
Abstract
Objectives:
Fatigue is common in people with inflammatory bowel disease (IBD) and is associated with IBD activity, sleep disturbance, anxiety and depression. The relative contribution of these factors to fatigue is unclear. This study aimed to investigate the relationship between fatigue and these factors through a novel approach using structural equation modelling.
Design:
Online questionnaire circulated via three tertiary IBD centres and Crohn’s Colitis Australia.
Methods:
Fatigue was assessed using the Functional assessment of chronic illness measurement system fatigue subscale. Validated measures of sleep, anxiety, depression and IBD activity were included. Following correlation analyses, a structural equation model was developed for the outcome of the fatigue score. Direct and indirect effects were calculated.
Results:
There were 630 complete responses to the online questionnaire. The median age of respondents was 41 with the majority female and over half (52%) on biologic medication. Structural equation models for Crohn’s disease and ulcerative colitis demonstrated a good fit. In Crohn’s disease, the relationship between IBD activity and fatigue was mostly mediated indirectly through the influence of IBD activity on sleep, anxiety and primarily depression. Sleep quality mediated the influence of IBD activity and the indirect effects of depression on fatigue, but not anxiety. Unlike in Crohn’s disease, the direct influence of IBD activity on fatigue in ulcerative colitis was non-negligible, although remained of lesser magnitude than the indirect effect of IBD activity on fatigue. Depression was the primary indirect mediator of the influence of IBD activity on fatigue in ulcerative colitis.
Conclusion:
In Crohn’s disease, IBD activity leads to fatigue through its influence on sleep quality and mental health. The data suggest treatment of clinically significant depression, in both ulcerative colitis and Crohn’s disease, may result in the largest decline in fatigue score compared to other variables. Treatment algorithms for fatigue should consider depression a priority.
Plain language summary
Fatigue is common in people with inflammatory bowel disease. Studies investigating the causes of fatigue in people with inflammatory bowel disease have consistently identified depression, anxiety, sleep quality and IBD activity as factors associated with fatigue. People with inflammatory bowel disease were asked about their fatigue levels, sleep quality, depression, anxiety and inflammatory bowel disease activity. These responses were used to generate a model to explain the interaction between these factors and how they influence fatigue. The contribution of each of these factors to fatigue was then determined. Depression had the largest overall contribution. The influence of inflammatory bowel disease activity on fatigue occurred mostly through its impact on other factors such as depression and sleep quality. Consideration should be given to screening for and treating depression in people with inflammatory bowel disease and fatigue.
Keywords
Introduction
Inflammatory bowel disease (IBD) is a chronic relapsing-remitting immune disorder that can affect any part of the gastrointestinal tract and may also lead to extra-intestinal manifestations such as joint and skin disease. Fatigue is common in IBD patients with a prevalence of 48%. 1 The pathophysiology of fatigue in IBD is poorly understood2,3 although frequently reported associations include IBD activity, sleep disturbance, anxiety and depression.4–8 Whether these factors directly cause fatigue or act via secondary mechanisms is currently unclear.
There has been increasing interest in a potential bidirectional relationship between sleep and IBD. Abnormal sleep patterns have been associated with poor health incomes including cardiovascular disease 9 and all-cause mortality. 10 Meta-analyses indicate that poor sleep is prevalent in patients with IBD, 11 more common than in controls 12 and worse in those with clinically active disease. 13 It is also associated with mental health conditions14,15 and poorer quality of life.16,17 Longitudinal studies suggest that sleep disturbance is associated with fatigue 18 and disease activity.19–21 Furthermore in Crohn’s disease, sleep disturbance increases the risk of hospitalisation. 22 Whilst anxiety and depression are prevalent in people with IBD, 23 it is the depression but not anxiety that is associated with poor sleep. 24
The aetiology of fatigue is complex and likely multifactorial. The frequently seen associations with fatigue in IBD (IBD activity, sleep, depression and anxiety) have the potential to influence each other along with their influence on fatigue. This leads to a complex inter-connected web of cause and effect between these different factors. It is consequently unclear what the value of targeting a single cause of fatigue would be and what potential flow-on effects it may have on other factors that also influence fatigue.
Structural equation modelling (SEM) is a technique that allows the testing of hypotheses about relationships between variables and is increasingly used to understand multivariate relationships. Path analysis is a subset of SEM that involves the development of a model incorporating causal paths between variables based on the relevant literature. The model is then evaluated based on observational data and modified in an iterative process with paths or variables added or removed to improve model fit. Direct and indirect effects of variables on other variables can then be calculated based on the paths in the model. Amongst other applications, SEM has been used in IBD to examine the influence of social support on disease activity and distress, 25 investigate the relationship between depression and Crohn’s disease, 26 evaluate patient satisfaction in IBD 27 and examine the factors influencing pain interference in IBD. 28
This study aimed to investigate the relationship between fatigue, sleep and IBD activity through SEM. We hypothesised that the effects of IBD activity and depression on fatigue are predominantly mediated via sleep quality.
Materials and methods
An online questionnaire was circulated to patients with IBD using tertiary hospital patient email lists, private gastroenterology practice email lists and social media with individuals, with a self-reported diagnosis of IBD and over 18 years of age, invited to participate. Demographic data such as age and sex were captured, along with IBD-related data including current treatment, disease duration and previous surgery. The study was approved by the Southern Adelaide Human Research Ethics Committee (203.20). The study has been reported according to the Checklist for reporting results of internet E-surveys. 29 Two consumer advocates (people with IBD) were asked to provide feedback on the proposed research.
Potential participants received online information regarding the study, including the expected duration and completion of the questionnaire was accepted as consent. No incentive was offered to complete the questionnaire. The questionnaire was available from January 2022 to December 2022. The questionnaire included 7 screens with an average of 15 items per screen. Participants were able to review and change their answers prior to survey completion. Neither cookies nor IP address tracking was used to identify duplicate entries. The data were examined by age, height and weight – with matching entries examined for duplicates.
Fatigue was measured using the functional assessment of chronic illness measurement system – fatigue (FACIT-F) scale which is a subscale of the Functional assessment of chronic illness measurement system. The FACIT-F subscale has been validated as a measure of fatigue in an IBD population. 30 This comprises 13 questions with responses recorded on a 5-point Likert scale, with a score ranging from 0 to 52, with lower scores indicating worse fatigue and a score less than 30 indicating severe fatigue. 31 Of the many fatigue scores previously used in IBD populations, FACIT-F was included due to its use in a variety of different diseases and its brevity. 2
Sleep quality was measured using the Pittsburgh Sleep Quality Index (PSQI). The PSQI is a validated tool that assesses perceived sleep quality. 32 The index consists of subscales on sleep duration, sleep disturbance, sleep latency, daytime dysfunction, sleep efficiency, overall sleep quality and medications for sleep. The PSQI score ranges from 0 to 21, with a value >5 representing poor sleep quality.
IBD disease activity was assessed using the Harvey Bradshaw Index (HBI) in the case of Crohn’s disease with HBI >5 considered active disease. 33 The patient-reported version of the HBI was utilised in the survey, although a decision was made to maintain the general well-being and abdominal pain score similar to the physician HBI rather than using a 10-point Likert scale. 34 The Simple Clinical Colitis Activity Index (SCCAI) was used in the case of ulcerative colitis, an SCCAI >5 was considered an active disease. 35 The patient-reported form of the SCCAI was utilised 36 in the survey. The use of a self-reported SCCAI has been previously validated with good agreement with physician-reported SCCAI. 37
Anxiety was assessed using the generalised anxiety disorder 7-item scale (GAD-7) 38 with a score >10 indicating likely clinically significant anxiety. Depression was assessed by the Patient Health Questionnaire 9 (PHQ-9) with a score over 15 considered to show likely clinically significant depression. 39
Statistical analysis
Statistical analysis was performed using Stata SE 16 (StataCorp, College Station, TX, USA). Submissions with inadequate completion of score or index were excluded. Mean and standard deviation were reported for normally distributed variables, with comparisons made by the Student’s t-test. The median and interquartile range were reported for non-normally distributed variables, with comparisons made using the Mann–Whitney U test. For categorical data, Pearson’s χ2 test or Fisher’s exact test were used as appropriate. Pearson’s or Spearman’s correlation was used as appropriate, with the interpretation of coefficients as very weak <0.19, weak 0.2–0.3, moderate 0.3–0.5, strong 0.5–0.79 and very strong >0.80. 40
To further investigate the relationship between sleep and fatigue and to test the hypothesis that sleep mediates the influence of IBD activity on fatigue SEM was performed using multivariate linear regression for path analysis. 41 Based on the correlational analysis, a general model was constructed using sleep quality, mental health and IBD activity (PSQI, GAD-7, PHQ-9, SCCAI and HBI) as inputs and fatigue (FACIT-F) as output. The model was optimised through an iterative process that involved sequential removal and the addition of variables and pathways to improve model performance. 42 Separate models were constructed for Crohn’s disease and ulcerative colitis (including indeterminate colitis). The model performance was assessed considering the following multiple fit criteria – root mean square error of approximation (RMSEA) < 0.05, comparative fit index (CFI) > 0.95, Tucker–Lewis Index (TLI) > 0.95, standardised root mean residual (SRMR) < 0.09, Chi-squared goodness of fit statistic (χ2P) > 0.05 and Chi-squared to degrees of freedom value (χ2/N) = 1−4. 43 Direct and indirect effects were then calculated based on this model. A direct or indirect effect was considered negligible if it was less than 10% of the associated direct or indirect effect. A direct or indirect effect was considered significant if it was statistically significant and non-negligible. To improve interpretability, the fatigue score has been inverted so that a numerically higher fatigue score indicates higher fatigue.
Results
There were 670 responses to the online questionnaire with 630 complete responses. The median age of the participants was 41 years (32–70), with the majority being female (78%), 61% with Crohn’s disease and 3% with indeterminate colitis. The mean disease duration was 12.6 years (±10.2), 32% had undergone surgery for IBD and approximately half were on biologic disease-modifying therapy (52.8%) (see Table 1).
Cohort demographics and IBD data, SCCAI, HBI and FACIT-FS.

FACIT-FS, functional assessment of chronic illness measurement system – fatigue score; HBI, Harvey Bradshaw Index; IBD, inflammatory bowel disease; IQR, interquartile range; SCCAI, simple clinical colitis activity index; SD, standard deviation.
The mean FACIT-F score was 27 (±11.9) with severe fatigue (FACIT-F <30) seen in 62% of respondents. The mean sleep quality (PSQI) score was 9.49 (±3.99) with 75% of patients reporting poor sleep quality (PSQI > 5). Clinically significant depression (PHQ-9 >15) was reported in 21%, and clinically significant anxiety (GAD-7 > 10) was seen in 33%.
Pearson correlation coefficients were calculated for fatigue (FACIT-F), sleep quality (PSQI), anxiety (GAD-7), depression (PHQ-9), IBD data, demographic and IBD medication (Tables 2 and 3). There was a strong correlation between fatigue and depression, anxiety and sleep quality in those with Crohn’s disease. In addition to this, sleep quality showed a strong correlation with depression and anxiety and a moderate correlation with IBD activity. In those with ulcerative colitis, there was a strong correlation between fatigue, depression and anxiety and a moderate correlation between fatigue and IBD activity and sleep quality. In addition to this, there was a moderate correlation between anxiety, depression and IBD activity.
Pearson’s correlation coefficients with significance levels for Crohn’s disease population.

Greater fatigue was seen with higher scores as measured by inverted FACIT-FS. Anxiety indicated by anxiety scores Generalised anxiety disorder 7-item, higher scores indicate worse anxiety. Depression is indicated by depression scores Patient Health Questionnaire 9-item, higher scores indicate worse depression. Sleep quality as per the Pittsburgh Sleep Quality Index, higher scores are seen in worse sleep quality.
p < 0.05. **p < 0.005. ***p < 0.0005. Bonferroni adjusted.
FACIT-FS, functional assessment of chronic illness measurement system – fatigue score; IBD, inflammatory bowel disease.
Pearson’s correlation coefficients with significance levels for ulcerative colitis and indeterminate colitis population.

Greater fatigue was seen with higher scores as measured by inverted FACIT-FS. Anxiety indicated by anxiety scores Generalised anxiety disorder 7-item, higher scores indicate worse anxiety. Depression is indicated by depression scores Patient Health Questionnaire 9-item, higher scores indicate worse depression. Sleep quality as per the Pittsburgh Sleep Quality Index, higher scores are seen in worse sleep quality.
p < 0.05. **p < 0.005. ***p < 0.0005. Bonferroni adjusted.
FACIT-FS, functional assessment of chronic illness measurement system – fatigue score; IBD, inflammatory bowel disease.
Depression showed a strong correlation with anxiety and a moderate correlation with IBD activity for both Crohn’s disease and ulcerative colitis. Anxiety showed a weak correlation with age and a moderate correlation with IBD activity both Crohn’s disease and ulcerative colitis. Previous IBD-related surgery showed a moderate correlation with IBD disease duration. There was a very weak correlation between age and fatigue in ulcerative colitis but not Crohn’s disease.
Crohn’s disease
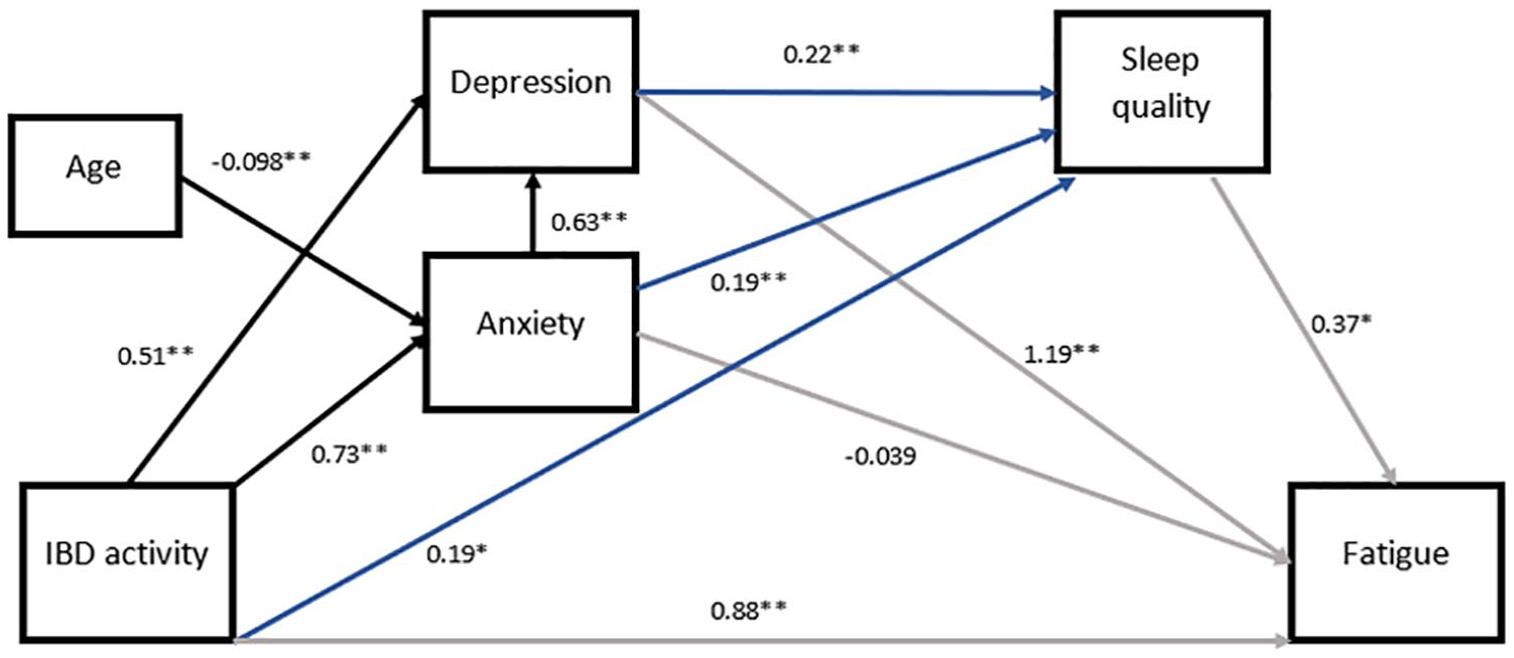
SEM was undertaken for the outcome of fatigue score (FACIT-F) including variables based on previous correlation analysis (see Figure 1 and supplementary material for further details). The model was optimised for fit with the final model demonstrating good fit (RMSEA 0.016, SRMR 0.013, CFI 1.00, TLI 0.99, χ2(N) = 3.46, χ2p = 0.32). The final model included IBD activity, depression, anxiety, sleep quality and weight. Consideration was given to including body mass index instead of weight; however, this resulted in an overall worse fit. The model accounted for 91.2% of the variance of fatigue. Fatigue had a direct relationship with IBD activity, depression, anxiety and sleep quality. Fatigue was indirectly influenced by depression, anxiety and IBD activity via sleep quality. Fatigue and sleep were indirectly influenced via body weight through depression.

Structural equation modelling using multivariate linear regression for Crohn’s disease. Incorporated all significant variables from correlational analysis. RMSEA 0.024, SRMR 0.019, CFI 0.999, TLI 0.996, χ2(N) = 3.57, χ2p = 0.31, AIC 12,562.03, BIC 12,634.21. Coefficients included on paths. Error terms not shown. Greater fatigue was seen with higher scores as measured by inverted FACIT-FS scores. Anxiety indicated by anxiety scores Generalised anxiety disorder 7-item, higher scores indicate worse anxiety. Depression indicated by depression scores Patient Health Questionnaire 9-item, higher scores indicate worse depression. Sleep quality as per the Pittsburgh Sleep Quality Index, higher scores are seen in worse sleep quality. IBD activity is described by the Harvey Bradshaw Index. For readability – the blue line indicates the paths influencing sleep quality, the grey indicates the paths influencing fatigue and the black indicates the paths amongst other variables.
Direct and indirect effects on fatigue scores were calculated from the SEM and were used to determine the direct effect on the fatigue score (see Table 4) as well as the indirect effects via other intermediate variables. The effect of IBD activity on fatigue was primarily mediated through indirect effects (effect size 1.35) with its direct effect significantly smaller but not negligible (effect size 0.35). Depression influenced fatigue directly (effect size 1.55) with negligible indirect effects mediated via sleep (effect size 0.06). The direct effect of anxiety on fatigue was negligible with indirect effects predominantly via depression and to a lesser extent, sleep quality. Anxiety influenced fatigue indirectly via its influence on depression and sleep quality. Considering the various values of the scores for clinically significant depression (PHQ-9 >15), clinically significant anxiety (GAD-7 >10), clinically active IBD (HBI > 5) and poor sleep (PSQI >5), clinically significant depression had the largest overall total effect on fatigue scores.
Direct and indirect effects for fatigue score (FACIT-F) incorporating depression (PHQ-9), anxiety (GAD-7), sleep quality (PSQI), IBD activity (Harvey Bradshaw Index) for structural equation models for Crohn’s disease and ulcerative colitis or indeterminate colitis.

p < 0.05. **p < 0.001.
CI, confidence interval; FACIT-F, functional assessment of chronic illness measurement system – fatigue score; GAD-7, generalised anxiety disorder 7-item scale; IBD, inflammatory bowel disease; PHQ-9, Patient Health Questionnaire 9; PSQI, Pittsburgh Sleep Quality Index.
Ulcerative colitis and indeterminate colitis
SEM was undertaken for the outcome of fatigue score (FACIT-F) including variables with at least a weak correlation with fatigue and sleep quality (see Figure 2 and supplementary material for further details). The model was optimised for fit with the final model demonstrating good fit (RMSEA 0.000, SRMR 0.016, CFI 1.00, TLI 1.00, χ2(N) = 2.997, χ2p = 0.39). The final model accounted for 94.4% of the variance in fatigue scores and included IBD activity, depression, anxiety, age and sleep quality. Fatigue had a direct relationship with IBD activity, depression, anxiety and sleep quality and was indirectly influenced by depression, anxiety and IBD activity via sleep quality. Fatigue was indirectly influenced by age through anxiety.
Structural equation modelling using multivariate linear regression for ulcerative colitis and indeterminate colitis. Incorporated all significant variables from correlational analysis. RMSEA < 0.001, SRMR 0.016, CFI 1.00, TLI 1.00, χ2(N) = 2.997, χ2p = 0.39, AIC 7517.046, BIC 7578.99. Coefficients included on paths. Error terms not shown. Greater fatigue was seen with higher scores as measured by inverted FACIT-FS scores. Anxiety indicated by anxiety scores Generalised anxiety disorder 7-item, higher scores indicate worse anxiety. Depression indicated by depression scores Patient Health Questionnaire 9-item, higher scores indicate worse depression. Sleep quality as per the Pittsburgh Sleep Quality Index, higher scores are seen in worse sleep quality. IBD activity is described by the Simple Clinical Colitis Activity Index. For readability – the blue line indicates the paths influencing sleep quality, the grey indicates the paths influencing fatigue and the black indicates the paths amongst other variables.
Direct and indirect effects were calculated from this model and reported for fatigue scores (see Table 4). The effect of IBD activity on fatigue score was primarily mediated through indirect effects but the direct effect, although smaller, remained relevant. Depression influenced fatigue directly with negligible indirect effects mediated through sleep quality. Anxiety influenced fatigue indirectly via its influence on depression and sleep quality with its direct effect on fatigue negligible. IBD activity had significant direct and indirect effects on fatigue. The influence of age on fatigue scores was mediated through anxiety. Considering the various values of the scores for clinically significant depression (PHQ-9 >15), clinically significant anxiety (GAD-7 >10) and poor sleep (PSQI >5), clinically significant depression had the largest overall total effect on fatigue scores.
Further analysis of indirect effects
Further analysis of indirect effects in terms of mediating variables yielded similar results for ulcerative colitis and Crohn’s disease (see Table 5). Sleep quality mediated the indirect effects of depression and IBD activity but did not mediate a significant proportion of the indirect effects of anxiety.
Indirect effects on fatigue score (FACIT-F) by mediating variables – sleep quality, depression (PHQ-9), anxiety (GAD-7) – from structural equation models for ulcerative colitis and Crohn’s disease.

FACIT-F, functional assessment of chronic illness measurement system – fatigue score; GAD-7, generalised anxiety disorder 7-item scale; IBD, inflammatory bowel disease; PHQ-9, Patient Health Questionnaire-9.
Discussion
This work describes a novel approach to understanding the causation of fatigue in patients with IBD using SEM to determine direct and indirect effects. Separate SEM models were developed for Crohn’s disease and ulcerative colitis with a good model fit. In both models, sleep was a mediating variable for IBD activity, anxiety and depression with similar results for both Crohn’s disease and ulcerative colitis. However, the effect size mediated by sleep was comparatively small. Rather, it was depression that primarily influenced fatigue in the IBD population and mediated most of the effect of IBD activity on fatigue. Noting the prevalence of depression in the IBD population, it is likely that treating depression may lead to the largest overall improvement in fatigue. The methods to treat depression may include decreasing IBD activity.
These data are consistent with earlier findings which have suggested a treatment approach for fatigue in IBD patients that includes attention to optimising mental health issues, improving sleep quality and controlling IBD activity if present, all factors used in this model. 2 However, although our model provides some support for this approach, in that overall fatigue scores were influenced by all of these factors, the new finding of the magnitude of the effect from depression warrants that it receives a higher priority for assessment and treatment. It should be considered that clinically active IBD may also have a significant role in the severity of depression in this context.
Although fatigue in IBD is often considered as a single entity, there were significant differences in the influence of disease activity on fatigue in patients with Crohn’s disease, which was primarily mediated via indirect effects, compared to those with ulcerative colitis where direct magnitude was non-negligible. This may in part reflect the more systemic nature of inflammation in Crohn’s disease or possibly the influence of symptoms such as abdominal pain, more frequently seen in Crohn’s disease, on sleep and mental health. Weight was included in the model of Crohn’s disease with its effect mediated via depression rather than an influence on IBD activity. The inclusion of weight in the ulcerative colitis model resulted in a worse overall fit and it was consequently not incorporated. Obesity is common in those with IBD with studies suggesting 15%–40% are overweight,44,45 with a hypothesised negative influence of obesity on the course of Crohn’s disease.44,46 Age was included in the ulcerative colitis model and influenced fatigue via anxiety, with increasing age associated with less fatigue – an association that has been previously documented although not consistently seen. 47 There was no significant correlation between age and fatigue in the Crohn’s disease population.
Limitations to this study include the possibility of selection bias due to the use of an online questionnaire. This may attract patients with fatigue or sleep problems. Similarly, the form of survey and method of recruitment is likely responsible for the predominantly female cohort. Crohn’s disease may be over-represented in this study population compared to the Australian IBD population. 48 However, we note that rates of anxiety, depression, fatigue and poor sleep quality were similar to other cohorts and consequently the results appear to be generalisable. Reporting bias may also be significant, noting a study of people with Crohn’s disease reported worse sleep quality than that observed by objective measures. 14 Unfortunately, implementing objective sleep measurement over such a large cohort is impractical. The absence of an objective measure of IBD activity is also a limitation.
Using the above method of data collection, there was no opportunity to assess for factors such as anaemia that has been associated with fatigue. 6 However, 1 anaemia has not been associated with fatigue in numerous cross-sectional studies, and hence its lack of inclusion in the current model is not considered a significant limitation.6,49,50 It is acknowledged that path analysis is unable to determine the direction of effects. The causes of fatigue in IBD are complex and likely numerous. Acknowledging the complexity of this area and the stigma surrounding mental health, the clinical implications of this study are limited and require further validation. Future work should consider a validation cohort incorporating other possible influences on fatigue and incorporate objective measures of IBD activity such as calprotectin and biochemical parameters such as C-reaction protein and albumin. Consideration should be given to screening and treating for depression as part of routine IBD clinic, noting that further work is required in this area.
Conclusion
A new model was developed to examine the mediation of factors influencing fatigue in people with IBD. Using this, we have shown that although sleep quality mediates the effects of clinically active IBD and depression on fatigue, the mediated effect size is comparatively small. In Crohn’s disease, unlike ulcerative colitis, the influence of IBD activity on fatigue was largely mediated indirectly through its influence on other factors. The data suggest treatment of clinically significant depression may result in the largest decline in fatigue score compared to other variables. Treating depression if present in people with IBD and fatigue should be considered a priority.
Supplemental Material
sj-docx-1-tag-10.1177_17562848241271987 – Supplemental material for Depression influences fatigue in inflammatory bowel disease amongst other factors: a structural modelling approach
Supplemental material, sj-docx-1-tag-10.1177_17562848241271987 for Depression influences fatigue in inflammatory bowel disease amongst other factors: a structural modelling approach by Alex Barnes, Robert V. Bryant, Sutapa Mukherjee, Jane M. Andrews, Peter Bampton, Robert J. Fraser and Réme Mountifield in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.