
Abstract
Background:
Despite the continuously rising rate of pediatric-onset inflammatory bowel diseases (PIBD), there are no consensus transitional guidelines or standardized practices.
Objectives:
We aimed to examine: (1) the determinants of a successful transfer, (2) the effects of the transfer versus transition on the disease course and patient compliance, (3) the unique characteristics of PIBD patients, that need special attention in adult care.
Design:
Longitudinal, follow-up, controlled study conducted between 2001 and 2022, with retrospective data collection until 2018, thence prospective.
Methods:
Three hundred fifty-one PIBD patients enrolled in the study, of whom 152 were moved to adult care, with a mean post-transfer follow-up time of 3 years. Seventy-three patients took part in structured transition, whereas 79 self-transferred to adult care. The main outcome measures were disease activity (defined by PCDAI, PUCAI, CDAI, and Mayo-scores) and course, hospitalizations, surgeries, IBD-related complications, including anthropometry and bone density, patient compliance, medication adherence, and continuation of medical care.
Results:
Patients who underwent structured transition spent significantly more time in remission (83.6% ± 28.5% versus 77.5% ± 29.7%, p = 0.0339) and had better adherence to their medications (31.9% versus 16.4% non-adherence rate, p = 0.0455) in adult care, with self-transferred patients having a 1.59-fold increased risk of discontinuing their medical care and a 1.88-fold increased risk of experiencing a relapse. Post-transfer the compliance of patients deteriorated (38.5% versus 29%, p = 0.0002), with the highest lost-to-follow-up rate during the changing period between the healthcare systems (12.7%), in which female gender was a risk factor (p = 0.010). PIBD patients had experienced IBD-related complications (23.4%) and former surgeries (15%) upon arriving at adult care, with high rates of malnutrition, growth impairment, and poor bone health.
Conclusion:
Structured transition plays a key role in ensuring the best disease course and lowering the lost-to-follow-up rate among PIBD patients.
Brief summary
Structured transition plays a key role in ensuring the best disease outcome among PIBD patients, as in our study it was associated with lower disease activity, fewer relapses, better medication adherence, and lower lost-to-follow-up rate as opposed to self-transfer.
Introduction
Inflammatory bowel disease (IBD) is an umbrella term including Crohn’s disease (CD), ulcerative colitis (UC), and inflammatory bowel disease unclassified (IBD-U), defined as chronic, progressive inflammatory disorders of the gastrointestinal tract, with a relapsing-remitting disease course, and possible extraintestinal manifestations.1,2
Approximately 10% of IBD patients have a pediatric-onset disease (PIBD), which is thought to be more complex and extensive compared to the adult-onset form, with a more severe phenotype and a tendency for rapid progression.3–6 The incidence and prevalence of IBD have been rising in the past decades, among the pediatric population even in a faster manner, with an incidence peak during preschool age and late adolescence.7–9
Transition was first defined by Blum et al. in 1993 as a purposeful, planned movement of adolescents with chronic conditions from the pediatric to the adult healthcare system, including the gradual shift of the healthcare- and disease-related responsibilities from the caregivers and the parents to the patients. 10 On the contrary, transfer implies only the point of handover of care between the pediatric and the adult healthcare-providing team, which should be considered as a part of the transitioning process, not necessarily the endpoint.11–13 The Society for Adolescent Medicine highlights the complexity and the multiple layers of this changing process, as they define transition as ‘a gradual, multi-dimensional and family-oriented process with a focus on the anticipated developmental stage of an individual and with the ultimate goal of transfer to adult healthcare settings by empowering patients with disease knowledge and self-management skills and by preparing healthcare providers with adequate knowledge’. 14
Despite transfer being inevitable in pediatric-onset chronic conditions, there are currently no official consensus guidelines and standardized transitional practices regarding IBD patients. However, transition has been in the focus of IBD care development in the past decade, with the first position paper being published in 2002 by NASPGHAN, followed by further recommendations from the United States (2011), Italy (2015), and the United Kingdom (2015).10,15–17 ECCO published its topical review in 2017, including 14 practice points for healthcare providers, but similarly to the previous publications, it mostly relies on expert opinions, clinical experience, and literature reviews of other chronic diseases.10–12,15,16,18,19
The existing recommendations, however, do not necessarily translate into practice. Reportedly, 40–80% of the gastroenterologists do not perform any formalized transition, although 79% of them would consider it highly important, to have transitional guidelines.11,20 In a survey-based study from the United States, 60% of pediatric gastroenterologists stated, that they were not familiar with transitional recommendations, and only 0.7% of them incorporated the recommendations into practice. 21
Transition is covering a vulnerable period of life, where unaddressed medical and healthcare needs can lead to long-term consequences.16,22 The association between inadequate transitional care and adverse health outcomes has been thoroughly documented in numerous chronic conditions, including type 1 diabetes mellitus, congenital heart diseases, cystic fibrosis, juvenile rheumatoid arthritis, and hematological disorders.23–26 Among pediatric-onset diabetes patients, the successful transition was shown to be associated with improved objective measures of glycaemic control, better outpatient control and engagement with screening programs, higher compliance to adult care providers, furthermore in decreased rates of hospitalization and diabetic ketoacidosis.16,27–30 Without a structured transitional program the risk of disengagement with healthcare rises. 16 Following solid organ transplantation, unsuccessful transition is associated with worsening compliance, increased graft loss, and higher mortality.16,31,32
The currently available literature examining the effects of transition in IBD is limited to single-center studies, mostly without randomization or a control group. 33 Inadequate transitional care in IBD is associated with non-adherence to medications and non-compliance regarding visits, a restricted growth potential, and an increased risk of surgery.16,33 Furthermore, in a French study, a structured transitional program was associated with improved patient and healthcare provider satisfaction. 34
We aimed our research to examine three main questions regarding the transitional care of PIBD patients:
(1) What are the determinants of a successful transitioning process?
(2) What are the short- and long-term effects of the changing process to adult care, including the comparison between transition and self-transfer on the disease activity, course, and patient compliance?
(3) What are the unique characteristics of PIBD patients that require special attention in adult care?
Materials and methods
Our longitudinal, follow-up, controlled observational study incorporated a retrospective and a prospective data collection period, intending to analyze the effects of the changing period to adult care, including the comparison of a structured transitional program with self-transfer on the disease course, activity, and compliance of the patients. Furthermore, we examined the determinants of a successful transfer and the special characteristics of the PIBD patients, that require special attention in adult care. The project was carried out in the Pediatric Center of Semmelweis University (Budapest, Hungary), in cooperation with the Department of Surgery, Transplantation, and Gastroenterology and the Department of Internal Medicine and Oncology of Semmelweis University.
The study was performed and reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 35 This study presents a detailed methodology in the Methods section, facilitating reproducibility and enabling fellow researchers to replicate the experiments conducted herein.
Study period and data collection
The study period was 20.5 years, between 1 September 2001 and 1 March 2022. We collected data from the medical systems of the participating Clinics and the eHealth Infrastructure of Hungary. The data was reviewed retrospectively until 2018, thence prospectively. Detailed information was collected about the patients (date of birth, gender, race, other chronic diseases, family history of IBD), disease [subtype, phenotype, extent, activity and disease course, extraintestinal manifestations (EIMs), complications], treatments (medical, nutritional, surgeries, hospitalizations, medication side effects), anthropometrical data (height, weight, BMI), patient compliance, and medication adherence. The basic data about the patients were reported at the time of diagnosis, whereas data about the disease, treatments, anthropometrics, compliance, and adherence were noted both at the time of the diagnosis and continuously during the visits during the study period.
Inclusion and exclusion process
The summary of the inclusion and exclusion process can be seen in Figure 1.
Inclusion criteria: All 382 PIBD patients (including CD, UC, and IBD-U) treated partially or entirely in our Pediatric Center during the examination period were available for the initial inclusion process in the study.
Exclusion criteria: Due to inaccessible medical data from the study period, 31 patients were excluded, resulting in 351 patients being enrolled in our research.
Transition and self-transfer: Of the included 351 patients, 152 were moved to adult care during the examination period, of whom 73 were enrolled in our transitional program, whereas 79 adolescents self-transferred to adult care and served as our control group. Every patient had the opportunity to enroll in the transitional program, but the inclusion was not mandatory. The patients who decided against the transitional program then self-transferred, with reasons behind their decision as declining to enroll in a structured transition, a completely different timing of their transfer as suggested, or transfer to a hospital not included in our transitional program. There was no significant difference between the two groups considering either of the examined patient-, disease-, or treatment-related variables noted in the data collection section (Table 1). Both self-transfer and transition were initiated in 2015. Until 2018, the transitional meetings were held irregularly, thence monthly.
Addressing the lost-to-follow-up patients: 18 patients discontinued their medical care during pediatric care, 16 during the changing period between the two healthcare systems, and 15 patients after being moved to adult care. As patient compliance and the determinants of a successful transferring process to adult care were among the aims of our study, the lost-to-follow-up patients were examined separately.

The inclusion and exclusion process of our study.
Main characteristics of the patients enrolled in our study.
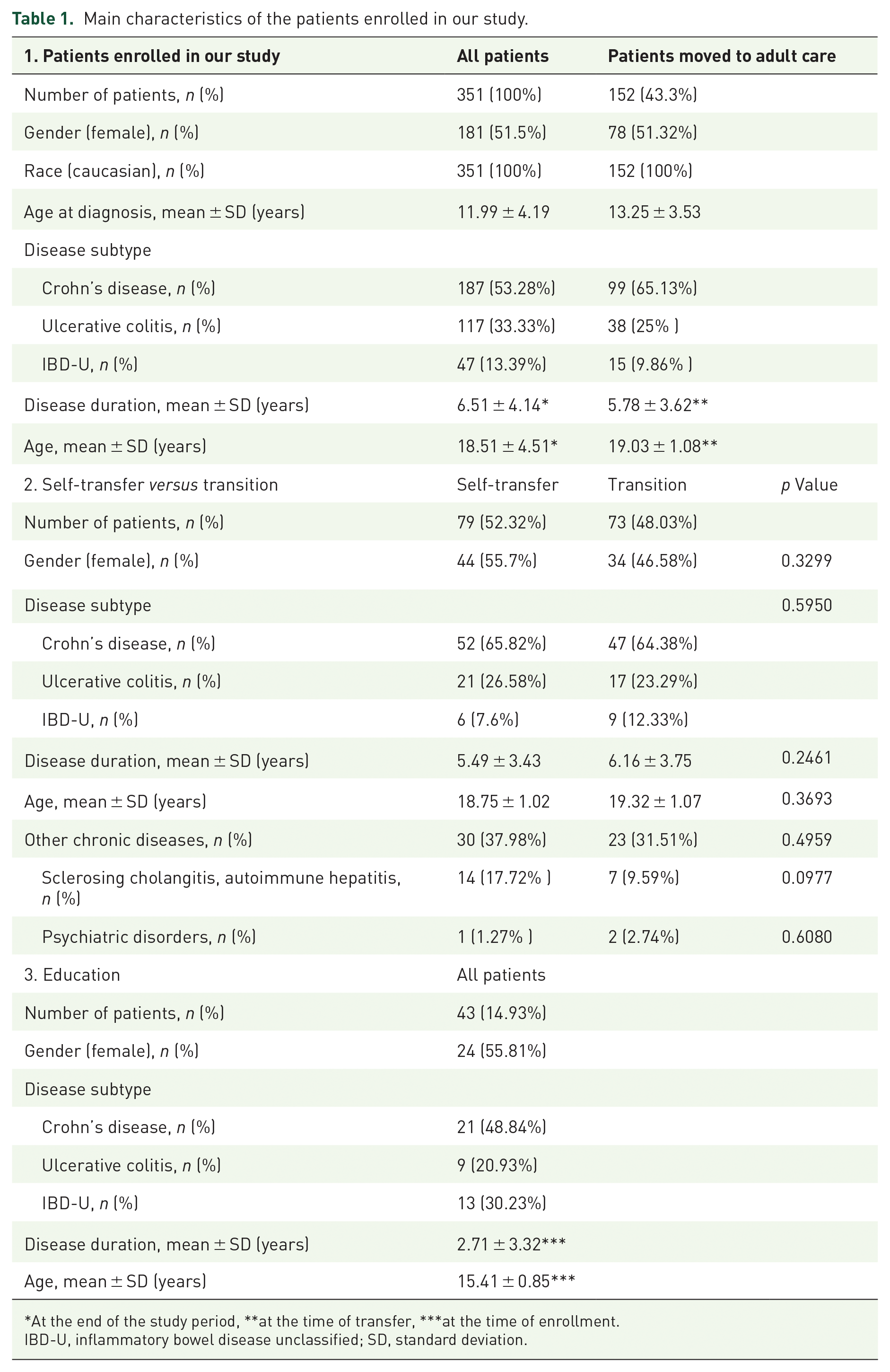
At the end of the study period, **at the time of transfer, ***at the time of enrollment.
IBD-U, inflammatory bowel disease unclassified; SD, standard deviation.
Study design
Our transitional program consisted of an integrated educational (mentor) program and a joint transitional meeting with a written handout summary.
Mentor program: From the age of 12, patients had the opportunity to be enrolled in our age-appropriate, personalized educational program. The teaching occasions took place before their scheduled visits, to make it accessible for all patients. They could learn in a step-wise manner during these one-by-one meetings from our transitional coordinator about their disease characteristics, the most important diagnostic methods, their medications, possible complications of their disease and non-compliance, family planning, and the effects of alcohol and smoking on their disease course. Our educational program was initiated in 2018.
Last year before moving to adult care: A year before the planned transfer to adult care, we actively started to prepare all of our patients, regardless of their participation in the mentor program. We encouraged them to take more responsibility in handling their disease, we required them to take a more active role during their visits, and initiated talks about the differences between the two healthcare systems and the changing process. During this last year, the scheduled endoscopic procedures were preferably performed with the attendance of both the pediatric and the future adult care providers.
Timing of the transfer: We aimed the transfer after finishing high school, around 18–19 years of age, with a disease in stable remission. Special requests from the patients considering the timing of their transfer were also taken into consideration.
Joint transitional meeting, adult healthcare providers: The joint transitional meetings were held in our Pediatric center, with the attendance of the former pediatric and the future adult care provider, the transitional coordinator, and the patient. In most cases, parents were also present, depending on the request of the patient.
A detailed handout summary was prepared for the meeting, which summarized the most important information about the medical history of the patient, as well as the former disease course, treatments, hospitalizations, surgeries, and diagnostic results regarding their IBD.
At the end of the meeting, the date of the first adult-care visit was planned, as well as the bridging medical therapy during the changing period.
During the examination period of our study, we worked together with three adult gastroenterologist specialists, from two adult IBD Centrums in Budapest, Hungary. There were both male and female adult physicians in our transition team, so we could recommend a physician with the same gender to each of the patients if requested.
Statistical analysis
The statistical tests were performed and figures were created using GraphPad Prism version 10.0.2 for macOS, GraphPad Software, Boston, MA, USA. p < 0.05 was considered significant.
We employed Fisher’s exact test to assess the association between categorical variables. The resulting odds ratio (OR) with a 95% confidence interval (CI) was reported. To examine the differences between continuous variables, Welch’s test was used, and in the case of non-normal distributions, the Mann–Whitney test was employed. The specific test names can be found in the figure descriptions. The Cox proportional hazard model was applied to evaluate the impact of various variables on the occurrence of the outcome variable. The results of the Cox proportional hazard model were reported as OR with a 95% CI. Both univariate and multivariate modeling were conducted using the enter method. Dichotomous variables were encoded as 0/1 during model development. In the construction of Kaplan–Meier curves, cumulative events were plotted, and the curves were compared using the log-rank test. The resulting hazard ratios (HR) with 95% CI were reported.
Applied definitions and scores
Disease activity: To exclude intraobserver differences between the participating physicians, for documenting disease activity age- and disease-subtype-specific, validated scores were applied. In pediatric care, these were PCDAI 36 and PUCAI, 37 while in adult care CDAI, 38 and Mayo-score, 39 for CD and UC patients, respectively. For IBD-U patients the applied scoring system was determined based on the decision of the healthcare provider. The cut-off values for the different activities were defined based on the official recommendation of the scoring systems.
Relapse: Relapse was defined as a significant worsening of the disease activity and/or a reported moderate or severe disease activity. Both the terms significant change and disease activity were defined based on the above-mentioned disease activity scores.
Disease extent and phenotype: The Paris classification was used. 40
Hospitalizations and surgeries: Only the IBD-related interventions were analyzed.
Medical and nutritional therapy: Examined medical treatments taken either as maintenance therapy or for remission induction for IBD included steroids, biologics, aminosalicylates, antibiotics, and immunomodulators (e.g. azathioprine, methotrexate). Exclusive enteral nutrition, Crohn’s disease exclusion diet, and tube feeding were considered and noted as nutritional treatments. Only the IBD-related treatments were analyzed.
Successful transfer to adult care: A successful transfer to adult care was defined based on the ECCO proposal as continuity of care, determined as the patient attending at least one planned adult care visit during the examination period. To strengthen this definition, we also recorded patients who discontinued their care just after one attended visit. Emergency room visits without further follow-up were not considered a successful transfer.
Lost-to-follow-up patients: During pediatric care, if at least a year elapsed since their last attended visit and the patients did not recontinue their medical care during the follow-up period they were considered lost-to-follow-up.
Those patients, who during their last pediatric visit, took part in a transitional meeting or expressed their will to self-transfer to adult care, but during the examination period neither attended any adult care visit nor requested prescriptions for their medications and at least a year elapsed since their last pediatric visit were considered lost-to-follow-up during the changing period.
Of those patients, who attended at least one planned visit in adult care, but then discontinued their medical care for more than a year, neither requested medications nor attended any more visits until the end of the study period were considered lost-to-follow-up during adult care. Exception: some adult healthcare providers requested visits with an active disease, without any regular planned visits, these patients were not considered lost-to-follow-up, if a year elapsed since their last visit.
Non-compliance: The regular visits during pediatric care took place every 3–4 months for CD and 4–6 months for UC patients; therefore, after 190 days of non-appearance to visits patients were reported non-compliance. Furthermore, non-compliance was documented when the patients showed non-adherence to their medications or discontinued them.
Ethical considerations
The Semmelweis University Ethics Committee reviewed the study protocol, and it was determined that formal ethics approval was not required due to the open inclusion process (every patient had the right to be included in the interventional group, without blinding or random allocation), and also to the lack of invasive interventions and foreseeable negative effects on the patients or their disease course, both among the interventional and the control group. However, all procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The de-identification of data ensured the anonymity of the patients.
Results
The main characteristics of all the 351 PIBD patients enrolled in our study, taking part in the education, as well as the ones moved to adult care, either with self-transfer or transition can be seen in Table 1.
The most common disease localization for CD patients was ileocolonic (57.81%) with 57.29% having also upper gastrointestinal involvement, whereas for UC patients pancolitis (55%). During the examination period, the disease became more extensive in 34.55% of the CD and 30.44% of the UC patients.
Transition and self-transfer to adult care
During the examination period, 43.3% (n = 152) of all patients got moved to adult care, of whom 73 (48%) enrolled in our transitional program and 79 (52%) self-transferred to adult care. The main characteristics of these patients can be seen in Table 1. With multivariable logistic regression, none of the examined variables showed to be a significant determinant for patients to be more likely to be enrolled in the transition or to self-transfer, including patient variables [gender, other chronic diseases (including sclerosing cholangitis, autoimmune hepatitis, and psychiatric disorders), age, disease duration, compliance], disease variables (subtype, extent, phenotype, activity, EIMs, complications), and treatment variables (medications, hospitalizations, surgeries, medication side effects).
A significantly higher proportion of the transitioned patients had their disease in remission at the time of transfer to adult care than the self-transferred patients [91.04% versus 68.16%, p = 0.0012; OR 0.2101 (95% CI: 0.08115–0.5472)]. At the first adult visit, the proportion of patients with their disease in remission was 83.58% among the transitioned and 69.57% among the self-transferred patients (p = 0.0691). The mean time elapsed between the last pediatric and the first adult care visit was significantly higher in the self-transferred group than in the transitional group (361.95 ± 476.01 days versus 141.44 ± 158.43 days, p = 0.0002). After being moved to adult care, the mean follow-up time was 3.04 ± 1.67 years, accounting for 3.73 ± 1.72 years in the self-transferred and 2.13 ± 1.27 years in the transitioned group (p < 0.0001).
Lost-to-follow-up patients, discontinuation of medical care
During the study period, 49 patients discontinued their medical care, accounting for 13.96% of all patients. The 5.13% lost-to-follow-up rate reported in pediatric care significantly increased after being transferred to adult care, affecting every fifth patient [20.4%, p < 0.0001, OR 5.331 (95% CI: 2.900–9.798)]. The rate of discontinuation of care was the highest during the changing period from the pediatric to the adult health care system, reaching 12.66% of all patients, accounting for 8.22% of the transitioned and 10.53% of the self-transferred patients [p = 0.4540; OR 0.6179 (95% CI: 0.2109–1.6650)]. The main characteristics of the lost-to-follow-up patients can be seen in Table 2.
Main characteristics of the lost-to-follow-up patients during the different periods of care.

IBD-U, inflammatory bowel disease unclassified; SD, standard deviation.
Transition showed to be a significant protective factor for continuing care, as after the initiation of the healthcare provider changes 13.7% (n = 10) of the transitioned and 26.58% (n = 21) of the self-transferred patients discontinued their medical care (p = 0.0367; OR 0.4384 [95% CI: 0.193–1.018]). With Kaplan–Meier analysis, compared to the transitioned group the self-transferred patients were shown to be at a 1.59-fold higher risk of discontinuing their medical care after leaving pediatric care, including both the changing and the adult healthcare period (p = 0.0489; Figure 2).

Kaplan–Meier curve analysis of the self-transferred and transitioned patients regarding the probability of discontinuation medical care.
The mean time elapsed since loss of care (last attended visit) was significantly higher among the self-transferred patients compared to the ones enrolled in our transitional program (2.71 ± 1.48 years versus 1.65 ± 0.90 years, p = 0.0490).
After performing multiple univariate and multivariate logistic regressions examining the risk factor for discontinuation of medical care (Table 3), the higher number of days being hospitalized yearly showed to be a risk factor during pediatric care [17.85 ± 23.1 days versus 9.27 ± 10.2 days, p = 0.014; OR 1.036 (95% CI: 0.010–0.062)]. Female gender was a risk factor during the changing period between the two healthcare systems, with 87.5% (n = 14) of the lost patients being female (p = 0.010). This accounts for 17.95% of all female patients being moved to adult care compared to 2.7% of the male patients being lost [p = 0.0027; OR 7.875 (95% CI: 1.946–35.61)]. The only significant protective factor for continuing care in the adult system was the enrollment in our transitional program (p = 0.0007), with a lost-to-follow-up-rate of 5.97% (n = 4) versus 15.94% (n = 11) among the transitioned and self-transferred patients.
Multivariate logistic regression for discontinuation of care.

AZA, azathioprine; CI, confidence interval; IBD, inflammatory bowel disease; IBD-U, inflammatory bowel disease unclassified; MTX, methotrexate; OR, odds ratio; UC, ulcerative colitis.The significant p-values are highlighted in bold and every other p-value is written in italic.
Treatment with biologics was a protective factor for continuing care both during pediatric care and the changing period (p = 0.028 and p = 0.038), but after multivariate analysis, it failed to reach the level of significance.
Disease activity
After being moved to adult care, 48.53% (n = 66) of the patients experienced a relapse during the follow-up period, accounting for significantly more patients of the self-transferred group than of the transitioned patients [59.42% versus 37.31%, p = 0.0108; OR 2.460 (1.258–4.993)]. With Kaplan–Meier curve analysis (Figure 3) this difference was also shown to be significant, resulting in a 1.88-fold increased risk of relapse among the self-transferred patients compared to the transitioned group during the same timeframe in adult care (95% CI 1.13–3.09, p = 0.013). The mean time elapsed until the first relapse since the last pediatric visit was 358.68 ± 343.68 days, without a significant difference between the self-transferred and the transitioned group (p = 0.6116).

Kaplan–Meier curve analysis of the self-transferred and transitioned patients regarding the probability of relapse.
The mean follow-up time among the patients who did not experience a relapse was 2.36 ± 1.36 years.
The transitioned patients spent a significantly higher proportion of time with a disease in remission in adult care compared to the self-transferred patients [83.63% ± 28.5% versus 77.47% ± 29.65%, p = 0.0339; OR 0.7703 (0.7448–0.7967)]. Additionally, the time while the disease of the self-transferred patients had severe disease activity was significantly higher compared to the transitioned patients (1.66% ± 4.88% versus 1.15% ± 5.27%, p = 0.0204). To exclude that the baseline disease activity was already higher among the self-transferred patients, we also compared the disease activity of the two groups during pediatric care. There was no significant difference either between the proportion of time spent in remission (p = 0.1337) or with severe disease activity (p = 0.5390) in pediatric care; therefore, in our study transition was shown to be a protective factor against serious disease activity, as well as a significant determinant of disease remission in adult care [Figure 4(a) and (b)].

Disease activity of the self-transferred and transitioned patients in pediatric and in adult care (a) Pediatric care and (b) Adult care.
Patient compliance
Compliance problems were reported in 69.52% (n = 244) of all patients, complicated by an increasing non-compliance rate with both higher age and longer disease duration, exceeding 50% non-compliance by the time of transferring to adult care [Figure 5(a) and (b)].

Non-compliance rate of all patients regarding age and disease duration with logarithmic trend line. (a) Patient age and (b) Disease duration.
Non-frequent clinical attendance accounted for the majority of the non-compliance in both pediatric and adult care (68.08% and 78.8%), followed by non-adherence to medications (26.49% and 20.74%). After being moved to adult care the compliance of all patients significantly decreased [38.46% versus 28.95%, p = 0.0002; OR 0.4148 (0.2591–0.6666)]. The non-compliance rate was 77.5% among the self-transferred and 63.01% among the transitioned patients (p = 0.0534), resulting in a significantly higher adherence to medications among the transitioned group compared to the self-transferred patients [31.88% versus 16.42% non-adherence rate, p = 0.0455; OR 2.383 (CI 95%: 1.042–5.156)]. During the changing period to adult care, 8.89% of all patients discontinued their medications, accounting for 10.94% of the self-transferred and 7.04% of the transitioned patients (p = 0.2900).
Adult healthcare providers and treatments
The transitioned patients continued their medical care during the majority (96.06%) of the follow-up period in IBD-Centrums, classified as healthcare providers specializing in the treatment of IBD patients, which rate was significantly lower among the self-transferred patients (36.7%, p < 0.0001; OR 0.0238 [0.0218–0.0261]). The proportion of the patients, who changed their adult care physician at least once during the follow-up period was 21.74% of the self-transferred and 8.96% of the transitioned patients (p = 0.0564).
After being moved to adult care, 63.97% (n = 87) of all patients required a therapy change, without a significant difference between the self-transferred and the transitioned group (p = 0.7233). The mean time elapsed until the first therapy change was 230.82 ±320.86 days among the transitioned and 154.47 ± 236.46 days among the self-transferred patients (p = 0.2107). Therapy escalations accounted for 62.5% of all these treatment modifications, of which 5% were the reinduction of the self-discontinued medications.
Side effects of IBD medications were reported in 34.76% of all patients, most frequently from methotrexate (every 1069 medicine-days), steroids (every 1252 medicine-days), and infliximab (every 1300 medicine-days).
Hospitalizations and surgical interventions
The hospitalization rate among the patients moved to adult care was 20.59%, accounting for 16.42% of the transitioned and 24.64% of the self-transferred patients [p = 0.2908, OR 1.396 (95% CI: 0.6258–3.102)]. The most common reasons for hospitalizations were surgeries (33.33%) and relapses (31.67%), with only one patient being admitted to the intensive care unit; she was a female with CD, self-transferred to adult care, and needed intensive care treatment after an emergency bowel resection surgery.
During pediatric care, 15.01% of the patients required surgical intervention (n = 53), with a mean age of 14.56 ± 3.76 years and a mean disease duration of 2.79 ± 2.94 years at the time of the first operation. In adult care, 12.5% of the patients required a surgical intervention, after a mean time of 1.86 ± 1.5 years since transfer, without a significant difference between the self-transferred or the transitioned group. 22.58% of these procedures were emergency interventions, without difference between the two groups.
IBD-related complications
Every fifth patient had an IBD-related complication during pediatric care (23.36%), with a mean of 15.64 ± 4.5 years and a mean disease duration of 4.83 ± 4.13 years at the time of the reported complication. Hospitalization was necessary in 51.24% of the cases, with a significantly higher surgical rate in adult care compared to pediatric care [30% versus 12%; p = 0.0255; OR 0.3475 (0.151–0.8323)].
Bone densitometry was performed in 77.49% of our patients (n = 272). Bone density was decreasing with both age and longer disease duration, with most patients having at the time of transfer and being at high risk for osteoporosis and pathologic fractures during adult care [Figure 6(a) and (b)]. The mean age for patients with osteoporosis was 16.44 ± 2.27 years with a disease duration of 6.10 ± 4.37 years. Pathologic fractures were reported in five patients, on six occasions (Figure 6).

Bone densitometry results of the patients regarding age and disease duration with linear trend model and 95% CI. (a) Age and (b) Disease duration.
CD patients were prone to malnutrition during the examination period, with 11.94% of their weight measurements being at the severely low range (<3 pc), and a significantly lower proportion of their measurements being in the normal range (10–90 pc), compared to either the IBD-U or the UC patients (81.57% and 78.27%, p < 0.0001).
IBD-U patients were shown to be at high risk of inadequate growth, as 9.23% of all their height measurements were at the severely low range (<3 pc), compared to the 4.62% reported among the CD and 0.26% of the UC patients [p = 0.0089 and p < 0.0001; OR 0.4767 (0.2884–0.8179)].
At the time of the diagnosis, all patients had their BMI percentile in the normal range (5–85 pc). The proportion of the patients being in the normal BMI percentile range significantly decreased for all disease subtypes after 5 years of disease duration, resulting in a high risk for non-adequate nutrition and/or growth by the time of transfer to adult care [p < 0.0001, OR 149.1 (9.012–2468)].
Malignancies were reported in two patients during the follow-up period. Both patients have CD and are male. A gastrointestinal neuroendocrine tumor was an accidental finding in pediatric care in an adolescent patient during the histological examination of a bowel segment resected during emergency surgery after an ileus. In a young adult patient, lymphoma was reported to be potentially linked to infliximab treatment after self-transferring to adult care.
Discussion
This study aimed to define the clinical determinants of a successful transition and examine the objective and measurable effects of the changing process from pediatric to adult care on the disease course, activity, and patient compliance, including the comparison of a structured transitional program with self-transfer. Furthermore, we wanted to determine the unique characteristics of PIBD patients, that require special attention in adult care.
Despite transition being inevitable for PIBD patients and in the past decades it has been increasingly recognized as an essential, yet challenging element in ensuring the best possible disease outcome and overall health for patients, there are currently no consensus transitional guidelines and practices. 41 To date, most of the transitional recommendations are based on single-center studies, expert opinions, or surveys, and did not detect the long-term outcomes of structured transitional interventions. 42 However, extrapolating from the research data from a broader pediatric spectrum, young adults are expected to face similar difficulties during and after the healthcare-changing period, resulting in disruptions in their medical care, more frequent relapses, complications, and increased morbidity. 21
What are the determinants of a successful transitioning process?
As there is no clear definition of the term ‘successful transition’, it is rather challenging to compare studies evaluating the success rate of different transitioning practices or a structured program with self-transfer. 42 The most commonly used outcome to measure the success of a transitional program, as suggested by ECCO, is the continuity of care, but other objective measures are also in use, such as hospitalization or surgical rates, or quality of life. 43 Continuity of care is a multi-dimensional, patient-oriented construct, composed of health-service-related domains, including care coordination, care integration, and patient-provider communication. 44 The importance of continuity of care has been documented and objectively measured in numerous pediatric-onset chronic diseases. 44 Even with a successful transition, it is challenging to keep up the continuity between the last pediatric and the first adult care visit, as this is the most vulnerable period of the changing process, without a definitive connection to either of the healthcare systems. This changing period was reported to be longer, than 6 months among type 1 diabetes mellitus patients, whereas Yearushalmy-Fehler et al. found it to be less than 3 months for their IBD patients.45,46 Among our patients who were successfully moved to adult care, this time spent without definitive care between the healthcare systems was significantly longer among the self-transferred group, with a mean of nearly 1 year elapsed until the first attended adult care visit.
Disease-specific knowledge, self-efficacy, and autonomy are thoroughly studied and recognized as critical parts of transition readiness. The reluctance of patients and their parents, due to the close relationship with their pediatric healthcare providers is generally considered one of the main limitations to a successful transfer.19,47–50 Furthermore, worries about working with a new healthcare provider, preconceptions of receiving poorer care in the adult healthcare system and parental involvement are frequently reported as barrier factors. 51 There are fewer studies examining the effects of clinical variables on the success of the transitioning process, and their reported results show great variability. Keefer et al. found, that patient demographics, disease, or socioeconomics did not impact transition readiness, once self-efficacy and resilience were taken into account.52–54 In a study examining patients between 16 and 25 years, higher age and female gender were associated with better transition readiness. 55 McManus et al. in their survey-based study found that male patients, and those with developmental, physical, or psychological impairments were less likely to successfully transition to adult care. 56 Van den Brink et al. examined 50 PIBD patients who enrolled in a structured transition and evaluated their clinical data after a 2- to 6-year-long follow-up period. Female patients and the ones with active disease before the transferring process were more likely to have an unsuccessful transfer, although these results did not reach the level of significance. 57 In correspondence with the results of Van den Brink et al., we found female gender to be a significant barrier factor for a successful transfer, with 87.5% of the patients who discontinued their medical care during the transferring period being female, regardless of their involvement in the transitioning process. On the contrary, in our study, the higher number of days spent hospitalized during pediatric care seemed to be the only significant risk factor for discontinuing care during the pediatric healthcare period.
The currently reported overall success rate of the changing process between the pediatric and adult healthcare systems is similar across the globe. In a Canadian study examining nearly three thousand PIBD patients a 17.5% lost-to-follow-up rate was documented, whereas in British Columbia it was reported as 15–18%.58,59 Correspondingly, we found a 13% lost-to-follow-up rate among our patients during transfer, which was higher than the one found in either pediatric or adult care. An unsuccessful transition to adult care is shown to be associated with an increased number of emergency interventions, hospitalizations, higher surgical rates, more frequent therapy escalation, and a worse overall disease outcome and health. 58
What are the short- and long-term effects of the changing process to adult care, including the comparison between transition and self-transfer on the disease activity, course, and patient compliance?
The changing process to adult care is very complex and dependent on numerous patient-, healthcare provider-, and family-related factors. Inadequate transitional care is associated with non-adherence to medications and non-compliance regarding visits, restricted growth potential, higher disease activity, and an increased risk of surgery. 16 Without a structured transitional program, adolescents and young adults with chronic medical conditions face many risks, with possible lifelong consequences, including delays in appropriate medical care and loss-to-follow-up.13,28,29,60 The risk of adverse health outcomes after transferring to adult care due to a poor or lack of a transitional process is firmly established.24,43,61–66 Improved health-related outcomes have been documented among patients with numerous different chronic conditions after being enrolled in transition as opposed to transfer; however, there is a lack of data comparing these two for IBD patients. 55 The transfer is advised to be done during stable disease and psychosocial remission, as the changing process itself is thought to have a negative effect on the disease activity.67,68 A study from the Netherlands comparing direct transfer with structured transitional care among IBD patients reported a significantly higher disease activity at the time of the changing process among the transferred patients, with every third patient having an active disease, compared to less, than 10% among the transitioned patients. 69 We found the same difference among our patients, as a significantly higher proportion of the self-transferred patients had an active disease during transfer, affecting every third patient; therefore, the timing of the transfer was better among the patients enrolled in our transitional program.
Continuity of care is a core issue during the changing process from pediatric to adult healthcare systems. 70 A study reported a decreased lost-to-follow-up rate in adult care after being enrolled in a structured transition among type 1 diabetes mellitus patients. 28 Cole et al. in the United Kingdom compared the patients enrolled in a transitional program with a historical group without any formalized transitioning process and reported significantly higher medication adherence rates and lower nonattendance, hospitalization, and surgical rates, although the treatment characteristics were not the same between the two groups. 33 The lost-to-follow-up rate among our patients after the initiation of transfer to adult care was significantly higher than it was during pediatric care, with every fifth patient discontinuing their medical care. After being moved to adult care, transition was shown to be the only significant protective factor in continuing care, resulting in a 1.59-fold increased risk among the self-transferred patients to discontinue their medical care.
The compliance of adolescent IBD patients is reported to be the lowest among all age groups and even tends to deteriorate after being moved to adult care. 71 We found the same tendency, with a significant worsening in the compliance of the patients after being moved to adult care, exceeding a 70% non-compliance rate. This accounted for 77% of the self-transferred and 63% of the transitioned patients and although it did not reach the level of significance, but showed a trend. The medication-nonadherence rate of adolescent IBD patients in the current publications ranges from 50% to 88%.72–74 Consequently, among nonadherent patients, a 5.5-fold greater risk of relapse had been reported, raising the annual healthcare costs by 12.5% compared to the adherent patients.75,76 A retrospective study from Canada, reviewing the cases of 95 pediatric-onset IBD patients who were moved to adult care without a structured transitional program reported significantly fewer outpatient visits and higher non-compliance rates in adult care, without differences in the hospitalization, surgical, or emergency visit rates. 77 During the changing process to adult care, nearly 10% of our patients discontinued their medications. After being successfully moved to adult care, the medication adherence of the transitioned patients was significantly higher, with a non-adherence rate being twice as high among the self-transferred patients. Brooks et al. found the same result in their study, as medication adherence was higher among the patients being enrolled in a transitional program. 16
A structured transitional program is potentially associated with a positive impact on patient compliance, disease course, and activity and promotes better healthcare resource utilization. 19 Accordingly, significantly more of the self-transferred patients enrolled in our study experienced relapses during the follow-up period in our study, resulting in a 1.88-fold increased risk of relapse after being moved to adult care compared to the transitioned patients. Furthermore, the self-transferred patients had severe disease activity in a significantly higher and remission significantly lower proportion of the follow-up time in adult care compared to the transitioned patients. We found no difference between the two groups regarding hospitalization or surgery rates, as reported by Cole et al. 33
What are the unique characteristics of PIBD patients that require special attention in adult care?
PIBD is usually more extensive compared to the adult-onset form, with more than 40% of pediatric-onset CD patients having simultaneous ileocolonic and upper gastrointestinal involvement compared to 3% among adult patients. 78 Significantly more pediatric UC patients have pancolitis than adult-onset patients, with a 60% to 80% rate compared to a 20% to 30% rate.78–80 Accordingly, simultaneous ileocolonic involvement was documented in 57% of our CD patients, with 55% of our UC patients having pancolitis. Additionally, the disease of every third patient became more extensive during the follow-up period.
PIBD is usually characterized by a rapid disease progression, with every tenth patient requiring surgery in the first year following the diagnosis and every third to fifth after 5 years of disease duration.81–83 The colectomy rate among pediatric UC patients is reaching 40%, compared to half as much reported among adults.78,84 Of all CD patients, up to 80% require surgical intervention, with every tenth needing a permanent stoma. 85 Among our patients, the surgical rate during pediatric care was 15%, after a mean of less, than 3 years of disease duration at the time of surgery and every fourth intervention being an emergency procedure.
By the time they arrive at adult care, PIBD patients are frequently affected by the complications of their disease, making their treatment especially complicated. The most commonly reported extraintestinal complications of PIBD are inadequate nutrition and growth, poor bone health, fertility problems, and malignancies.86–90 Every third pediatric CD patient is reported to experience linear growth retardation prior to the gastrointestinal manifestations, secondary to malnutrition and chronic inflammation, which consequently can lead to delayed puberty and further related complications.91,92 Approximately in half of the adult patients with PIBD the final height is 10% lower than in the general population. 93 Among our patients, IBD-U patients were reported to be at high risk for growth retardation, with nearly 10% of their measurements being in the severely low range. During our study period, the CD patients were at high risk for malnutrition, with more, than 10% of their measurements being in the severely low range. Additionally, considering all of our patients, the range of patients being in the normal BMI percentile significantly decreased after 5 years of disease duration, affecting every disease subgroup.
Chronic blood loss and inflammation, increased energy requirements, intestinal malabsorption, and frequent treatment with corticosteroids contribute to poor bone health among IBD patients. 86 The measured bone density of our patients was decreasing with both higher age and longer disease duration, with patients being at high risk for osteoporosis and consequential pathologic fractures at the time of transfer to adult care. Every fifth patient experienced an IBD-related complication already during their pediatric care, further complicating their disease by the time of transfer.
Despite adolescents with IBD tend to have a medically more complex disease compared to adult patients, they have lower compliance to their care or adherence to their medications.65,77 During our study, 14% of all patients discontinued their medical care before being moved to adult care, in which the higher number of days spent in hospital yearly was a risk factor. A systematic review of studies published since 2005 found a 93% oral medication non-adherence rate among adolescents. They pointed out that this high non-adherence rate can lead to mistakenly perceived treatment failure, prompting ill-founded therapy escalations. 94 Other researchers are reporting a slightly lower medication non-adherence rate, it being between 50% and 66%. 95 Non-compliance was reported in two-thirds of our patients, with the most common problem being non-adherence to clinical attendance, followed by every third of patients having medication non-adherence. Of our patients, every third experienced a medication side-effect during the examination period, which can also contribute to medication non-adherence. The non-compliance rate was increasing with both higher age and longer disease duration among our patients, reaching more than 50% at the mean age and disease duration of transfer.
The differences between the pediatric- and adult-onset IBD and two healthcare systems, the high complication rate and rapid progression of the PIBD, the inadequate knowledge and self-efficacy of young adults on the verge of being transferred to adult care emphasize the need for a structured, organized, and planned transitional process. 46 Furthermore, it is essential for PIBD patients to be treated in IBD-Centrums both before and after transition, where the healthcare-providing multidisciplinary team has access to all those diagnostic and therapeutic interventions that are necessary to ensure the best possible disease outcome for this unique patient group.65,96 During the follow-up period in adult care, the transitioned patients continued their medical care in IBD-Centrums 96% of the time, compared to 37% found among the self-transferred patients. This can result in suboptimal disease control and impaired treatment possibilities, with a higher complication rate and a worse overall disease outcome among the self-transferred patient group. Adult healthcare providers should be aware, that the patients being transferred to them greatly differ from the same-aged, but adult onset-IBD patients, with a medically already complex disease course with former surgeries, often complicated with growth impairment and malnutrition, emotional distress, and non-compliance. Addressing the differences in the clinical characteristics and the course of pediatric- and adult-onset IBD, as well as the differences among the two healthcare systems is a critical step in understanding how to manage and perform a successful transition. 42
Strength and limitations
To our knowledge, our study has the highest number of patients enrolled in a structured transitional program with a comparable control group, that examined objective and measurable clinical outcomes with a long follow-up period. Furthermore, the strength of our study is the long examination period with an accessible medical databank from all patients from both pediatric and adult care.
We acknowledge that our research has limitations. The enrollment in the transitional and the self-transfer groups was not randomized, although there was no difference in any patient-, disease-, or treatment-specific variable between the two groups. The data collection was partially retrospective. The transition readiness was not objectively measured, but rather based on the assessment of the pediatric care physician, and the opinion of the patients and their parents. As there are currently no clear definitions for successful transfer and lost-to-follow-up patients, we had to define these based on the most common recommendations of the literature. Finally, from the pediatric time period the study included a single center, as patients just partially were treated in other clinics.
Conclusion
We found a positive association between a structured transitional program and lower disease activity, fewer relapses, and better adherence to medications as opposed to self-transfer. Furthermore, enrollment in transition was shown to be the only significant protective factor for continuing medical care after transfer. The changing process to adult care was linked to a deterioration in medication adherence and in overall compliance of the patients, with a high lost-to-follow-up rate between the healthcare systems regardless of enrollment in a structured transition, in which female gender was a risk factor. The PIBD patients had an extensive and medically complex disease upon arriving at adult care, with a history of former surgeries and IBD-related complications, high rates of malnutrition, growth impairment, and poor bone health, and with their compliance worsening with both higher age and longer disease duration.
Based on our results and the corresponding reports of the current literature, the conduction of numerous, multi-centric transitional studies is advised in the future, as structured transitional programs seem to have a key role in ensuring the best possible disease outcome for PIBD patients. These future studies could guide the recommendations, and help the establishment of a gold-standard transitional and educational method.
Supplemental Material
sj-doc-1-tag-10.1177_17562848241252947 – Supplemental material for Transition is associated with lower disease activity, fewer relapses, better medication adherence, and lower lost-to-follow-up rate as opposed to self-transfer in pediatric-onset inflammatory bowel disease patients: results of a longitudinal, follow-up, controlled study
Supplemental material, sj-doc-1-tag-10.1177_17562848241252947 for Transition is associated with lower disease activity, fewer relapses, better medication adherence, and lower lost-to-follow-up rate as opposed to self-transfer in pediatric-onset inflammatory bowel disease patients: results of a longitudinal, follow-up, controlled study by Luca Tóbi, Bence Prehoda, Anna M. Balogh, Petra Nagypál, Krisztián Kovács, Pál Miheller, Ákos Iliás, Antal Dezsőfi-Gottl and Áron Cseh in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.