
Abstract
Clostridioides difficile infection (CDI) is a complex disease that by virtue of both its initial virulence and proclivity toward recurrent episodes causes a high morbidity, mortality, and financial burden. This burden is felt by patients and their families as well as the U.S. healthcare system. Recurrent CDI episodes can occur in 25–65% of patients, with a cycle of multiple recurrences in a single patient contributing to the complexity of care. Patients with or suspected of having CDI will receive treatment and their care will be managed across multiple healthcare settings and will include many different levels of healthcare workers. The understanding of this infection is essential for all who are involved in the care of these patients. A well-structured and implemented Transition of Care process can ease the burden on the healthcare system, patients, and their families; reduce the cost of care; and improve patient outcomes. We review the development of Transitions of Care processes, resource guides, and their relevance to improving the management of CDI.
Introduction
Clostridioides difficile (C. difficile) is a Gram-positive, spore-forming anaerobic bacillus that can be transmitted from person to person or through contact with environmental contamination, 1 which can lead to a diarrheal illness in humans: C. difficile infection (CDI). 2 Data show that after an initial episode of CDI, up to 25% of patients experience a recurrence.1–4 Furthermore, of the patients who have had a recurrence, up to 65% will experience subsequent recurrence.5–7 A vicious cycle of infection–reinfection impedes recovery, thereby exacerbating the substantial morbidity and economic impact associated with CDI. 8
Patients with suspected CDI are recognized, diagnosed, and managed in multiple healthcare settings which provide a complex web of potential pathways for CDI transmission. Traditionally known to infect the hospitalized elderly, CDI now affects community members and residents of post-acute and long-term care facilities. CDI complications such as dehydration, profuse diarrhea, electrolyte disturbances, pseudomembranous colitis, or sepsis can result in hospitalizations,9,10 and patients with a CDI have an average hospital length of stay of 8.0 days for an index episode and 9.3 days for a recurrent CDI (rCDI) episode. 11 Hospitalized patients with CDI are frequently discharged home or to long-term care facilities prior to completion of CDI therapy and with a high risk of recurrence and readmissions. Recurrent CDI not only impacts patient quality of life, but recurrent CDI requiring rehospitalization imposes an increased health care burden and costs in terms of 30-day readmission, length of stay, and mortality.
These considerations make transitions of care in CDI critical in reducing the likelihood of recurrence and to improve health outcomes in these patients. Resource guides for effective transition of care and CDI patient homecare have been developed. We will now review the key components and barriers in the context of managing CDI.
Epidemiology
Recent studies on the incidence of C. difficile in the United States show a slight decrease in overall numbers but a growing proportion of community-acquired infections. In 2017, the estimated national burden of both community-associated and health care‒associated C. difficile was 428,600 cases (95% CI: 428,600–495,600 cases) 12
In 2017, Ma et al. 13 studied the incidence of recurrent CDI in the United States using a database of almost 39 million commercially insured people, of whom 45,341 developed CDI between 2001 and 2012. During this period, the annual incidence of CDI increased by 42.7%, from 0.4408 to 0.6289 cases per 1000 person-years (p = 0.004). However, the annual incidence of multiple-recurrence CDI (mrCDI) increased by 188.8%, from 0.017 to 0.0309 cases per 1000 person-years over the same period (p < 0.001).
The movement of patients between healthcare settings has been shown to have an impact on the acquisition of C. difficile. This transfer can occur between hospitals or between hospitals and long-term facilities. DiDodato 14 studied the effect inter-hospital transfer of patients has on the transmission of C. difficile using a network approach and demonstrated a 4.5% increase in CDI in university hospitals and a 3.5% increase in CDI in community hospitals. It was noted that antimicrobial stewardship programs could reduce this cross infection but that the heterogeneity of these programs may not provide consistent advice on reducing or preventing the transfer of CDI. Ponnada et al. 15 demonstrated some colonization of patients transferred from a Veteran Affairs hospital to long-term care facilities with 3 of 4 patients developing CDI within a month of transfer. These studies highlight the ease with which C. difficile is transmitted between healthcare units and that thorough information transfer and transitions of care can contribute to enhancing post-hospitalization care.
Burden of recurrent CDI (rCDI)
The Centers for Disease Control and Prevention (CDC) define a recurrent episode as one in which a positive C. difficile stool specimen is documented between 2 and 8 weeks after the last positive specimen. 16 Although this definition of rCDI is commonly used to identify and characterize recurrence, especially in clinical trial settings, it is not uniformly used. Various studies use 4, 8, or 12 weeks as the period to determine recurrence, and some studies report recurrences over longer periods of time.3,17
Data show that after an initial episode of CDI, up to 25% of patients will experience a recurrence.1,3,16 Data indicate that in the United States, recurrence accounts for 75,000 to 175,000 additional cases of CDI per year. 18 A recent retrospective, real-world analysis of 46,571 patients with CDI found that those with three or more recurrences had a mean of 5.8 inpatient visits and 4.6 emergency department visits per patient in a 12-month follow-up period. 19
Recurrent CDI requiring rehospitalization imposes an increased health care burden in terms of 30-day readmission, length of stay, and mortality. Zilberberg et al. 19 studied diagnosis-related group reimbursement for these parameters in 39,274,132 discharges in the Healthcare Cost and Utilization Project (HCUP) for California, Florida, Iowa, and New York. Of the total, 385,682 were discharged with a CDI code (initial CDI hospitalization), and in the following 60 days, 99,175 (25.7%) were re-hospitalized. Of the latter group, 36,504 (36.8%) were readmitted for CDI (rCDI); rCDI was the principal diagnosis in 14,005 patients (38.4%), and rCDI was the secondary diagnosis in 22,499 (61.6%). 19
Moreover, 6% of CDI patients have been shown to require surgical intervention, such as a colectomy. 20 Mortality has been shown to be 5–15% with rCDI, and more serious manifestations such as fulminant disease show mortality rates of 34.7%. 21 Demonstrating the potential long-term impact, a CDI infection can have upon a patient’s life.
Data from 2014 published in 2016 from 3554 hospitals showed that 11% had reported an increase in CDI incidence, with a Standardized Infection Ratio (SIR) of 0.92 compared to the national SIR. The implications of these increases can lead to the reduction in Centers for Medicaid and Medicare Services (CMS) payments to the offending healthcare system. 22
Zilberberg et al. 23 examined patients aged >65 years who were transferred to a nursing home, revealing a recurrence rate of more than 33%. The adjusted excess hospital days per patient were 20.3 (95% CI: 19.1–21.4) and Medicare reimbursements in the recurrence group was US$12,043 (95% CI: US$11,469–US$12,617). There were no excess deaths reported in this recurrence group. It was notable that the risk of a repeat hospitalization following recurrent CDI was significantly higher in this group compared with a case matched cohort. These data were corroborated by Dubberke et al. 24 who reported an excess cost of US$11,000 to recurrence within 180 days.
Impact of CDI on the patient
The long-term impact on patients with CDI includes reduced quality of life and generally poor outcomes.25,26 Moreover, there is a higher likelihood of patient discharge from the hospital setting with CDI to another healthcare facility such as hospice or a nursing home health facility compared to discharge to their home.
C. difficile infection has been associated with an increased incidence of psychiatric conditions, with anxiety and depression most commonly reported. The impact of CDI on quality of life has only recently begun to be understood. Garey et al. 27 explored three different Health-Related Quality of Life (HRQoL) instruments to develop a 36-item survey tool. This tool evaluated three major domains: physical, mental, and social with four associated subdomains. Ultimately, the researchers developed the CDiff32 HRQoL questionnaire. 27 This scoring system revealed that overall, the lowest scores (meaning highest impact) occurred with social questions relating to relationships, such as ‘My C. diff infection is affecting my closest relationships’, ‘Because of my C diff infection, I have difficulty being around people I do not know’, and ‘I feel that no one understands my C diff infection’. The most impactful question related to general physical complaints was: ‘Has C. diff infection prevented you from leaving your home?’ 27 Indicating that CDI infection can greatly influence a patient’s HRQoL, especially within the context of social interactions and activities.
Multifaceted management of CDI
Antibiotic treatment
If possible, the initial step is to be prudent in initiating antibiotics and to utilize them for the shortest appropriate clinical duration. The discontinuation and limitation of duration of any antibiotics being used to treat a systemic infection should be a consideration where safely possible. While it is important to limit the use of antibiotics in the CDI patient, antimicrobials are the mainstay of therapy along with infection control measures. The choice of antibiotic agent depends on disease severity and risk factors for recurrence. Cost considerations should be taken into account, but cost should be evaluated in a long-term perspective, importantly, more cost-effective in the long term is the most efficacious agent to resolve CDI, prevent recurrences, and avoid costly hospitalizations.
Healthcare network
The recognition of a recurrent case of CDI can be a challenge in terms of patient history and management. More rapid movement through the healthcare system in the course of an acute episode of care with many newer payment systems such as Accountable Care Organizations (ACO), 28 Bundled Payment Care Plans (BCMP), 29 and Special Needs Plans (SNP) 30 among others fracture the care of patients who may need longitudinal management of their illness such as CDI. The many different healthcare providers (HCP) which can be part of the overall care management process need to be aware of each case and where the patient may be on the recurrence CDI spectrum.
Surveillance & reporting
National Healthcare Safety Network (NHSN) 31 collects and provides facilities, states, regions, and the nation with data required to identify infectious problem areas, measure progress of prevention efforts, and with the goal to ultimately eliminate healthcare-associated infections (HAI). Moreover, facilities which participate in these programs operated by CMS must submit HAI outcome measures into NHSN system. CMS uses CDI outcomes as well as other HAI and quality metrics to determine hospital reimbursement levels as part of both the Value-Based Purchasing and Hospital-Acquired Conditions programs based on hospitals’ relative rankings. CMS institutes penalties for hospitals that fall into the lowest quartile of performance which can translate into losses of millions of dollars for healthcare facilities. CDI rates have not been decreasing in contrast to other HAIs.
Communication
State and federal public health authorities support interfacility transfer communication (ITFC) through recommendations, position statements, and laws. 32 Council of State and Territorial Epidemiologists 201633 regulates the communications regarding C. difficile during the process of transition of care. Recent data from one state, Oregon, 34 examined the compliance on mandated communications implemented during interfacility transfer. Currently no regulatory authority monitors compliance with the Oregon Administrative Rule 333-019-0052. There is no incentive to adhere to this rule thus implementation is generally suboptimal and communication methods nonstandardized. Interestingly in the state of Oregon, a survey conducted in 2015 and 2016 across hospitals and SNFs compared the application of multi-drug-resistant organisms (MDRO)/C. difficile written interfacility communications to anecdotally evaluate compliance with the State guidance, which showed a 10% increase in acute care hospitals self-reported compliance with State IFTC regulations (77% to 87%) over the period 2015 and 2016 while compliance in skilled nursing facilities remained static at 67%. The authors suggested that a registry with a common portal for data entry and access could help facilitate reliable knowledge about a patient’s status. They also suggested adaptation of a standardized IFTC form recommended by the CDC. 35
The breakdown of communications during the transition of patients between healthcare facilities and from healthcare facilities to home can result in patient harm and unnecessary expense to the patient and system. State and federal public health authorities via recommendations, position statements, and law will support interfacility transfer communication (ITFC). 36
The Council of State and Treatment Epidemiologists (CTSE) addressed the interfacility communication issues in their 16-ID-09 document. 37 Recently, the average length of stay in acute care institutions has declined while more extensive, complicated care is increasingly provided in long-term acute care hospitals, inpatient rehabilitation centers, and nursing homes. 38 The increasing movement of complex patients across the healthcare system brings new challenges for transitions of care and the facilities patients are transitioned to.
Communication failures both prior to or during post-acute care are frequent and cause significant patient harm. 39 Moreover, in the case of resistant or recurring infections such as CDI, a receiving institution may not have been informed of the critical need for recurrent infection control measures, thus leading to further CDI and other MDRO infections.
This poor communication can lead to surveillance being inadequate and result in inaccurate rates for public reporting and reimbursement under CMS Quality Reporting Programs and contribute to poor patient outcomes. The reasons for this poor interfacility communication are many and can include the following:
Lack of accountability
Resource limitation
The belief that these ‘infections are everywhere so why bother passing on the information’
Inadequate discharge planning and coordination on the part of the sending institution can contribute to the receiving facility being poorly informed.
Incomplete understanding of HIPPA laws and the circumstances under which protected information can be shared with the receiving facility.
Lack of adequate patient history, or contact information can also jeopardize effective transition of care.
Communication between the patient, their caregiver and the clinical team is another potential gap in supporting a positive discharge or transition plan. The lack of communication with the patient’s caregiver tends to create miscommunication, lack of understanding of the support needed for their loved one, and contributes to adverse outcomes.
Transitions of care, and its role in managing C. difficile infection
In 2003, the American Geriatric Society issued a position statement 40 which described transitional care as a set of defined actions developed to provide for the coordination and continuity of health. This statement specifically defined operational, research, and educational goals to further the understanding of transitional care. Timely transfer of accurate, relevant diagnostic findings, therapy, complications, consultations, and laboratory test results including any that are in process as well as arrangements for post-discharge handoff will improve the continuity of care. The discharge summary was the most common route of documenting a patient’s history and JCAHO required that discharge summaries be completed within 30 days of hospital discharge. 41 However, it is notable that not all care is from the hospital outwards, the continuum applies to anyone who provides care for a patient and transfers their care to another provider (either temporarily or permanently). This complex network of potential pathways is illustrated in Figure 1. 41 This figure shows the multitude of professionals that can come into contact with a patient.

Network of healthcare providers and care givers.
Clearly, accurate and timely communication is essential, but there are multiple barriers to effective transition of care which are particularly essential in the management of a recurrent disease such as CDI. Comorbidities are common among CDI patients and contribute to complicating factors or additional treatment needs. Another contributing factor, furthering the occurrence is that the patient will receive care and treatment in a variety of settings including acute, subacute care, long-term care facilities, primary care, and home health. The recurrent nature of the disease necessitates that accurate timely information is available to all involved in the care of CDI patients which includes the patient and care-givers as well as HCPs. That instruction should include infection control practices to be maintained by home-based caregivers as well. It is important that patients be educated to identify symptoms and to maintain appropriate treatment with CDI specific therapies. By effectively and consistently implementing transition of care methods the risk of recurrence, readmission to hospital, emergency room visits, and various complications are greatly reduced. Unfortunately, barriers exist which can prevent this effective process and can be at the system, clinician/HCP, and patient levels.
Systemic barriers
There are three principal system barriers that are recognized: suboptimal transition process, inadequate information transfer, and suboptimal medication management. Many health care systems tend to focus on a rapid discharge rather than a customized patient plan. Consequently, CDI patents may be discharged prematurely from the hospital without an adequate follow-up plan in place. Several components are essential for an ideal discharge plan and need to be provided to both the patient and care-giver. These include hygiene practices, both immediate and long-term medication management, and symptom recognition. This information can be provided in a printed form. Unfortunately, in today’s pressured environment, there is often diminishing time to effectively plan for transitions.
Information transfer is critical in the transition process, but often it is inadequate or occasionally inaccurate. Electronic health record (EHR) systems can potentially enable these data to be accessible but not all healthcare providers have the ability to access these data and electronic systems may be incompatible. Indeed, not all EHR systems support access to CDI discharge information. The available patient discharge information must be in multiple languages for the patient and their family caregiver. Transition information must be written with low health literate patients in mind, and offered through multiple formats, that is, written, verbal, and digital.
Medication management is an essential component of the discharge or transition process. The need for details of existing therapies must be passed on and a clear treatment plan outlined to the patient and caregivers. If the medications are not reconciled and appropriately transmitted at discharge, clinicians at subsequent HC facilities will be unaware of the correct list of patient medications. This lack of awareness can lead to medication errors, adverse events and possible readmission to the hospital. Insurance and formulary plan limitations also need to be considered with regard to continuation and duration of medications prescribed in the acute setting. Discrepancies can lead to facilities administrating an inappropriate drug regimen. Pharmacists have an important role in not only education and communication to the patient and their caregiver but also to the post-acute facilities. The intervention role must include a discussion of the CDI related medications being transferred with the patient and the ability of the long-term care facility to continue with the prescribed medication plan.
Clinical barriers: knowledge and training
Clinical barriers include lack of familiarity with the specific disease process such as CDI and the facility and clinician role in the transition process. In addition, discharge information may be delayed or the prescribing HCP be unaware of the range of medical services available for specific diseases. CDI is a complex infection, and the phenomenon of recurrent infections is not always fully appreciated. Nor is it well understood that rates of recurrence escalate as the patient has repeat events. HCPs across the many facilities may need education which they can subsequently pass onto the patient and their care-provider.
Moreover, clinicians, pharmacists, nursing staff, and other HCPs who ‘touch’ a patient should be involved in the transition process. However, not everyone in the chain appreciates their responsibilities and role in the transition of care pathway.
The efficiency and access to EHR systems may compromise data transfer and availability. Equally, the health services available in the community are unlikely to be known to all HCPs. It would be the role of case managers to assimilate this information and ensure it is accessible to the care team. Equally, community HCPs may not be aware of the history of a patient with CDI and the implications of ongoing observation.
Patient level barriers
Barriers also exist at the patient level which can play a major role in the management of CDI as well as other conditions. Several factors at the individual level can influence the transition process. These factors may include socioeconomic issues such as income level, education, employment status as well as access to essential services such as water, transportation, food and housing. Each of these can influence health outcomes. Unfortunately, some of these factors mean that patients do not access preventive or primary care and resort to receiving medical care in the emergency room or urgent care clinic where patient history information may not be available, and current issues may not then be transmitted to their HCP. Discharge details can present major challenges to some patients. They may be unable to recall or understand the instructions provided. This can be especially difficult in patients with chronic or recurring diseases who may have received frequently modified discharge instructions, some of which may actually contradict each other. In addition, care-givers and community health providers are often not included in the discharge process and are unable to maintain the appropriate prescribed care. It is useful to begin establishing patent assistance, prior authorization and collaboration with hospital pharmacists to create a plan to manage medications at the time of diagnosis rather than hurriedly at discharge. Finally, the cost of medication can provide a significant patient barrier and disrupt the transition of care process. If medication costs are not covered, community or post-acute healthcare facilities may prescribe alternative less expensive drugs which may be inappropriate, such as wrong antibiotics leading to recurrence of the original condition. Insurance authorization and coverage is also important to ensuring patient adherence to medication.
The combination of these socioeconomic and institutional factors and comorbidities can lead to lower adherence of medications which can lead to recurrent CDI.
Patient-centered approach
Gadbois et al. 42 conducted a qualitative nationwide survey to evaluate the patient experience of being transitioned from the hospital to the SNF. Overall, the patients felt that they were hurried into making decisions and were not appropriately prepared for the transition from hospital to SNF. The authors concluded that a failure to include patients with their family members in the care coordination process is of major importance.
Historically the effectiveness of transition of care has been assessed from the health care system perspective, which measures things like length of stay and re-hospitalizations and often excludes the patient viewpoint. The purpose of health care is to maintain or improve health; thus, a patient-centric approach is required. Issues of importance to the patient include physical and mental well-being, having a clear route of communication to discuss problems, knowing what to expect in the post-discharge period, and what medications to take or avoid, among other concerns. Consideration of vision impairment, hearing impairment, cognitive decline, and primary language must be elicited and accounted for in the transition instruction process.
To put these factors into focus, it is important to review them in the context of Clostridioides difficile which is the number one healthcare-associated infection in the United States. The condition is still prevalent and burdensome despite recent advances in management.
In a Medicare population, Zilberberg et al. 23 observed a recurrence rate of 33%, and of these two-thirds required readmission within a short time-period. Although in this specific study no effect was seen on mortality, readmission was associated with excess hospital days and the costs were significant. Interestingly, examining mortality further Olsen et al. 43 reported in an adult population there was no significant difference in mortality at 30 days, but a trend was seen at 60 days and significantly higher mortality at 90 and 180 days. These findings emphasized the need for care models in acute conditions which can recur, such as CDI, and patients should be informed about the possible long-term events and recognize the early signs and symptoms to enable rapid care. The subject of CDI and mortality is beyond this review, but it shows that the transition information must include information about potential long-term events and their consequences.
In addition to patients and caregivers being informed of the longer term issues with CDI it is vital that nursing home and SNF staff understand these as well. The transition of care process of CDI patients includes information on avoidance of certain medications such as broad-spectrum antibiotics, proton pump inhibitors (PPI), and other drugs which can directly affect the GI tract. Patients and caregivers must also be informed of the importance of noting key signs and symptoms suggestive of a recurrence of CDI such as frequency and type of bowel movement.
Strategies for the development of transition of care pathways
Many of the barriers described can be overcome with a planned approach to the transition of care for patients across the healthcare system. The National Transitions of Care Coalition (NTOCC), a coalition of multiple healthcare entities, has developed a seven-step approach to essential intervention categories during transitions to provide the highest probability of a successful transfer; 44 these are shown in Figure 245 and include the following:
Leadership support
Multidisciplinary collaboration
Early identification of patients
Transitional planning
Medication management
Patient or care provider engagement
Transfer of information

Effective transitions of care intervention categories.
Transition team
At the outset, it is essential to identify the members of an effective transition team. This should be inter-disciplinary and include all clinicians who may be involved in managing the patient: pharmacy, primary or community care providers, case managers, at-home or long-term care personnel and all others who interact with the transitioning patient. The interplay between the community and the hospital is a two-way pathway, so it is important for all concerned to know their role. The establishment of a transition coach encompassed within several transition programs such as the Care Transition Initiative 40 and the Transitional Care Model 46 can support post-discharge patient engagement as well as self-management. This role may best be fulfilled by case managers, patient navigators, social workers, and transition nurses rather than nurses or clinical staff physicians and pharmacists within the hospital system. Once the team is identified the discharge team must then develop a patient-centered transition process which should include a consistent messaging to patients, care providers, and post-acute facility personnel. The information should be clear, concise, and in a language and format that is accessible to patients and subsequent sites of care. Information should be a single concise packet if possible, and provision of contact numbers of critical staff must be included. Educate the patient and family members to practice self-care and medication management. In rural settings ensure the necessary members of the transition team are familiar with local resources and as appropriate establish telehealth or online access to HCPs.
The patient and their caregiver play an integral role in the transition process by being educated on their condition and being empowered to manage their own resources and ask the relevant person if they need assistance. With regard to CDI, some of these questions are shown in Table 1.
Standard questions for patient to ask after Clostridioides difficile infection discharge.

CDI, Clostridioides difficile infection.
The ability to personalize each patient’s care plan and educate them about their illness goes a long way to ensuring patient acceptance of their own care. Alternatively, family and/or caregiver will fill that role. An understanding of the recurrent nature of CDI must be stressed so that any future symptoms are noted and reported to the relevant transition manager or HCP. Self-determination and informed decision-making lead to a better prognosis especially in a recurrent illness such as CDI.
Implementing guidance and protocols to address barriers
Health care organizations should create discharge management protocols by consolidating discharge instructions into a single document with simple instructions that can be incorporated into the EHR and sent to the post-acute health facilities. A consolidated summary can help to minimize communication deficits. This summary should reflect the EHR which is accessible by all care providers in the next site of care, including those in the community. Patient education is important. Providing a checklist that providers can share with patients can ensure a smooth transition. The checklist should include medication payment assistance information, a medication management tool, instructions regarding reducing the potential transmission to household members, identification of risk factors (such as subsequent antibiotics or PPI prescribed by the HCP unaware of the patients CDI history), and tools to recognize the symptoms of CDI. An example of this type of guide is the color-coded guide for patients developed by the Doctor of Nursing Practice Project in Figure 3. 47
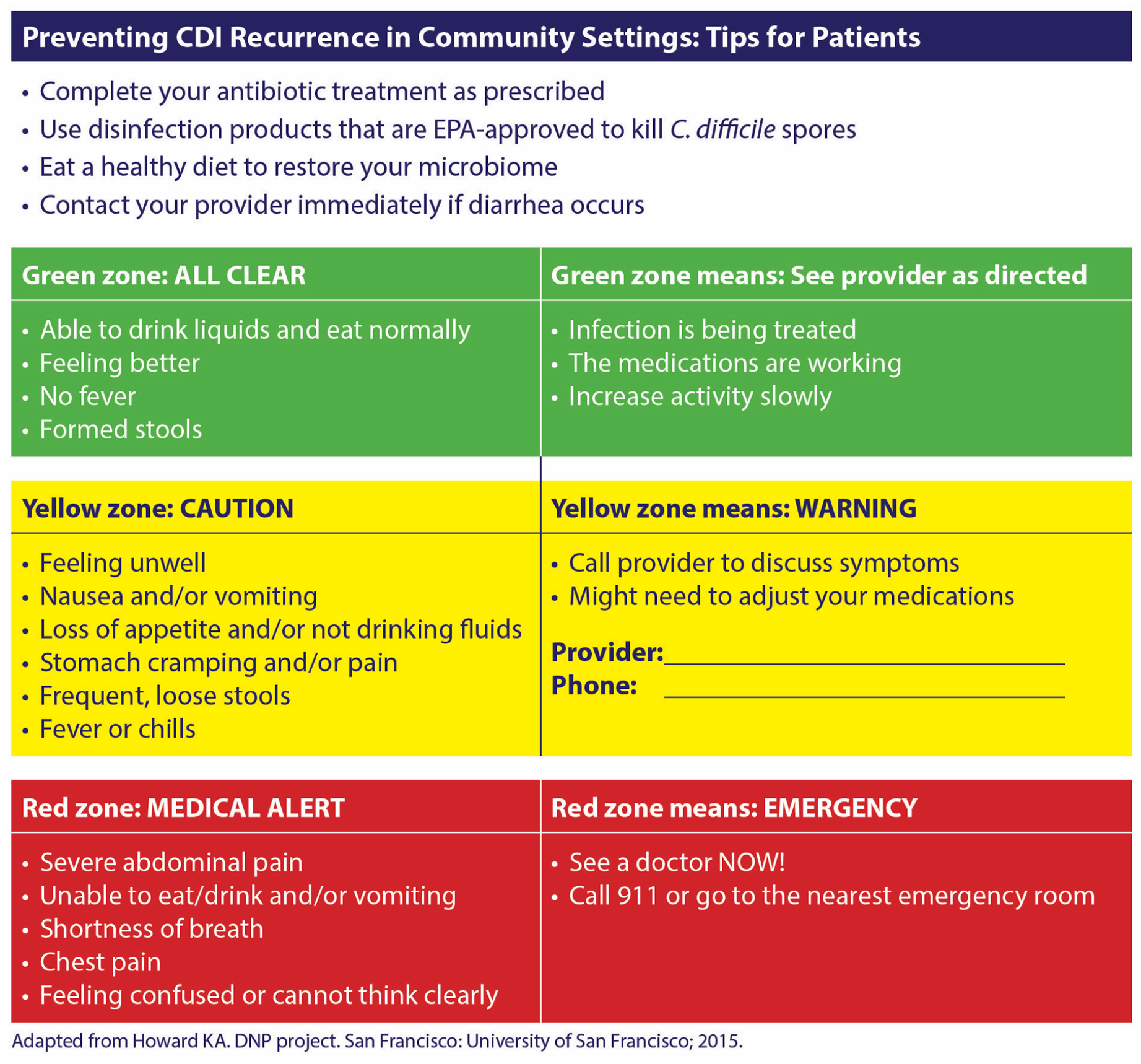
Preventing CDI recurrence in community settings tips for patients.
Discussion
Over 20 years ago, the Institute of Medicine (IOM) highlighted the relationship between medical errors and patient harm. 48 One year later the IOM addressed improved continuity of care as a priority of care in effective and responsible heath care delivery systems. 49 The older age group was recognized as being particularly at risk.
Clearly one of the most CDI susceptible patient populations is the elderly, many of whom are frail and may have cognition issues. It is estimated that over 20 million Medicare beneficiaries have five or more chronic conditions, and of these, 20% will be discharged to a SNF from hospital for post-acute care. It is known that there are problems associated with the hospital to SNF transfer. 50 Of concern is the fact that of these discharged patients, 20% will be readmitted to hospital within 30 days and many of these readmissions are preventable. As there are more than 5 million individuals who move from hospitals to SNF annually, it is the nurses who play a key role in receiving these patients. 51
In an effort to better understand the situation regarding this vital process, King et al. 52 evaluated the experience of 27 registered nurses and the transition of care from hospital to SNF using a qualitative study which employed grounded dimensional analysis, focus groups, and in-depth interviews. Unsurprisingly the SNF nurses reported difficulty in hospital to SNF transitions being the norm. Indeed, none were able to recall a recent good transition. Nurses reported many deficiencies with poor quality discharge communication being a major barrier to safe and effective transitions. In order to facilitate a safe transition, nurses need specific and current information, including descriptions of remarkable hospital events, written orders for medications, treatments, activity level, diet, accurate descriptions of functional and cognitive status, and pending hospital laboratory results in addition to social information. There was a litany of deficiencies and consequences reported by the respondents.
New systems are being developed to manage these complex multi-disciplinary processes, for example, DispatchHealth 53 (formerly CareLoop.com) which is a web-based information system accessible to all care providers specific to a single patient. Although not tested in the CDI situation, this holds the promise of fulfilling the NTOCC Seven Essential Interventions of Safe and Effective Transition of Care to home.
As an alternative to the conventional transitions process, telehealth offers great promise in helping lower avoidable readmissions, reducing adverse events, improving patient–provider communication, ensuring medication reconciliation, augmenting patient education, and as an educational resource for patients and family. Noel et al. 54 conducted a parallel-group, superiority, randomized controlled trial in which they enrolled 180 patients in the standard of care or Telehealth arms. Patients were evaluated at 30 days post discharge, with an endpoint of hospital re-admission. Patients were provided with telemedicine devices, ‘tablet monitor’, blood pressure monitor, pulse oximeter, and weight scale. Data were collected using the REDcap electronic data capture tool. Compared with the standard of care, Telehealth patients were more likely to have medication reconciliation (p = 0.013) and were 7 times more likely to adhere to medications than the control group (0.03). However, the study did not show any difference in hospital readmissions between the two cohorts despite patients expressing satisfaction with the system and adhering to medications more effectively. 55
In summary, it is vitally important that HCPs provide clear and relevant information for each patient as they progress through the healthcare system. This involves multiple ‘actors’ and ideally information should be accessible via an electronic portal for all potential care providers whether in hospital, SNF, Assisted Living Facility, primary care physician, or patient/care giver. Conditions which are acute but have the potential to recur should be explained thoroughly to avoid or reduce disease recurrences such as CDI, which can be costly and potentially life-threatening. The Transition of Care has multiple components and adherence to these steps by implementation of appropriate CDI focused discharge plans will enable optimal healthcare to be provided.
Footnotes
Acknowledgements
The authors would like to thank Nicolette Theriault for her editorial assistance.
Author contributions
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.L. and C.L. have no disclosures to declare. G.T. is a consultant to Melinta, Spero Pharmaceuticals, and Ferring Pharmaceuticals. S.K. is a consultant to Ferring.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Compliance with ethics guidelines
This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.