
Abstract
Background:
There is an increasing diversification in the treatment landscape for inflammatory bowel diseases (IBD) leading to therapeutic challenges that can only incompletely be covered by prospective randomized double-blind trials. Real-world observations are therefore an important tool to provide insights into therapeutic strategies.
Objectives:
To describe the real-world treatment algorithms in an IBD referral centre.
Design:
Single-centre retrospective cohort study.
Methods:
We retrospectively analysed prospectively collected data on treatment sequences and outcomes from 502 patients with Crohn’s disease (CD) and ulcerative colitis (UC) treated with infliximab, adalimumab, vedolizumab or ustekinumab at a large German tertiary referral centre.
Results:
Treatment decisions correlated to baseline patient characteristics. Over time, infliximab continued to be the preferred first-line option in CD and UC, although ustekinumab and vedolizumab, respectively, became increasingly important choices. Remission rates decreased with the advancement of therapy lines.
Conclusion:
We provide insights into the evolution of tertiary centre real-world treatment sequences that might – together with other observations – help to guide the selection of therapies in IBD. Our data also strongly underscore the unmet need for biomarkers supporting treatment decisions.
Trial registration:
None.
Keywords
Introduction
The treatment landscape in inflammatory bowel disease (IBD) is rapidly evolving. Since the approval of infliximab for Crohn’s disease (CD) around 25 years ago, numerous further therapeutic agents have been developed, evaluated in clinical trials and approved by regulatory authorities for the treatment of CD and/or ulcerative colitis (UC).1–4 Today, not only biologics such as anti-TNF, anti-integrin, anti-IL-12/23 and anti-IL-23 antibodies but also small molecules such as Jak inhibitors and sphingosine-1-phosphate receptor modulators are available.5–11
While this offers plenty of options for the treatment of patients with CD or UC, it also enhances the necessity to choose between these different classes and their representatives. 12 Only little data are available to guide such decisions since only a few head-to-head trials directly comparing specific compounds have been performed.13–15 Moreover, the heterogeneity of individual disease phenotypes, courses and previous treatments adds substantial further complexity to the picture and virtually precludes evidence-based therapeutic algorithms fitting to every patient.
At the same time, randomized trials have consistently demonstrated that pre-treated patients show lower rates of remission to a new drug than bio-naïve patients,5–7 which suggests that it is important to select the individually most effective drug right at the beginning and early in the disease course.
Therefore, in parallel to huge efforts to identify biomarkers that predict individual response to therapy,16–18 real-world observational studies are an important source of information that helps to assess the efficacy of various treatment options under more realistic conditions and in a specific clinical context. While numerous such studies have been conducted to address the clinical performance of a specific compound in pro- or retrospective cohorts, far fewer data are available on the real-world relative positioning of therapeutic substances in treatment algorithms as well as their context-dependent performance.
Thus, we here report a post hoc tertiary single-centre analysis of prospectively collected real-world data from a cohort of patients with IBD treated at a large German tertiary referral centre. Focussing on the biologics infliximab, adalimumab, vedolizumab and ustekinumab, we explore individual treatment trajectories and their historical trends as well as the outcomes of therapy depending on their positioning in the treatment algorithms. We show that, while the advent of novel therapeutic options has clearly changed the choice of drugs in the second and third line of therapy, infliximab continues to be the preferred first-line agent and that, indeed, remission rates for all compounds decrease in advanced therapy lines.
Hence, in addition to providing interesting insights into the evolution of tertiary centre real-world therapeutic algorithms, these data further support the notion that precision approaches for individually tailored therapy are urgently needed.
Methods
Patients
543 consecutive patients treated with infliximab, adalimumab, ustekinumab or vedolizumab for either CD or ulcerative colitis at the IBD outpatient clinic of the Department of Medicine 1, University Hospital Erlangen, between January 2018 and June 2022 were included into the study. Patients were identified with the help of the Clinic’s electronic booking system with an established diagnosis of either UC or CD and active treatment with one of the above-mentioned substances being the sole inclusion criteria. 41 patients whose data were previously reported in other real-world cohorts were excluded. The full electronic records of these patients were retrospectively reviewed to retrieve information on previous and ongoing treatments and their outcomes. The first, second and third lines of advanced therapy were defined as the first, second and third treatment with one of the above-mentioned biologics and not taking into account any previous conventional treatment. Patients treated with other compounds (e.g. golimumab, tofacitinib, filgotinib) were not included due to the substantially smaller cohort sizes.
Treatment was indicated as per the label at the discretion of the responsible physicians. Clinical information was retrieved from the electronic patient records including standardized and prospectively collected disease characteristics and assessment of disease activity.
The baseline clinical parameters of the patient cohort are summarized in Table 1 and refer to the initiation of first-line therapy.
Baseline characteristics at initiation of first-line therapy.
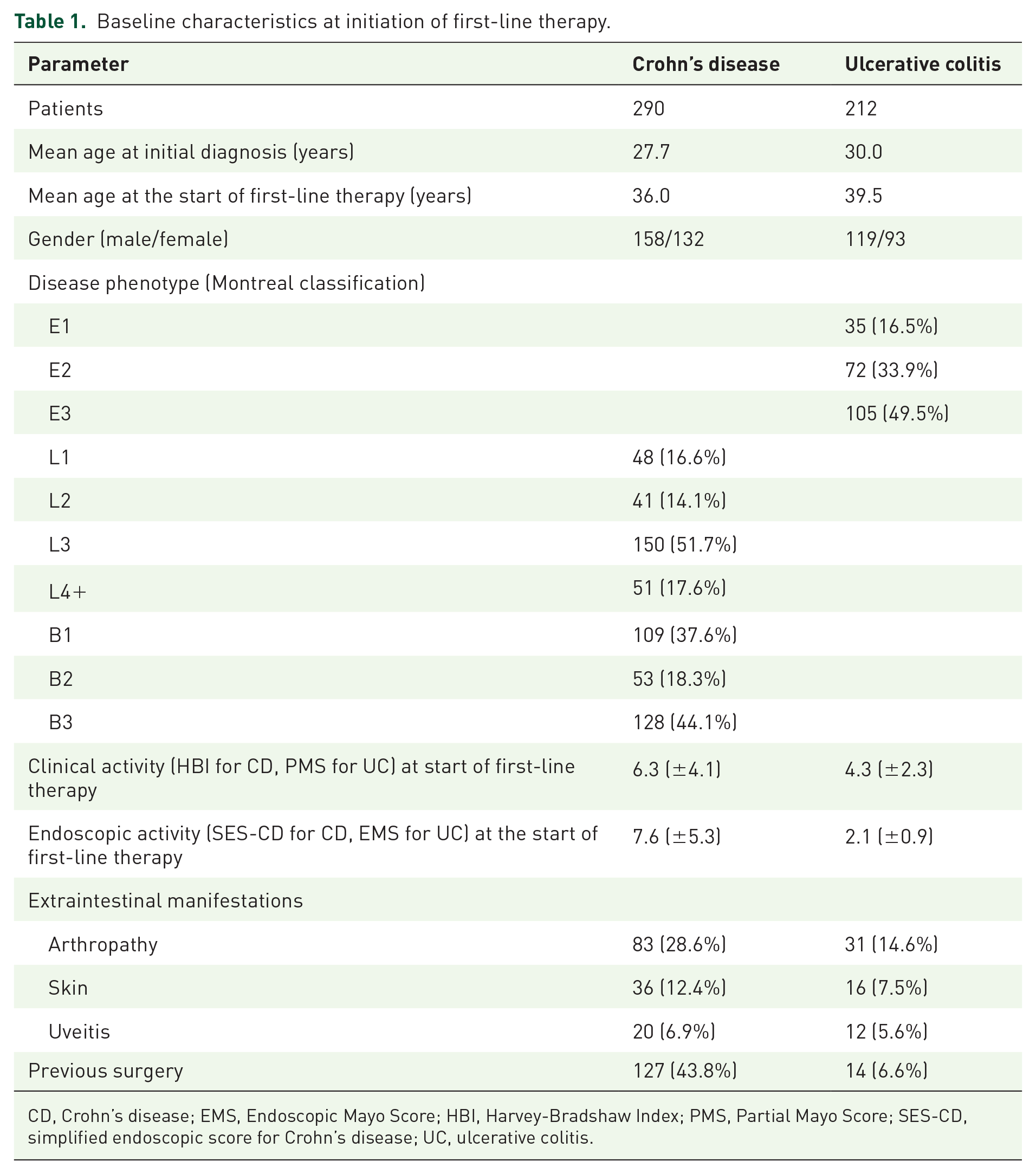
CD, Crohn’s disease; EMS, Endoscopic Mayo Score; HBI, Harvey-Bradshaw Index; PMS, Partial Mayo Score; SES-CD, simplified endoscopic score for Crohn’s disease; UC, ulcerative colitis.
Outcomes
Clinical remission was defined as a partial Mayo Score (PMS) below 2 points for UC and a Harvey-Bradshaw Index (HBI) below six points for CD and was determined at weeks 16 and 52. Steroid-free remission was defined as clinical remission without the intake of any corticosteroids and was determined at week 52. Endoscopic remission was defined as a Simple Endoscopic Score for Crohn’s disease (SES-CD) of less than three points for Crohn’s disease and an endoscopic Mayo Score (EMS) of less than 2 points for UC on the first follow-up endoscopy under treatment (week 35.2 ± 2.6 for UC, week 50.4 ± 2.8 for Crohn’s disease (mean ± SEM)). Biochemical remission was determined at week 52 and was determined as normal levels of C-reactive protein (<5 mg/L).
Statistical analysis
Statistical analyses were performed using Microsoft Excel and GraphPad Prism. Results are shown as mean (with standard error of the mean (SEM)), percentages, fractions or absolute numbers depending on the type of graph. Statistical comparisons were performed with Brown-Forsythe ANOVA and Dunnett’s T3 multiple comparisons test or Fisher’s exact test.
Ethics
The study was approved by the Ethics Committee of the Friedrich-Alexander-Universität Erlangen-Nürnberg (20-288-Br). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement 19 (Supplemental Material).
Results
Treatment trajectories in CD
In all, 290 patients with CD were included in the analysis and were followed up over a mean of 29.4 ± 1.2 months. The majority of them commenced advanced therapy with an anti-TNF antibody: 160 (55.2%) received infliximab as a first-line agent and 93 (32.1%) adalimumab. 31 (10.7%) and 6 (2.1%) patients were started on ustekinumab and vedolizumab, respectively, as their first biologic (Figure 1). Interestingly, there were obvious differences between these groups. This concerned disease phenotypes, but there was also a clear trend towards higher disease activity in patients starting with anti-TNF agents (Supplemental Table 1) suggesting that these aspects probably contributed to the choice of treatment. Surprisingly, no such differences were observed in the proportion of patients suffering from extraintestinal manifestations.

Real-world treatment sequences in Crohn’s disease. Flow chart of the real-world sequences of advanced treatments initiated with infliximab (a), adalimumab (b), vedolizumab (c) or ustekinumab (d) in patients with Crohn’s disease.
88 out of 160 patients (55.0%) starting on infliximab were switched to a second-line biologic during follow-up. Here, ustekinumab was the preferred choice (55.7%) followed by adalimumab (34.1%) and vedolizumab (10.2%). The predominant third-line treatment after second-line ustekinumab was adalimumab and ustekinumab after second-line adalimumab or vedolizumab (Figure 1(a)). Out of the 93 patients starting on adalimumab, 79 (84.9%) were switched to a second-line biologic, most often infliximab (49.4%) followed by ustekinumab (38.0%). In the third line, ustekinumab was preferentially used after infliximab and vedolizumab, whereas infliximab was most often selected following ustekinumab (Figure 1(b)). Only a few patients required a switch to second- or third-line therapy after first-line vedolizumab or ustekinumab (Figure 1(c) and (d)).
Since vedolizumab (2014) and ustekinumab (2016) were approved only shortly before our study period, we also wanted to address whether these treatment sequences changed over time. To this end, we analysed the percentages of patients receiving any of these antibodies in 2017 and earlier, in 2018 and 2019 as well as in 2020–2022 (Figure 2). Over this timeframe, infliximab was consistently the most used compound in first-line therapy and even increased its share over time. On the contrary, the use of adalimumab clearly declined, whereas the use of ustekinumab gradually increased from 3% to 32% and vedolizumab was only rarely used. In the second line, ustekinumab was the preferentially used agent from 2018 on along with the rarer use of infliximab and adalimumab. In the third line, ustekinumab was already frequently used in the 2017 and earlier period and continued to be the preferred choice later on. Here, vedolizumab was chosen in 37% of the patients in 2017 and earlier, but subsequently only used in 9% (2018/2019) and 13% (2020–2022) of the patients, while the use of infliximab increased over time.

Evolution of treatment choices in Crohn’s disease. Percentages of patients with Crohn’s disease assigned to treatment with infliximab, adalimumab, ustekinumab or vedolizumab stratified according to treatment line and according to treatment initiation 2017 and earlier (a), 2018/2019 (b) and 2020–2022 (c).
Collectively, these data showed that infliximab continued to be the first choice for the therapy of CD, while ustekinumab developed into the preferred second-line treatment shortly after approval mainly at the expense of adalimumab.
Efficacy of biologics in different treatment lines in CD
We further aimed to address whether the real-world efficacy of these biologics differed in different treatment lines and analysed clinical remission at week 52 (Figure 3), clinical remission at week 16 (Supplemental Figure 1), steroid-free remission at week 52 (Supplemental Figure 2), endoscopic remission (week 50.4 ± 2.8; Supplemental Figure 3) and biochemical remission at week 52 (Supplemental Figure 4). Although some exceptions occurred, the overall picture clearly showed that remission rates were highest in first-line therapy and gradually worsened in second- and third-line. This was particularly evident in patients who were treated ‘per protocol’ until these endpoints, but the same trend could also be observed in an ‘intention-to-treat’ approach, thus also including patients who had switched therapy before the respective time point. Despite some variations across the groups, there was no clear association of age, disease duration or sex with treatment outcomes (Supplemental Figure 5).
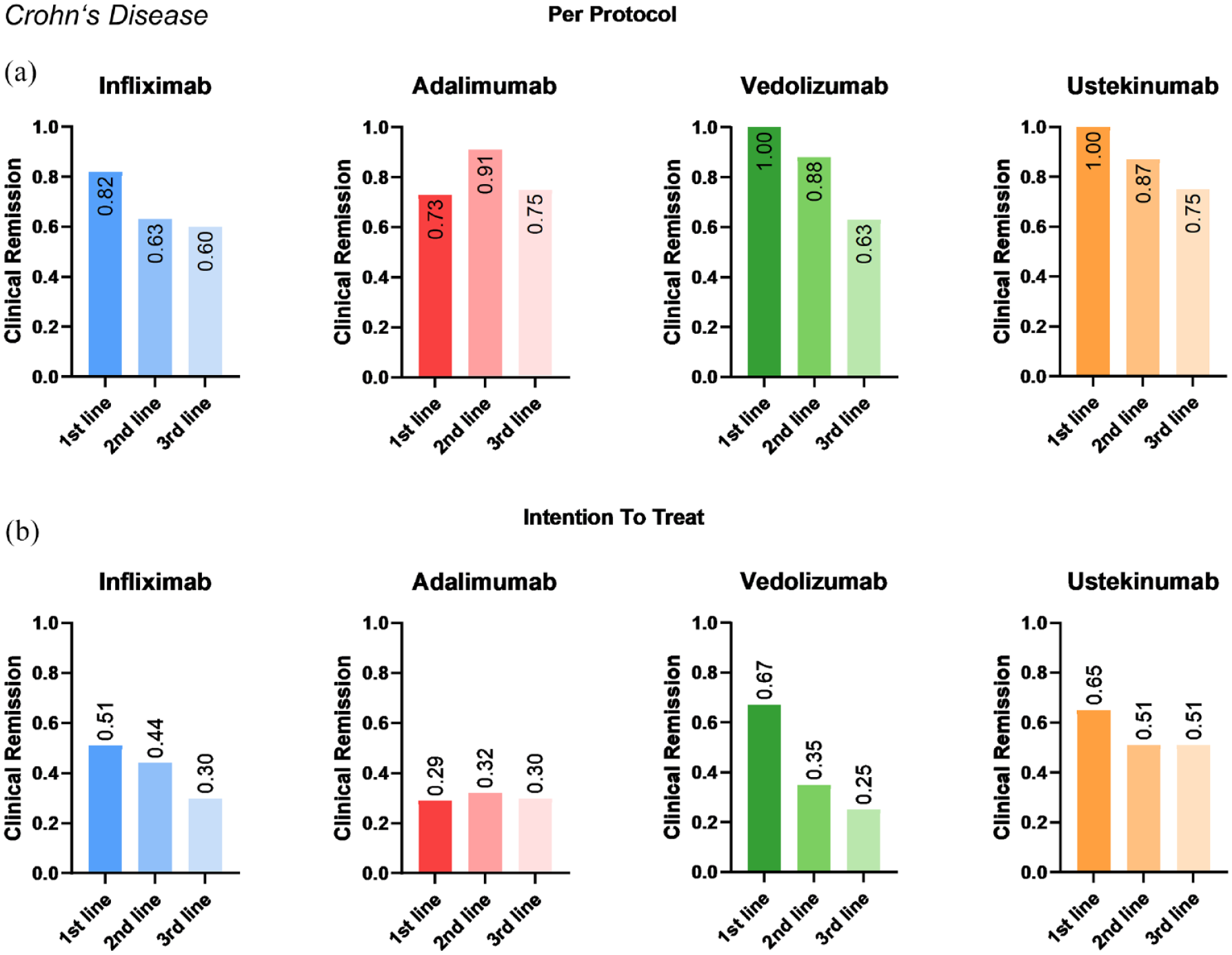
Real-world efficacy of biologic treatment in Crohn’s disease. Fractions of patients with Crohn’s disease achieving clinical remission at week 52 under treatment with infliximab, adalimumab, vedolizumab or ustekinumab stratified according to treatment line and depending on whether treatment was continued until week 52 (‘per protocol’, a) or not (‘intention to treat’, b).
Therefore, these data underscored that the selection of a highly effective therapy in early therapy lines seems particularly important.
Treatment trajectories in UC
In all, 212 patients with UC were included in the analysis and were followed up over a mean of 27.5 ± 4.2 months. The majority of them (125, 59.0%) received infliximab as their first advanced therapy. Vedolizumab was used in 45 patients (21.2%), adalimumab in 36 patients (17.0%) and ustekinumab in six patients (2.8%; Figure 4). Similar to CD, baseline characteristics of these patient groups differed apparently and patients starting on an anti-TNF agent had higher clinical and endoscopic disease activity (Supplemental Table 2), but not increased rates of extraintestinal manifestations. This suggested that disease activity but not extraintestinal manifestations were considered in the choice of treatment.

Real-world treatment sequences in ulcerative colitis. Flow chart of the real-world sequences of advanced treatments initiated with infliximab (a), adalimumab (b), vedolizumab (c) or ustekinumab (d) in patients with ulcerative colitis.
In total, 74 out of 125 patients (59.2%) starting on infliximab were switched to a second-line biologic during follow-up. In most cases, this was vedolizumab (44, 59.5%), followed by adalimumab (17, 23.0%) and ustekinumab (13, 17.6%). In the third line, ustekinumab and adalimumab were predominantly followed by vedolizumab, while adalimumab and ustekinumab were evenly used after vedolizumab (Figure 4(a)). Out of the 36 patients starting on adalimumab, 30 (83.3%) were switched to a second-line biologic, most often infliximab (66.7%) followed by vedolizumab and ustekinumab (both 16.7%). In the third line, vedolizumab was preferentially used after infliximab and infliximab after vedolizumab (Figure 4(b)). In all, 21 patients (46.7%) had to be switched to second-line treatment following first-line vedolizumab. Infliximab was chosen as second-line therapy in 71.4% and ustekinumab was the preferred choice in third-line therapy (Figure 4(c)).
To address, how dynamic this situation developed following the approval of vedolizumab (2014) and ustekinumab (2019), we additionally addressed changes in the treatment sequences over time (2017 and earlier, 2018/2019 and 2020–2022; Figure 5). Although with a small decrease, infliximab kept the pole position as the preferred therapeutic agent over this time course. However, the use of vedolizumab as a first-line agent substantially increased from 2018 on, mainly at the expense of adalimumab. In the second line, ustekinumab was used in around one-sixth and one-third of the patients in the 2018/2019 and 2020–2022 period, respectively, which went along with reductions in the use of vedolizumab and adalimumab. In the third line, ustekinumab was most frequently used right after its approval, whereas the use of vedolizumab in this therapy line substantially decreased.

Evolution of treatment choices in ulcerative colitis. Percentages of patients with ulcerative colitis assigned to treatment with infliximab, adalimumab, ustekinumab or vedolizumab stratified according to treatment line and according to treatment initiation 2017 and earlier (a), 2018/2019 (b) and 2020–2022 (c).
Altogether, it appears that infliximab remained the preferred first choice for the therapy of UC in this referral centre cohort, while there was an evolution towards the use of vedolizumab in the first or second and the use of ustekinumab in the second or third line.
Efficacy of biologics in different treatment lines in UC
Again, we also analysed the real-world efficacy of these biologics stratified according to the different lines of therapy and evaluated clinical remission at week 52 (Figure 6), clinical remission at week 16 (Supplemental Figure 6), steroid-free remission at week 52 (Supplemental Figure 7), endoscopic remission (week 35.2 ± 2.6, Supplemental Figure 8) and biochemical remission at week 52 (Supplemental Figure 9). Similar to CD, these analyses overall, although not in every constellation, demonstrated a reduction of response rates with the advancement of therapy lines in a ‘per protocol’ analysis, while no clear trends could be observed in the ‘intention-to-treat’ analysis. Although we observed some variations across the groups, there was no clear association of age, disease duration or sex with treatment outcomes (Supplemental Figure 10).
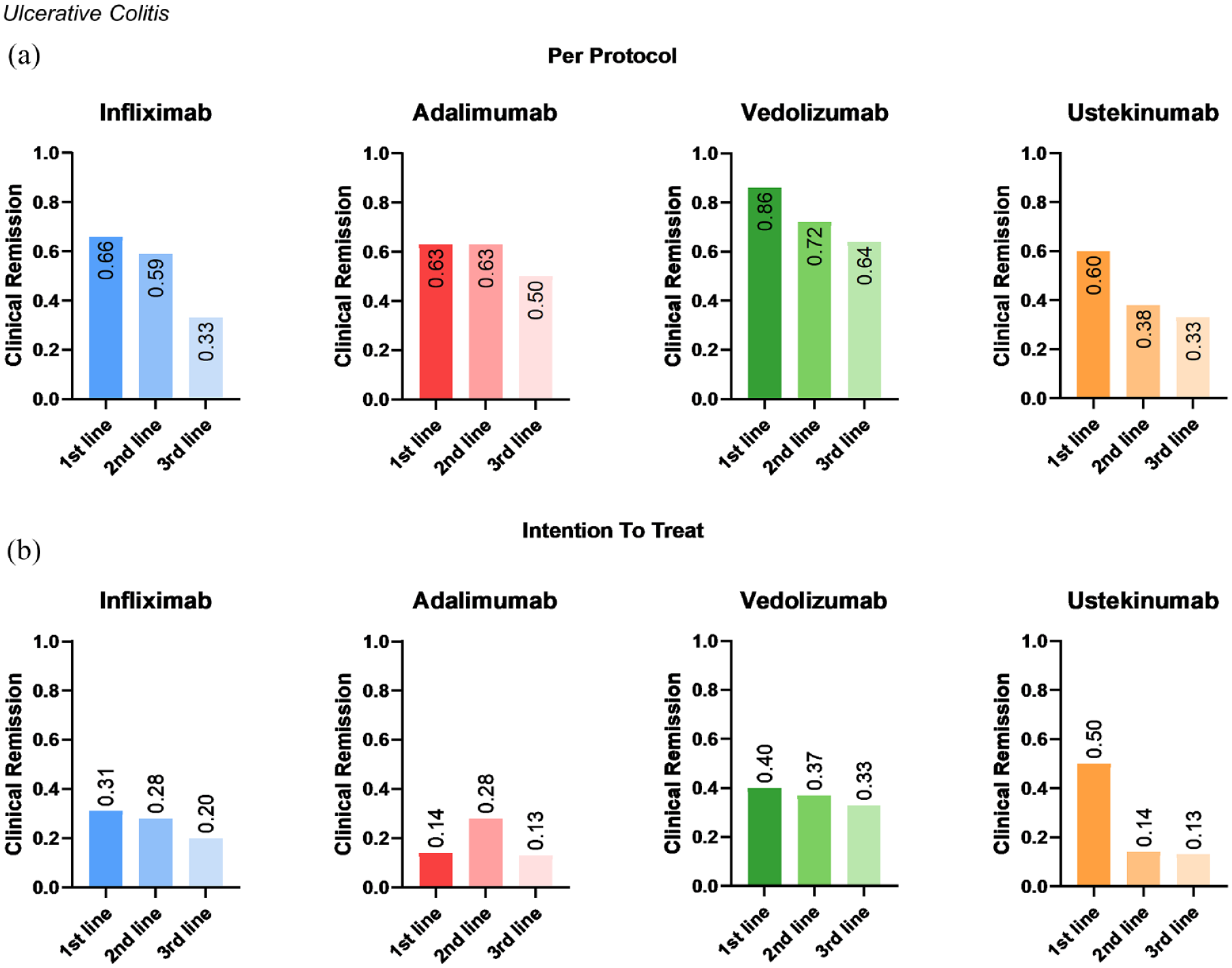
Real-world efficacy of biologic treatment in ulcerative colitis. Fractions of patients with ulcerative colitis achieving clinical remission at week 52 under treatment with infliximab, adalimumab, vedolizumab or ustekinumab stratified according to treatment line and depending on whether treatment was continued until week 52 (‘per protocol’, a) or not (‘intention to treat’, b).
Persistence on treatment
Finally, we aimed to answer the question of how long patients continued to be treated with these drugs. In both entities, persistence on treatment was worst with adalimumab and best with Ustekinumab (Figure 7). Persistence on vedolizumab in CD was similar to adalimumab over the first 20 months but then approached the curve of infliximab. In UC, persistence on vedolizumab and infliximab was similar over 50 months.
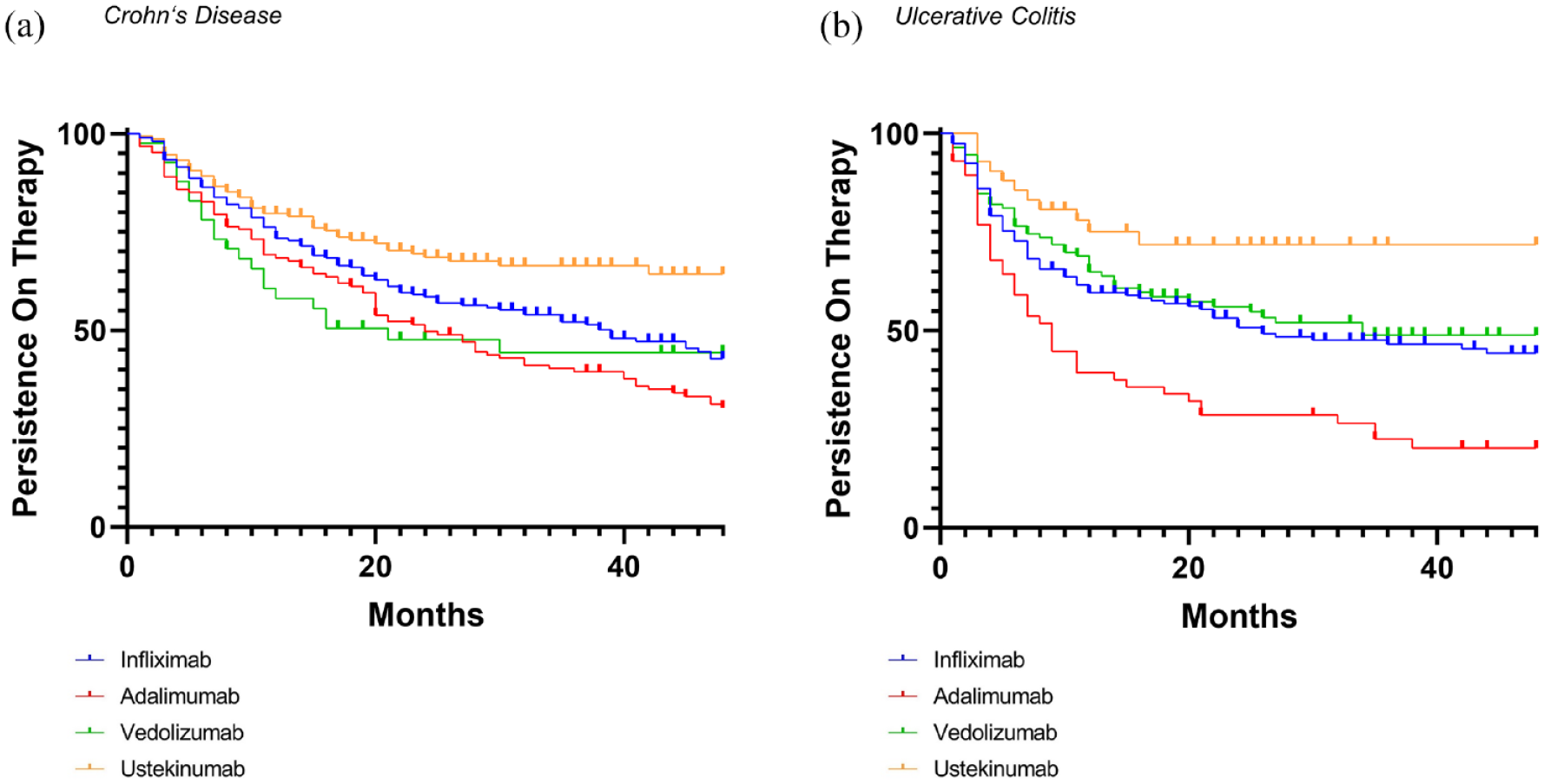
Persistence on therapy. Kaplan–Meier plots showing the persistence on therapy with infliximab, adalimumab, vedolizumab and ustekinumab in patients with Crohn’s disease (a) and ulcerative colitis (b).
Discussion
Treatment options for IBD are rapidly increasing and, thus, the question of which drug to use in which patient becomes more and more important. Only a few randomized head-to-head trials have been performed: The VARSITY trial compared vedolizumab versus adalimumab in UC and demonstrated the superiority of vedolizumab, 13 the SEAVUE trial compared ustekinumab and adalimumab in CD and showed similar efficacy 14 and data from the SEQUENCE trial in CD suggest that risankizumab is superior to ustekinumab. 15
Although these trials provided very important information for guiding treatment decisions, the pure amount of treatment options will make it impossible to generate comparative evidence for all potential choices. While network meta-analyses have tried to indirectly compare drugs used for IBD, 20 they cannot overcome the problem that data have been generated in different trials. Moreover, it emerges that the relative positioning of a drug in the treatment algorithm, that is in which line it is used and after which previous treatments, also seems to affect its efficacy, further enhancing the lack of high-quality evidence for individual therapeutic choices. Thus, in addition to criteria such as extraintestinal manifestations, co-morbidities or lifestyle, many drugs are currently selected based on the physicians’ and patients’ experiences and preferences.
One way to shed more light on these aspects is through real-world studies. Initially, such real-world studies in IBD mainly focussed on validating the results of randomized trials in more realistic patient cohorts.21–23 However, they have also been able to elucidate novel aspects that are difficult to address in randomized controlled trials such as comparative and sequential aspects, which have recently come into the focus of real-world reports.24–26 Here, we report the experiences made at a large tertiary IBD centre in southern Germany between 2018 and 2022. We show that vedolizumab (mainly in UC) and ustekinumab (more in CD than in UC) have been increasingly used over time, but have not been able to challenge the predominance of infliximab as the preferred first-line treatment for both indications, whereas the importance of adalimumab clearly decreased. Moreover, our data further support the concept that the odds of achieving remission decrease with the advancement of therapy lines and therefore strongly underscore the unmet need for appropriate patient stratification to enable the selection of the individually most effective treatment early in the disease course.
When interpreting these data, it is important to consider that they concern a cohort from a tertiary centre, where it is very likely that severe and more refractory cases accumulate and that the patient cohorts are therefore more likely to resemble clinical trial collectives than elsewhere. This might also explain the persisting predominance of infliximab in UC in this cohort, although other real-world investigations have shown that vedolizumab is now more frequently used. 27 Indeed, our data support the notion that the disease severity had an impact on the choice of therapy. It was also noteworthy that the fraction of patients achieving the remission endpoints was higher than in many of the pivotal trials adding to the recently emerging picture that real-world outcomes may be substantially better than in randomized trials. 28 Our data further show that the persistence on ustekinumab was longer than for the other drugs both in CD and UC, but this might be biased by the fact that ustekinumab was the last of the four agents to be introduced to the market and predominantly used in second- and third-line therapy. Thus, when interpreting the presented data, it is mandatory to take into account the historical availability of the drugs instead of drawing conclusions based on the current choice of options. Moreover, in general, it must be considered that persistence on treatment might not only be driven by disease activity but also by other factors.
Overall, our data are well in line with other real-world observations. In accordance with data from the ROTARY study, 24 adalimumab showed the least persistence on treatment in our cohort and, in accordance with a South Korean registry, 29 ustekinumab the highest persistence in CD. Superior persistence on ustekinumab in CD had also been reported in the Australian PANIC study, which yet described the highest persistence on vedolizumab in UC in contrast to our study. 30 Superior persistence on vedolizumab compared to anti-TNF antibodies was also found in a recent meta-analysis, highlighting that some variation exists between different cohorts. 31 Since vedolizumab is more likely to have a benefit in patients with lower disease activity, 32 the enrichment in refractory cases in our cohort might have contributed to this finding.
Similar to other cohorts, however, we observed unexpectedly high remission rates for first-line vedolizumab that were nominally higher than with the other biologics. 33 Although, for a single-centre study, we included a large number of patients, we observed substantial distribution to specific therapy sequences and therefore rather low patient numbers in different algorithms in advanced therapy lines. Thus, we primarily aimed to describe treatment algorithms and outcomes rather than to perform direct statistical comparisons between the different agents in specific therapy sequences. Our data demonstrating that baseline differences were associated with the choice of first-line agents show that such direct comparisons would not be valid. Thus, the data must be understood as descriptive.
It is therefore not surprising that our data do not replicate some previous reports using propensity-score matching to compare cohorts and demonstrating, for example, higher efficacy of second-line ustekinumab compared with vedolizumab in CD 34 or higher persistence on vedolizumab than infliximab in UC. 27
Our data are also limited by the fact that it is a single-centre retrospective study that might not easily be generalized to other settings. Moreover, the focus on the four biologics infliximab, adalimumab, vedolizumab and ustekinumab has been outdated by the rapid evolution of therapeutic choices in IBD. We decided not to include tofacitinib despite its approval for UC during the study period in 2018, 5 since too few patients received the drug to report meaningful remission rates. For filgotinib and ozanimod, which were approved for UC in 2021,6,9 the follow-up period was too short for our analyses. Upadacitinib (UC and CD), risankizumab (CD and UC), mirikizumab (UC) and etrasimod (UC) were approved after the study period.7,8,10,11,35 However, while these compounds will likely have a substantial impact on real-world treatment sequences, it is clear that it will take considerable time to collect similar data for these agents.
In conclusion, the tertiary centre real-world therapeutic patterns that we describe add further details to a growing fund of observational studies that might together contribute to clinical practice guidelines and help to shape individual therapeutic decisions. Moreover, our data strongly encourage further efforts to identify biomarkers for the precise tailoring of effective therapy to patients.
Supplemental Material
sj-docx-1-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-docx-1-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-pdf-2-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-pdf-2-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-10-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-tif-10-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-11-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-tif-11-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-12-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-tif-12-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-3-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-tif-3-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-4-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-tif-4-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-5-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-tif-5-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-6-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-tif-6-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-7-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-tif-7-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-8-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-tif-8-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-9-tag-10.1177_17562848241284051 – Supplemental material for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience
Supplemental material, sj-tif-9-tag-10.1177_17562848241284051 for Treatment trajectories and outcomes in inflammatory bowel disease: a tertiary single-centre experience by Kim Wagner, Tanja M. Müller, Francesco Vitali, Sarah Fischer, Sophie Haberkamp, Rachel Rouse-Merkel, Raja Atreya, Markus F. Neurath and Sebastian Zundler in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The research of TMM, RA, MFN and SZ was supported by the Interdisciplinary Center for Clinical Research (IZKF) and the ELAN program of the University Erlangen-Nuremberg, the Else-Kröner-Fresenius-Stiftung, the Fritz Bender-Stiftung, the Dr. Robert Pfleger Stiftung, the Litwin IBD Pioneers Initiative of the Crohn’s and Colitis Foundation of America (CCFA), the Kenneth Rainin Foundation, the Ernst Jung-Stiftung for Science and Research, the German Crohn’s and Colitis Foundation (DCCV) and the German Research Foundation (DFG).
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.