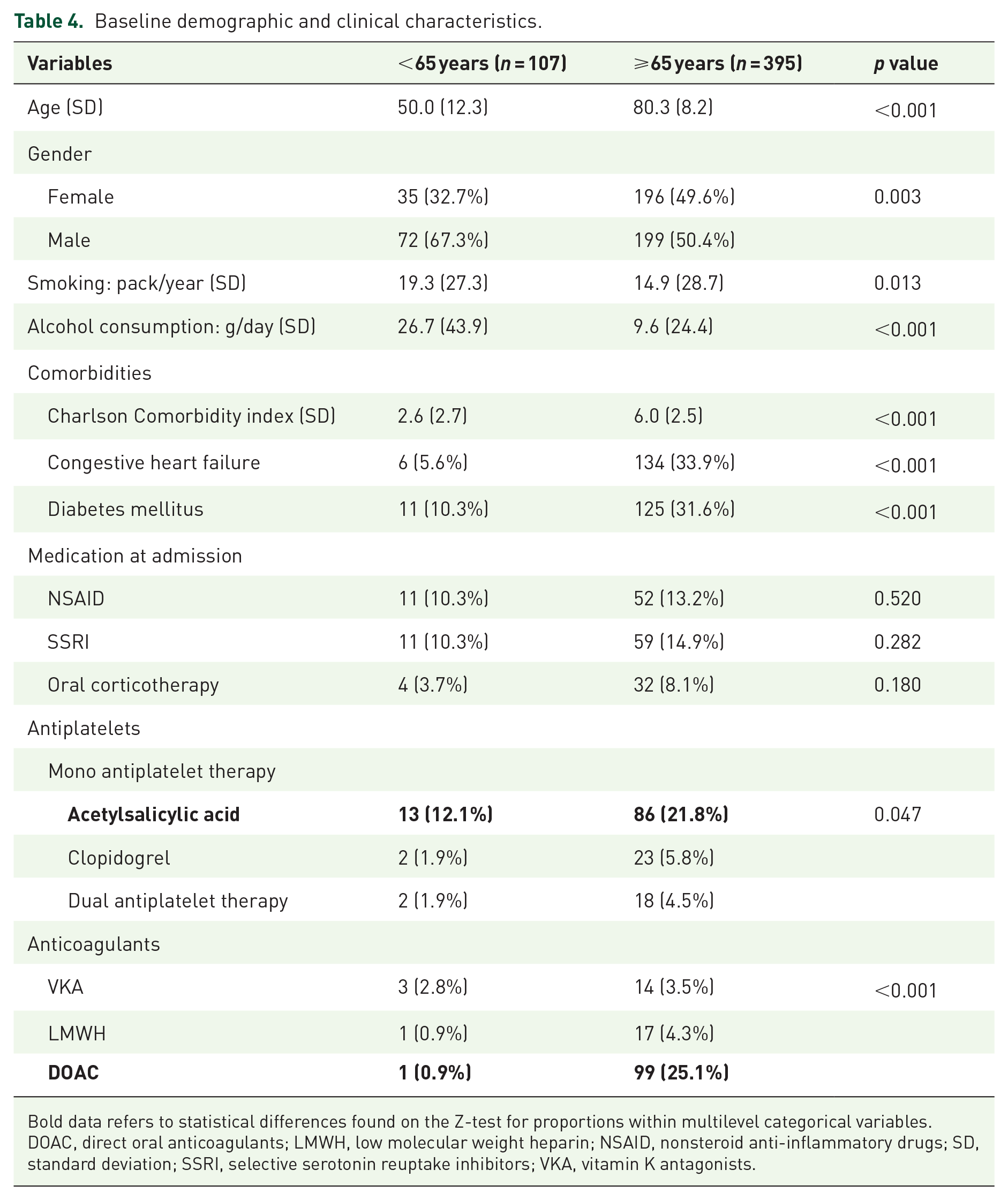
Bold data refers to statistical differences found on the Z-test for proportions within multilevel categorical variables.
DOAC, direct oral anticoagulants; LMWH, low molecular weight heparin; NSAID, nonsteroid anti-inflammatory drugs; SD, standard deviation; SSRI, selective serotonin reuptake inhibitors; VKA, vitamin K antagonists.
A comparative analysis of the clinical manifestations of UGIB across the two groups revealed a significant difference: melena was observed more frequently in the older group, while hematemesis was observed more frequently in the younger group.
The causes of UGIB were similar in the two groups, with angiodysplasia being the only condition that occurred more commonly in the older patients. PUD was the most common cause of UGI in both groups (42.1% and 37.3%, respectively), followed by angiodysplasia, erosive gastroduodenitis, and malignancy. Regarding risk assessment scores, both the Rockall and the GBS were higher in the older group (Mann–Whitney test, p < 0.001 and p < 0.001, respectively). Bleeding episode characteristics upon presentation, according to age group, are summarized in Table 5.
Bleeding episode characteristics.

Bold data refers to statistical differences found on Z-test for proportions within multilevel categorical variables.
GAVE, gastric antral vascular ectasia.
Prior to the initial endoscopy, 83%–85% of patients from both groups received PPI treatment. Regarding prokinetic therapy, less than 20% have received this pharmacological therapy. Both vasopressor and antibiotic prophylaxis use were prescribed in 5.6% of the younger group, attributed to presumed variceal UGIB. Therapeutic procedures were performed in both groups in 30.8% (age <65) and 38.9% (age ⩾65) during the initial endoscopy, respectively. Argon plasma coagulation was more commonly used ⩾65 years (p = 0.043). Management of bleeding episodes, according to age group, is summarized in Table 6.
Management of bleeding episode.

Bold data refers to statistical differences found on the Z-test for proportions within multilevel categorical variables.
Hospitalization was needed more frequently in the older group (p = 0.007), who also required more days admitted in the gastroenterology/internal medicine ward (p = 0.005). ICU admission was more common in the younger group (p = 0.018). In-hospital mortality was higher in the older group, although it did not reach statistical significance (p = 0.383). No differences were found regarding blood transfusions and the need for surgery. Table 7 summarizes the use of healthcare resources according to a study group.
Use of healthcare resources.

ICU, intensive care unit.
After adjusting for confounders, multivariate analysis identified the use of antiplatelets (OR 1.443; CI 1.198–1.989; p = 0.047) and/or anticoagulants (OR 1.385; CI 1.171–1.868; p = 0.021) as independent predictors of in-hospital mortality. In addition, the GBS and RS were significantly associated with the need for hospitalization, length of hospital stay, and blood transfusions. The RS is also strongly associated with in-hospital mortality (OR 1.398; CI 1.159–1.686; p < 0.001). A higher CCI was associated with an increased likelihood of requiring blood transfusions (IRR 1.913; CI 1.863–1.965; p = 0.001), second-look endoscopy (OR 1.493; CI 1.250–1.784; p < 0.001), rebleeding (OR 1.849; CI 1.746–1.965; p = 0.013), re-hospitalization (OR 1.158; CI 1.016–1.321; p = 0.028), and in-hospital mortality (OR 1.186; CI 1.040–1.352; p = 0.011). Table 8 summarizes the predictive factors associated with adverse outcomes.
Predictive factors (first row) of adverse outcomes (first column).

Predictor coefficients comprise the OR, or the IRR, confidence intervals, and the Wald test p value.
ICU, intensive care unit; IRR, incidence rate ratio; OR, odds ratio.
Discussion
UGIB clinical and endoscopic management underwent considerable changes over time as a result of several improvements in pharmacologic therapies and the quality of endoscopic care. However, the increasingly frequent elderly population, with several comorbidities and associated polypharmacy, faded the improvement in these patient outcomes.
Our study, specifically designed to compare characteristics of UGIB between younger and older adults in a “real-life” setting, showed substantial differences regarding clinical/endoscopic characteristics, management, and outcomes in UGIB. Our results, considering also previous studies,21 –24 reflect a trend toward older and frailer patients that present with UGIB, highlighting new differential characteristics that may be overlooked. Although cirrhosis may occur in all age groups,25,26 in this study, it was the only comorbidity more common in younger patients, which may reflect a national/regional trend of higher alcohol consumption in these populations, also seen in other European studies.27,28
The main cause for UGIB in both groups was PUD. The low proportion of patients in this cohort who were prescribed NSAIDs differs from the findings of other studies 29 but may be indicative of a bias related to the loss of information rather than a significant decrease in the consumption of these drugs. Our study suggests that the epidemiology of UGIB appears to be shifting, with a decline in PUD (previously accounting for 60% of all presentations of UGIB 30 ), possibly due to reduced H. pylori infection and lesser use of NSAIDs, and an increase in causes commonly associated with aging, namely angiodysplasia.31,32 Also, although without statistical significance, esophagitis was more common in the elderly, potentially reflecting long-standing acid reflux and medication-induced esophagitis. 33
Management of bleeding episodes, including pharmacological therapy, varied widely in this study. Continuous infusion was the most common method of administration of PPI, although according to ESGE guidelines, intravenous bolus or oral administration are considered reasonable alternatives. 12 Regarding prokinetic therapy, metoclopramide was more commonly prescribed in older patients, although its use in UGIB cannot be supported due to insufficient data 34 and in older adults it may cause tardive dyskinesia. 35 Since cirrhosis was more common in the younger group, it is no surprise that the higher prescription of “empiric” vasopressor and antibiotic prophylaxis in this age group.
Concerning adverse outcomes in this study, surprisingly they did not differ in both study groups. After adjusting for confounders, and in line with other studies,36 –38 cirrhosis emerged as an independent predictor of in-hospital mortality and may provide a rationale for the adverse outcomes observed in the younger population.
UGIB in non-cirrhotic patients occurred mainly in the elderly group, accounting for almost 80% of UGIB. Interestingly, we still found “empiric” vasopressor and antibiotic prophylaxis in the younger group, probably due to higher alcohol consumption and presumed cirrhosis and variceal UGIB at the emergency room, as recommended.39,40
Our study established the impact of higher CCI in the older population, with a clear association with adverse outcomes (second-look endoscopy, re-hospitalization, and in-hospital mortality). Moreover, as several comorbidities are associated with antiplatelet and/or anticoagulant use, those therapies increase the morbidity from UGIB and correlate with in-hospital mortality. These findings align with other studies that suggest the outcome of UGIB in the elderly is determined not only by the nature of the lesion but also by the existence of comorbidities and the use of antiplatelets/anticoagulants.41 –43 In addition, it is known that the use of anticoagulants is associated with increased second-look endoscopy and recurrent bleeding in patients admitted with UGIB. 44 Geriatric patients may present a high likelihood of continued bleeding in the setting of the lack of vasospasm due to deranged thrombotic and/or platelet function (secondary to consumption coagulopathy and/or to antiplatelet/anticoagulant therapy), highlighting the importance of monitoring for bleeding recurrence. 4
A study of healthcare resource utilization reveals that younger patients face more expeditious admission to the ICU. This phenomenon may reflect an age bias, as there is a concern that the prognosis for older patients is less favorable than that for younger patients, irrespective of the underlying diagnosis. 45 However, as stated by Brunker et al., 46 there is a growing population of older adults requiring admission to the ICU. In some cases, acute situations may outpace the ability of clinicians with geriatric training to assist in their management. Consequently, the determination of mortality in the ICU is not solely reliant on age.47,48
The need for hospitalization was more common in the older patients, as well as the time admitted to the gastroenterology/internal medicine ward, highlighting the complexity of these patients and the possible decompensation of other organs and systems. Despite this, upper endoscopy is a largely safe procedure in this population. A higher proportion of normal findings on endoscopy is seen in the elderly reinforces the importance of a careful selection of patients. 49
Risk scores (GBS and the complete RS) were applied to most of the patients in this study. On multivariate analysis, both scores had a good correlation with the need and length of hospitalization, as well as the need for blood transfusions. However, in the present study, the complete RS was a better predictor of in-hospital mortality, which differs from other studies that suggested GBS was the better score overall in terms of prediction of hospital-based intervention or death. 50 When GBS was formulated, age was not found to be an independent predictive factor of adverse outcomes and was not included in this score. With a progressively older population, this score may underestimate the risk of adverse outcomes. For instance, age ⩾60 years is included as a risk factor in the complete RS. 15 Other risk scores not addressed in this research, such as the pre-endoscopic AIMS-65 or the ABC score, which perform reasonably well for prediction of mortality, may have a role in future studies, although not recommended in the latest guidelines on UGIB.38,51 Furthermore, in the era of artificial intelligence, machine-learning models have shown significant promise in risk scoring for UGIB and may overcome the criticism of complexity regarding current risk scores. 52
In-hospital mortality was superior in older patients (12% against 9%), in line with other studies. 15 This trend reflects several age-related processes and risk factors that not only predispose these patients to UGIB but also to poor outcomes, as demonstrated by this study and by other authors. 4 The trends observed in UGIB mortality vary across published studies, with most assuming stable rates over the past few decades. The global mortality rate observed in this study (15%) surpasses those reported in most contemporary studies,3,21 –23 largely attributable to non-bleeding-related causes. This fact should again alert clinicians to the support of other major organ systems in patients with UGIB while hospitalized.
Since UGIB in non-cirrhotic patients is a frequent and severe condition among older patients, we believe it may be regarded as a geriatric syndrome. One of the widely accepted definitions for the geriatric syndrome is a “condition in which symptoms develop when the accumulated effect of the several impairments in multiple domains compromise compensatory ability and reserve and the final outcome is a single phenomenology.” 53 UGIB has a high prevalence in the elderly population, accounting for 77.6% of all cases of gastrointestinal bleeding, 5 and can manifest anywhere on a spectrum from occult bleeding to life-threatening hemorrhage. This condition shares common risk factors with other geriatric syndromes, such as age, polypharmacy, and multimorbidity, besides having close interactions with “geriatric giants,” namely frailty, as stated by Guliyara et al., 54 who concluded that frailty is an important independent predictor of mortality in patients with UGIB. Furthermore, like other geriatric syndromes, UGIB has a clear, unfavorable impact on older patients, as demonstrated in this study. A multidimensional intervention with a multidisciplinary team is of utmost importance for managing this condition in older patients, including compensatory and rehabilitative approaches. For those reasons and according to all the literature mentioned, we believe that, in non-cirrhotic patients, UGIB may be considered a geriatric syndrome. Interventions aimed at reducing risk factors will improve the incidence and severity rates of UGIB in older citizens.
A major strength of this study is its multicentric nature, involving departments with different characteristics and from a variety of regions across the country. Furthermore, our observational study represents a comprehensive analysis of a large number of bleeding patients in a real-world clinical setting, in which guidelines are being implemented in the clinical management of a large, diverse group of patients with UGIB.
However, some limitations need to be outlined. The study design was retrospective, and data were collected from electronic medical records that lacked standardization, resulting in heterogeneous clinical data. In addition, upper endoscopy findings were inconclusive in some cases, and after excluding lower gastrointestinal bleeding, these patients were included in the sample. It is plausible that a few cases were small bowel bleeding rather than genuine UGIB. Nevertheless, we posit that the preponderance of cases were UGIBs that were not identified during upper endoscopy. The infrequent occurrence of small bowel bleeding in the patient population is unlikely to have substantially impacted the results and subsequent analysis.
In the coming years, a new study prospectively evaluating UGIB outcomes in the progressively older population is warranted, hopefully with the involvement of more centers from European countries. Gastroenterology departments must increase their commitment to the digestive care of geriatric patients.
Conclusion
UGIB seems to present different features in elderly citizens. In younger patients, cirrhosis accounts for the poor outcomes. In non-cirrhotic patients, these hemorrhages are almost exclusive of older patients who show several severity characteristics and worse outcomes than younger adults. In older patients, UGIB may present characteristics of a geriatric syndrome.
Supplemental Material
sj-jpeg-1-tag-10.1177_17562848251343416 – Supplemental material for Upper gastrointestinal bleeding differences between older and younger adults: should bleeding in non-cirrhotic patients be considered a geriatric syndrome?
Supplemental material, sj-jpeg-1-tag-10.1177_17562848251343416 for Upper gastrointestinal bleeding differences between older and younger adults: should bleeding in non-cirrhotic patients be considered a geriatric syndrome? by Francisco Vara-Luiz, Ivo Mendes, Carolina Palma, Paulo Mascarenhas, Diogo Simas, Plácido Gomes, André Ruge Gonçalves, Inês Simão, Madalena Teixeira, Sara Ramos Lopes, Francisca Côrte-Real, Maria Antónia Duarte, Catarina Bravo, Marta Patita, Gonçalo Nunes, Pedro Pinto-Marques and Jorge Fonseca in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.