
Abstract
Background:
Delayed postpolypectomy bleeding (DPPB) constitutes one of the most prevalent complications following endoscopic mucosal resection (EMR) for colonic polyps and can be life-threatening. It has been affirmed that prophylactic clip closure can effectively diminish the risk of DPPB for colonic polyps exceeding 20 mm in the right half of the colon after EMR. Nevertheless, there remains controversy regarding whether prophylactic clip closure can prevent postoperative bleeding for polyps measuring less than 20 mm. To date, no literature has reported whether the complete closure of titanium clips following EMR for colorectal polyps ⩽20 mm can effectively prevent delayed bleeding.
Objectives:
The aim of this study is to determine whether complete closure can prevent delayed postoperative bleeding and analyze the related factors that might influence delayed postoperative bleeding.
Design:
In this retrospective study, a total of 1259 colorectal polyps detected in 1025 patients between January 2020 and October 2024 were evaluated for EMR.
Methods:
Univariate and logistic regression analyses were conducted to assess patient-related, polyp-related, and procedure-related factors.
Results:
DPPB was observed in 37 patients, representing an incidence rate of 3.6%. Logistic regression analysis indicated that male (odds ratio, 3.870; 95% confidence interval (CI), 1.594–9.396; p = 0.003), presence of large polyps (OR, 1.158; 95% CI, 1.044–1.285; p = 0.006), and partial closure (OR, 5.447; 95% CI, 2.250–13.186; p < 0.001) are significant risk factors for the development of DPPB.
Conclusion:
Male, polyp size, and partial closure have been identified as potential risk factors for the development of DPPB. While gender and polyp size are immutable factors, partial closure is particularly associated with an increased risk of DPPB. Therefore, it is imperative to ensure complete closure of the wound following EMR to minimize the occurrence of DPPB.
Keywords
Introduction
Colorectal cancer is a malignant tumor characterized by high incidence and mortality rates, making early detection, diagnosis, and treatment particularly crucial. Screening via colonoscopy, accompanied by endoscopic colorectal polypectomy, has been demonstrated to effectively reduce colorectal cancer mortality.1,2 With the ongoing advancements in medical technology, various methods for colorectal polypectomy have emerged, including hot snare polypectomy, cold snare polypectomy, endoscopic mucosal resection (EMR), endoscopic submucosal dissection (ESD), hot biopsy, and argon plasma coagulation. 3 Among these, EMR is one of the most frequently employed techniques for polyp removal, initially introduced by Deyhle et al. 4 in 1973 for the excision of rectal polyps. As endoscopic techniques have evolved, EMR has been shown to be both safe and effective. 5 The removal of colorectal polyps through EMR can significantly decrease the incidence of colorectal cancer. 6
Delayed postpolypectomy bleeding (DPPB) is one of the most common complications following polypectomy, typically occurring after 24 h, with an incidence rate ranging from 2.6% to 9.7%. 7 The primary risk factors associated with delayed bleeding can be categorized into patient-related, polyp-related, and procedure-related factors. 8 Patient-related factors encompass the patient’s gender, age, comorbidity, and whether the patient is an outpatient or inpatient. Polyp-related factors include the size, morphology, location, and pathohistological type of the polyp. Procedure-related factors involve the endoscopist’s experience, wound management techniques to prevent bleeding, and the bowel preparation employed during polypectomy. In recent years, the prevention of delayed bleeding following EMR has emerged as a significant area of research. There is an ongoing debate regarding the necessity of using endoscopic clips to close the wound post-EMR. 9 Most literature suggests that the application of endoscopic clips for wounds after EMR of colorectal polyps larger than 20 mm can significantly reduce the incidence of delayed bleeding.10,11 However, only a few authors have indicated that complete closure with endoscopic clips is a crucial factor in preventing delayed bleeding.7,12 Currently, there is a lack of relevant literature addressing whether complete closure using titanium clips after EMR of colorectal polyps measuring ⩽20 mm can prevent delayed bleeding. This study aims to conduct a retrospective analysis to determine the effectiveness of complete closure with titanium clips in preventing delayed bleeding and to examine the factors that may influence this outcome.
Materials and methods
Patients
A retrospective cohort study was employed to collect the medical records of patients who underwent EMR resection of colorectal polyps in our hospital from January 2020 to October 2024. Inclusion criteria: (1) Patients who underwent EMR for colorectal polyps in our hospital and received outpatient follow-up within 30 days. (2) Normal coagulation function. (3) Prohibition of antiplatelet agents and anticoagulants for at least 5 days prior to colonoscopy. Exclusion criteria: (1) Incomplete case data. (2) History of inflammatory bowel disease, ischemic bowel disease, familial adenomatous polyposis, radiation colitis, and surgery for colorectal cancer. (3) EMR resection of polyps accompanied by ESD or nylon cord ligation. (4) Polyps larger than 20 mm. (5) Postoperative pathology of the polyps suggesting carcinoma or failed tissue recovery. During the study period, a total of 5596 patients were treated with EMR for colorectal polyps. According to the inclusion and exclusion criteria, a total of 1259 colorectal polyps that underwent EMR were identified in 1025 patients and included in the analysis. The study was examined and approved by the Ethics Institutional Review Board of Luohu District People’s Hospital, Shenzhen, China.
Preoperative preparation
All patients underwent electrocardiogram examinations prior to the surgery. Patients were prescribed a low-fiber, semi-liquid diet commencing 2 days before the examination. Those scheduled for an afternoon examination were instructed to take two bags of polyethylene glycol electrolyte solution (dissolved in 2 L of warm water) on the evening prior to the examination and one bag on the morning of the examination (dissolved in 1 L of warm water). Those slated for an afternoon examination were directed to commence taking three bags of polyethylene glycol electrolyte solution (dissolved in 3 L of warm water) on the day of the examination to cleanse the colon until watery stool was excreted, and a supplementary enema was administered if necessary.
Preparations for equipment
An electronic colonoscope (CF-H290; Olympus, Japan), disposable biopsy forceps (Hangzhou Kangsheng Medical, Chin), disposable endoscope injection needles (Micro-Tech, Nanjing, China), rechargeable endoscope snare (COOK USA), titanium clips (Micro-Tech), and a high-frequency electrocautery device (Erbe, Germany) were employed, with a commonly utilized coagulation power ranging from 20 to 50 W.
Endoscopic polyp EMR resection
All study polyps were removed by standard EMR. 7 First, the submucosal injection of diluted adrenaline (1:10,000) was utilized to elevate the polyp from the submucosal layer, offering a secure cushion for resection. Subsequently, the polyp is excised using an electrical snare through a combination of electrocoagulation and electrical resection. After the polyp was removed, the wound was closed using titanium clips, as depicted in Figure 1.
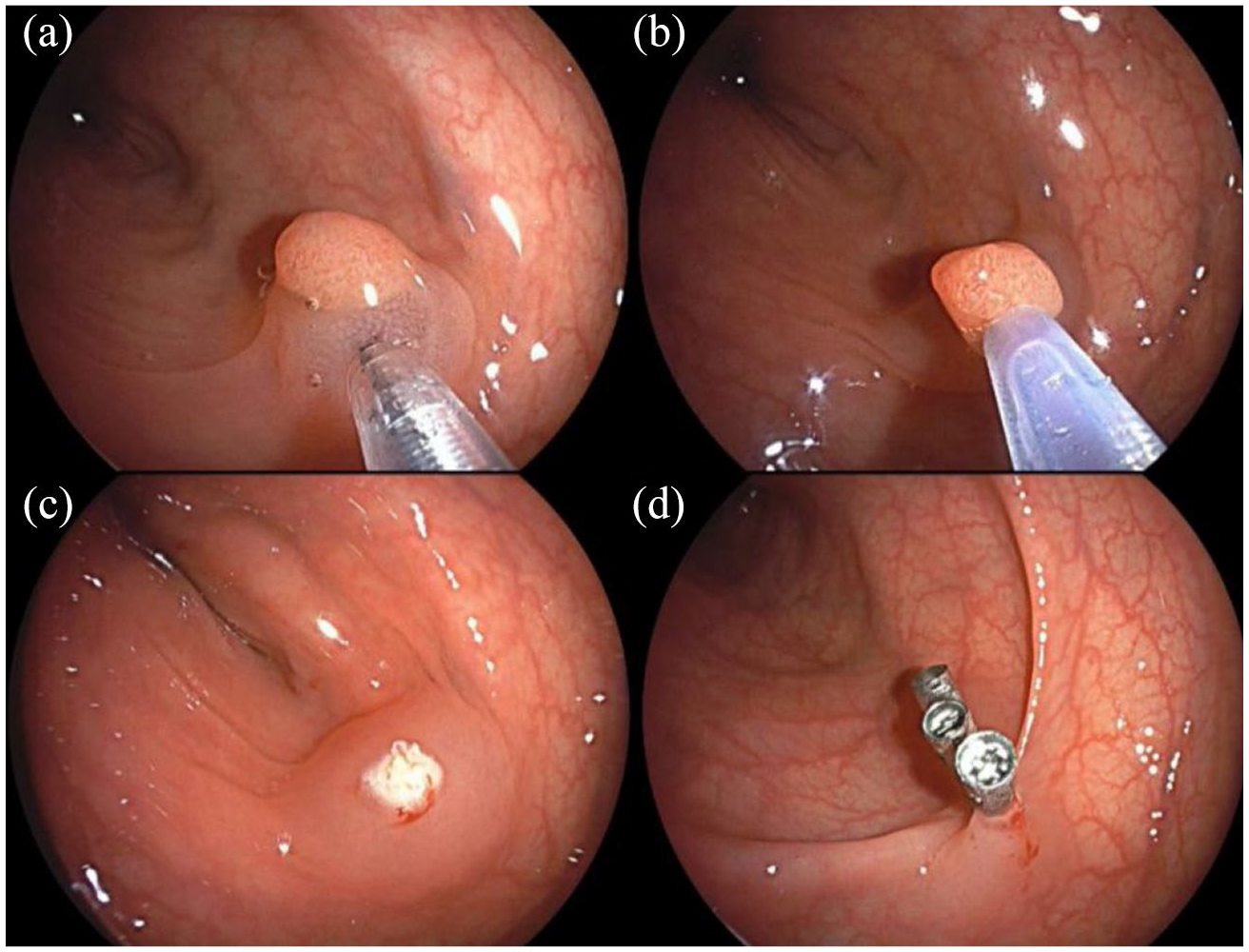
Procedure of EMR surgery. (a) Submucosal injection of epinephrine. (b) Encircling the polyp with the snare. (c) The postoperative wound following blended current resection of the polyp. (d) Closure of the postoperative wound with titanium clips.
Definition
Delayed postpolypectomy bleeding
DPPB is defined as bleeding occurring within 30 days after polyp resection, characterized by hematochezia. The bleeding was confirmed via colonoscopy to originate from the wound site of the polypectomy.
Parallel position closure
The axis resulting from the closure by the titanium clip has an angle of not more than 30° with the adjacent colon wall (Figure 2(a)) and is frequently employed for the closure of the surgical site following EMR for pedunculated polyps. The specific approach is to position the titanium clamp parallel to the postoperative wound surface, with the two arms, respectively, placed on either side of the wound surface. After pressing down, the clamp is transversely closed from the bottom of the wound surface.

Diverse forms of complete closure. (a) Complete closure in parallel position. (b) Complete closure in standing position (no submucosal wound visible). (c) Complete closure in standing position (visible submucosal wound, but titanium clamps closed tightly, impossible to add titanium clamps). (d) Mixed type of complete closure.
Standing position closure
The axis formed upon the closure of the metal titanium clamp exhibits an angle of more than 30° with the adjacent colon wall (Figure 2(b) and (c)), and it can be utilized for the closure of the wound resulting from the resection of sessile or pedunculated polyps by EMR. The specific procedure is as follows: Position the titanium clamp perpendicular to the postoperative wound, grasp the mucosa on both sides of the wound with the two arms of the clamp, apply suction to reduce the size of the wound, then press the clamp and tighten the closure.
Mixed closure
It incorporates both parallel and standing closure modalities (Figure 2(d)).
Complete closure
According to Albéniz et al., 12 the definition of complete closure is as follows: the titanium clamps are adjacent to one another, and there is no visible submucosal wound on the closure line. To make it more specific, we modify it into the following contents: (1) Standing position complete closure (Figure 2(b) and (c)), mixed complete closure (Figure 2(d)): The titanium clamps are adjacent to one another, and all the non-clamping mucosal parts of the clamps are in close proximity to the mucosa of the intestinal wall. There is no visible submucosal wound on the closure line, or although there is a submucosal wound between the clamps, the clamps are closed tightly and another titanium clamp cannot be inserted. (2) Parallel position complete closure (Figure 2(a)): The titanium clamps are fully transversely closed after clamping the wound, that is, the front end of the clamped mucosa exceeds the wound.
Partial closure
(1) Standing position partial closure (Figure 3(a) and (b)) and mixed partial closure (Figure 3(d)): Visible submucosal wounds on the closed line remain unclosed. Owing to the considerable gap between adjacent titanium clamps, an additional titanium clamp can be employed to close the wound. Alternatively, after the titanium clamp is closed, no visible submucosal wound is present, but more than half of the two arms of the titanium clamp holding the mucosa are exposed above the mucosal surface. (2) Parallel position partial closure (Figure 3(c)): After the wound is closed by the titanium clip, the wound is not completely transversely severed, that is, the front end of the mucosa held by the titanium clip does not surpass the wound. Another titanium clip can be added to continue closing the wound.

Originates from cases of delayed bleeding after EMR, featuring various types of partially closed wounds. (a, b) Both represent standing position partial closure. (c) Parallel position partial closure. (d) Mixed partial closure (the two arms of the titanium clamp holding the mucosa on the left have more than half exposed on the mucosal surface).
Patient-related factors
This encompasses gender, age, comorbidity, and the mode of consultation. Among them, some patients may have comorbidities such as hypertension, diabetes, hyperlipidemia, and coronary heart disease. The mode of consultation encompasses outpatient and inpatient patients. In this study, all patients are proposed to cease taking antiplatelet and anticoagulant drugs 5–7 days prior to colonoscopy. After EMR for colonic polyps, patients should be advised to refrain from taking antiplatelet and anticoagulant drugs for at least 5 days postoperatively based on their conditions.
Polyp-related factors
The size, macroscopic form, location, and histopathological type of all polyps removed by EMR should be recorded. The size of each polyp is measured using a single biopsy forceps (with the maximum possible opening angle of 6 mm) as close to the lesion as feasible. Macroscopic appearance was classified as either nonprotruded (sessile or flat elevated) or protruded (pedunculated or semipedunculated). 13 The location of the polyps is divided into cecum, ascending colon, transverse colon, hepatic flexure, splenic flexure, descending colon, sigmoid colon, and rectum. Among these, the cecum, ascending colon, hepatic flexure, and the right half of the transverse colon are classified as the right half of the colon, while the left half of the transverse colon, splenic flexure, descending colon, sigmoid colon, and rectum are classified as the left half of the colon. 8 The histopathological types include hyperplastic polyps, inflammatory polyps, tubular adenomas, villous adenomas, tubular-villous adenomas, retention polyps, serrated polyps, and low-grade intraepithelial neoplasia.
Procedure-related factors
Procedure-related factors involve the endoscopist experience, wound management techniques to prevent bleeding, and the bowel preparation employed during polypectomy. According to the endoscopic surgery authorization standards of our hospital’s Gastrointestinal Endoscopy Center, endoscopist experience is categorized into three levels based on the number of EMR procedures performed: fewer than 100 cases (beginner level), 100–300 cases (intermediate level), and more than 300 cases (advanced level). The methods of wound management to prevent bleeding include the completion status of titanium clips, the closure method of titanium clips, and the number of titanium clips used. The completion status of titanium clips is categorized as either complete closure or partial closure. The closure method of titanium clips includes parallel position closure, standing position closure, and mixed closure, as previously defined. Bowel preparation is evaluated using the Boston bowel preparation scale, which divides the colon and rectum into three regions: the right colon (cecum and ascending colon), the transverse colon (including the hepatic flexure and splenic flexure), and the left colon (descending colon, sigmoid colon, and rectum). Each region is scored individually, with higher scores indicating superior bowel preparation quality. 14
Data analysis
In the univariate analysis, normally distributed continuous data are analyzed using the independent samples t test, and categorical data are analyzed using the Chi-square test or Fisher’s exact test. When a variable has more than two subgroups, Fisher’s exact test is employed. The results of the multivariate logistic regression analysis are presented as odds ratios (OR), and a p-value < 0.05 indicates a statistically significant difference. Data are recorded using Microsoft Excel, and statistical analyses are conducted using SPSS 27.0 software.
Results
Patient-related factors
A total of 5596 patients underwent EMR surgery for colorectal polyps, of whom 1025 patients with 1259 colorectal polyps were included in the analysis. According to Table 1, 37 patients (3.6%) experienced DPPB after EMR, while 988 patients (96.4%) did not experience DPPB. All patients with DPPB were hospitalized at our center and successfully treated with titanium clip hemostasis, leading to their discharge after recovery. In the bleeding group, 31 patients (83.8%) were male, and 6 patients (16.2%) were female. In the control group, 559 patients (56.6%) were male, and 429 patients (43.4%) were female. Univariate analysis revealed that male patients had a significantly higher risk of bleeding compared to female patients (p = 0.001). However, age, whether the patient is an outpatient or inpatient, and the presence of hypertension, diabetes, hyperlipidemia, and coronary heart disease were not found to be significantly associated with DPPB as risk factors.
Patient-related risk factors for DPPB.

Values are the mean with SD or number (%).
DPPB, delayed postpolypectomy bleeding.
Polyp-related factors
According to Table 2, 39 out of 1259 polyps (3.1%) experienced postoperative bleeding, while 1220 (96.9%) did not. Univariate analysis revealed that there was no significant difference in polyp location or pathological type between the bleeding group and the control group, whereas polyp size and morphology were significantly different (p values of 0.004 and <0.001, respectively). The mean size of polyps in the bleeding group was 10.38 ± 3.632 mm, compared to 8.61 ± 2.611 mm in the control group. Larger polyps were associated with a higher risk of bleeding. Among the 39 bleeding polyps, 13 were Ip-type polyps (33.3%), 9 were Isp-type polyps (23.1%), 8 were Is-type polyps (20.5%), and 9 were IIa-type polyps (23.1%). Pedunculated polyps were more prone to bleeding compared to sessile polyps.
Polyp-related risk factors for DPPB.

Others included: inflammatory polyps: 147, hyperplastic polyps: 203, retention polyps: 7.
DPPB, delayed postpolypectomy bleeding; LGIN, low-grade intraepithelial neoplasia.
Procedure-related factors
According to the univariate analysis in Table 3, the endoscopist’s level of experience, the number of titanium clips used, the closure method of titanium clips, and the Boston bowel preparation scale were not statistically significant. However, the completion status of titanium clips was statistically significant (p < 0.001). In the bleeding group, 6 cases (15.4%) were complete closure, while 33 cases (84.6%) were partially closure. In the control group, 634 cases (52.0%) were complete closure, while 586 cases (48.0%) were partially closure. These data indicate that complete closure can significantly reduce the risk of bleeding after EMR, while partial closure is a risk factor for DPPB.
Procedure-related risk factors for DPPB.

Endoscopist experience: fewer than 100 cases (beginner level), 100–300 cases (intermediate level), and more than 300 cases (advanced level).
DPPB, delayed postpolypectomy bleeding.
Logistic analysis for DPPB
Univariate analysis indicated that male, polyp size, polyp morphology, and partial closure were statistically significant. Further logistic regression analysis was performed as below. According to the multivariate analysis results in Table 4, male, larger polyp size, and partial closure of titanium clips were identified as risk factors for DPPB. Male patients were 3.87 times more likely to develop late hemorrhage compared to female patients (95% confidence interval (CI), 1.594–9.396; p = 0.003). In addition, larger polyps were associated with a 1.158-fold increase in bleeding risk compared to smaller polyps (95% CI, 1.044–1.285; p = 0.006). Notably, partial closure of titanium clips was associated with a 5.447-fold higher risk of late hemorrhage compared to complete closure (95% CI, 2.250–13.186; p < 0.001).
Multivariate analysis of risk factors for DPPB.

Macroscopic appearance was classified as either protruded (Isp, Ip) or nonprotruded (IIa, Is).
CI, confidence interval; DPPB, delayed postpolypectomy bleeding.
Conclusion
EMR is more likely to result in DPPB compared to cold resection, as thermal resection causes more extensive damage to deeper layers of the intestinal wall and involves more major blood vessels.3,15 The ongoing debate regarding the efficacy of endoscopic clips in preventing DPPB underscores the need for further investigation. The underlying causes of DPPB following EMR have thus emerged as a critical area of study. Numerous meta-analyses and randomized controlled trials have clearly demonstrated that the use of clips to prophylactically close the wound after EMR for large polyps greater than 20 mm in diameter located in the right colon can effectively reduce the risk of DPPB.10–12,16–18 With the continuous development of ESD technology, the rates of en bloc resection and curative resection are significantly higher than those of EMR, while the incidence of complications remains low. For large lesions, the rate of polyp malignant transformation increases, making ESD clearly more advantageous than EMR. 19 Therefore, the study of EMR resection for colorectal polyps ⩽20 mm in clinical practice has significant clinical importance. According to some studies, for polyps with a diameter of less than 20 mm, prophylactic clipping may not be necessary to prevent post-polypectomy bleeding.20–22 However, these studies did not perform EMR resection on all polyps, and the closure group did not specify whether complete closure was achieved. Currently, there is no literature on whether complete closure of titanium clips after EMR resection of colorectal polyps ⩽20 mm can prevent DPPB, prompting us to conduct a retrospective study.
Currently, there are two different views on the definition of complete closure in the relevant literature. Some scholars define complete closure as the method where the interspace between adjacent clamps is less than 10 mm.7,10 This definition is applicable to polyps with a diameter greater than 20 mm and is suitable for closing the wound using hemostatic clips rather than titanium clips. Hemostatic clips provide a more secure closure but are more expensive. Titanium clips have good grasping power and are also frequently used for sealing wounds after ESD. In clinical practice, for small wounds resulting from EMR of polyps ⩽20 mm in diameter, titanium clips are typically used due to their lower cost and practicality, making the aforementioned definition unsuitable. Therefore, we prefer the definition of complete closure proposed by Albéniz et al., 12 which states that the clips were applied next to each other and there were no substantial submucosal areas in the closure line (as shown in Figure 1(d)). Our data show that partial closure significantly increases the risk of DPPB, and the risk of delayed bleeding caused by partial titanium clip closure is 5.447 times that of complete closure (95% CI, 2.250–13.186; p < 0.001). Thus, improving the ability to achieve complete closure of the wound after EMR will help further reduce the risk of postoperative bleeding. This conclusion is consistent with findings from some previous studies.7,12 Accordingly, surgeons are required to improve their operational skills to achieve complete closure of the endoscopic clips and reduce the risk of bleeding. Single-factor and multivariate analyses revealed that male patients and larger polyp sizes were also statistically significant. Some literature suggests that female patients are more likely to adhere to postoperative behavior guidelines compared to male patients. 3 In our study, we observed that male patients have a higher incidence of DPPB. Follow-up assessments revealed that male patients are less likely to adhere to the recommended postoperative dietary guidelines and activity restrictions. Specifically, most male patients resumed consumption of solid foods within 1–2 days post-surgery, whereas female patients generally complied with our advice to maintain a liquid diet. Therefore, for male patients undergoing EMR, healthcare providers should emphasize detailed dietary instructions and educate patients on potential risk factors that may contribute to DPPB. Previous research has indicated that polyp size is one of the key factors influencing the incidence of DPPB,23–25 which aligns with our findings. The reason may be that larger polyps have more vascular supply, leading to larger wounds and more severe vascular damage during resection, thereby increasing the likelihood of bleeding. 3
There is currently controversy regarding whether the location of polyps is a risk factor for bleeding. Some scholars propose that right colonic polyps are risk factors for DPPB,25,26 possibly due to histological differences between the left and right colon, where the collagen fibers in the submucosal layer of the left colon are smaller and more tightly packed, making the submucosal layer of the right colon thinner. 27 However, other scholars have found that DPPB is more likely to occur when the lesion is located in the rectum. 28 In our study, a total of 39 polyps exhibited post-procedural bleeding. Among them, seven cases (17.9%) involved rectal polyps that bled following EMR surgery, representing a relatively small proportion of the overall bleeding polyps. Our study suggests that the location of polyps is not significantly associated with DPPB, and further prospective studies are needed. Literature indicates that pedunculated polyps are an important risk factor for delayed bleeding, 29 but some studies suggest that pedunculated polyps do not increase the risk of DPPB, 8 and our study also shows that pedunculated polyps are not significantly associated with bleeding.
Interestingly, we further classified complete closure into parallel complete closure, standing complete closure, and mixed complete closure based on the clinical titanium clip closure method, and there is currently no related literature reporting this classification. In the univariate analysis, these three closure methods were not statistically significant for bleeding risk (p = 0.140). Regardless of the closure method used, achieving complete closure significantly reduces the risk of bleeding. A limited number of prior studies have examined the relationship between endoscopist experience and bleeding risk.8,29 However, our findings indicate no significant association between these factors. Further prospective studies are warranted to validate these results.
Certainly, there are some limitations in our study. As a retrospective study, control over patients who underwent polyp resection was limited. However, we better controlled the factors affecting the study by implementing strict inclusion and exclusion criteria. This study did not investigate the relationship between the type of submucosal injection solution, submucosal injection elevation, the type of electrosurgical current or cutting current, and DPPB. There have been reports in the literature on the relationship between the choice of resection current and bleeding. 30 However, in our study, all cases involved blended current, which requires further investigation in the future. Our study demonstrates that incomplete closure is a risk factor for delayed postoperative bleeding after EMR, and complete closure with titanium clips can significantly reduce the risk of DPPB in lesions ⩽20 mm. In addition, male and larger polyps are also risk factors for DPPB. For male patients, postoperative emphasis should be placed on avoiding vigorous exercise, consuming rough and hard foods, and drinking alcohol to prevent postoperative bleeding. The size of the polyp is an uncontrollable variable, but complete closure with titanium clips is achievable.
Therefore, in daily clinical practice, surgeons should focus on completely closing the surgical site after EMR of colorectal polyps to reduce the risk of DPPB. We look forward to more randomized controlled trials in the future to verify this conclusion.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251332836 – Supplemental material for Complete closure utilizing titanium clips minimizes delayed postpolypectomy bleeding after colorectal endoscopic mucosal resection: a retrospective analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848251332836 for Complete closure utilizing titanium clips minimizes delayed postpolypectomy bleeding after colorectal endoscopic mucosal resection: a retrospective analysis by Wei-Feng Li, Bing Lai, Li Lv, Xi-Qiu Yu, Jia-Le Fan, Zhi-Wei Zhou, Jing-Wen Xu, Ruo-Yu Gao, Ze-Ming Chen and Bi-Xia Xu in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.