
Abstract
The prevalence of anxiety, depression, and other psychological comorbidities among patients with inflammatory bowel disease (IBD) significantly exceeds that of the general population. Moreover, a bidirectional relationship exists between psychological comorbidities and IBD. This intricate interplay has substantial clinical implications, impacting treatment adherence, therapeutic efficacy, and disease recurrence rates. In this review, we explore the multifaceted mechanisms through which psychological factors influence IBD progression, treatment response, and prognosis. Specifically, we delve into the involvement of the hypothalamic-pituitary-adrenal axis, autonomic nervous system, enteric nervous system, microbiota-gut-brain axis, systemic inflammatory cytokines, and immune cell function. Additionally, we discuss the potential benefits of antidepressant therapy in mitigating IBD risk and the role of psychotropic drugs in reducing peripheral inflammation. Recognizing and addressing psychological comorbidity is pivotal in comprehensive IBD management. We advocate for the integration of biopsychosocial approaches into IBD treatment strategies, emphasizing the need for innovative psychological interventions as adjuncts to conventional therapies. Rigorous research investigating the impact of antidepressants and behavioral interventions on IBD-specific outcomes may herald a paradigm shift in IBD management.
Keywords
Introduction
Inflammatory bowel disease (IBD) represents a group of chronic intestinal disorders characterized by inflammation, which are believed to arise due to a complex interplay of genetic, environmental, and immunological factors. 1 These conditions are associated with a high rate of recurrence, significant intestinal morbidity, and substantial healthcare expenditures. 2 Globally, the prevalence of IBD has shown a marked increase in recent years, posing a serious threat to public health. 3 Emerging research indicates that the prevalence of psychological comorbidities, such as anxiety and depression, is considerably higher in individuals with IBD compared to the general population. This suggests a bidirectional association between psychological disturbances and IBD. 4 However, the exact causal relationship and direct correlation between IBD and psychological comorbidities remain to be conclusively established. Consequently, there is a pressing need for further clinical and fundamental research to elucidate the underlying pathophysiological mechanisms in IBD patients with concomitant psychological disorders. Understanding these mechanisms is crucial for the development of more effective therapeutic strategies.
This review aims to encapsulate the current advancements in this domain and tries to explore the effective management and treatment of IBD from the perspective of psychological comorbidities. While this is not a systematic review, we have employed a targeted approach to identify relevant literature that aligns with our research focus. Specifically, we have utilized a combination of search strings to ensure a comprehensive and relevant selection of articles, including primary search string with a combination of the terms “IBD” and “Psychological comorbidities,” and additional search strings such as “anxiety in IBD,” “depression in IBD patients,” “IBD and quality of life,” and “psychological impact of IBD.” Furthermore, we have also drawn upon our accumulated knowledge and expertise in the field over the years, which has informed our selection of articles that are particularly pertinent to our research questions and objectives.
The bidirectional relationship between IBD and psychological comorbidities
Proof of the bidirectional relationship between IBD and psychological disorders
IBD, which includes Crohn’s disease (CD) and ulcerative colitis (UC), is witnessing a concerning uptrend in global incidence. 1 The chronicity of these conditions has been significantly correlated with increased instances of anxiety, depression, and mood disorders, particularly among young individuals with long-standing medical issues who exhibit a heightened prevalence of major depression. 4 Our prior research has demonstrated a greater frequency of psychological comorbidities among patients with IBD relative to those with other chronic diseases or the healthy population. 5 Furthermore, numerous studies have highlighted a susceptibility to depression in patients with IBD, which not only worsens their clinical outcomes but also suggests a bidirectional interplay. 6 For example, depression is reported associated with a diminished quality of life (QoL), sexual dysfunction, intensified disease activity, and more frequent exacerbations. 7 Notably, depression can manifest even in patients with IBD in clinical remission. 8 Longitudinal observations indicate that initial depression may predict suboptimal disease management in subsequent evaluations. 9 Inversely, psychological disturbances may act as precursors to IBD, influencing its onset, progression, and prognosis. 10 A comprehensive cohort analysis has revealed a significantly elevated risk of developing CD and UC among depressed individuals. 11 The unadjusted risk for CD development in depressed patients was 67% higher than their non-depressed counterparts, and this association persisted even after adjusting for variables such as age, gender, socioeconomic status, comorbidities, obesity, smoking habits, anxiety, and use of antidepressants. The unadjusted risk increase for UC in the depressed cohort was 41%, and post-adjustment, the risk was found to be more than double compared to those without depression. 11
In a recent population-based cohort study, structured psychiatric interviews were utilized as the gold standard for diagnosing psychological conditions, facilitating a comparison of the prevalence rates of psychological disorders between the IBD cohort and matched community samples without the disease. The investigation revealed a heightened prevalence of anxiety, generalized anxiety disorder, obsessive-compulsive disorder, and major depressive disorder in the IBD group, whereas the rates of social anxiety and bipolar affective disorder were comparatively lower. Remarkably, the incidence of depressive disorders in the IBD cohort was nearly twice that observed in the community sample, with more than a quarter of the patients with IBD experiencing major depressive disorder. Additionally, individuals with coexisting anxiety or mood disorders reported a reduced QoL, an earlier onset of IBD symptoms, and a trend toward a younger age at IBD diagnosis. Moreover, among those with IBD and concurrent anxiety or mood disorders, 79% had their initial anxiety disorder onset more than 2 years before the IBD diagnosis, and about half of those with coexisting mood disorders had their initial depressive episode more than 2 years before the onset of IBD. Extensive analysis indicated that disease activity, IBD subtype (CD or UC), educational level, marital status, employment status, and age were not significantly associated with psychiatric comorbidity diagnoses. 10 The presence of psychological comorbidity was linked to the female gender, a lower QoL index IBD questionnaire (IBDQ), and perceptions of psychological health and stress. Notably, a multiple logistic regression analysis incorporating all variables determined that only female gender and diminished psychological health were independently associated with the presence of recent anxiety or mood disorders. 10 In another large-scale investigation, data from 152,461 women aged 29–72 years from the Nurses’ Health Study cohort were analyzed 12. Employing self-assessment of depression symptoms via the Mental Health Index-5 and blind review confirmation of CD and UC diagnoses by two expert gastroenterologists, the study identified an increased risk of developing CD in women with recent depressive symptoms, but not an elevated risk for UC, during 1,787,070 person-years of follow-up, which included 170 cases of CD and 203 cases of UC. 12 These previous researches indicated that psychological comorbidities are not only more prevalent in patients with IBD compared to those with other chronic conditions or the healthy population but also contribute to a bidirectional relationship that exacerbates IBD’s clinical outcomes (Figure 1), and this bidirectional relationship was very solid even after excluding potential confounding variables. These findings highlight the need for a comprehensive approach to IBD treatment that includes regular mental health assessments and the integration of biopsychosocial models to tailor personalized treatment plan and to improve patient outcomes and QoL.

Bidirectional relationship between IBD and psychological comorbidities.
Measures used to diagnose the psychological disorders in IBD
As psychological comorbidities are prevalent in patients with IBD and can exacerbate IBD’s clinical outcomes, psychological assessment of the patients is important for the clinicians to tailor suitable treatment schedules. Various psychological assessment tools have now been utilized in the evaluation of patients with IBD. The most frequently used are listed as follows: (1) The Zung Self-Rating Anxiety Scale (SAS) and Self-rating Depression Scale (SDS) are widely recognized self-report questionnaires designed to assess the symptoms, severity, and clinical status of diseases. Each item in these scales is scored from 1 to 4, and the total scores are multiplied by 1.25 for standardized interpretation. A SAS score of 50 or above indicates the presence of anxiety, while a score of over 53 on the SDS suggests persistent depression. Higher scores on these scales are correlated with a higher likelihood of psychological morbidity 13 ; (2) The Hamilton Anxiety Scale (HAMA) and Hamilton Rating Scale for Depression (HRSD) are classic examiner-rating scales used to assess a patient’s condition over the past week and can be utilized for efficacy evaluation. They are simple, easy to administer, and applicable to various conditions, including physical illnesses with depressive symptoms. However, as examiner-rating scales, they may not be widely used in the IBD field due to the lack of qualifications among many gastroenterologists 14 ; (3) The Hospital Anxiety and Depression Scale (HADS) is a 14-item self-assessment scale that evaluates symptoms of depression and anxiety, with each item scored from 0 to 3. A score above 7 is considered pathological, and higher scores indicate more severe symptoms. 15 HADS is designed for patients with physical illnesses or those who are hospitalized and has been proven to have high specificity in IBD 16 ; (4) The Patient Health Questionnaire-9 items (PHQ-9) for depression is the most extensively evaluated tool in primary care research and has been identified as the most reliable screener for depressive disorders. It demonstrates an optimal balance between sensitivity and specificity, offering the highest performance and accuracy in a primary care setting and supporting concurrent screening for depression and suicide risk. Higher scores indicate more severe depressive symptoms in the respondent. The PHQ-9 has been validated for use in patients with IBD, and there are also studies utilizing the abbreviated Patient Health Questionnaire-8 (PHQ-8) for measurement, as referenced previously in the literature 17 ; (5) The Symptom Checklist-90 (SCL-90) comprises 90 items and serves as a self-report scale suitable for individuals older than 16 years. It assesses the conditions of the most recent week, encompassing a broad spectrum of psychopathological symptoms, such as thought processes, emotions, behaviors, interpersonal relationships, and sleep and eating habits. The scale utilizes a 5-point rating system from 1 to 5, allowing for the calculation of both total scores and scores for nine specific factors, including somatization, obsession-compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobia, paranoia, and psychoticism. A total score exceeding 160 points, or any factor score exceeding 2 points, warrants consideration for positive screening and further diagnostic evaluation and treatment. The SCL-90 can provide a comprehensive assessment of psychological symptoms, including anxiety and depression, and enjoys extensive application in clinical practice 18 ; (6) The Patient-Reported Outcomes Measurement Information System (PROMIS) encompasses the Depression Short Form (PROMIS Depression) and Anxiety Short Form (PROMIS Anxiety), which are self-reported questionnaires consisting of eight items each. These instruments are designed to assess levels of anxiety and depression experienced over the past week. 19 PROMIS has been proven to provide a valid assessment of the health-related quality of life (HRQoL) and functioning in large IBD internet-based cohorts and in ambulatory adults with IBD 20 ; (7) The Generalized Anxiety Disorder-7 (GAD-7) is a 7-item self-report questionnaire that exhibits strong psychometric properties, including reliability and structural validity. While the GAD-7 was primarily designed as a screening instrument for generalized anxiety, it has also demonstrated efficacy in identifying three other prevalent anxiety disorders: panic disorder, social anxiety disorder, and post-traumatic stress disorder, which has been used for assessing depression and anxiety disorders in patients with IBD 21 ; (8) Depression Anxiety Stress Scales (DASS-21). This instrument consisted of a set of three 7-item depression, anxiety, and stress survey tools. A 4-point Likert-like scale ranging from 0 to 3 was used to rate the tent of stress, anxiety, and depression over the previous week. Scores were doubled and summed to give a range of stress from 0 to 42, with higher scores indicating higher levels of distress 22 ; (9) The Short Form-36 Health Survey (SF-36), also known as the Medical Outcomes Study Short Form-36, is one of the most used standardized measures of HRQoL internationally. The SF-36 consists of 9 dimensions and 36 items, assessing 8 aspects of health: Physical Functioning, Role Limitations due to Physical Health, Bodily Pain, General Health Perceptions, Vitality, Social Functioning, Role Limitations due to Emotional Problems, and Mental Health. Additionally, there is a self-rated health transition item that compares the individual’s health to that of 1 year prior, which is not included in the scoring of the subscales or the total score; it reflects longitudinal changes in health status. The SF-36 can be completed by self-administration, by proxy, or through a telephone interview. Higher scores on the scale indicate better QoL.23,24 However, the SF-36, commonly used in IBD clinical trials to assess overall HRQoL, lacks a domain that evaluates the impact of the disease on sleep, which is significant for patients with IBD; 10) The 29-item Patient-Reported Outcomes Measurement Information System® (PROMIS-29) is a validated tool for assessing HRQoL, encompassing seven domains (depression, anxiety, physical function, pain interference, fatigue, sleep disturbance, and social role participation), each with four items. An additional item for pain intensity is also included. Compared to the SF-36, PROMIS-29 features an easy-to-use, publicly available scoring system. It is extensively utilized in clinical research outcomes for a variety of chronic conditions. Summary scores (Physical Component Summary (PCS) and Mental Component Summary (MCS)) are derived from individual scores, from which the PCS focuses more on pain, physical function, and the ability to participate in social roles, while the MCS emphasizes emotional distress (depression/anxiety). 25
Other screening tools, such as the 5-item Anxiety and Depression Detector, utilize five straightforward yes-or-no questions. It has been found to be sensitive and possesses reasonable specificity. The Luebeck Interview offers a more comprehensive scope of information for patient management, covering areas including social support, depression, and anxiety caused by IBD, and it takes an average of 5–10 min to administer. 26 Beck’s inventories for anxiety and depression are also notable. 27 Most studies employ various questionnaires to assess disease diagnosis or quantify symptoms, with the HADS being the most common. However, there is a significant variation in cutoff values even among studies utilizing HADS, complicating comparisons between studies. 28
Collectively, the plethora of psychological assessment tools available for use with IBD patients underscores the importance of careful consideration when selecting the most appropriate measures for a given study or clinical context. Each instrument possesses unique psychometric properties that cater to specific aspects of psychological distress, such as anxiety, depression, or stress. The choice of assessment tool should be guided by several factors, including the study’s objectives, the population under investigation, the desired depth of assessment, and the practicality of administration and scoring. For example, the Zung SAS and SDS provide a standardized approach to self-reported symptom evaluation, while the HAMA and HRSD offer a clinician’s perspective on the patient’s condition; the HADS stands out for its specificity in assessing psychological distress in physically ill populations, including patients with IBD. The PHQ-9 is renowned for its reliability in primary care settings, and the SCL-90 offers a comprehensive assessment of a broad spectrum of psychopathological symptoms; the PROMIS measures, GAD-7, and DASS-21 provide concise yet robust evaluations of depression and anxiety, while the SF-36 and PROMIS-29 provide a more holistic view of HRQoL, with the latter being particularly adept at capturing the impact of IBD on sleep. Given the heterogeneity of IBD and its psychological comorbidities, no single tool can fully encapsulate the breadth of the patient experience. Therefore, a multifaceted approach, potentially combining multiple instruments, may be necessary to capture the nuanced interplay between psychological well-being and IBD. Ultimately, the selection of psychological measures should be tailored to the needs of the research or clinical setting, ensuring that the chosen tools offer the most relevant and accurate assessment of the constructs of interest.
Psychological comorbidity in IBD under remission, other illness or symptoms
It is indeed a critical issue that even when patients with IBD are in remission, they may continue to experience anxiety due to concerns about the unpredictable nature of their disease. Studies have reported that the rate of anxiety remains between 29% and 35% during remission. 26 A Romanian cross-sectional study involving 132 patients with IBD in remission found that 34.1% of patients exhibited anxiety, with the majority (68.9%) experiencing mild symptoms. The proportion of patients with depressive symptoms was lower (18.2%), while the vast majority (91.7%) had mild symptoms. 15 Furthermore, an international multicenter prospective study conducted during the COVID-19 pandemic recruited patients with IBD from eight European centers and Israel who were in clinical remission, had not used corticosteroids within the past 12 months, and had no symptom flare-ups or complications. These patients showed higher rates of anxiety and depression than usual, suggesting that the pandemic has exacerbated the degree of emotional disorders in these patients. 29 These findings underscore the importance of recognizing and addressing the persistent psychological impact on patients with IBD, even in the absence of active disease. The COVID-19 pandemic has further complicated this issue, highlighting the need for continued mental health support and tailored interventions to improve the well-being of patients with IBD.
Moreover, the COVID-19 pandemic could have impacts on the pathologies of the bidirectional interactions between IBD and psychological comorbidities. For example, several large case studies highlighted that the indirect damages caused by the fears and anxieties associated with the COVID-19 pandemic had impacts on IBD. Specifically, a study from Japan investigated the impact of the COVID-19 pandemic on the anxiety and behavioral changes of patients with IBD from March 2020 to June 2021. 30 The analysis of 3032 questionnaires from patients with IBD across 31 medical centers revealed that the top 3 causes of anxiety were the risk of contracting COVID-19 during hospital visits, the risk of SARS-CoV-2 infection due to IBD, and the risk of infection from IBD medications. Factors associated with anxiety included gender (women), being a homemaker, hospital visit duration, mode of transportation (train), the use of immunosuppressive drugs, and nutritional therapy. Most patients continued to visit hospitals and take medications as scheduled, seeking guidance and information about COVID-19 from doctors, television, and the internet. However, a minority reduced their medication dosage or discontinued treatment due to stable abdominal symptoms, doctor’s advice, or fear of infection from medication. Both timely medical visits and the deferral or cancellation of check-ups significantly affected patients’ anxiety scores, which notably decreased after vaccination. A significant proportion of patients (42.6%) received explanations from their doctors regarding the continuation of their medication, which reduced their anxiety levels after the explanation. 30 Additionally, a study from the Hepato-gastroenterology Unit of the University of Campania in Italy reported an overall treatment non-adherence rate of 32.8% (69/210) among patients with IBD from February 2021 to February 2022. 31 Females, younger patients, and those diagnosed with IBD at a younger age showed higher treatment non-adherence. Non-adherence was also higher among patients with a previous SARS-CoV-2 infection. However, patients with a higher level of education exhibited better adherence. Some patients were fearful that they were more susceptible to severe COVID-19, and the majority opted for telemedicine as their preferred follow-up tool. A small portion of patients were skeptical about vaccination due to concerns about interference with IBD treatment, adverse reactions, or perceived ineffectiveness. A significant number (61.4%) felt they were not adequately informed or reassured by their family doctors. This underscores the need for reassurance in chronic disease management even at the primary care level, especially in the context of the COVID-19 environment. 31 Collectively, the COVID-19 pandemic has not only heightened the anxiety levels of these patients but also affected their therapeutic adherence, which is a critical factor in the management of chronic conditions like IBD. The findings underscore the importance of psychological support and clear communication from healthcare providers to ensure continued medication adherence and mitigate the indirect effects of the pandemic on patient well-being.
In addition, the IBD patient may suffer from disability symptoms such as incapacity, fatigue, poor health, treatment side effects, and limited participation in various aspects of life, including social and psychological services. 32 These symptoms in patients with IBD have been proven related to psychological comorbidities in several ways. A systematic review focusing on patients with IBD aged 10–24 highlights that QoL-related symptoms, such as abdominal pain, negative illness cognition, sleep disturbances, and non-adherence to medication, may strengthen psychiatric comorbidities in young patients. 33 Conversely, HRQoL in the IBD population has been reported significantly determined by psychological comorbidities, including perceived stress, anxiety, and affective comorbidities. 34 Moreover, participants with active IBD symptoms and psychological comorbidities are more likely to suffer from poor sleep and insomnia. Patients with IBD report longer sleep latencies and reduced sleep efficiency, and sleep complaints are predictive of increased risk of surgery and hospitalization and are independently associated with reduced QoL. These comorbidities further resulted in a lack of interest in eating or food, or concerns about the adverse consequences of eating, leading to restricted nutritional intake and poor QoL or severe psychological comorbidities. 35 The Inflammatory Bowel Disease Disability Index (IBD-DI) was recently developed in IBD populations to provide a patient-reported outcome measure to assess functional impairment and disease burden in patients with IBD. It found that disability scores, as measured by the IBD-DI, were closely correlated with depression and anxiety. Moreover, it discussed the broader psychosocial impact of IBD, including the effects on social functioning and QoL, finding that depression and anxiety can exacerbate these impacts, leading to further disability in various life domains. 32 While the IBD-DI is a valid and reliable measure of disability in IBD populations, the clinical application of the IBD-DI is complex and time-consuming, requiring the assistance of trained nurses. As such, the IBD Connect group developed the IBD-disk, a visual self-management tool for measuring disability in patients with IBD. It assesses 10 dimensions of disability with 10 items, including joint pain, abdominal pain, bowel regulation, interpersonal relationships, education and work, sleep, energy, mood, body image, and sexual function. It provides more information than a simple one-dimensional score and is easy to use from both the patient’s and healthcare professional’s perspectives. The benefits of this tool may aid in remote monitoring, especially in the era of COVID-19. 36
In addition, general physical activity (PA) is recognized for its positive impact on disease outcomes and QoL in patients with IBD, with the potential to improve mood and reduce anxiety due to the release of endorphins during exercise. However, challenges such as chronic pain, fatigue, fear of symptom exacerbation, and the lack of clear guidelines on safe exercise regimens often result in physical inactivity among patients with IBD. A study from Southern Italy using the International Physical Activity Questionnaire found a significant proportion (42.9%) of patients with IBD to be physically inactive, whereas patients with CD in remission who engage in regular PA have been shown to achieve better disease activity scores compared to those who are less active. 37 Furthermore, decreased muscle and increased adiposity are common in IBD, potentially caused by chronic inflammation, malnutrition, and reduced PA, and are associated with adverse outcomes. Moderate-intensity aerobic exercise combined with resistance training can help reduce adiposity and improve cardiovascular health in patients with IBD. Even mild PA can have beneficial effects on body composition and QoL. 38 Social support provided by group exercises or sports activities can significantly enhance psychological well-being in patients with IBD, fostering a sense of community and belonging. Moderate and consistent PA can modulate inflammatory markers in IBD, suggesting a potential anti-inflammatory effect of exercise. Moreover, a single session of moderate-intensity exercise in a healthy individual can activate the β-2 adrenergic pathway, which in turn inhibits the production of tumor necrosis factor (TNF) within monocytes. This mechanism can help prevent diseases associated with low-grade inflammation. 39 Exercise-induced changes in the microbiome may also contribute to its beneficial effects in the treatment and prevention of IBD. Various forms of exercise, including walking, running, swimming, and yoga, have significant stress-relieving effects, which can alleviate symptoms of anxiety and improve QoL, thus playing a role in prolonging the disease remission of patients with IBD. 40 A recent review by the European Crohn’s and Colitis Organisation identified PA as having potential beneficial effects on overall health, physical fitness, perceived stress, and QoL in IBD participants. 41 Low-to-moderate PA programs have been studied and found to be safe, while the benefits of high-intensity PA are less clear due to potential short-term exacerbation of IBD symptoms. As such, walking and gardening are the most common forms of PA among patients with IBD. Although no adverse reactions have been reported in limited data on high-intensity PA, non-adherence is often observed in high-intensity activities. 42 These evidence suggest that PA plays a crucial role in improving both the physical and psychological aspects of health in patients with IBD. We advocate for the inclusion of PA in the management of IBD, emphasizing the bidirectional relationship between PA and IBD.
Bidirectional aggravation mechanisms between psychological comorbidity and IBD
IBD is a multifaceted condition characterized by the interplay of environmental and genetic factors, culminating in immune dysregulation and intestinal inflammation. 43 The above reference proofs have highlighted the bidirectional relationship between psychological comorbidities—such as depression, anxiety, and mood disorders—and IBD, which exacerbate each other. 44 These reciprocal interactions are thought to be linked to intricate mechanisms within the immune and nervous systems. 45 Research suggests that depression—a psychological state marked by immune activation and cytokine release—may modulate the risk of immune-mediated diseases through its impact on the hypothalamic-pituitary-adrenal (HPA) axis, the autonomic nervous system (ANS), systemic inflammatory cytokines, or immune cell functionality. 46 For instance, in a dextran sulfate sodium colitis mouse model, depression induced by olfactory bulbectomy or intracerebroventricular lipopolysaccharide injection was correlated with the reactivation of inflammation in mice with previously quiescent chronic inflammation. This phenomenon is partially mediated by an upsurge in pro-inflammatory cytokines, such as interleukin (IL)-6 and IL-1β, secreted by macrophages. 47 Further studies have identified that the generation and dissemination of peripheral pro-inflammatory cytokines in IBD, including TNF (TNF-α), IL (IL-1β and IL-6), which can stimulate receptors on the vagal nerve, thereby altering central neurotransmitter release and behavior. 48 For example, brain regions densely populated with pro-inflammatory cytokine receptors, particularly those for IL-1β, IL-6, and TNF-α, encompass the hypothalamus, hippocampus, and cortex, which are pivotal for antidepressant efficacy and cognitive performance. The etiology of depression and its associated symptoms, such as anorexia, sleep disturbances, fatigue, and cognitive impairment, have been linked to pro-inflammatory cytokines (e.g. IL-1β, TNF-α, and IL-6). 49 The heightened intestinal inflammation and dysfunction of the gut enteric nervous system (ENS) in IBD can lead to increased intestinal permeability, which allows for the translocation of intestinal pro-inflammatory cytokines into the bloodstream, crossing the blood-brain barrier (BBB) and causing depression associated psychological conditions.50,51 Notably, in clinical practice, cytokine antagonist therapies, such as anti-TNF treatments in patients with IBD, have demonstrated efficacy in mitigating disease-associated depressive behaviors. 52 Depression is frequently linked to the activation of the HPA axis and subsequent elevations in circulating cortisol levels. Chronic activation of the HPA axis, as observed in persistent stress or inflammation, such as that seen in IBD, leads to sustained cortisol elevation. This condition results in a diminished sensitivity of glucocorticoid receptors, which in turn amplifies immune responses and intensifies inflammation, potentially precipitating the manifestation of clinically apparent IBD in predisposed individuals. 53 Moreover, other psychological conditions, such as early life stress, along with ongoing stress, may contribute to an individual’s vulnerability to psychiatric disorders, including depression, thus playing adverse effects on IBD through various mechanisms, such as activation of mast cells, stimulation of the sympathetic nervous system, inhibition of the vagus nerve, interactions between the prefrontal-amygdala complex and the immune system, downregulation of the hypothalamic corticotropin-releasing factor (CRF) system, involvement of the peripheral CRF system in inflammatory responses, modulation by the gut microbiota-gut-brain axis (MGBx), early-life events influencing colitis, and the direct impact of depression on colitis. 45 Life events and chronic stress are also recognized as factors that increase the risk of relapse in IBD. In patients with UC, rectal mucosal stress augments cytokine production (IL-6 and IL-13) upon lipopolysaccharide stimulation, with the inflammatory response correlating with psychometric assessments of chronic perceived stress levels among participants. 54 Norepinephrine (NE) tissue levels in both noninflamed and inflamed colonic mucosa from patients with CD are significantly lower than those in control subjects. In inflamed mucosa, levels of L-DOPA are twice as high as in noninflamed tissue, while dopamine (DA) and serotonin (5-HT) levels are markedly reduced compared to controls. Similar, though not identical, findings have been reported in UC. Tissue ratios of DA/L-DOPA and 5-HT/L-5HTP decrease in both CD and UC patients, suggesting that the inflammatory process may be influenced by neural factors. The intestinal cellular structures responsible for the synthesis and storage of DA, NE, and 5-HT may be compromised by the inflammation associated with IBD. 55 These neurotransmitters are also targets for anxiolytic and antidepressant medications. Research has revealed significantly diminished blood oxygen level-dependent signals in the amygdala, thalamus, and cerebellum in resting UC patients in response to positive emotional stimuli, indicating disrupted emotional processing circuits in these individuals. 56 The gut-brain axis is a complex bidirectional communication system that encompasses the central nervous system, ANS, ENS, HPA axis, and the gut microbiota. 57 Stress exposure activates sympathetic spinal nerves, leading to the release of NE into the gastrointestinal tract. This release enhances bacterial quorum sensing and iron uptake, increasing the virulence and proliferation of pathogenic bacteria such as Escherichia coli and Campylobacter.58,59 Emerging research underscores the influence of the gut microbiome and its metabolites, including neurotransmitters and bile acids, on behaviors associated with depression, anxiety, and stress responses.60,61 The gut microbiota synthesizes a spectrum of neurotransmitters, such as DA, NE, 5-HT, and gamma-aminobutyric acid (GABA), which modulate the activity of the ENS and, by extension, affect the MGBx. 62 Elevated serum bile acid levels may increase the permeability of the BBB, potentially leading to neuropsychological disturbances.63,64 Certain bile acids, like lithocholic acid, activate central pregnane X receptors and vitamin D receptors, both of which are associated with antidepressant effects.65,66 Notably, the concentration of 7-dehydrocholesterol is significantly higher in the serum of patients with CD and psychological disorders. 67 Additionally, bile acids can inhibit the transcription of brain-derived neurotrophic factor through the negative regulation of the transcription factor cAMP response element-binding protein via farnesoid X receptor signaling, thus may lead to various neurological and psychiatric conditions such as depression, Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, etc.68,69 Collectively, the bidirectional aggravation mechanisms between psychological comorbidity and IBD are complex and multidimensional, which involve various immune- and nervous-system-mediated mechanisms (Figure 2). The clinical value derived from understanding the bidirectional aggravation mechanisms between psychological comorbidities and IBD is multifaceted and crucial for comprehensive patient care, which allows for the development of more holistic therapeutic strategies that address both the physical and psychological aspects of the diseases, leading to effective treatments and improved patient outcomes.
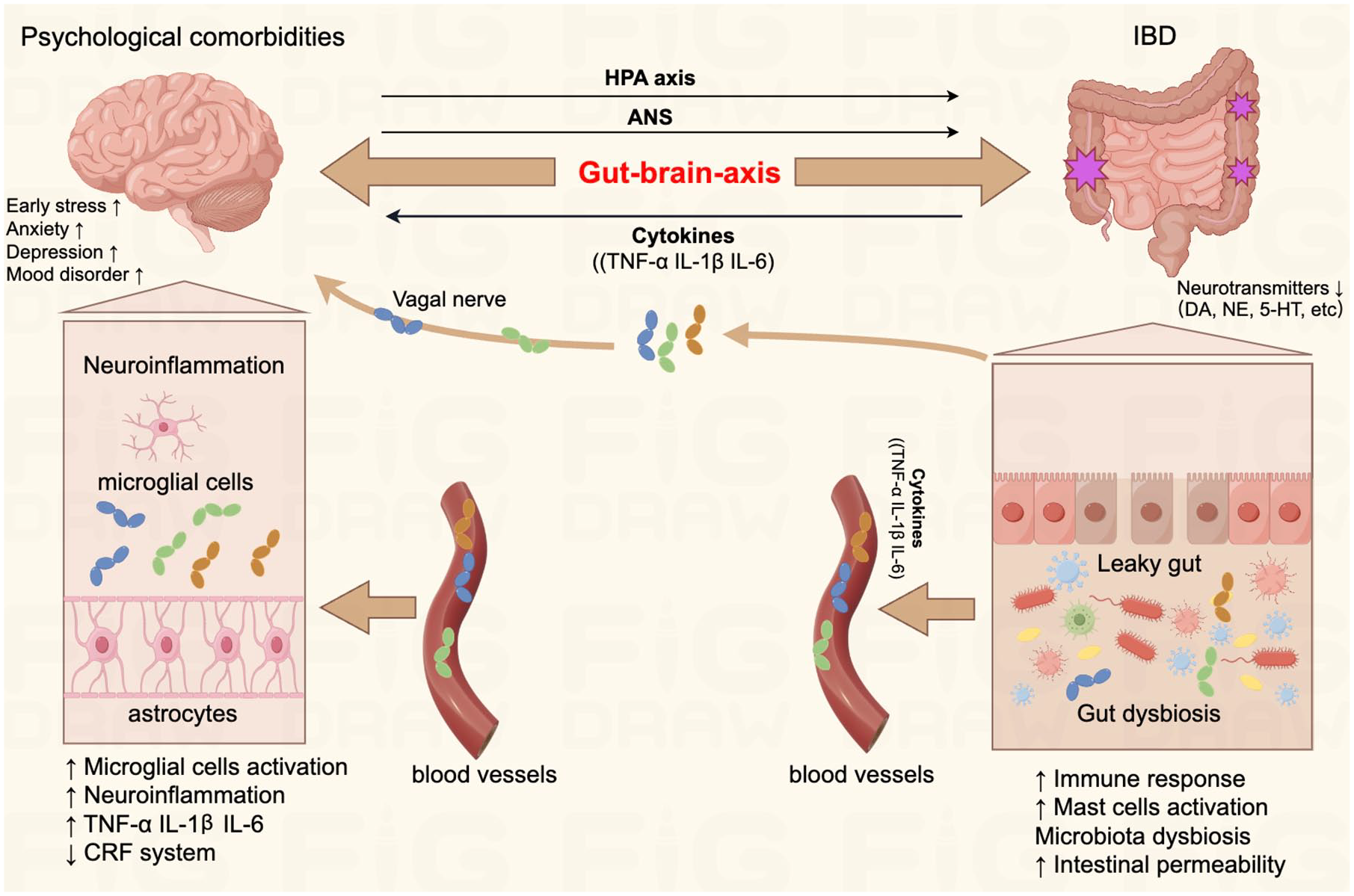
Bidirectional aggravation mechanisms between psychological comorbidity and IBD.
Impact of psychological comorbidities and their treatment measures on the prevention, treatment outcomes, and prognosis of IBD
The interplay between psychological comorbidities and their therapeutic interventions significantly influences the prevention, management outcomes, and prognosis of IBD. Depression is frequently correlated with suboptimal treatment adherence among patients with IBD, suggesting an additional mechanism by which depression may aggravate the disease. 70 Anti-TNF therapy is the cornerstone of treatment for severe IBD cases, with infliximab being the preferred first-line agent. 71 A prospective study of 100 consecutive CD patients underwent blinded psychological evaluations at the commencement and at 4 weeks into infliximab monotherapy. The presence of major depressive disorder was assessed by the self-administered PHQ-9. Subsequent follow-up for 9 months or until retreatment for disease recurrence revealed that baseline major depression was associated with higher mean Crohn’s Disease Activity Index (CDAI) scores and necessitated retreatment, identifying major depression as a predictor of infliximab treatment failure. Moreover, a significant link was found between major depression and a reduced interval to retreatment, indicating a need for earlier intervention 72 (Table 1). Additionally, patients with IBD and comorbid anxiety and mood disorders (AMDs) bear a more substantial symptom burden and are prone to extraintestinal manifestations like fatigue. An analysis of a Canadian database from 2001 to 2016, which included 1135 patients with IBD receiving anti-TNF therapy, showed that 15.7% had concurrent AMDs. These patients demonstrated a notably higher discontinuation rate of anti-TNF therapy within the first year compared to those without such comorbidities. The reasons for cessation are multifaceted; they may include medication noncompliance, an increased frequency of adverse drug reactions, or misinterpretation of severe gastrointestinal symptoms as treatment ineffectiveness when the inflammatory burden is not substantial. AMDs may also contribute to an inadequate response to biologic therapies 73 (Table 1). Furthermore, depression can have grave repercussions, such as elevated suicide rates among patients with IBD, 33 and may lead to an increased number of medical investigations, thereby posing a risk factor for radiation exposure in this population. 74 Data from a large, prospective, multicenter cohort across seven US academic centers highlighted a significant correlation between baseline depression and an increased risk of invasive IBD procedures during the follow-up period. In the context of IBD, patients presenting with baseline depression were observed to have a higher frequency of relapses, earlier initiation of biologics and steroids, more frequent hospitalizations, and a propensity for sooner surgical interventions compared to their non-depressed counterparts. Those with moderate to severe depression, as indicated by a PHQ-8 score of 10 or higher, were at an increased risk for the development of aggressive CD phenotypes. 75 Active disease at baseline was also strongly associated with a higher incidence of comorbid depression relative to patients in remission. 75 A retrospective cohort study utilizing the UK-based electronic medical record database, The Health Improvement Network, spanning from 1986 to 2012, identified 403,665 patients (7.05%) with depression. The study monitored these individuals and a control group until the initial diagnosis of CD or UC was made. The findings suggest that individuals with depression have a heightened risk of developing CD and UC. Notably, the use of antidepressants during the treatment of depression appeared to reduce the risk of IBD onset, while the risk of developing UC remained consistent between antidepressant users and non-users within the control group. 55 This indicates that antidepressants may mitigate inflammation associated with depression and, consequently, influence peripheral inflammation in IBD, potentially improving prognosis by controlling somatic symptoms and exerting anti-inflammatory effects 55 (Table 1). Selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants (TCAs) have been identified as preventive for CD, while mirtazapine, serotonin-norepinephrine reuptake inhibitors, SSRIs, serotonin modulators, and TCAs may prevent UC. 11 These findings point to differential neurotransmitter responses in CD and UC, which may be related to variations in mucosal immunity and barrier functions between these two diseases. 46 Antidepressant usage in patients with IBD has been associated with improvements in psychological comorbidities, significantly related to improvements in depression, anxiety, QoL, sexual functioning scores, and hemoglobin levels over a 6-month period, alongside a trend towards reduced CDAI and Mayo scores. 7 Furthermore, psychological therapy for comorbid depression in pediatric patients with IBD has been linked to decreased gastrointestinal healthcare costs. 76 Antidepressant treatment has also been shown to lower disease relapse rates, reduce corticosteroid use, and decrease the need for endoscopic examinations in patients with IBD and psychological comorbidities. 77 A UK-based study revealed that among patients with IBD commencing antidepressant therapy, sertraline was the most commonly prescribed medication. However, 67% of these patients had treatment durations that fell below the internationally recommended adequate treatment duration, with 34% receiving only a single prescription during their initial treatment phase, suggesting a treatment period of 28 days or less. This pattern of antidepressant treatment may be insufficient and could potentially increase the risk of disease recurrence in patients with IBD and psychological comorbidities. 78 These previous clinical studies suggest that the impact of psychological comorbidities on the prevention, treatment outcomes, and prognosis of IBD is substantial and cannot be overlooked in future clinical practice (Table 1). Early identification and effective management of psychological conditions, alongside appropriate pharmacological and psychological interventions, are essential components of a comprehensive IBD management strategy. Future research should focus on optimizing treatment durations, exploring the mechanisms underlying the differential effects of antidepressants on CD and UC, and developing personalized interventions to improve the overall health and well-being of patients with IBD and psychological comorbidities.
Primary studies on the impact of psychological comorbidities and their treatment measures on the prevention, treatment outcomes, and prognosis of IBD.

AMD, anxiety and mood disorder; ASEX, Arizona Sexual Experience Scale; CD, Crohn’s disease; CDAI, Crohn’s Disease Activity Index; CDI-C, Children’s Depression Inventory-Child; CDI-P, Children’s Depression Inventory-Parent; CDRS-R, Children’s Depression Rating Scale-Revised; DSM-IV-TR, Diagnostic and Statistical Manual of Mental Disorders-4th Edition-Text Revision; GDS, geriatric depression scale; HADS, Hospital Anxiety and Depression Scale; IBD, inflammatory bowel disease; KSADS-PL, Kiddie-Schedule for Affective Disorders and Schizophrenia for Children-Present and Lifetime; PHQ-8, Patient Health Questionnaire-8; PHQ-9, Patient Health Questionnaire-9 items; QoL, quality of life; SCID-I, Structured Clinical Interview for DSM-IV Axis I Disorders; SF-36, Short Form-36 Health Survey; THIN, The Health Improvement Network; TNF, tumor necrosis factor; UC, ulcerative colitis.
IBD management from the perspective of psychological comorbidities
Integration of the evaluation and treatment of psychological comorbidities
In the management of IBD, the incorporation of biopsychosocial models is essential. A paradigm shift is required in patient care, transitioning from an exclusive emphasis on inflammatory pathology to a holistic treatment strategy. 79 The evaluation and treatment of psychological comorbidities are integral to IBD patient care, especially considering the elevated suicide rates among this population compared to control groups. 33 Thus, proper screening for depression is not only vital for preventing disease exacerbation but may also be life-saving. Despite the critical nature of these assessments, current access to psychological and psychiatric support within adult IBD units in the United Kingdom is markedly inadequate, with only 2% meeting the recommended standards. 80 Surveys indicate that mental and emotional health is infrequently addressed during clinical consultations, with only a quarter of patients with IBD being queried on these aspects. 81 There is a recommendation to increase vigilance for IBD in patients with depression and gastrointestinal symptoms and to consider early antidepressant intervention to potentially delay or prevent the onset and progression of IBD. 11 The HADS or PHQ-9 can routinely be utilized as our primary self-report measure for assessing depression. They are widely recognized and validated instruments that have been extensively used in IBD research, demonstrated to possess high specificity in the context of IBD.15–17 Patients with IBD routinely contend with stress, pain, fatigue, and control issues, 82 with stress and distress significantly contributing to the development of depressive and anxiety disorders, highlighting the importance of stress management in therapeutic regimens. 83 The onset of AMDs may parallel the progression of IBD, underscoring the need for heightened awareness and support from IBD specialists, including the provision of psychological and pharmacological interventions. These measures aim to improve long-term outcomes, enhance QoL, and reduce the healthcare and societal costs associated with IBD management. Notably, young individuals diagnosed with IBD between the ages of 18–24 are more likely to prematurely discontinue antidepressant therapy compared to those diagnosed between 40 and 60 years of age. 78 This trend is more pronounced among patients from economically disadvantaged backgrounds. Given that the typical onset age for IBD is between 15 and 40 years, and young individuals frequently move for education or employment, resulting in inconsistent healthcare follow-up, special attention to this demographic is imperative to ensure continuity of care and treatment adherence. 78
Emerging research indicates that while psychological therapy alone may have a limited effect on anxiety, depression, QoL, and disease progression in patients with IBD, it has shown potential in reducing pain, fatigue, and the frequency of relapses and hospitalizations, as well as improving medication adherence, suggesting a cost-effective approach. 84 The placebo effect in IBD treatment underscores the importance of patient perception and cognitive experience in the regulation of the disease and clinical outcomes. Advancements in the understanding of the brain-gut axis through animal models provide valuable insights for the management of IBD in humans. 44 The exploration of alternative psychological interventions, serving as adjuncts or substitutes to conventional IBD treatments, is encouraged. Future research directions include investigating biomarkers of brain-gut interactions, such as those related to the HPA axis, sympathetic-vagal balance, and brain imaging studies. In the context of the brain-gut hypothesis, it is imperative to explore adjunctive therapies to standard anti-TNF treatments, focusing on the gut microbiota and their metabolites. Practices such as compassion meditation have been shown to attenuate the inflammatory response (IL-6) to psychosocial stress in laboratory settings. Short-term meditation practices have been associated with increased heart rate variability and decreased skin conductance, indicative of enhanced parasympathetic nervous system activity. Similarly, Tai Chi and yoga have been reported to modulate social network activity and augment parasympathetic drive, respectively. A positive correlation has been observed between hypnotic susceptibility and autonomic nervous responses, with highly hypnotizable individuals exhibiting increased vagal efferent activity. 45 Repetitive transcranial magnetic stimulation, which enhances the cholinergic anti-inflammatory pathway, has piqued interest, although evidence of its efficacy in IBD treatment remains limited. Both electroacupuncture and fluoxetine treatments have demonstrated anti-inflammatory effects, as evidenced by reductions in IL-1β levels, with electroacupuncture also affecting TNF-α and IL-4 levels. 85 These modalities may serve as complementary or alternative options to traditional IBD therapies in the future.
The utilization of behavior-based approaches
A thorough investigation into the effects of antidepressant medication and behavioral therapy on IBD, particularly their impact on disease-specific outcomes, is essential. In the realm of IBD management, a variety of behavior-based approaches are employed to address both the physical and psychological aspects of the condition. 86 These approaches could be classified into two categories, that is, behavioral therapies and self-management behaviors.87,88 As for behavioral therapies, Cognitive Behavioral Therapy (CBT), Acceptance and Commitment Therapy (ACT), and Gut-Directed Hypnosis are the most frequently adopted. CBT is a structured psychological intervention that assists individuals in identifying and modifying negative thought patterns and behaviors, successfully employed in treating adolescents with IBD and depression, and as a method to enhance self-management behaviors in patients with CD. CBT focuses on identifying and changing unhelpful thoughts and/or behaviors to improve symptoms, emotions, and life functioning. It is a multi-component treatment that includes psychoeducation about the bidirectional role of stress in gastrointestinal diseases and the brain-gut axis, relaxation training, cognitive restructuring, coping skills training, and exposure techniques 89 ; ACT complements this by focusing on psychological flexibility and mindfulness, encouraging patients to accept their current circumstances and commit to actions that align with their values, thereby enhancing their QoL despite the challenges of IBD. Unlike CBT, ACT does not aim to eliminate or change negative thoughts or feelings but encourages individuals to accept their existence90,91; Gut-directed hypnosis is another method used to treat a range of gastrointestinal disorders in children and adults. Hypnotherapy targets visceral hypersensitivity, motility disorders, hypervigilance to benign sensations, and somatization. It is a treatment form that relies on a special state of mental focus, induced through the therapist’s verbal guidance to facilitate the receptivity of therapeutic suggestions. 92 While both CBT and hypnotherapy have been established as primary psychotherapies in gastrointestinal treatments, they have been hindered by limited scalability and high costs. The evidence from randomized controlled trials suggests that CBT is more effective than hypnosis. However, there is a lack of comparative efficacy trials that pit these therapies against each other or against psychopharmacological interventions. 93
In contrast to these professional behavioral therapies, self-management behaviors encompass a broader spectrum of actions that individuals can take to actively monitor and control their diseases. These behaviors include medication adherence, dietary adjustments, regular exercise, stress reduction, and maintaining overall health, all of which are tailored to the patient’s specific needs and circumstances. Self-management is essential for maintaining remission, preventing flare-ups, and ensuring better disease outcomes.94,95 While CBT and ACT address cognitive and emotional processes, and gut-directed hypnosis targets the mind-gut connection, self-management focuses on the practical, everyday behaviors that influence health. However, the most effective IBD management strategies often integrate medical treatments with both professional therapies and self-management, creating a comprehensive and personalized approach to care. It is crucial for healthcare providers to recognize the value of each approach and to work with patients to develop a treatment plan that suits their individual needs, preferences, and responses to treatment.
Although behavioral therapies are useful and effective in the management of IBD, some patients cannot get these therapies from their healthcare providers. Consequently, digital tools are needed to make them accesses, which would facilitate communication between patients and healthcare providers and offer remote tracking and monitoring for patients to understand their conditions, and address their questions. Patients who utilize digital interventions may feel more secure about their health, be more engaged in their care plans, and feel better cared for outside of the hospital setting. For example, a digital health program launched in Finland in May 2020 for patients with IBD has demonstrated promising results. 96 This intervention increases the frequency of health behaviors through goal setting, self-monitoring, and the gamification of health-related tasks, encompassing categories such as nutrition, PA, stress management, and psychological education. Patients receive weekly automated messages and personalized daily tasks to complete certain tasks within the platform, such as PA, practicing mindfulness and meditation, watching educational videos, and assessing their sleep quality, stress, and energy levels. A dedicated IBD nurse monitors patient activities and sends weekly feedback and motivational messages. Statistically significant improvements in stress reduction and energy levels were observed from baseline to the end of treatment among completers.
Moreover, digital tools would help the patients’ get access to what they consider the most reliable sources of health information. Patients express a desire for a digital tool that provides up-to-date, reliable, and practical health and social service information related to IBD self-management. High-quality digital health information can promote treatment adherence and self-management in patients with IBD. 97 In summary, digital health tools offer a significant opportunity to enhance patient engagement with behavioral therapies and self-management strategies in IBD. By leveraging these technologies, healthcare providers can better support patients in managing their condition, improving adherence to treatment, and ultimately enhancing their QoL.
There is an anticipation that these methods mentioned above may develop into new standards of care for IBD treatment. As such, the management of IBD must evolve to encompass a comprehensive approach that acknowledges the significant impact of psychological comorbidities on patient outcomes. The integration of the psychological assessment is paramount and should be systematically implemented as a routine part of clinical assessments for IBD treatment (Figure 3). Such a comprehensive multidisciplinary management process that includes gastroenterologists, psychologists, and nutritionists will ensure that patients with IBD receive the most effective and personalized care possible.

The suggested multidisciplinary-integrated IBD management process.
Conclusion and future prospects
In conclusion, this review revealed that the intricate relationship between inflammatory IBD and psychological comorbidities, such as anxiety and depression, is increasingly recognized as a critical factor in the comprehensive management of IBD. The bidirectional nature of this relationship suggests that psychological disturbances not only exacerbate IBD symptoms but may also contribute to the onset and progression of the disease. This understanding underscores the necessity for a paradigm shift in clinical practice, moving towards a multidisciplinary-integrated management process that addresses both the physical and psychological aspects of IBD.
The impact of psychological comorbidities on the prevention, treatment outcomes, and prognosis of IBD is substantial. Depression has been linked to suboptimal treatment adherence, higher disease activity, and an increased risk of treatment failure, particularly in patients undergoing anti-TNF therapy. Moreover, the presence of AMDs in patients with IBD leads to a more significant symptom burden and a higher likelihood of extraintestinal manifestations. These findings highlight the importance of early identification and effective management of psychological conditions as part of a holistic IBD treatment strategy. Additionally, it is imperative for IBD specialists to routinely assess the mental health of their patients alongside biological treatment considerations, managing stress, and providing appropriate interventions as needed.
The prospects of IBD management from the perspective of psychological comorbidities involve several key areas. Firstly, there is a need to improve access to psychological and psychiatric support within IBD care settings, ensuring that all patients receive the necessary attention to their mental health. Secondly, the development and implementation of routine screening tools, such as the PHQ-9 and HADS, can help identify patients at risk and facilitate timely interventions. Furthermore, the exploration of alternative and complementary psychological interventions, such as general PA, meditation, Tai Chi, and yoga, holds promise as adjunctive therapies to conventional treatments. These practices may help modulate the gut-brain axis and improve both psychological well-being and IBD disease outcomes. Additionally, a thorough investigation into the effects of antidepressant medication and behavioral therapy on IBD is essential, with the potential to develop into new standards of care. Finally, developing digital tools provide a significant opportunity to enhance patient engagement with treatment effectively.
Collectively, the management of IBD must evolve to encompass a comprehensive approach that acknowledges the significant impact of psychological comorbidities on patient outcomes. The integration of psychological assessment and intervention should be systematically implemented as a routine part of clinical practice. By adopting such a multidisciplinary approach, healthcare providers can ensure that patients with IBD receive the most effective and personalized care possible, ultimately improving their QoL and long-term outcomes. Future research should continue to explore the mechanisms underlying the bidirectional relationship between IBD and psychological comorbidities and identify novel therapeutic strategies to further enhance patient care.